Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 3 (9-2025)
J Res Dent Maxillofac Sci 2025, 10(3): 248-261 |
Back to browse issues page

Ethics code: IR.SBMU.DRC.REC.1399.019
Clinical trials code: IR.SBMU.DRC.REC.1399.019
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Valian A, Madani T, Kheirkhah Dabbagh N. A Comparative Analysis of Resin-Modified Glass Ionomers and Composite Resins for Restoration of Non-Carious Cervical Lesions: A Systematic Review and Meta-Analysis. J Res Dent Maxillofac Sci 2025; 10 (3) :248-261
URL: http://jrdms.dentaliau.ac.ir/article-1-701-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-701-en.html



1- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Undergraduate Student, Department of Biomedical Engineering, Faculty of Engineering, South Tehran Branch, Islamic Azad University, Tehran, Iran.
3- Department of Restorative Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran. ,Kheirkhahneda.nk@gmail.com
2- Undergraduate Student, Department of Biomedical Engineering, Faculty of Engineering, South Tehran Branch, Islamic Azad University, Tehran, Iran.
3- Department of Restorative Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran. ,
Keywords: Composite Resins, Dental Restoration, Temporary, Glass Ionomer Cements, Evidence-Based Medicine
Full-Text [PDF 693 kb]
(1603 Downloads)
| Abstract (HTML) (4364 Views)
Figure 2. Comparison of primary outcome: retention failure
Table 3. RMGI versus composite restorations for NCCLs
Figure 3. Comparison of secondary outcome: marginal integrity
Figure 4. Comparison of secondary outcome: marginal discoloration
Discussion
Full-Text: (1376 Views)
Abstract
Background and Aim: The objective of this review was to assess the clinical efficacy of resin-modified glass ionomers (RMGIs) and composite resins for management of non-carious cervical lesions (NCCLs).
Materials and Methods: A systematic search was conducted using the Cochrane Oral Health Group Trials Register, MEDLINE via Ovid, EMBASE via Ovid, and PubMed Health, with no restrictions on language up to 2021. The review included randomized controlled trials (RCTs) with a minimum follow-up period of 12 months, comparing RMGI restorations to composite resin restorations in adult populations with NCCLs. The primary outcomes assessed were retention rate, marginal integrity, and marginal discoloration. The search results were rigorously screened, and relevant trial data were extracted. Additionally, the risk of bias for the included studies was evaluated. The results were presented as risk ratios (RRs) with 95% confidence intervals (CIs), and a meta-analysis was performed using Review Manager 5 (RevMan 5).
Results: Of 978 retrieved references, 12 trials (15 articles) were included in this systematic review. Nine trials were split-mouth studies involving 414 RMGI restorations and 454 composite restorations. The remaining three trials were parallel group studies involving 83 RMGI restorations and 131 composite restorations. The meta-analysis showed that RMGI restorations had a significantly lower failure rate (RR: 0.35, 95% CI: 0.23 to 0.52) than composite restorations. However, no significant difference was found between the two materials for marginal integrity and marginal discoloration (P>0.05).
Conclusion: RMGI restorations exhibited superior clinical performance regarding the retention rate for NCCLs.
Keywords: Composite Resins; Dental Restoration, Temporary; Glass Ionomer Cements; Evidence-Based Medicine
Materials and Methods: A systematic search was conducted using the Cochrane Oral Health Group Trials Register, MEDLINE via Ovid, EMBASE via Ovid, and PubMed Health, with no restrictions on language up to 2021. The review included randomized controlled trials (RCTs) with a minimum follow-up period of 12 months, comparing RMGI restorations to composite resin restorations in adult populations with NCCLs. The primary outcomes assessed were retention rate, marginal integrity, and marginal discoloration. The search results were rigorously screened, and relevant trial data were extracted. Additionally, the risk of bias for the included studies was evaluated. The results were presented as risk ratios (RRs) with 95% confidence intervals (CIs), and a meta-analysis was performed using Review Manager 5 (RevMan 5).
Results: Of 978 retrieved references, 12 trials (15 articles) were included in this systematic review. Nine trials were split-mouth studies involving 414 RMGI restorations and 454 composite restorations. The remaining three trials were parallel group studies involving 83 RMGI restorations and 131 composite restorations. The meta-analysis showed that RMGI restorations had a significantly lower failure rate (RR: 0.35, 95% CI: 0.23 to 0.52) than composite restorations. However, no significant difference was found between the two materials for marginal integrity and marginal discoloration (P>0.05).
Conclusion: RMGI restorations exhibited superior clinical performance regarding the retention rate for NCCLs.
Keywords: Composite Resins; Dental Restoration, Temporary; Glass Ionomer Cements; Evidence-Based Medicine
Introduction
Non-carious cervical lesions (NCCLs), also known as cervical wear, involve the loss of dental hard tissue at the cementoenamel junction. NCCLs have become increasingly prevalent, especially as the aging population retains their natural teeth for longer periods of time. The etiology of NCCLs is multifactorial, encompassing abrasion, erosion, and abfraction. These factors contribute to the variability in prevalence and distribution of NCCLs, making it a complex area of study [1-3]. The prevalence of NCCLs varies significantly across different populations and studies, influenced by factors such as age, dietary habits, and lifestyle choices[4-6]. In comparison, other studies reported prevalence rates ranging from as low as 0.8% to as high as 85.7% [2, 5, 6]. A global study indicated an overall prevalence of approximately 46.7% in adults [4]; while a cohort of male footballers exhibited a prevalence of 39.5% [7]. Notably, a Brazilian study reported a remarkably high prevalence of 76.84% among workers exposed to acid mists and chemical products [8]. Furthermore, the prevalence of NCCLs is known to increase with age, as evidenced by a study on Japanese adults, which revealed an overall prevalence of 60.2% that also increased with age [9, 10].
The intraoral distribution of NCCLs is also a controversial topic. Some studies suggested that NCCLs commonly occur on the labial surfaces of maxillary incisors; while, others identified maxillary first molars and premolars as the most affected teeth [11-14]. Conversely, other studies indicated that mandibular molars and premolars are more frequently affected by NCCLs. These discrepancies may arise from the varying classification systems and diagnostic criteria employed across different studies [15, 16]. The etiology of NCCLs involves multiple mechanisms [11, 14]. Abrasion, defined as the mechanical loss of tooth structure, has been linked to excessive tooth brushing, utilization of abrasive toothpastes, and specific oral habits, such as nail biting and pipe smoking [17, 18]. Previous studies have identified these factors as contributors to cervical wear. Although historical evidence often attributed NCCLs primarily to abrasion, it is now acknowledged that abrasion alone is not sufficient to induce cervical wear [17, 19-21].
Erosion, or chemical dissolution of tooth structure due to acids, leads to smooth, round lesions, and is sometimes referred to as "biocorrosion," which encompasses both chemical and biochemical factors. Endogenous acid sources include bacterial plaque, gingival crevicular fluid, and gastric acid from conditions like gastroesophageal reflux disease [19, 22]. Exogenous sources involve dietary acids from citrus fruits, carbonated beverages, and excessive alcohol consumption. The corrosive potential of these substances is influenced by factors such as pH, acid strength (pKa), and buffering capacity. Enamel and dentin have different susceptibility to erosion, with dentin being more affected by proteolytic enzymes and piezoelectric effects [17, 23, 24].
Abfraction is characterized by wedge-shaped lesions caused by biomechanical stresses from occlusal loading or malocclusion. Research has linked bruxism and malocclusion to abfraction lesions, although the theory remains controversial due to limited clinical evidence directly connecting occlusal loading to NCCLs. Stress corrosion, observed in vitro, occurs as a result of a combination of tensile stress and a corrosive environment [25-27]. Studies have shown increased enamel loss under flexural stresses in presence of citric acid and lesions similar to NCCLs in teeth subjected to axial loading and sulfuric acid [28-32]. Despite understanding these mechanisms, the precise contributions of abrasion, erosion, and abfraction to NCCLs and their interactions remain unclear, highlighting the need for further research. The primary aim of this study was to evaluate and compare the clinical performance of resin-modified glass ionomer (RMGI) and composite resin restorations for NCCLs using the modified US Public Health Service (USPHS) criteria. This includes assessing retention rate, esthetics, and other clinical factors to test the null hypothesis that there would be no significant difference in clinical performance of these materials. RMGIs are polymerized through a dual mechanism that includes an acid-base reaction and light polymerization. Research indicates that during the early stages of polymerization, these two mechanisms can compete with each other and inhibit one another, depending on the timing of light activation after mixing the components [33-35].
Specifically, if light activation occurs too soon, it may limit the extent of the acid-base reaction, potentially affecting the material's properties and performance. Thus, RMGIs can be used for treatment of NCCLs through both chemical and photo-polymerization methods. The findings of the present study can guide clinicians in selecting the most appropriate material for managing NCCLs, improving treatment outcomes, patient satisfaction, and overall oral health.
Materials and Methods
The intraoral distribution of NCCLs is also a controversial topic. Some studies suggested that NCCLs commonly occur on the labial surfaces of maxillary incisors; while, others identified maxillary first molars and premolars as the most affected teeth [11-14]. Conversely, other studies indicated that mandibular molars and premolars are more frequently affected by NCCLs. These discrepancies may arise from the varying classification systems and diagnostic criteria employed across different studies [15, 16]. The etiology of NCCLs involves multiple mechanisms [11, 14]. Abrasion, defined as the mechanical loss of tooth structure, has been linked to excessive tooth brushing, utilization of abrasive toothpastes, and specific oral habits, such as nail biting and pipe smoking [17, 18]. Previous studies have identified these factors as contributors to cervical wear. Although historical evidence often attributed NCCLs primarily to abrasion, it is now acknowledged that abrasion alone is not sufficient to induce cervical wear [17, 19-21].
Erosion, or chemical dissolution of tooth structure due to acids, leads to smooth, round lesions, and is sometimes referred to as "biocorrosion," which encompasses both chemical and biochemical factors. Endogenous acid sources include bacterial plaque, gingival crevicular fluid, and gastric acid from conditions like gastroesophageal reflux disease [19, 22]. Exogenous sources involve dietary acids from citrus fruits, carbonated beverages, and excessive alcohol consumption. The corrosive potential of these substances is influenced by factors such as pH, acid strength (pKa), and buffering capacity. Enamel and dentin have different susceptibility to erosion, with dentin being more affected by proteolytic enzymes and piezoelectric effects [17, 23, 24].
Abfraction is characterized by wedge-shaped lesions caused by biomechanical stresses from occlusal loading or malocclusion. Research has linked bruxism and malocclusion to abfraction lesions, although the theory remains controversial due to limited clinical evidence directly connecting occlusal loading to NCCLs. Stress corrosion, observed in vitro, occurs as a result of a combination of tensile stress and a corrosive environment [25-27]. Studies have shown increased enamel loss under flexural stresses in presence of citric acid and lesions similar to NCCLs in teeth subjected to axial loading and sulfuric acid [28-32]. Despite understanding these mechanisms, the precise contributions of abrasion, erosion, and abfraction to NCCLs and their interactions remain unclear, highlighting the need for further research. The primary aim of this study was to evaluate and compare the clinical performance of resin-modified glass ionomer (RMGI) and composite resin restorations for NCCLs using the modified US Public Health Service (USPHS) criteria. This includes assessing retention rate, esthetics, and other clinical factors to test the null hypothesis that there would be no significant difference in clinical performance of these materials. RMGIs are polymerized through a dual mechanism that includes an acid-base reaction and light polymerization. Research indicates that during the early stages of polymerization, these two mechanisms can compete with each other and inhibit one another, depending on the timing of light activation after mixing the components [33-35].
Specifically, if light activation occurs too soon, it may limit the extent of the acid-base reaction, potentially affecting the material's properties and performance. Thus, RMGIs can be used for treatment of NCCLs through both chemical and photo-polymerization methods. The findings of the present study can guide clinicians in selecting the most appropriate material for managing NCCLs, improving treatment outcomes, patient satisfaction, and overall oral health.
Materials and Methods
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [36].
Eligibility criteria:
The eligibility criteria for this review were specifically defined to ensure the inclusion of relevant studies. Randomized controlled trials (RCTs) that compared RMGI restorations with composite resin restorations in treatment of NCCLs were included. Both parallel group and split-mouth study designs were considered, provided that they had a minimum follow-up period of 12 months. Studies had to use the modified USPHS criteria for assessing the clinical performance of restorations. Exclusions were made for studies involving children with NCCLs, treatment of carious cervical lesions, use of mechanical retention, follow-up periods shorter than 12 months, and cases where restorations were not placed according to the manufacturer’s instructions.
Information source and search strategy:
To identify relevant studies, a comprehensive search strategy was developed and applied across several electronic databases. The primary database searched was MEDLINE via OVID, with search terms such as "resin-modified glass ionomer", "composite resin", "non-carious cervical lesions", and "RCT". This search strategy incorporated the Cochrane Highly Sensitive Search Strategy for RCTs and was adapted to other databases, including EMBASE, using terms like "glass ionomer restorations", "composite restorations", and "cervical lesions". Additional search was conducted in PubMed Central, the US National Institutes of Health Trials Register, and the WHO International Clinical Trials Registry Platform. Reference lists of the included papers were also reviewed, and hand search was performed in journals like the British Dental Journal and Dental Materials. All searches were updated through 2021.
Selection process and data extraction:
The selection process involved screening of titles and abstracts of all retrieved articles to identify studies meeting the inclusion criteria. Full-texts of potentially relevant studies were then obtained and thoroughly assessed. A data extraction form was designed to capture detailed information from each study, including publication details, trial methods, participant characteristics, intervention details, and outcome measures. The key data extracted included the first author and year of publication, trial methodology details (e.g., sequence generation, allocation concealment), participant demographics, types of restorations used, and results related to retention, marginal integrity, and discoloration.
Risk of bias assessment:
The risk of bias of the included studies was evaluated using six specific domains outlined in the Cochrane Handbook for Systematic Reviews of Interventions [16,37].
Results
Eligibility criteria:
The eligibility criteria for this review were specifically defined to ensure the inclusion of relevant studies. Randomized controlled trials (RCTs) that compared RMGI restorations with composite resin restorations in treatment of NCCLs were included. Both parallel group and split-mouth study designs were considered, provided that they had a minimum follow-up period of 12 months. Studies had to use the modified USPHS criteria for assessing the clinical performance of restorations. Exclusions were made for studies involving children with NCCLs, treatment of carious cervical lesions, use of mechanical retention, follow-up periods shorter than 12 months, and cases where restorations were not placed according to the manufacturer’s instructions.
Information source and search strategy:
To identify relevant studies, a comprehensive search strategy was developed and applied across several electronic databases. The primary database searched was MEDLINE via OVID, with search terms such as "resin-modified glass ionomer", "composite resin", "non-carious cervical lesions", and "RCT". This search strategy incorporated the Cochrane Highly Sensitive Search Strategy for RCTs and was adapted to other databases, including EMBASE, using terms like "glass ionomer restorations", "composite restorations", and "cervical lesions". Additional search was conducted in PubMed Central, the US National Institutes of Health Trials Register, and the WHO International Clinical Trials Registry Platform. Reference lists of the included papers were also reviewed, and hand search was performed in journals like the British Dental Journal and Dental Materials. All searches were updated through 2021.
Selection process and data extraction:
The selection process involved screening of titles and abstracts of all retrieved articles to identify studies meeting the inclusion criteria. Full-texts of potentially relevant studies were then obtained and thoroughly assessed. A data extraction form was designed to capture detailed information from each study, including publication details, trial methods, participant characteristics, intervention details, and outcome measures. The key data extracted included the first author and year of publication, trial methodology details (e.g., sequence generation, allocation concealment), participant demographics, types of restorations used, and results related to retention, marginal integrity, and discoloration.
Risk of bias assessment:
The risk of bias of the included studies was evaluated using six specific domains outlined in the Cochrane Handbook for Systematic Reviews of Interventions [16,37].
Results
Included studies:
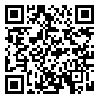
In total, 12 studies were included in this review [38-49]. All the studies were in English. The earliest and most recent studies had been published in 1998 and 2021, respectively. The characteristics of the included studies are presented in Table 1.
Participants:
Across the 12 included studies, 361 adult participants (one study did not report the number of patients) and 1,643 restorations were evaluated. The age of the participants in the included studies ranged from 18 to 92 years. All the studies reported the age range of the participants; however, only five studies provided the mean age of the participants [38, 39, 44, 46, 48]. All the patients had NCCLs.
Setting and design:
The studies had been conducted in Nigeria [38], Mexico [39], Brazil [40, 45, 46, 48], Germany [41], Turkey [42, 43] Sweden [44], India [47], and Romania [49]. From the 12 included studies, 9 studies had a split-mouth design [38-40, 43, 45-49] and 3 had a parallel-group design [41, 42, 44].
The observation period across the studies ranged from 1 to 7 years. Five studies had a follow-up of one year [38, 41, 45, 47, 48], 3 had a two-year follow-up [39, 42, 49], 3 had a three-year follow-up [43, 44, 46] and one had a follow-up of 7 years [40].
In all studies except 4 [2,7,16,43], the restorations were placed by one single clinician/operator. The studies by Federlin et al, [41] and Hussainy et al. [47] did not provide any information on the number of operator(s). In all the included studies except for 2 [47, 49], at least two examiners assessed the restorations at the follow-up periods. One study [47] had only one investigator and another one [49] did not provide any information about the number of evaluators. In the included trials, RMGI and composite resin were used as the restorative materials. Three studies [41, 42, 47] also investigated the clinical effectiveness of poly-acid modified composite resins (compomers). The data on compomer restorations and modifications of RMGI and composite resins were not reported in this review.
Four studies compared RMGI with three-step etch-and-rinse adhesive systems [42-45], and 7 studies compared RMGI with two-step etch-and-rinse adhesive systems [38-41, 47-49]. The study by van Dijken [44] used both two-step and three-step etch-and-rinse systems in comparison with RMGI. Only one study compared RMGI with universal adhesive systems [46].
In the majority of the studies, the cervical lesions were cleaned with pumice and water prior to placement of restoration. In terms of clinical technique, 2 studies employed rubber dam isolation [38, 40] and the remainder used a combination of retraction cord, cotton wool rolls, and suction. Only 2 studies reported enamel beveling [43, 45] when placing the restoration and 2 studies reported dentin preparation by bur roughening [42-44].
In total, 12 studies were included in this review [38-49]. All the studies were in English. The earliest and most recent studies had been published in 1998 and 2021, respectively. The characteristics of the included studies are presented in Table 1.
Participants:
Across the 12 included studies, 361 adult participants (one study did not report the number of patients) and 1,643 restorations were evaluated. The age of the participants in the included studies ranged from 18 to 92 years. All the studies reported the age range of the participants; however, only five studies provided the mean age of the participants [38, 39, 44, 46, 48]. All the patients had NCCLs.
Setting and design:
The studies had been conducted in Nigeria [38], Mexico [39], Brazil [40, 45, 46, 48], Germany [41], Turkey [42, 43] Sweden [44], India [47], and Romania [49]. From the 12 included studies, 9 studies had a split-mouth design [38-40, 43, 45-49] and 3 had a parallel-group design [41, 42, 44].
The observation period across the studies ranged from 1 to 7 years. Five studies had a follow-up of one year [38, 41, 45, 47, 48], 3 had a two-year follow-up [39, 42, 49], 3 had a three-year follow-up [43, 44, 46] and one had a follow-up of 7 years [40].
In all studies except 4 [2,7,16,43], the restorations were placed by one single clinician/operator. The studies by Federlin et al, [41] and Hussainy et al. [47] did not provide any information on the number of operator(s). In all the included studies except for 2 [47, 49], at least two examiners assessed the restorations at the follow-up periods. One study [47] had only one investigator and another one [49] did not provide any information about the number of evaluators. In the included trials, RMGI and composite resin were used as the restorative materials. Three studies [41, 42, 47] also investigated the clinical effectiveness of poly-acid modified composite resins (compomers). The data on compomer restorations and modifications of RMGI and composite resins were not reported in this review.
Four studies compared RMGI with three-step etch-and-rinse adhesive systems [42-45], and 7 studies compared RMGI with two-step etch-and-rinse adhesive systems [38-41, 47-49]. The study by van Dijken [44] used both two-step and three-step etch-and-rinse systems in comparison with RMGI. Only one study compared RMGI with universal adhesive systems [46].
In the majority of the studies, the cervical lesions were cleaned with pumice and water prior to placement of restoration. In terms of clinical technique, 2 studies employed rubber dam isolation [38, 40] and the remainder used a combination of retraction cord, cotton wool rolls, and suction. Only 2 studies reported enamel beveling [43, 45] when placing the restoration and 2 studies reported dentin preparation by bur roughening [42-44].
{kind=link}
Outcome measures:
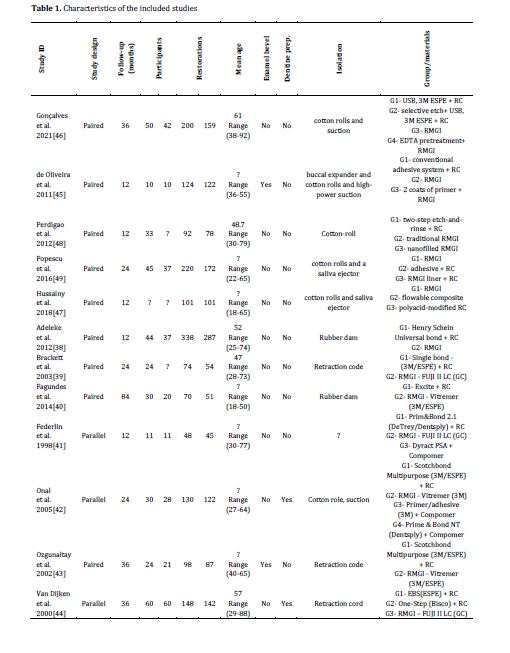
All the studies reported using the modified USPHS criteria for clinical evaluation of dental restorative materials. The principal outcome was retention. This parameter was reported in all the included studies in one or more of the following formats: retention rates (percentage of retained restorations), number of failed restorations, or cumulative survival rate. The secondary outcomes (i.e. marginal discoloration and marginal integrity) were measured and presented as either “clinically acceptable” or “clinically unacceptable” based on the modified USPHS scores. The retention rate and percentage of “clinically acceptable” restorations in terms of marginal discoloration and marginal integrity for all the study groups are summarized in Table 2.
The retention rate of NCCL restorations varied depending on the type of adhesive system and the follow-up period of the study. For a follow-up period of 1-3 years, the retention rate ranged from 51% to 100% with a mean retention rate of 91.5%. Only the study by Fagundes et al. [40] had a follow-up period of more than 3 years. The reported survival rate for the two-step etch-and-rinse adhesive and RMGI was 52% and 88.5%, respectively at a recall period of 7 years.
The poorest clinical performance in terms of retention rate was found for a 2-step etch-and-rinse adhesive with 51% clinically acceptable restorations at 3 years. On a further note, the 2-step etch-and-rinse system had the lowest reported marginal integrity, with 51% clinically acceptable restorations at 3 years.
Risk of bias of the included studies:
Randomization:
The sequence generation process was considered as having a low risk of bias in only 3 studies [38, 40, 47] while others were unclear about the details of their randomization process. Fagundes et al. [40] reported a sequentially numbered randomization process; while, Adeleke and Oginni [38] stated simple random sampling by using ballots. Moreover, Hussainy et al. [47] performed randomization using a block randomization procedure with unknown block sizes to the investigators until the end of the study.
Allocation:
The method used to conceal the allocation sequence was only reported in 2 studies [16,37] and hence other studies were judged as having an unclear risk of selection bias. Hussainy et al. [47] and Goncalves et al. [46] implemented the sealed envelope method for allocation concealment.
Blinding of participants and personnel:
All the studies were judged as having a high risk of performance bias due to the type of interventions performed since blinding of the operators was not feasible. No information on blinding of the participants was provided by the studies; however, the outcomes were unlikely to be influenced by inadequate patient blinding.
Blinding of outcome assessors:
Seven studies were considered to have a low risk of bias as the outcome assessors were independent of the operators [38-40, 42, 46-48].
Incomplete outcome data:
The attrition bias was considered as being at low risk of bias in 8 of the included studies [38-40, 42, 44-47]. This was due to sufficient information on the number and reasons of participant drop-outs at recall periods.
Selective reporting:
All 12 studies reported their pre-specified outcomes and therefore the studies were judged as having low risk of reporting bias.
Other potential sources of bias:
None of the studies had clearly indicated whether the effect of clustering was taken into account to avoid unit of analysis error; thus, this domain was judged to have unclear risk of bias.
Summary of risk of bias assessment:
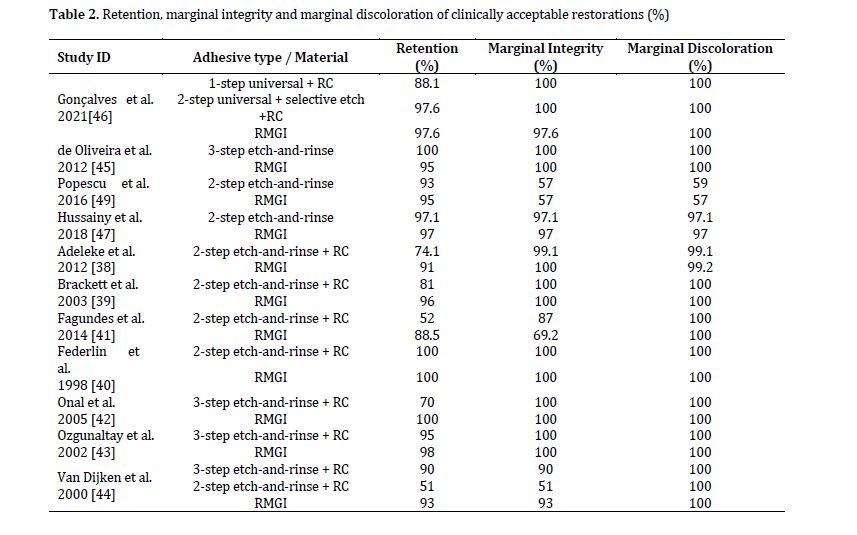
All the included studies were judged to have unclear risk of bias (plausible bias that raises some doubt about results) as one or more of the domains were graded as unclear (Figure 1).
All the studies reported using the modified USPHS criteria for clinical evaluation of dental restorative materials. The principal outcome was retention. This parameter was reported in all the included studies in one or more of the following formats: retention rates (percentage of retained restorations), number of failed restorations, or cumulative survival rate. The secondary outcomes (i.e. marginal discoloration and marginal integrity) were measured and presented as either “clinically acceptable” or “clinically unacceptable” based on the modified USPHS scores. The retention rate and percentage of “clinically acceptable” restorations in terms of marginal discoloration and marginal integrity for all the study groups are summarized in Table 2.
The retention rate of NCCL restorations varied depending on the type of adhesive system and the follow-up period of the study. For a follow-up period of 1-3 years, the retention rate ranged from 51% to 100% with a mean retention rate of 91.5%. Only the study by Fagundes et al. [40] had a follow-up period of more than 3 years. The reported survival rate for the two-step etch-and-rinse adhesive and RMGI was 52% and 88.5%, respectively at a recall period of 7 years.
The poorest clinical performance in terms of retention rate was found for a 2-step etch-and-rinse adhesive with 51% clinically acceptable restorations at 3 years. On a further note, the 2-step etch-and-rinse system had the lowest reported marginal integrity, with 51% clinically acceptable restorations at 3 years.
Risk of bias of the included studies:
Randomization:
The sequence generation process was considered as having a low risk of bias in only 3 studies [38, 40, 47] while others were unclear about the details of their randomization process. Fagundes et al. [40] reported a sequentially numbered randomization process; while, Adeleke and Oginni [38] stated simple random sampling by using ballots. Moreover, Hussainy et al. [47] performed randomization using a block randomization procedure with unknown block sizes to the investigators until the end of the study.
Allocation:
The method used to conceal the allocation sequence was only reported in 2 studies [16,37] and hence other studies were judged as having an unclear risk of selection bias. Hussainy et al. [47] and Goncalves et al. [46] implemented the sealed envelope method for allocation concealment.
Blinding of participants and personnel:
All the studies were judged as having a high risk of performance bias due to the type of interventions performed since blinding of the operators was not feasible. No information on blinding of the participants was provided by the studies; however, the outcomes were unlikely to be influenced by inadequate patient blinding.
Blinding of outcome assessors:
Seven studies were considered to have a low risk of bias as the outcome assessors were independent of the operators [38-40, 42, 46-48].
Incomplete outcome data:
The attrition bias was considered as being at low risk of bias in 8 of the included studies [38-40, 42, 44-47]. This was due to sufficient information on the number and reasons of participant drop-outs at recall periods.
Selective reporting:
All 12 studies reported their pre-specified outcomes and therefore the studies were judged as having low risk of reporting bias.
Other potential sources of bias:
None of the studies had clearly indicated whether the effect of clustering was taken into account to avoid unit of analysis error; thus, this domain was judged to have unclear risk of bias.
Summary of risk of bias assessment:
All the included studies were judged to have unclear risk of bias (plausible bias that raises some doubt about results) as one or more of the domains were graded as unclear (Figure 1).
{kind=link}
Figure 1. Summary of risk of bias of the included studies
Effects of interventions:
The longest follow-up of each study was selected for inclusion in the meta-analysis. One study [48] just reported the alpha percentage while alpha+ bravo indicated the success rate in other included studies. Therefore, it was not included in the meta-analysis. Table 2 shows a summary of the studies included in the meta-analyses.
Primary outcome: retention rate
The pooled estimate of the parallel group studies (83 RMGI and 131 composite restorations) showed that RMGI restorations had a significantly lower risk of retention failure than composite restorations [risk ratio (RR): 0.20, 95% CI: 0.07 to 0.56, P=0.002; random-effect model)] (Figure 2 and Table 3). There was no evidence of heterogeneity (P=0.44; I²=0%).
A subgroup meta-analysis of the split-mouth studies (414 RMGI and 454 composite restorations) also indicated that RMGI restorations had significantly lower failure rates than composite restorations (RR: 0.38, 95% CI: 0.24 to 0.60, P<0.00; random-effects model). There was no evidence of heterogeneity (P=0.62; I²=0%) (Table 3).
There was no difference in the outcome derived from the split-mouth and parallel-group studies. The results of the combined subgroup meta-analysis confirmed reduced risk of retention failures (i.e. a significantly higher survival rate) for RMGI compared to composite (RR: 0.35, 95% CI: 0.23 to 0.52, P<0.000; random-effects model) in cervical lesions. There was no evidence of heterogeneity (P=0.61; I²=0%) (Table 3).
Secondary outcome: marginal integrity
Meta-analysis of the parallel group studies (83 RMGI and 125 composite restorations) showed that RMGI restorations had a significantly superior marginal integrity than composite restorations (RR: 0.23, 95% CI: 0.07 to 0.72, P=0.01; fixed-effects model) (Figure 3 and Table 3).
The outcome data from the split-mouth studies (224 RMGI and 181 composite restorations) showed a borderline statistical significance for marginal integrity (RR: 0.97, 95% CI: 0.64 to 1.45, P=0.87; fixed-effects model). There was no evidence of heterogeneity (P=0.61; I² = 0%) (Figure 3 and Table 3).
The results of combined subgroup meta-analysis of split-mouth and parallel group studies showed borderline statistical significance in favor of RMGI for marginal integrity in comparison with composite (RR: 0.70; 95% CI: 0.47 to 1.03; P=0.07; fixed-effects model) with no evidence of heterogeneity (P=0.12; I²=0%) (Figure 3 and Table 3).
Secondary outcome: marginal discoloration
The meta-analysis found no statistically significant difference between RMGI and composite restorations with regard to marginal discoloration (RR: 0.00; 95% CI: -0.02 to 0.03; P=0.92) (Figure 4).
{kind=link}
Effects of interventions:
The longest follow-up of each study was selected for inclusion in the meta-analysis. One study [48] just reported the alpha percentage while alpha+ bravo indicated the success rate in other included studies. Therefore, it was not included in the meta-analysis. Table 2 shows a summary of the studies included in the meta-analyses.
Primary outcome: retention rate
The pooled estimate of the parallel group studies (83 RMGI and 131 composite restorations) showed that RMGI restorations had a significantly lower risk of retention failure than composite restorations [risk ratio (RR): 0.20, 95% CI: 0.07 to 0.56, P=0.002; random-effect model)] (Figure 2 and Table 3). There was no evidence of heterogeneity (P=0.44; I²=0%).
A subgroup meta-analysis of the split-mouth studies (414 RMGI and 454 composite restorations) also indicated that RMGI restorations had significantly lower failure rates than composite restorations (RR: 0.38, 95% CI: 0.24 to 0.60, P<0.00; random-effects model). There was no evidence of heterogeneity (P=0.62; I²=0%) (Table 3).
There was no difference in the outcome derived from the split-mouth and parallel-group studies. The results of the combined subgroup meta-analysis confirmed reduced risk of retention failures (i.e. a significantly higher survival rate) for RMGI compared to composite (RR: 0.35, 95% CI: 0.23 to 0.52, P<0.000; random-effects model) in cervical lesions. There was no evidence of heterogeneity (P=0.61; I²=0%) (Table 3).
Secondary outcome: marginal integrity
Meta-analysis of the parallel group studies (83 RMGI and 125 composite restorations) showed that RMGI restorations had a significantly superior marginal integrity than composite restorations (RR: 0.23, 95% CI: 0.07 to 0.72, P=0.01; fixed-effects model) (Figure 3 and Table 3).
The outcome data from the split-mouth studies (224 RMGI and 181 composite restorations) showed a borderline statistical significance for marginal integrity (RR: 0.97, 95% CI: 0.64 to 1.45, P=0.87; fixed-effects model). There was no evidence of heterogeneity (P=0.61; I² = 0%) (Figure 3 and Table 3).
The results of combined subgroup meta-analysis of split-mouth and parallel group studies showed borderline statistical significance in favor of RMGI for marginal integrity in comparison with composite (RR: 0.70; 95% CI: 0.47 to 1.03; P=0.07; fixed-effects model) with no evidence of heterogeneity (P=0.12; I²=0%) (Figure 3 and Table 3).
Secondary outcome: marginal discoloration
The meta-analysis found no statistically significant difference between RMGI and composite restorations with regard to marginal discoloration (RR: 0.00; 95% CI: -0.02 to 0.03; P=0.92) (Figure 4).
Figure 2. Comparison of primary outcome: retention failure
Table 3. RMGI versus composite restorations for NCCLs
Figure 3. Comparison of secondary outcome: marginal integrity
Figure 4. Comparison of secondary outcome: marginal discoloration
Discussion
Twelve clinical trials reporting outcome data on retention rate, marginal integrity, and marginal discoloration were identified and deemed appropriate for this review. All the included studies were assessed as having an unclear risk of bias. The results of the meta-analysis showed that RMGI restorations exhibited significantly superior performance than composite restorations with respect to retention rate. However, no significant differences were found between the two materials for marginal integrity and marginal discoloration. In addition, no difference between the outcomes of parallel group and split-mouth studies was observed in retention rate and marginal discoloration but in assessment of marginal integrity, the parallel group studies showed a significant difference between RMGI and composite resin restorations; while, in split-mouth studies, no significant difference was observed.
Overall completeness and applicability of evidence
The 12 included studies were RCTs that compared RMGI restorations with composite resin restorations for NCCLs. The follow-up period ranged from 1 and 7 years. The outcome results on the retention rate, marginal integrity, and marginal discoloration were reported based on the modified USPHS criteria.
The overall body of evidence from the 12 included RCTs was not of sufficient quality. All the included studies used restoration rather than patient as the unit of analysis. It was also unclear whether the effect of clustering had been taken into account for sample size calculations and statistical analysis. Failure to account for clustering creates a ‘unit of analysis error’ which underestimates the required sample size, produces over-precise results and P values that are too small [50-54].
Blinding of clinicians was not possible in these studies due to the nature of interventions and the fact that specific adhesive protocols had to be followed during the restorative phase. However, lack of clinician or patient blinding was not considered as a potential source of bias.
Agreements and disagreements with prior research:
The findings of this review supported the results of previous systematic reviews and studies. Santos et al. [55] found significantly lower risk of loss of RMGI restorations compared to composite restorations including both the three-step etch-and-rinse and the two-step etch-and-rinse adhesive systems in class V lesions. Matis et al. [56] reported significantly better retention rates for glass ionomer compared to composite after 10 years. In another study by Peumans et al. [57], glass ionomer restorations revealed superior bonding performance and lower annual failure rate compared to five other classes of adhesive materials (three-step etch-rinse, two-step etch-rinse, two step self-etch, one-step self-etch and self-adhesive composites) in class V lesions. RMGI restorations offer several advantages over traditional composite restorations, especially in specific clinical situations. One of the main benefits of RMGIs is their enhanced bond strength. They chemically bond to dentin, and the bond strength improves over time, leading to reduced microleakage compared to composites, which can suffer from polymerization shrinkage and subsequent debonding [58, 59]. This property makes RMGIs a reliable option for long-term restorations.
Another significant advantage of RMGIs is their ability to continuously release fluoride ions. This fluoride release is essential for prevention of secondary caries, as it inhibits bacterial proliferation and promotes the remineralization of tooth structure. This characteristic is particularly beneficial in pediatric dentistry and for patients at high risk of caries, providing an extra layer of protection for vulnerable teeth. RMGIs also feature a dual-cure property, utilizing both chemical and light curing mechanisms. This dual-cure capability allows for a faster setting while ensuring strong initial strength. Additionally, it reduces moisture sensitivity during the setting process, addressing a common issue faced by traditional glass ionomer cements, which can be compromised when exposed to saliva or blood during placement [51, 58]. In terms of mechanical properties, RMGIs exhibit higher flexural strength, improved wear resistance, and lower solubility compared to the conventional glass ionomer cements. These features make RMGIs more suitable for areas subjected to occlusal forces, as they are less brittle than traditional composites and can better withstand stresses in the oral environment. Esthetically, RMGIs excel in comparison to conventional glass ionomer cements. They provide improved esthetic qualities that approach those of composites while retaining their advantageous properties. This makes RMGIs an excellent choice for visible areas in the oral cavity, where esthetics is crucial. Furthermore, RMGIs demonstrate versatility in application, effectively used across various techniques, such as serving as a base for composite restorations in the "sandwich technique." This enhances their utility in complex restorative procedures that may require multiple materials. Finally, clinical studies have shown that RMGI restorations generally have lower annual failure rate compared to composite restorations, indicating superior long-term performance. These advantages position RMGIs as a valuable option in restorative dentistry, especially for specific indications such as Class V lesions and for patients at increased risk of caries [60].
Conclusion
Overall completeness and applicability of evidence
The 12 included studies were RCTs that compared RMGI restorations with composite resin restorations for NCCLs. The follow-up period ranged from 1 and 7 years. The outcome results on the retention rate, marginal integrity, and marginal discoloration were reported based on the modified USPHS criteria.
The overall body of evidence from the 12 included RCTs was not of sufficient quality. All the included studies used restoration rather than patient as the unit of analysis. It was also unclear whether the effect of clustering had been taken into account for sample size calculations and statistical analysis. Failure to account for clustering creates a ‘unit of analysis error’ which underestimates the required sample size, produces over-precise results and P values that are too small [50-54].
Blinding of clinicians was not possible in these studies due to the nature of interventions and the fact that specific adhesive protocols had to be followed during the restorative phase. However, lack of clinician or patient blinding was not considered as a potential source of bias.
Agreements and disagreements with prior research:
The findings of this review supported the results of previous systematic reviews and studies. Santos et al. [55] found significantly lower risk of loss of RMGI restorations compared to composite restorations including both the three-step etch-and-rinse and the two-step etch-and-rinse adhesive systems in class V lesions. Matis et al. [56] reported significantly better retention rates for glass ionomer compared to composite after 10 years. In another study by Peumans et al. [57], glass ionomer restorations revealed superior bonding performance and lower annual failure rate compared to five other classes of adhesive materials (three-step etch-rinse, two-step etch-rinse, two step self-etch, one-step self-etch and self-adhesive composites) in class V lesions. RMGI restorations offer several advantages over traditional composite restorations, especially in specific clinical situations. One of the main benefits of RMGIs is their enhanced bond strength. They chemically bond to dentin, and the bond strength improves over time, leading to reduced microleakage compared to composites, which can suffer from polymerization shrinkage and subsequent debonding [58, 59]. This property makes RMGIs a reliable option for long-term restorations.
Another significant advantage of RMGIs is their ability to continuously release fluoride ions. This fluoride release is essential for prevention of secondary caries, as it inhibits bacterial proliferation and promotes the remineralization of tooth structure. This characteristic is particularly beneficial in pediatric dentistry and for patients at high risk of caries, providing an extra layer of protection for vulnerable teeth. RMGIs also feature a dual-cure property, utilizing both chemical and light curing mechanisms. This dual-cure capability allows for a faster setting while ensuring strong initial strength. Additionally, it reduces moisture sensitivity during the setting process, addressing a common issue faced by traditional glass ionomer cements, which can be compromised when exposed to saliva or blood during placement [51, 58]. In terms of mechanical properties, RMGIs exhibit higher flexural strength, improved wear resistance, and lower solubility compared to the conventional glass ionomer cements. These features make RMGIs more suitable for areas subjected to occlusal forces, as they are less brittle than traditional composites and can better withstand stresses in the oral environment. Esthetically, RMGIs excel in comparison to conventional glass ionomer cements. They provide improved esthetic qualities that approach those of composites while retaining their advantageous properties. This makes RMGIs an excellent choice for visible areas in the oral cavity, where esthetics is crucial. Furthermore, RMGIs demonstrate versatility in application, effectively used across various techniques, such as serving as a base for composite restorations in the "sandwich technique." This enhances their utility in complex restorative procedures that may require multiple materials. Finally, clinical studies have shown that RMGI restorations generally have lower annual failure rate compared to composite restorations, indicating superior long-term performance. These advantages position RMGIs as a valuable option in restorative dentistry, especially for specific indications such as Class V lesions and for patients at increased risk of caries [60].
Conclusion
This review revealed that RMGI restorations exhibited superior clinical performance in terms of retention rate compared to composite resin restorations in NCCLs. Furthermore, no difference was found between the two materials in terms of marginal discoloration or marginal integrity. All the trials were rated as having unclear risk of bias, and therefore the findings of this review should be interpreted with caution.
In addition, the quality of the included studies was not of high standard. Most of the studies exhibited fundamental weaknesses in their study design, methodology, data reporting, and analysis. It is therefore essential to conduct well-designed, high-quality studies with long follow-up periods to unravel the uncertainties in the results of previous studies. In addition, further clinical studies are necessary to compare the clinical performance of various adhesive systems and determine the effect of enamel beveling and dentin roughening on the performance of cervical restorations.
In addition, the quality of the included studies was not of high standard. Most of the studies exhibited fundamental weaknesses in their study design, methodology, data reporting, and analysis. It is therefore essential to conduct well-designed, high-quality studies with long follow-up periods to unravel the uncertainties in the results of previous studies. In addition, further clinical studies are necessary to compare the clinical performance of various adhesive systems and determine the effect of enamel beveling and dentin roughening on the performance of cervical restorations.
Type of Study: Review article |
Subject:
Restorative Dentistry
References
1. Kikly A, Jaâfoura S, Bouslema A, Garouachi E, Belghuith AC. Non-Carious Cervical Lesions: From Diagnosis to Treatment. Ameri J Clin Med Re: AJCMR. 2024;116.
2. Villamayor KGG, Codas-Duarte D, Ramirez I, Souza-Gabriel AE, Sousa-Neto MD, Candemil AP. Morphological characteristics of non-carious cervical lesions. A systematic review. Arch Oral Biol. 2024 Nov;167:106050. [DOI:10.1016/j.archoralbio.2024.106050] [PMID]
3. Goodacre CJ, Eugene Roberts W, Munoz CA. Noncarious cervical lesions: Morphology and progression, prevalence, etiology, pathophysiology, and clinical guidelines for restoration. J Prosthodont. 2023 Feb;32(2):e1-e18. [DOI:10.1111/jopr.13585]
4. Gomes RR, Zeola LF, Barbosa TAQ, Fernandes Neto AJ, de Araujo Almeida G, Soares PV. Prevalence of non-carious cervical lesions and orthodontic treatment: a retrospective study. Prog Orthod. 2022 May 16;23(1):17. [DOI:10.1186/s40510-022-00409-4] [PMID] []
5. Intaraprasong N, Banomyong D, Chotvorrarak K, Ngoenwiwatkul Y, Pittayachawan P. Influence of Different Post-endodontic Restorations on the Survival Rate Against Fracture of Endodontically Treated Anterior Teeth Affected by Cervical Lesions with Pulpal Involvement: A Retrospective Clinical Study. Eur Endod J. 2024 Jan 1;9(1):44-56. [DOI:10.14744/eej.2023.15870] [PMID] []
6. Zakirulla M, Alhaydan AY, Alqahtani MS, Abdullah SM, Alkhammash SM, Ulhaqban HA, Alqahtani HS, Alshehri Y, Alharbi MM, Alharbi RM, Al Moadi RA. Prevalence and Characteristics of Non-Carious Cervical Lesions in Abha City, Saudi Arabia. Bahrain Med Bull. 2024 Mar 1;46(1).
7. Medeiros TLM, Mutran SCAN, Espinosa DG, do Carmo Freitas Faial K, Pinheiro HHC, D'Almeida Couto RS. Prevalence and risk indicators of non-carious cervical lesions in male footballers. BMC Oral Health. 2020 Jul 29;20(1):215. [DOI:10.1186/s12903-020-01200-9] [PMID] []
8. Bomfim RA, Crosato E, Mazzilli LE, Frias AC. Prevalence and risk factors of non-carious cervical lesions related to occupational exposure to acid mists. Braz Oral Res. 2015;29:S1806-83242015000100280. [DOI:10.1590/1807-3107BOR-2015.vol29.0085] [PMID]
9. Kitasako Y, Ikeda M, Takagaki T, Burrow MF, Tagami J. The prevalence of non-carious cervical lesions (NCCLs) with or without erosive etiological factors among adults of different ages in Tokyo. Clin Oral Investig. 2021 Dec;25(12):6939-47. [DOI:10.1007/s00784-021-03984-8] [PMID]
10. Salas MM, Nascimento GG, Huysmans MC, Demarco FF. Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis. J. Dent . 2015;43(1):42-50. [DOI:10.1016/j.jdent.2014.10.012] [PMID]
11. Arafa A, Filfilan SS, Fansa HA. Erosive effect of beverages on surface hardness and ultra-structure of deciduous teeth enamel. Pediatric Dental Journal. 2022 Dec 1;32(3):186-92. [DOI:10.1016/j.pdj.2022.08.001]
12. Sognnaes RF, Wolcott RB, Xhonga FA. Dental erosion. I. Erosion-like patterns occurring in association with other dental conditions. J Am Dent Assoc. 1972 Mar;84(3):571-6. [DOI:10.14219/jada.archive.1972.0116] [PMID]
13. Duangthip D, Man A, Poon PH, Lo ECM, Chu CH. Occlusal stress is involved in the formation of non-carious cervical lesions. A systematic review of abfraction. Am J Dent. 2017 Aug;30(4):212-20.
14. Rees J, Hammadeh M, Jagger D. Abfraction lesion formation in maxillary incisors, canines and premolars: a finite element study. Eur. J Oral Sci. 2003;111(2):149-54. [DOI:10.1034/j.1600-0722.2003.00018.x] [PMID]
15. Poiate IAVP, Muramatsu M, Mori M, Campos TT, Matsuda K, Lopez MAPA, et al. Abfraction lesion in central incisor tooth: Displacement and stress evaluation by laser speckle and finite element analysis. Med Res Arch. 2023;11(8). [DOI:10.18103/mra.v11i8.4220]
16. Goradia Y, Gouasmi S, Reffas SA. Influence of Mechanical Properties of Dental Implants on Biomechanical Behavior: A Three-Dimensional Finite Element Analysis. J Biomim. 2024 Apr 15;64:39-54. [DOI:10.4028/p-g22CO2]
17. Grippo JO, Simring M, Schreiner S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. J Am Dent Assoc. 2004;135(8):1109-18. [DOI:10.14219/jada.archive.2004.0369] [PMID]
18. Singh TK, Johnson AJ, Gupta A, Gill I. Novel 3-dimensional classification of cervical abrasion using CBCT: A comprehensive analysis. J Oral Biol. Craniofac. Res. 2024;14(5):638-44. [DOI:10.1016/j.jobcr.2024.08.007] [PMID] []
19. Karan K, Yao X, Xu C, Wang Y. Chemical profile of the dentin substrate in non-carious cervical lesions. J Dent. Mater. 2009;25(10):1205-12. [DOI:10.1016/j.dental.2009.04.006] [PMID] []
20. Gutierrez B, Goyes H, Perez J, Arango M. Non-carious Cervical Lesions, an Approach of the Associated Factors in a Teaching Service Clinic. 2024. [DOI:10.21203/rs.3.rs-4688481/v1]
21. Kong W, Ma H, Qiao F, Xiao M, Wang L, Zhou L, et al. Risk factors for noncarious cervical lesions: A case-control study. J Oral Rehabil. 2024;51(9):1684-91. [DOI:10.1111/joor.13772] [PMID]
22. Mehta SB, Banerji S, Millar BJ, Suarez-Feito J-M. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012;212(4):169-77. [DOI:10.1038/sj.bdj.2012.137] [PMID]
23. Grippo JO, Simring M, Coleman TA. Abfraction, abrasion, biocorrosion, and the enigma of noncarious cervical lesions: a 20‐year perspective. J Esthet Restor Dent. 2012;24(1):10-23. [DOI:10.1111/j.1708-8240.2011.00487.x] [PMID]
24. Özgöz M, Arabaci T, Sümbüllü MA, Demir T. Relationship between handedness and toothbrush-related cervical dental abrasion in left-and right-handed individuals. J Dent Sci. 2010;5(4):177-82. [DOI:10.1016/j.jds.2010.11.001]
25. Badavannavar AN, Ajari S, Nayak KUS, Khijmatgar S. Abfraction: Etiopathogenesis, clinical aspect, and diagnostic-treatment modalities: A review. Indian J Dent Res. 2020 Mar-Apr;31(2):305-11. [DOI:10.4103/ijdr.IJDR_863_18] [PMID]
26. Nascimento MM, Dilbone DA, Pereira PN, Duarte WR, Geraldeli S, Delgado AJ. Abfraction lesions: etiology, diagnosis, and treatment options. Clin Cosmet Investig Dent. 2016 May 3;8:79-87. [DOI:10.2147/CCIDE.S63465] [PMID] []
27. Roberts WE, Mangum JE, Schneider PM. Pathophysiology of Demineralization, Part I: Attrition, Erosion, Abfraction, and Noncarious Cervical Lesions. Curr Osteoporos Rep. 2022 Feb;20(1):90-105. [DOI:10.1007/s11914-022-00722-1] [PMID] []
28. Costăchel BC, Bechir A, Burcea A, Mihai LL, Ionescu T, Marcu OA, Bechir ES. Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study. Clin Pract. 2023 Aug 26;13(5):1043-58. [DOI:10.3390/clinpract13050093] [PMID] []
29. Costăchel BC, Bechir A, Târcolea M, Mihai LL, Burcea A, Bechir ES. The Stresses and Deformations in the Abfraction Lesions of the Lower Premolars Studied by the Finite Element Analyses: Case Report and Review of Literature. Diagnostics (Basel). 2024 Apr 9;14(8):788. [DOI:10.3390/diagnostics14080788] [PMID] []
30. Duangthip D, Man A, Poon PH, Lo ECM, Chu CH. Occlusal stress is involved in the formation of non-carious cervical lesions. A systematic review of abfraction. Am J Dent. 2017 Aug;30(4):212-20.
31. Haskell B, Stern JK, Ghiassi J, Kurialacherry A, Gaud-Quintana S, Peacock ME. Resolution of Abfraction-Associated Gingival Fenestration Utilizing Connective Tissue Grafting. Case Rep Dent. 2019 Jun 12;2019:6810670. [DOI:10.1155/2019/6810670] [PMID] []
32. Jakupović S, Šehić A, Julardžija F, Gavranović-Glamoč A, Sofić A, Bajsman A, Kazazić L. The Influence of Different Occlusal Loading on Six Restorative Materials for Restoration of Abfraction Lesions-Finite Element Analysis. Eur J Dent. 2022 Oct;16(4):886-94. [DOI:10.1055/s-0041-1741376] [PMID] []
33. Berzins DW, Abey S, Costache MC, Wilkie CA, Roberts HW. Resin-modified glass-ionomer setting reaction competition. J Dent Res. 2010 Jan;89(1):82-6. [DOI:10.1177/0022034509355919] [PMID] []
34. Roberts HW, Berzins DW. Early reaction kinetics of contemporary glass-ionomer restorative materials. J Adhes Dent. 2015 Feb;17(1):67-75.
35. Thomas JT, Roberts HW, Diaz L, Bradley TG, Berzins DW. Effect of light-cure initiation time on polymerization efficiency and orthodontic bond strength with a resin-modified glass-ionomer. Orthod Craniofac Res. 2012 May;15(2):124-34. [DOI:10.1111/j.1601-6343.2011.01531.x] [PMID]
36. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. [DOI:10.1136/bmj.n71] [PMID] []
37. Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: The Cochrane Collaboration and John Wiley & Sons Ltd; 2008. [DOI:10.1002/9780470712184]
38. Adeleke, Oginni A. Clinical evaluation of resin composite and resin-modified glass ionomer cement in non-carious cervical lesions. J West Afr Coll Surg. 2012 Oct;2(4):21-37.
39. Brackett WW, Dib A, Brackett MG, Reyes AA, Estrada BE. Two-year clinical performance of Class V resin-modified glass-lonomer and resin composite restorations. Oper Dent. 2003 Sep-Oct;28(5):477-81.
40. Fagundes TC, Barata TJ, Bresciani E, Santiago S, Franco EB, Lauris JR, et al. Seven-year clinical performance of resin composite versus resin-modified glass ionomer restorations in noncarious cervical lesions. Oper Dent. 2014 Nov-Dec;39(6):578-87. [DOI:10.2341/13-054-C] [PMID]
41. Federlin M, Thonemann B, Schmalz G, Urlinger T. Clinical evaluation of different adhesive systems for restoring teeth with erosion lesions. Clin Oral Investig. 1998 Jun;2(2):58-66. [DOI:10.1007/s007840050046] [PMID]
42. Onal B, Pamir T. The two-year clinical performance of esthetic restorative materials in noncarious cervical lesions. J Am Dent Assoc. 2005 Nov;136(11):1547-55. [DOI:10.14219/jada.archive.2005.0085] [PMID]
43. Ozgünaltay G, Onen A. Three-year clinical evaluation of a resin modified glass-ionomer cement and a composite resin in non-carious class V lesions. J Oral Rehabil. 2002 Nov;29(11):1037-41. [DOI:10.1046/j.1365-2842.2002.00995.x] [PMID]
44. van Dijken JW. Clinical evaluation of three adhesive systems in class V non-carious lesions. Dent Mater. 2000 Jul;16(4):285-91. [DOI:10.1016/S0109-5641(00)00019-1] [PMID]
45. de Oliveira FG, Machado LS, Rocha EP, de Alexandre RS, Briso AL, Mazza ML, Sundfeld RH. Clinical evaluation of a composite resin and a resin modified glass ionomer cement in non-carious cervical lesions: one-year results. IJCD. 2012 Sep 18;5:1-1.
46. Gonçalves DFM, Shinohara MS, Carvalho PRMA, Ramos FSES, Oliveira LC, Omoto ÉM, et al. Three-year evaluation of different adhesion strategies in non-carious cervical lesion restorations: a randomized clinical trial. J Appl Oral Sci. 2021 Oct 22;29:e20210192 [DOI:10.1590/1678-7757-2021-0192] [PMID] []
47. Hussainy SN, Nasim I, Thomas T, Ranjan M. Clinical performance of resin-modified glass ionomer cement, flowable composite, and polyacid-modified resin composite in noncarious cervical lesions: One-year follow-up. J Conserv Dent. 2018 Sep-Oct;21(5):510-5. [DOI:10.4103/JCD.JCD_51_18] [PMID] []
48. Perdigão J, Dutra-Corrêa M, Saraceni SH, Ciaramicoli MT, Kiyan VH. Randomized clinical trial of two resin-modified glass ionomer materials: 1-year results. Oper Dent. 2012 Nov-Dec;37(6):591-601. [DOI:10.2341/11-415-C] [PMID]
49. Popescu SM, Ţuculină MJ, Manolea HO, Mercuţ R, Scrieciu M. Randomized clinical trial of adhesive restorations in non carious cervical lesions. Key Engineering Materials. 2016 Jun 30;695:3-11. [DOI:10.4028/www.scientific.net/KEM.695.3]
50. Litaker MS, Gordan VV, Rindal DB, Fellows JL, Gilbert GH; National Dental PBRN Collaborative Group. Cluster Effects in a National Dental PBRN restorative study. J Dent Res. 2013 Sep;92(9):782-7. [DOI:10.1177/0022034513497752] [PMID] []
51. Boku GG, Garoma Abeya S, Ayers N, Abera Wordofa M. The Effect of School-Linked Module-Based Friendly-Health Education on Adolescents' Sexual and Reproductive Health Knowledge, Guji Zone, Ethiopia - Cluster Randomized Controlled Trial. Adolesc Health Med Ther. 2024 Jan 23;15:5-18 [DOI:10.2147/AHMT.S441957] [PMID] []
52. Chen J, Zhou X, Li F, Spiegelman D. swdpwr: A SAS macro and an R package for power calculations in stepped wedge cluster randomized trials. Comput Methods Programs Biomed. 2022 Jan;213:106522. [DOI:10.1016/j.cmpb.2021.106522] [PMID] []
53. Kennedy-Shaffer L, Hughes MD. Power and sample size calculations for cluster randomized trials with binary outcomes when intracluster correlation coefficients vary by treatment arm. Clin Trials. 2022 Feb;19(1):42-51. [DOI:10.1177/17407745211059845] [PMID] []
54. Crider K, Williams J, Qi YP, Gutman J, Yeung L, Mai C, et al. Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas. Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. [DOI:10.1002/14651858.CD014217] [PMID] []
55. 55 Santos MJ, Ari N, Steele S, Costella J, Banting D. Retention of tooth-colored restorations in non-carious cervical lesions--a systematic review. Clin Oral Investig. 2014;18(5):1369-81. [DOI:10.1007/s00784-014-1220-7] [PMID]
56. Matis BA, Cochran M, Carlson T. Longevity of glass-ionomer restorative materials: results of a 10-year evaluation. Quintessence Int. 1996 Jun;27(6):373-82.
57. Peumans M, De Munck J, Mine A, Van Meerbeek B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater. 2014 Oct;30(10):1089-103. [DOI:10.1016/j.dental.2014.07.007] [PMID]
58. Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, Luján-Valencia SA, Meza-Málaga JM, Aguirre-Ipenza R, et al. Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis. Dent J (Basel). 2024 May 24;12(6):158. [DOI:10.3390/dj12060158] [PMID] []
59. Ferraresso LFOT, Küster I, Besegato JF, Pfau EA, Hoeppner MG. Multidisciplinary management of a tooth with severe root dilaceration and enamel hypoplasia: a case report. Gen Dent. 2023 Sep-Oct;71(5):64-69.
60. V S R, Prabha J L, Priscilla Antony S D. Assessment of Occlusal Load Strength of Glass Ionomer Cement and Composite in Class V Cavities: An In-Vitro Study. Cureus. 2023 Nov 27;15(11):e49529.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |