Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 4 (12-2025)
J Res Dent Maxillofac Sci 2025, 10(4): 262-273 |
Back to browse issues page

Ethics code: IR.SBMU.DRC.REC.1399.045
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jaberi Ansari Z, Valian A, Maghsoudlou nejad M. Effect of Different Repair Protocols on Repair Bond Strength of Aged Composite Restorations. J Res Dent Maxillofac Sci 2025; 10 (4) :262-273
URL: http://jrdms.dentaliau.ac.ir/article-1-745-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-745-en.html



1- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Restorative Dentistry, School of Dentistry, Golestan University of Medical Sciences, Gorgan, Iran. ,maghsoudlou.mahsa@gmail.com
2- Department of Restorative Dentistry, School of Dentistry, Golestan University of Medical Sciences, Gorgan, Iran. ,
Full-Text [PDF 587 kb]
(406 Downloads)
| Abstract (HTML) (1528 Views)
Full-Text: (451 Views)
Abstract
Background and Aim: This study assessed the effects of composite type, adhesive type, adhesive application protocol, and storage time on repair microshear bond strength (µSBS) of composite restorations.
Materials and Methods: This in vitro, experimental study was conducted on Z350 and Point 4 (n=360) composite discs that were stored in water for 3 weeks at 37°C. After roughening by bur and etching, the specimens were divided into 24 groups (n=15) based on the type of composite (Z350 and Point 4), type of universal adhesive (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instructions, waiting for 30 seconds, or diode laser irradiation of adhesive prior to polymerization for 30 seconds), and storage time (24 hours or 1 year). The specimens were bonded to Z250 repair composite, and underwent µSBS test. The mode of failure was also determined. Data were analyzed by four-way ANOVA and Tukey’s test (alpha=0.05).
Results: Four-way ANOVA showed significant effects of adhesive application protocol (P=0.000) and storage time (P=0.000) on µSBS. The interaction effect of the two on µSBS was also significant (P=0.046). The µSBS after 24 hours was higher than that after 1 year irrespective of the adhesive application protocol. The µSBS was maximum in the laser group followed by waiting for 30 seconds, and all pairwise comparisons were significant in this respect (P=0.000).
Conclusion: In aged composite restoration repair, diode laser irradiation of adhesive prior to polymerization or waiting for 30 seconds prior to adhesive curing can enhance the µSBS.
Keywords: Composite Resins; Dental Restoration Repair; Shear Strength
Introduction
Materials and Methods: This in vitro, experimental study was conducted on Z350 and Point 4 (n=360) composite discs that were stored in water for 3 weeks at 37°C. After roughening by bur and etching, the specimens were divided into 24 groups (n=15) based on the type of composite (Z350 and Point 4), type of universal adhesive (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instructions, waiting for 30 seconds, or diode laser irradiation of adhesive prior to polymerization for 30 seconds), and storage time (24 hours or 1 year). The specimens were bonded to Z250 repair composite, and underwent µSBS test. The mode of failure was also determined. Data were analyzed by four-way ANOVA and Tukey’s test (alpha=0.05).
Results: Four-way ANOVA showed significant effects of adhesive application protocol (P=0.000) and storage time (P=0.000) on µSBS. The interaction effect of the two on µSBS was also significant (P=0.046). The µSBS after 24 hours was higher than that after 1 year irrespective of the adhesive application protocol. The µSBS was maximum in the laser group followed by waiting for 30 seconds, and all pairwise comparisons were significant in this respect (P=0.000).
Conclusion: In aged composite restoration repair, diode laser irradiation of adhesive prior to polymerization or waiting for 30 seconds prior to adhesive curing can enhance the µSBS.
Keywords: Composite Resins; Dental Restoration Repair; Shear Strength
Introduction
Resin-based composites are currently the most commonly used dental materials for restorative procedures [1]. Despite the great advances made in their mechanical and physical properties, failure of composite restorations still occurs due to several reasons, mainly related to oral environmental conditions [1,2]. The annual failure rate of anterior and posterior composite restorations ranges from 1% to 4% [3,4]. In general, failed restorations should either be replaced or repaired [5]. Repair of partially fractured restorations is often preferred by dental clinicians, accounting for approximately 50% to 71% of the cases of failure [6]. The popularity of this approach is due to the following reasons: not requiring the removal of sound tooth structure in areas far from the fracture line, not requiring unnecessary extension of the cavity margins and subsequent weakening of tooth structure, lower risk of pulpal exposure, lower cost, and saving time, compared with complete restoration replacement [7].
The bonding of repair composite to aged composite is mediated by three mechanisms:
(I) micromechanical retention through the penetration of resin monomers into the surface irregularities, (II) formation of chemical bonds with the resin matrix, and (III) formation of chemical bonds with filler particles [8].
Bonding to aged composite restorations is highly challenging due to the decreased number of the available C=C bonds for bonding to repair composite [9]. Upon curing of composite, a non-polymerized oxygen-inhibited layer is formed on the surface exposed to air. This layer can bond to the next composite layer due to the presence of unreacted monomers. However, due to water sorption and loss of this superficial layer, which is rich in free radicals in aged composites, some concerns exist with regard to bonding of the aged composite to repair composite [10]. Therefore, several methods have been suggested to enhance the mechanical and chemical bond of the repair composites to aged composites. However, no consensus has been reached on this topic so far.
The bond strength at the composite-composite interface is influenced by a number of factors such as irrigation, etching, surface roughening by bur or disc, sandblasting, laser irradiation, type of composite, silanization, and type of adhesive [11]. According to a recent systematic review, surface roughening by bur and etching with phosphoric acid are more commonly used for elimination of surface impurities, and bonding agents are frequently used for bonding [12]. Also, surface conditioning is recommended for demineralization of dental hard tissue and elimination of superficial debris from the composite surface when part of the aged composite, enamel, and dentin are exposed [13,14].
Universal or multi-mode adhesives have recently gained increasing popularity since they can be used in self-etch, etch-and-rinse, and selective enamel etching modes [1,15]. They decrease the treatment time, technical sensitivity of the procedure, and procedural errors [16]. Also, they can bond to all types of substrates such as enamel, dentin, composite, noble and non-precious metals, and zirconia due to the presence of functional acidic monomers such as 10-MDP and 4-META in their composition [15]. Universal adhesives are more user friendly for composite restoration repair since enamel, dentin and composite borders are often present in aged composite restorations that require repair [17]. G-Premio Bond is a universal adhesive with “no-wait” protocol, which can be immediately cured after application [18]. However, Huang et al. [19] reported that increasing the working time by 10 seconds improved its short-term clinical efficacy. Clearfil Universal Bond Quick is another universal adhesive with the “no-wait” protocol. Its manufacturer claims that it provides a higher shear bond strength (SBS) to dentin due to its unique composition [20,21]. The effect of waiting time after adhesive application on the short-term and long-term bond strength of this new generation of universal adhesives for aged composite repair has not been evaluated before, and studies on this topic are required.
Presence of hydrophilic monomers and higher water content in single-bottle universal adhesives result in their higher permeability and subsequently greater susceptibility to degradation in the oral cavity [22,23]. It appears that increasing the temperature can effectively improve the adhesive-dentin bond strength [24]. Several studies have assessed the effect of diode laser irradiation before and after adhesive polymerization on bond strength to dentin and microleakage [22-24]. However, no previous study has addressed the effect of diode laser irradiation prior to adhesive polymerization on the bond strength of universal adhesives applied for composite repair.
The repair bond strength mainly depends on the type of aged composite rather than the type of repair composite. It has been discussed that the best results are achieved when the aged and the repair composite are of the same type. However, this is not often possible due to the lack of knowledge of dental clinicians about the type of aged composite in most cases [25]. Thus, the effect of type of repair composite should be further evaluated. On the other hand, some variations have been reported in immediate and delayed (after storage) composite repair bond strength [5], which should be further addressed.
Considering all the above, this study aimed to assess the effect of composite type (Z250 repair composite bonded to Z350 and Point 4), adhesive type (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instruction, waiting for 30 seconds, or laser irradiation of adhesive prior to its polymerization), and storage time (24 hours versus 1 year) on repair microshear bond strength (µSBS) of composite restorations.
Materials and Methods
The bonding of repair composite to aged composite is mediated by three mechanisms:
(I) micromechanical retention through the penetration of resin monomers into the surface irregularities, (II) formation of chemical bonds with the resin matrix, and (III) formation of chemical bonds with filler particles [8].
Bonding to aged composite restorations is highly challenging due to the decreased number of the available C=C bonds for bonding to repair composite [9]. Upon curing of composite, a non-polymerized oxygen-inhibited layer is formed on the surface exposed to air. This layer can bond to the next composite layer due to the presence of unreacted monomers. However, due to water sorption and loss of this superficial layer, which is rich in free radicals in aged composites, some concerns exist with regard to bonding of the aged composite to repair composite [10]. Therefore, several methods have been suggested to enhance the mechanical and chemical bond of the repair composites to aged composites. However, no consensus has been reached on this topic so far.
The bond strength at the composite-composite interface is influenced by a number of factors such as irrigation, etching, surface roughening by bur or disc, sandblasting, laser irradiation, type of composite, silanization, and type of adhesive [11]. According to a recent systematic review, surface roughening by bur and etching with phosphoric acid are more commonly used for elimination of surface impurities, and bonding agents are frequently used for bonding [12]. Also, surface conditioning is recommended for demineralization of dental hard tissue and elimination of superficial debris from the composite surface when part of the aged composite, enamel, and dentin are exposed [13,14].
Universal or multi-mode adhesives have recently gained increasing popularity since they can be used in self-etch, etch-and-rinse, and selective enamel etching modes [1,15]. They decrease the treatment time, technical sensitivity of the procedure, and procedural errors [16]. Also, they can bond to all types of substrates such as enamel, dentin, composite, noble and non-precious metals, and zirconia due to the presence of functional acidic monomers such as 10-MDP and 4-META in their composition [15]. Universal adhesives are more user friendly for composite restoration repair since enamel, dentin and composite borders are often present in aged composite restorations that require repair [17]. G-Premio Bond is a universal adhesive with “no-wait” protocol, which can be immediately cured after application [18]. However, Huang et al. [19] reported that increasing the working time by 10 seconds improved its short-term clinical efficacy. Clearfil Universal Bond Quick is another universal adhesive with the “no-wait” protocol. Its manufacturer claims that it provides a higher shear bond strength (SBS) to dentin due to its unique composition [20,21]. The effect of waiting time after adhesive application on the short-term and long-term bond strength of this new generation of universal adhesives for aged composite repair has not been evaluated before, and studies on this topic are required.
Presence of hydrophilic monomers and higher water content in single-bottle universal adhesives result in their higher permeability and subsequently greater susceptibility to degradation in the oral cavity [22,23]. It appears that increasing the temperature can effectively improve the adhesive-dentin bond strength [24]. Several studies have assessed the effect of diode laser irradiation before and after adhesive polymerization on bond strength to dentin and microleakage [22-24]. However, no previous study has addressed the effect of diode laser irradiation prior to adhesive polymerization on the bond strength of universal adhesives applied for composite repair.
The repair bond strength mainly depends on the type of aged composite rather than the type of repair composite. It has been discussed that the best results are achieved when the aged and the repair composite are of the same type. However, this is not often possible due to the lack of knowledge of dental clinicians about the type of aged composite in most cases [25]. Thus, the effect of type of repair composite should be further evaluated. On the other hand, some variations have been reported in immediate and delayed (after storage) composite repair bond strength [5], which should be further addressed.
Considering all the above, this study aimed to assess the effect of composite type (Z250 repair composite bonded to Z350 and Point 4), adhesive type (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instruction, waiting for 30 seconds, or laser irradiation of adhesive prior to its polymerization), and storage time (24 hours versus 1 year) on repair microshear bond strength (µSBS) of composite restorations.
Materials and Methods
This in vitro, experimental study was conducted on 360 composite discs fabricated from two different composite types (Z350 and Point 4). The sample size was calculated to be 15 in each group (a total of 360) using the one-way ANOVA feature of PASS 15 software assuming α=0.05, β=0.2, study power of 80%, effect size of 0.558, and standard deviation of 3.8 [24].
This study was approved by the ethics committee of the Faculty of Dentistry, Shahid Beheshti University of Medical Sciences (IR.SBMU.DRC.REC.1399.045).
Preparation of specimens:
A total of 360 disc-shaped composite specimens were fabricated in prefabricated plastic molds with an internal diameter of 6 mm, and 1 mm height from each of the Z350 and Point 4 composite resins (180 discs from each composite). One repair composite specimen was fabricated per each disc (for the µSBS test). The composite was applied into the mold. Mylar strips were placed on the top and at the bottom of each specimen before curing. The mold was then compressed between two glass slabs to obtain specimens with smooth surfaces [9]. Light curing was performed with a curing unit (Guilin Woodpecker Medical Instrument Co., Ltd., China) with a light intensity of 1000 mW/cm2 at 1 mm distance for 20 seconds from all directions. The output of the curing unit was measured by a LED radiometer (Light Curing Meter; SDI) prior to curing of the specimens [10].
Aging:
The composite specimens were immersed in boiling water for 8 hours, and were then stored in distilled water at 37°C for 3 weeks [17,26].
Surface treatments:
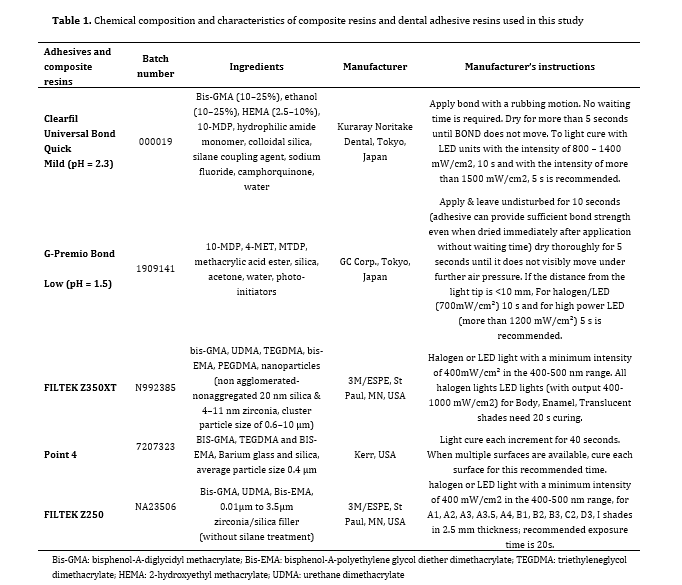
All specimens were roughened by bur (#882 round-end cylindrical diamond bur; Jota, Switzerland) with five sweeping motions. Each bur was replaced after five preparations. All specimens were etched with 35% phosphoric acid (K-ETCHANT Syringe, Kuraray Noritake Dental Inc., Japan) for 15 seconds, rinsed for 15 seconds, and dried with oil-free air spray [11]. Next, the specimens were divided into 24 groups (n=15) based on the type of composite (Z350 and Point 4), type of universal adhesive (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instructions, waiting for 30 seconds, or diode laser irradiation of adhesive prior to polymerization for 30 seconds), and storage time (24 hours or 1 year) [2, 8, 23] (Figure 1). Table 1 presents the characteristics of the adhesives and composite resins used in this study.
With respect to the adhesive application protocol, the adhesive was applied according to the manufacturer’s instructions in one subgroup. In the second subgroup, the adhesive was applied and allowed 30 seconds to react with the surface prior to polymerization, and was then cured. In the third subgroup, the applied adhesive underwent diode laser irradiation (Doctor Smile, LAMBDA Spa, Italy) with 810 nm wavelength and 1 W power in continuous-wave mode with a 300-nm fiber tip in non-contact mode (at 1 mm distance) prior to curing. The fiber tip was perpendicular to the composite disc, and scanned the surface in a circular motion from the center towards the periphery of the disc at a speed of 2 mm/second for a total of 30 seconds. Next, the adhesive was cured similar to other subgroups [23].
Figure 1. Study groups
Table 1. Chemical composition and characteristics of composite resins and dental adhesive resins used in this study
Application of repair composite:
Filtek Z250 composite (3M ESPE, St. Paul, MN, USA) was used for repair in all groups. Transparent Tygon tubes (Saint-Gobain Performance Plastics Corp., Akron, USA) with an internal diameter of 0.86 mm and 2 mm height were used for this purpose. The Tygon tubes were positioned on the surface-treated discs, and composite was packed into the tubes by a probe. Curing was performed for 20 seconds. Next, the specimens were incubated in distilled water at 37°C for 24 hours. The Tygon tubes were then removed by a scalpel. Half of the specimens underwent immediate SBS testing while the other half were stored in distilled water at 37°C for 1 year [5].
µSBS test:
A stainless-steel wire was tied around the composite cylinders along the bonded interface. The µSBS was measured by a microtensile tester (Bisco Inc.) at a crosshead speed of 0.5 mm/minute. Load at failure was recorded in Newtons (N) and converted to megapascals (MPa) using the following formula [2]:
µSBS (MPa) = Load (N) / Area (mm²)
Area = (π· r²) (mm²) r = bonding surface diameter
Mode of failure:
The mode of failure was determined under a stereomicroscope (Olympus LS, SZX9, Japan) at ×20 magnification and categorized as adhesive, cohesive, or mixed.
Statistical analysis:
The normality of data distribution was evaluated by the Kolmogorov-Smirnov test. The effect of type of adhesive, method of adhesive application, type of composite, and storage time (independent variables) on µSBS (dependent variable) was analyzed by four-way ANOVA. Since none of the interaction effects were significant, only the main effects were analyzed. Pairwise comparisons were performed by the Tukey’s HSD test. All statistical analyses were carried out using SPSS version 20 at 0.05 level of significance.
Results
This study was approved by the ethics committee of the Faculty of Dentistry, Shahid Beheshti University of Medical Sciences (IR.SBMU.DRC.REC.1399.045).
Preparation of specimens:
A total of 360 disc-shaped composite specimens were fabricated in prefabricated plastic molds with an internal diameter of 6 mm, and 1 mm height from each of the Z350 and Point 4 composite resins (180 discs from each composite). One repair composite specimen was fabricated per each disc (for the µSBS test). The composite was applied into the mold. Mylar strips were placed on the top and at the bottom of each specimen before curing. The mold was then compressed between two glass slabs to obtain specimens with smooth surfaces [9]. Light curing was performed with a curing unit (Guilin Woodpecker Medical Instrument Co., Ltd., China) with a light intensity of 1000 mW/cm2 at 1 mm distance for 20 seconds from all directions. The output of the curing unit was measured by a LED radiometer (Light Curing Meter; SDI) prior to curing of the specimens [10].
Aging:
The composite specimens were immersed in boiling water for 8 hours, and were then stored in distilled water at 37°C for 3 weeks [17,26].
Surface treatments:
All specimens were roughened by bur (#882 round-end cylindrical diamond bur; Jota, Switzerland) with five sweeping motions. Each bur was replaced after five preparations. All specimens were etched with 35% phosphoric acid (K-ETCHANT Syringe, Kuraray Noritake Dental Inc., Japan) for 15 seconds, rinsed for 15 seconds, and dried with oil-free air spray [11]. Next, the specimens were divided into 24 groups (n=15) based on the type of composite (Z350 and Point 4), type of universal adhesive (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instructions, waiting for 30 seconds, or diode laser irradiation of adhesive prior to polymerization for 30 seconds), and storage time (24 hours or 1 year) [2, 8, 23] (Figure 1). Table 1 presents the characteristics of the adhesives and composite resins used in this study.
With respect to the adhesive application protocol, the adhesive was applied according to the manufacturer’s instructions in one subgroup. In the second subgroup, the adhesive was applied and allowed 30 seconds to react with the surface prior to polymerization, and was then cured. In the third subgroup, the applied adhesive underwent diode laser irradiation (Doctor Smile, LAMBDA Spa, Italy) with 810 nm wavelength and 1 W power in continuous-wave mode with a 300-nm fiber tip in non-contact mode (at 1 mm distance) prior to curing. The fiber tip was perpendicular to the composite disc, and scanned the surface in a circular motion from the center towards the periphery of the disc at a speed of 2 mm/second for a total of 30 seconds. Next, the adhesive was cured similar to other subgroups [23].
Figure 1. Study groups
{kind=link}
Table 1. Chemical composition and characteristics of composite resins and dental adhesive resins used in this study
{kind=link}
Application of repair composite:
Filtek Z250 composite (3M ESPE, St. Paul, MN, USA) was used for repair in all groups. Transparent Tygon tubes (Saint-Gobain Performance Plastics Corp., Akron, USA) with an internal diameter of 0.86 mm and 2 mm height were used for this purpose. The Tygon tubes were positioned on the surface-treated discs, and composite was packed into the tubes by a probe. Curing was performed for 20 seconds. Next, the specimens were incubated in distilled water at 37°C for 24 hours. The Tygon tubes were then removed by a scalpel. Half of the specimens underwent immediate SBS testing while the other half were stored in distilled water at 37°C for 1 year [5].
µSBS test:
A stainless-steel wire was tied around the composite cylinders along the bonded interface. The µSBS was measured by a microtensile tester (Bisco Inc.) at a crosshead speed of 0.5 mm/minute. Load at failure was recorded in Newtons (N) and converted to megapascals (MPa) using the following formula [2]:
µSBS (MPa) = Load (N) / Area (mm²)
Area = (π· r²) (mm²) r = bonding surface diameter
Mode of failure:
The mode of failure was determined under a stereomicroscope (Olympus LS, SZX9, Japan) at ×20 magnification and categorized as adhesive, cohesive, or mixed.
Statistical analysis:
The normality of data distribution was evaluated by the Kolmogorov-Smirnov test. The effect of type of adhesive, method of adhesive application, type of composite, and storage time (independent variables) on µSBS (dependent variable) was analyzed by four-way ANOVA. Since none of the interaction effects were significant, only the main effects were analyzed. Pairwise comparisons were performed by the Tukey’s HSD test. All statistical analyses were carried out using SPSS version 20 at 0.05 level of significance.
Results
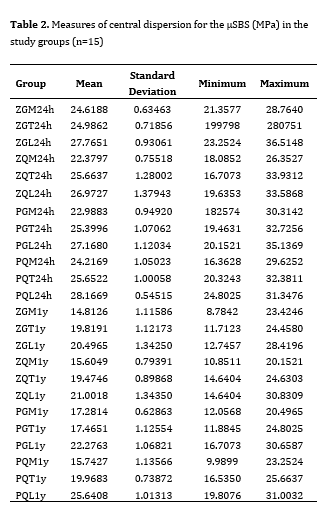
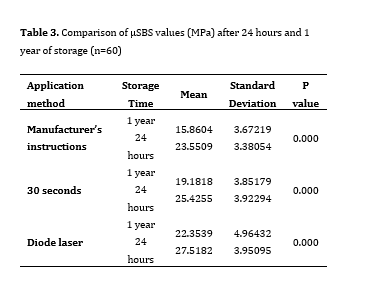
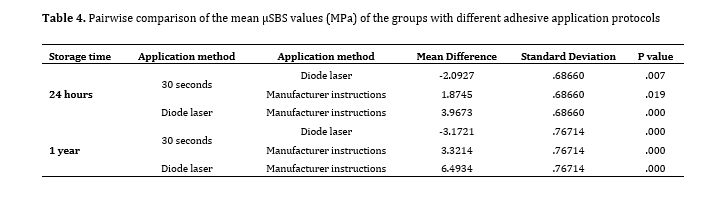
The mean µSBS of the groups is presented in Table 2. None of the specimens broke prior to the µSBS test. Four-way ANOVA showed significant effects of adhesive application protocol (P=0.000) and storage time (P=0.000) on µSBS. The interaction effect of the two on µSBS was also significant (P=0.046). No other significant interaction effect was noted. Since the interaction was ordinal type, it was concluded that the µSBS after 24 hours was higher than that after 1 year in all groups, irrespective of the adhesive application protocol (Table 3). The Tukey’s test was applied to compare different adhesive application techniques, which showed significant differences in all pairwise comparisons (Table 4).
ANOVA showed that the µSBS was not affected by the type of composite (P=0.94) or type of universal adhesive (P=0.278).
Figure 2 shows the frequency of different modes of failure. All groups with 24 hours of storage had lower frequency of adhesive failure than those with 1 year of storage. According to the adhesive application protocol, all laser groups had lower frequency of adhesive failure. As mentioned earlier, in groups with 1 year of storage, the minimum µSBS belonged to ZGM1y and ZQM1y which showed only adhesive failure and no mixed or cohesive failures. Also, in 1-year storage groups, the highest frequency of mixed failure and the lowest frequency of adhesive failure belonged to PQL1y group with maximum bond strength.
Table 2. Measures of central dispersion for the µSBS (MPa) in the study groups (n=15)
Table 3. Comparison of µSBS values (MPa) after 24 hours and 1 year of storage (n=60)
Table 4. Pairwise comparison of the mean µSBS values (MPa) of the groups with different adhesive application protocols
Figure 2. Frequency of different failure modes
Discussion
ANOVA showed that the µSBS was not affected by the type of composite (P=0.94) or type of universal adhesive (P=0.278).
Figure 2 shows the frequency of different modes of failure. All groups with 24 hours of storage had lower frequency of adhesive failure than those with 1 year of storage. According to the adhesive application protocol, all laser groups had lower frequency of adhesive failure. As mentioned earlier, in groups with 1 year of storage, the minimum µSBS belonged to ZGM1y and ZQM1y which showed only adhesive failure and no mixed or cohesive failures. Also, in 1-year storage groups, the highest frequency of mixed failure and the lowest frequency of adhesive failure belonged to PQL1y group with maximum bond strength.
Table 2. Measures of central dispersion for the µSBS (MPa) in the study groups (n=15)
{kind=link}
Table 3. Comparison of µSBS values (MPa) after 24 hours and 1 year of storage (n=60)
{kind=link}
Table 4. Pairwise comparison of the mean µSBS values (MPa) of the groups with different adhesive application protocols
{kind=link}
Figure 2. Frequency of different failure modes
{kind=link}
Discussion
Direct repair of broken composite restorations is often preferred to their replacement. However, the durability of repaired composite restorations mainly depends on the durability of the composite-composite interface and the bond strength [17]. Aging of composite restorations adversely affects the durability of the bonding interface [17]. Presence of saliva in the oral environment leads to water sorption of the resin matrix, and leakage through the silane-coated filler-matrix interface, resulting in hydrolytic degradation of the restoration, which adversely affects the mechanical properties [27].
This study assessed the effect of composite type (Z250 repair composite bonded to Z350 and Point 4), adhesive type (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instruction, waiting for 30 seconds, or laser irradiation of adhesive prior to its polymerization), and storage time (24 hours versus 1 year) on repair bond strength of composite restorations. The results showed no significant difference between the two universal adhesives and different composite substrates in repair µSBS after 24 hours and 1 year. However, the adhesive application protocol and storage time of the specimens significantly affected the µSBS such that the µSBS was maximum in the laser group followed by waiting for 30 seconds, and all pairwise comparisons in this respect were significant. Also, the µSBS at 24 hours was significantly higher than that after 1 year, irrespective of adhesive type.
With respect to the type of adhesive, evidence shows that application of one layer of adhesive before the composite application can increase the surface wetting and significantly improve the repair bond strength of composite [28]. Universal adhesives are highly favorable for composite repair since their functional monomers and silane can bond to exposed fillers of aged composite made of barium glass or zirconia [29]. Clearfil Universal Bond Quick and G-Premio Universal Bond were used in the present study, which are different in terms of pH, type of solvent, type of monomer, presence/absence of silane, and type of thickener. Nonetheless, no significant difference was noted between the two adhesives in µSBS, but the maximum µSBS was recorded in PQM24h group with Clearfil Universal Bond Quick adhesive. This finding may be attributed to the presence of silane since it is a bifunctional molecule that acts as a bridge, and can form covalent (siloxane) bonds between the inorganic (such as glass filler particles in composite substrate or metal oxides) and organic (such as resin monomers in the repair composite) substrates [17]. Silane needs hydrolysis by water for activation. However, Hooshmand et al. [30] and Yoshihara et al. [31] stated that silane hydrolysis took 24 hours, and it was inactivated after 24 hours. Immediately after hydrolysis, silane may undergo dehydration condensation, form oligomers, and lose its capability for bonding to glass [23]. However, the speed of oligomer formation depends on several factors such as the structure of silane, pH, and type of solvent [32]. According to 3M ESPE’s US Patent 4673354A [33], silane can remain stable in alcohol/water at a pH of 4.6 while the pH of Clearfil Universal Bond Quick is 2.3. Such a low pH can cause dehydration condensation. This explains lack of a significant difference in µSBS between the two universal adhesives in the present study despite the numerically higher value in Clearfil Universal Bond Quick. Also, minimum µSBS was noted in ZGM1y group, treated with G-Premio Bond. According to the results of Papadogiannis et al. [34] this finding may be attributed to the lower degree of conversion of this adhesive due to the interference of several acidic monomers such as 10-MTDP, 4-MET, and MPD and absence of HEMA-2 in its formulation, compared with Clearfil Universal Bond Quick. According to Cuevas-Suárez et al. [9] the efficacy of universal adhesives in the repair process is independent of the presence of silane in their composition, which agrees with the present findings. Also, the present results were in agreement with those of Tsujimoto et al. [35], who found no significant difference in composite-composite SBS in use of G-Premio Bond and Scotchbond Universal after 24 hours and also after 10,000 thermal cycles.
Laser can have several applications in composite repair process. It can be used to remove the superficial degraded parts of the aged composite, and create adequate surface roughness for micromechanical retention, increasing the surface free energy as such [11]. Kiomarsi et al. [10] reported higher repair bond strength of composite in specimens prepared by bur compared with laser. Thus, we only used bur to roughen the specimen surface in this study. Golbari et al. [23] reported that 810 nm diode laser irradiation significantly decreased the microleakage of multi-mode adhesive systems and attributed this finding to the formation of hybrid layer, temperature rise, and solvent evaporation. Maenosono et al. [22] reported enhancement of microtensile bond strength to dentin by irradiation of 970 nm diode laser due to formation of new substrate in dentin and its fusion to adhesive in addition to temperature rise and better evaporation of solvent. The present results indicated that the µSBS in laser group was significantly higher than that in other groups after both 24 hours and 1 year. This finding may be attributed to the heat generated by laser irradiation, which can increase the molecular vibration and cross-linking of resin monomers, increase the degree of conversion, decrease water sorption and solubility, and consequently guarantee the durability of the bond [36]. Also, temperature rise can decrease the adhesive viscosity [37] and increase solvent evaporation and result in higher polymerization reactions [38]. The difference between the 30-second wait and laser groups in the present study may be due to the fact that in 30-second wait group, the solvent vapor pressure decreases with time, while in the laser group, the generated heat compensates for the lower vapor pressure and leads to greater loss of solvent. This is particularly important in universal adhesives with higher water content [39]. In contrast to the present findings, Rezaei-Soufi et al. [40] reported that laser irradiation of 6th generation self-etch primers with 940 nm diode laser before bonding had no significant effect on gingival margin microleakage. Difference between their results and ours may be due to the use of different substrates, bonding agents, and laser wavelengths. Also, Burrer et al. [41] demonstrated that increasing the application time of universal adhesives on dentin had no significant effect on microtensile bond strength. This difference can be due to differences in types of substrates, adhesives, and type of bond strength test.
Two different composite types, namely Point 4 microhybrid and Filtek Z350 XT nanohybrid composites, were used as aged composite substrates in the present study, and were repaired with Z250 composite. The results showed no significant difference in µSBS of the two composite types. However, Point 4 showed numerically higher values irrespective of the type of adhesive at both 24 hours and 1 year, which can be attributed to the composition of these composites and type of monomer, type, size, shape, percentage and distribution of filler particles, and their bonding to resin matrix. One reason explaining the higher µSBS of Point 4 is the higher percentage of inorganic fillers in this composite compared with Z350, because it has been reported that composites with higher filler content have higher resistance to shear loads applied in µSBS test [42]. Also, composites with smaller filler particles such as Z350 have a larger filler-matrix interface and are more susceptible to degradation by oral fluids [43]. Koç-Vural et al. [44] discussed that even the size of filler particles can affect the success of the repair process. These findings explain the higher repair bond strength of the Point 4 microhybrid composite, although it was not statistically significant.
The present results indicated a significant reduction in µSBS at 1 year. However, Kiomarsi et al. [10] found no significant difference in the repair bond strength after 24 hours and after 5000 thermal cycles, which may be due to the different aging protocol employed in their study.
Despite the absence of a significant difference in µSBS of the groups, the maximum numerical value of µSBS was noted in PQL24h group while the minimum value was recorded in ZGM1y group. This finding may be due to the presence of silane in Clearfil Universal Bond Quick, which can bond to filler content of Point 4 composite while G-Premio Bond does not contain silane. Also, Clearfil Universal Bond Quick contains large bis-GMA molecules along with HEMA-2 while G-Premio Bond is devoid of both monomers. Bis-GMA confers strength and stiffness to the polymer network. Also, Clearfil Universal Bond Quick contains hydrophobic aliphatic dimethacrylates, which confer resilience, and increase the efficacy of cross-linking with hydrophobic restorative materials. Higher degree of conversion of Clearfil Universal Bond Quick can also explain the higher bond strength of PQL24h group [45]. Mismatch between the sizes of filler particles of the aged and repair composites and lower weight percentage of filler in Z350 composite can explain the lower bond strength of ZGM1y group.
Failure mode analysis revealed that most adhesive failures belonged to ZGM1y and ZQM1y with minimum bond strength values. This result could be due to the lower inorganic filler percentage of Z350 composite resin, making it susceptible to hydrolytic degradation as a result of smaller size of fillers and larger filler-matrix interface, as well as the inconsistency between the aged and repair composite resins. The 24-hour groups showed the highest frequency of mixed failure, and the 1-year groups showed the highest frequency of adhesive failure, which was in line with the findings of Michelotti et al. [1]. As mentioned earlier, among the 1-year groups, the highest frequency of mixed failure and the lowest frequency of adhesive failure belonged to PQL1y group, which showed the maximum bond strength. This could be the result of coordination between the filler particle size in Point 4 and repair composite resin, higher degree of conversion of Clearfil Universal Bond Quick, and presence of silane in this adhesive resin. Also, all laser groups (with otherwise similar variables) showed lower frequency of adhesive failure, and higher frequency of mixed and cohesive failures. This result was inconsistent with the findings of Kiomarsi et al. [10], who reported higher frequency of adhesive failure in the laser group in comparison with the bur group. This controversy may be due to differences in laser type (Er,Cr:YSGG vs. diode) and their effect on the surface (surface roughening and temperature rise, respectively).
Despite the water storage of the specimens, the clinical setting was not ideally simulated in this in vitro study. Future studies should better simulate the clinical setting by thermal and mechanical cycles to assess the effect of thermal alterations and masticatory forces on repair bond strength of composite restorations. Moreover, future studies are recommended to use other generations of bonding agents with different percentages of solvent to assess the effect of laser on adhesives. Furthermore, the efficacy of diode lasers with different powers should be investigated in further studies.
Conclusion
This study assessed the effect of composite type (Z250 repair composite bonded to Z350 and Point 4), adhesive type (G-Premio Bond and Clearfil Universal Bond Quick), adhesive application protocol (according to the manufacturer’s instruction, waiting for 30 seconds, or laser irradiation of adhesive prior to its polymerization), and storage time (24 hours versus 1 year) on repair bond strength of composite restorations. The results showed no significant difference between the two universal adhesives and different composite substrates in repair µSBS after 24 hours and 1 year. However, the adhesive application protocol and storage time of the specimens significantly affected the µSBS such that the µSBS was maximum in the laser group followed by waiting for 30 seconds, and all pairwise comparisons in this respect were significant. Also, the µSBS at 24 hours was significantly higher than that after 1 year, irrespective of adhesive type.
With respect to the type of adhesive, evidence shows that application of one layer of adhesive before the composite application can increase the surface wetting and significantly improve the repair bond strength of composite [28]. Universal adhesives are highly favorable for composite repair since their functional monomers and silane can bond to exposed fillers of aged composite made of barium glass or zirconia [29]. Clearfil Universal Bond Quick and G-Premio Universal Bond were used in the present study, which are different in terms of pH, type of solvent, type of monomer, presence/absence of silane, and type of thickener. Nonetheless, no significant difference was noted between the two adhesives in µSBS, but the maximum µSBS was recorded in PQM24h group with Clearfil Universal Bond Quick adhesive. This finding may be attributed to the presence of silane since it is a bifunctional molecule that acts as a bridge, and can form covalent (siloxane) bonds between the inorganic (such as glass filler particles in composite substrate or metal oxides) and organic (such as resin monomers in the repair composite) substrates [17]. Silane needs hydrolysis by water for activation. However, Hooshmand et al. [30] and Yoshihara et al. [31] stated that silane hydrolysis took 24 hours, and it was inactivated after 24 hours. Immediately after hydrolysis, silane may undergo dehydration condensation, form oligomers, and lose its capability for bonding to glass [23]. However, the speed of oligomer formation depends on several factors such as the structure of silane, pH, and type of solvent [32]. According to 3M ESPE’s US Patent 4673354A [33], silane can remain stable in alcohol/water at a pH of 4.6 while the pH of Clearfil Universal Bond Quick is 2.3. Such a low pH can cause dehydration condensation. This explains lack of a significant difference in µSBS between the two universal adhesives in the present study despite the numerically higher value in Clearfil Universal Bond Quick. Also, minimum µSBS was noted in ZGM1y group, treated with G-Premio Bond. According to the results of Papadogiannis et al. [34] this finding may be attributed to the lower degree of conversion of this adhesive due to the interference of several acidic monomers such as 10-MTDP, 4-MET, and MPD and absence of HEMA-2 in its formulation, compared with Clearfil Universal Bond Quick. According to Cuevas-Suárez et al. [9] the efficacy of universal adhesives in the repair process is independent of the presence of silane in their composition, which agrees with the present findings. Also, the present results were in agreement with those of Tsujimoto et al. [35], who found no significant difference in composite-composite SBS in use of G-Premio Bond and Scotchbond Universal after 24 hours and also after 10,000 thermal cycles.
Laser can have several applications in composite repair process. It can be used to remove the superficial degraded parts of the aged composite, and create adequate surface roughness for micromechanical retention, increasing the surface free energy as such [11]. Kiomarsi et al. [10] reported higher repair bond strength of composite in specimens prepared by bur compared with laser. Thus, we only used bur to roughen the specimen surface in this study. Golbari et al. [23] reported that 810 nm diode laser irradiation significantly decreased the microleakage of multi-mode adhesive systems and attributed this finding to the formation of hybrid layer, temperature rise, and solvent evaporation. Maenosono et al. [22] reported enhancement of microtensile bond strength to dentin by irradiation of 970 nm diode laser due to formation of new substrate in dentin and its fusion to adhesive in addition to temperature rise and better evaporation of solvent. The present results indicated that the µSBS in laser group was significantly higher than that in other groups after both 24 hours and 1 year. This finding may be attributed to the heat generated by laser irradiation, which can increase the molecular vibration and cross-linking of resin monomers, increase the degree of conversion, decrease water sorption and solubility, and consequently guarantee the durability of the bond [36]. Also, temperature rise can decrease the adhesive viscosity [37] and increase solvent evaporation and result in higher polymerization reactions [38]. The difference between the 30-second wait and laser groups in the present study may be due to the fact that in 30-second wait group, the solvent vapor pressure decreases with time, while in the laser group, the generated heat compensates for the lower vapor pressure and leads to greater loss of solvent. This is particularly important in universal adhesives with higher water content [39]. In contrast to the present findings, Rezaei-Soufi et al. [40] reported that laser irradiation of 6th generation self-etch primers with 940 nm diode laser before bonding had no significant effect on gingival margin microleakage. Difference between their results and ours may be due to the use of different substrates, bonding agents, and laser wavelengths. Also, Burrer et al. [41] demonstrated that increasing the application time of universal adhesives on dentin had no significant effect on microtensile bond strength. This difference can be due to differences in types of substrates, adhesives, and type of bond strength test.
Two different composite types, namely Point 4 microhybrid and Filtek Z350 XT nanohybrid composites, were used as aged composite substrates in the present study, and were repaired with Z250 composite. The results showed no significant difference in µSBS of the two composite types. However, Point 4 showed numerically higher values irrespective of the type of adhesive at both 24 hours and 1 year, which can be attributed to the composition of these composites and type of monomer, type, size, shape, percentage and distribution of filler particles, and their bonding to resin matrix. One reason explaining the higher µSBS of Point 4 is the higher percentage of inorganic fillers in this composite compared with Z350, because it has been reported that composites with higher filler content have higher resistance to shear loads applied in µSBS test [42]. Also, composites with smaller filler particles such as Z350 have a larger filler-matrix interface and are more susceptible to degradation by oral fluids [43]. Koç-Vural et al. [44] discussed that even the size of filler particles can affect the success of the repair process. These findings explain the higher repair bond strength of the Point 4 microhybrid composite, although it was not statistically significant.
The present results indicated a significant reduction in µSBS at 1 year. However, Kiomarsi et al. [10] found no significant difference in the repair bond strength after 24 hours and after 5000 thermal cycles, which may be due to the different aging protocol employed in their study.
Despite the absence of a significant difference in µSBS of the groups, the maximum numerical value of µSBS was noted in PQL24h group while the minimum value was recorded in ZGM1y group. This finding may be due to the presence of silane in Clearfil Universal Bond Quick, which can bond to filler content of Point 4 composite while G-Premio Bond does not contain silane. Also, Clearfil Universal Bond Quick contains large bis-GMA molecules along with HEMA-2 while G-Premio Bond is devoid of both monomers. Bis-GMA confers strength and stiffness to the polymer network. Also, Clearfil Universal Bond Quick contains hydrophobic aliphatic dimethacrylates, which confer resilience, and increase the efficacy of cross-linking with hydrophobic restorative materials. Higher degree of conversion of Clearfil Universal Bond Quick can also explain the higher bond strength of PQL24h group [45]. Mismatch between the sizes of filler particles of the aged and repair composites and lower weight percentage of filler in Z350 composite can explain the lower bond strength of ZGM1y group.
Failure mode analysis revealed that most adhesive failures belonged to ZGM1y and ZQM1y with minimum bond strength values. This result could be due to the lower inorganic filler percentage of Z350 composite resin, making it susceptible to hydrolytic degradation as a result of smaller size of fillers and larger filler-matrix interface, as well as the inconsistency between the aged and repair composite resins. The 24-hour groups showed the highest frequency of mixed failure, and the 1-year groups showed the highest frequency of adhesive failure, which was in line with the findings of Michelotti et al. [1]. As mentioned earlier, among the 1-year groups, the highest frequency of mixed failure and the lowest frequency of adhesive failure belonged to PQL1y group, which showed the maximum bond strength. This could be the result of coordination between the filler particle size in Point 4 and repair composite resin, higher degree of conversion of Clearfil Universal Bond Quick, and presence of silane in this adhesive resin. Also, all laser groups (with otherwise similar variables) showed lower frequency of adhesive failure, and higher frequency of mixed and cohesive failures. This result was inconsistent with the findings of Kiomarsi et al. [10], who reported higher frequency of adhesive failure in the laser group in comparison with the bur group. This controversy may be due to differences in laser type (Er,Cr:YSGG vs. diode) and their effect on the surface (surface roughening and temperature rise, respectively).
Despite the water storage of the specimens, the clinical setting was not ideally simulated in this in vitro study. Future studies should better simulate the clinical setting by thermal and mechanical cycles to assess the effect of thermal alterations and masticatory forces on repair bond strength of composite restorations. Moreover, future studies are recommended to use other generations of bonding agents with different percentages of solvent to assess the effect of laser on adhesives. Furthermore, the efficacy of diode lasers with different powers should be investigated in further studies.
Conclusion
The results demonstrated that in aged composite restoration repair, diode laser irradiation of adhesive prior to polymerization or waiting for 30 seconds before adhesive curing can enhance the µSBS.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Michelotti G, Niedzwiecki M, Bidjan D, Dieckmann P, Deari S, Attin T, Tauböck TT. Silane Effect of Universal Adhesive on the Composite-Composite Repair Bond Strength after Different Surface Pretreatments. Polymers (Basel). 2020 Apr 19;12(4):950. [DOI:10.3390/polym12040950] [PMID] []
2. Martos R, Hegedüs V, Szalóki M, Blum IR, Lynch CD, Hegedüs C. A randomised controlled study on the effects of different surface treatments and adhesive self-etch functional monomers on the immediate repair bond strength and integrity of the repaired resin composite interface. J Dent. 2019 Jun;85:57-63. [DOI:10.1016/j.jdent.2019.04.012] [PMID]
3. Baldissera RA, Corrêa MB, Schuch HS, Collares K, Nascimento GG, Jardim PS, Moraes RR, Opdam NJ, Demarco FF. Are there universal restorative composites for anterior and posterior teeth? J Dent. 2013 Nov;41(11):1027-35. [DOI:10.1016/j.jdent.2013.08.016] [PMID]
4. Demarco FF, Collares K, Coelho-de-Souza FH, Correa MB, Cenci MS, Moraes RR, Opdam NJ. Anterior composite restorations: A systematic review on long-term survival and reasons for failure. Dent Mater. 2015 Oct;31(10):1214-24. [DOI:10.1016/j.dental.2015.07.005] [PMID]
5. Flury S, Dulla FA, Peutzfeldt A. Repair bond strength of resin composite to restorative materials after short- and long-term storage. Dent Mater. 2019 Sep;35(9):1205-13. [DOI:10.1016/j.dental.2019.05.008] [PMID]
6. Kanzow P, Wiegand A, Göstemeyer G, Schwendicke F. Understanding the management and teaching of dental restoration repair: Systematic review and meta-analysis of surveys. J Dent. 2018 Feb;69:1-21. [DOI:10.1016/j.jdent.2017.09.010] [PMID]
7. Kanzow P, Wiegand A, Schwendicke F. Cost-effectiveness of repairing versus replacing composite or amalgam restorations. J Dent. 2016 Nov;54:41-7. [DOI:10.1016/j.jdent.2016.08.008] [PMID]
8. Alizadeh Oskoee P, Savadi Oskoee S, Rikhtegaran S, Pournaghi-Azar F, Gholizadeh S, Aleyasin Y, Kasrae S. Effect of Various Laser Surface Treatments on Repair Shear Bond Strength of Aged Silorane-Based Composite. J Lasers Med Sci. 2017 Fall;8(4):186-90. [DOI:10.15171/jlms.2017.34] [PMID] []
9. Cuevas-Suárez CE, Nakanishi L, Isolan CP, Ribeiro JS, Moreira AG, Piva E. Repair bond strength of bulk-fill resin composite: Effect of different adhesive protocols. Dent Mater J. 2020 Mar 31;39(2):236-41. [DOI:10.4012/dmj.2018-291] [PMID]
10. Kiomarsi N, Espahbodi M, Chiniforush N, Karazifard MJ, Kamangar SSH. In vitro evaluation of repair bond strength of composite: Effect of surface treatments with bur and laser and application of universal adhesive. Laser Ther. 2017 Sep 30;26(3):173-80. [DOI:10.5978/islsm.17-OR-12] [PMID] []
11. Shokripor M, Soufi LR, Ahmadi B, Najafrad E, Mosleh MA. Comparison the Effect of Different Surface Treatments on Shear Bond Strength of Repaired Composite. Avicenna J Dent Res. 2019;11(1):30-36. [DOI:10.34172/ajdr.2019.06]
12. Kanzow P, Wiegand A, Schwendicke F, Göstemeyer G. Same, same, but different? A systematic review of protocols for restoration repair. J Dent. 2019 Jul;86:1-16. [DOI:10.1016/j.jdent.2019.05.021] [PMID]
13. Fawzy AS, El-Askary FS, Amer MA. Effect of surface treatments on the tensile bond strength of repaired water-aged anterior restorative micro-fine hybrid resin composite. J Dent. 2008 Dec;36(12):969-76. [DOI:10.1016/j.jdent.2008.07.014] [PMID]
14. Cavalcanti AN, De Lima AF, Peris AR, Mitsui FH, Marchi GM. Effect of surface treatments and bonding agents on the bond strength of repaired composites. J Esthet Restor Dent. 2007;19(2):90-8; discussion 99. [DOI:10.1111/j.1708-8240.2007.00073.x] [PMID]
15. Nagarkar S, Theis-Mahon N, Perdigão J. Universal dental adhesives: Current status, laboratory testing, and clinical performance. J Biomed Mater Res B Appl Biomater. 2019 Aug;107(6):2121-31. [DOI:10.1002/jbm.b.34305] [PMID]
16. Kuno Y, Hosaka K, Nakajima M, Ikeda M, Klein Junior CA, Foxton RM, Tagami J. Incorporation of a hydrophilic amide monomer into a one-step self-etch adhesive to increase dentin bond strength: Effect of application time. Dent Mater J. 2019 Dec 1;38(6):892-9. [DOI:10.4012/dmj.2018-286] [PMID]
17. Altinci P, Mutluay M, Tezvergil-Mutluay A. Repair bond strength of nanohybrid composite resins with a universal adhesive. Acta Biomater Odontol Scand. 2017 Dec 12;4(1):10-9. [DOI:10.1080/23337931.2017.1412262] [PMID] []
18. Karadas M, Bedir F, Demirbuga S. The role of etching protocols on bond strength of universal adhesives applied to caries affected dentin: a systematic review and meta-analysis. Clin Oral Invest. 2024 Dec;28(12): 683. [DOI:10.1007/s00784-024-06089-0] [PMID]
19. Huang XQ, Pucci CR, Luo T, Breschi L, Pashley DH, Niu LN, Tay FR. No-waiting dentine self-etch concept-Merit or hype. J Dent. 2017 Jul;62:54-63. [DOI:10.1016/j.jdent.2017.05.007] [PMID]
20. Ahmed MH, Yoshihara K, Mercelis B, Van Landuyt K, Peumans M, Van Meerbeek B. Quick bonding using a universal adhesive. Clin Oral Investig. 2020 Aug;24(8):2837-51. [DOI:10.1007/s00784-019-03149-8] [PMID]
21. Sarialioglu GA, Aycan UB. Influence of Etching Mode and Composite Type on Bond Strength to Biodentine Using a "No-Wait" Universal Adhesive. Odovtos-Int J Dent Sc. 2022 Sep-Dec;24(3):36-47.
22. Maenosono RM, Bim Júnior O, Duarte MA, Palma-Dibb RG, Wang L, Ishikiriama SK. Diode laser irradiation increases microtensile bond strength of dentin. Braz Oral Res. 2015; 29:1-5. [DOI:10.1590/1807-3107BOR-2015.vol29.0004]
23. Golbari N, Kasraei S, Afrasiabi A, Mostajir E, Mojahedi SM. Effect of Diode Laser (810 nm) Irradiation on Marginal Microleakage of Multi-mode Adhesive Resins in Class V Composite Restorations. J Lasers Med Sci. 2019 Fall;10(4):275-82. [DOI:10.15171/jlms.2019.45] [PMID] []
24. Malekipour M, Alizadeh F, Shirani F, Amini S. The effect of 808 nm diode laser irradiation on shear bond strength of composite bonded to dentin before and after bonding. Journal of Dental Lasers. 2015 Jul;9(2):69. [DOI:10.4103/0976-2868.158465]
25. Li J. Effects of surface properties on bond strength between layers of newly cured dental composites. J Oral Rehabil. 1997 May;24(5):358-60. [DOI:10.1046/j.1365-2842.1997.00508.x] [PMID]
26. Tezvergil A, Lassila LV, Vallittu PK. Composite-composite repair bond strength: effect of different adhesion primers. J Dent. 2003 Nov;31(8):521-5. [DOI:10.1016/S0300-5712(03)00093-9] [PMID]
27. Tarumi H, Torii M, Tsuchitani Y. Relationship between particle size of barium glass filler and water sorption of light-cured composite resin. Dent Mater J. 1995 Jun;14(1):37-44. [DOI:10.4012/dmj.14.37] [PMID]
28. Brosh T, Pilo R, Bichacho N, Blutstein R. Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. J Prosthet Dent. 1997 Feb;77(2):122-6. [DOI:10.1016/S0022-3913(97)70224-5] [PMID]
29. Tantbirojn D, Fernando C, Versluis A. Failure Strengths of Composite Additions and Repairs. Oper Dent. 2015 Jul-Aug;40(4):364-71. [DOI:10.2341/14-042-L] [PMID]
30. Hooshmand T, van Noort R, Keshvad A. Storage effect of a pre-activated silane on the resin to ceramic bond. Dent Mater. 2004 Sep;20(7):635-42. [DOI:10.1016/j.dental.2003.08.005] [PMID]
31. Yoshihara K, Nagaoka N, Sonoda A, Maruo Y, Makita Y, Okihara T, Irie M, Yoshida Y, Van Meerbeek B. Effectiveness and stability of silane coupling agent incorporated in 'universal' adhesives. Dent Mater. 2016 Oct;32(10):1218-25. [DOI:10.1016/j.dental.2016.07.002] [PMID]
32. Altmann S, Pfeiffer J. The hydrolysis/condensation behaviour of methacryloyloxyalkylfunctional alkoxysilanes: structure-reactivity relations. Monatshefte für Chemie/Chemical Monthly. 2003 Aug;134(8):1081-92. [DOI:10.1007/s00706-003-0615-y]
33. Wu, C-Y., Nakamura K, Miyashita-Kobayashi A, Haruyama A, Yokoi Y, Kuroiwa A, Yoshinari N, Kameyama A. The Effect of Additional Silane Pre-Treatment on the Microtensile Bond Strength of Resin-Based Composite Post-andCore Build-Up Material. Appl. Sci. 2024 Jun-Jul;14(15), 6637. [DOI:10.3390/app14156637]
34. Papadogiannis D, Dimitriadi M, Zafiropoulou M, Gaintantzopoulou MD, Eliades G. Universal Adhesives: Setting Characteristics and Reactivity with Dentin. Materials (Basel). 2019 May 27;12(10):1720. [DOI:10.3390/ma12101720] [PMID] []
35. Tsujimoto A, Barkmeier WW, Takamizawa T, Wilwerding TM, Latta MA, Miyazaki M. Interfacial Characteristics and Bond Durability of Universal Adhesive to Various Substrates. Oper Dent. 2017 Mar/Apr;42(2):E59-E70. [DOI:10.2341/15-353-L] [PMID]
36. Brianezzi LFF, Maenosono RM, Bim O Júnior, Zabeu GS, Palma-Dibb RG, Ishikiriama SK. Does laser diode irradiation improve the degree of conversion of simplified dentin bonding systems? J Appl Oral Sci. 2017 Jul-Aug;25(4):381-6. [DOI:10.1590/1678-7757-2016-0461] [PMID] []
37. Bail M, Malacarne-Zanon J, Silva SM, Anauate-Netto A, Nascimento FD, Amore R, Lewgoy H, Pashley DH, Carrilho MR. Effect of air-drying on the solvent evaporation, degree of conversion and water sorption/solubility of dental adhesive models. J Mater Sci Mater Med. 2012 Mar;23(3):629-38. [DOI:10.1007/s10856-011-4541-y] [PMID]
38. Cho BH, Dickens SH. Effects of the acetone content of single solution dentin bonding agents on the adhesive layer thickness and the microtensile bond strength. Dent Mater. 2004 Feb;20(2):107-15. [DOI:10.1016/S0109-5641(03)00071-X] [PMID]
39. Batista GR, Barcellos DC, Rocha Gomes Torres C, Damião ÁJ, de Oliveira HP, de Paiva Gonçalves SE. Effect of Nd:YAG laser on the solvent evaporation of adhesive systems. Int J Esthet Dent. 2015 Winter;10(4):598-609.
40. Rezaei-Soufi L, Kasraei S, Fekrazad R, Vahdatinia F, Moghim Beigi A, Haddad M, et al. Evaluation of Diode laser (940 nm) irradiation effect on microleakage in class V composite restoration before and after adhesive application .J Dent Mater Tech. 2018 Jul; 7(1): 11-8.
41. Burrer P, Dang H, Par M, Attin T, Tauböck TT. Effect of Over-Etching and Prolonged Application Time of a Universal Adhesive on Dentin Bond Strength. Polymers (Basel). 2020 Dec 3;12(12):2902. [DOI:10.3390/polym12122902] [PMID] []
42. Ribeiro JC, Gomes PN, Moysés MR, Dias SC, Pereira LJ, Ribeiro JG. Shear strength evaluation of composite-composite resin associations. J Dent. 2008 May;36(5):326-30. [DOI:10.1016/j.jdent.2008.01.015] [PMID]
43. Curtis AR, Shortall AC, Marquis PM, Palin WM. Water uptake and strength characteristics of a nanofilled resin-based composite. J Dent. 2008 Mar;36(3):186-93. [DOI:10.1016/j.jdent.2007.11.015] [PMID]
44. Koç-Vural U, Kerimova L, Baltacioglu İH, Kiremitçi A. Bond strength of dental nanocomposites repaired with a bulkfill composite. J Clin Exp Dent. 2017 Mar 1;9(3):e437-42. [DOI:10.4317/jced.53501] [PMID] []
45. Hanabusa M, Yoshihara K, Yoshida Y, Okihara T, Yamamoto T, Momoi Y, Van Meerbeek B. Interference of functional monomers with polymerization efficiency of adhesives. Eur J Oral Sci. 2016 Apr;124(2):204-9. [DOI:10.1111/eos.12245] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |