Journal of Research in Dental
and Maxillofacial Sciences
Volume 3, Issue 4 (10-2018)
J Res Dent Maxillofac Sci 2018, 3(4): 26-32 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jalalian S, Emami Arjomand M, Mahavi A. Comparative Evaluation of Fracture Strength of Cusp Coverage with Composite Versus Unsupported Enamel Reinforced with Composite in Posterior Dental Restorations. J Res Dent Maxillofac Sci 2018; 3 (4) :26-32
URL: http://jrdms.dentaliau.ac.ir/article-1-215-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-215-en.html



1- Assistant professor, Restorative Dept, faculty of Dentistry,Islamic Azad University of Medical Sciences, Tehran, Iran. , shahariar.jalalian@yahoo.com
2- Restorative Dept,faculty of Dentistry
3- Dentist
2- Restorative Dept,faculty of Dentistry
3- Dentist
Full-Text [PDF 274 kb]
(2345 Downloads)
| Abstract (HTML) (5238 Views)
Abstract
Background and aim: Efficient bonding techniques should be employed for strengthening tooth structure. Whether to preserve intact dental tissue or to sacrifice some undermined parts can still be challenging. We aimed to evaluate the fracture strength of cusp coverage with composite versus unsupported enamel reinforced with composite in posterior restorations.
Materials and methods: In this in-vitro study, over-impressions were made from 36 sound human maxillary premolars using bleaching shields. The teeth were randomly divided into three groups (n=12): group 1) intact teeth, group 2) teeth with MOD cavities without cusp coverage, and group 3) teeth with MOD cavities and 1.5 mm of buccal and palatal cusp coverage. Wide MOD cavities were prepared such that only 1 mm of intact enamel was left unsupported at margins. The cavities were restored using light-cure glass ionomer and P60 composite using the over-impressions to achieve the normal tooth anatomy. The teeth were stored in water at 37°C for a week, and their fracture resistance was assessed using a universal testing machine. The load at fracture was recorded in Newton (N). Data were analyzed using one-way analysis of variance (ANOVA) and Tukey’s test with a 95% confidence interval (CI).
Results: The mean±standard deviation (SD) of fracture load was 1834.62±104.04 N in group 1, 750.34±147.46 N in group 2, and 1211.30±210.85 N in group 3. One-way ANOVA revealed significant differences between the groups (P=0.001). Likewise, Tukey’s test showed that the difference between the groups was statistically significant (P<0.05).
Conclusion: Using composite in restoring unsupported enamel must be combined with cusp coverage to increase fracture strength.
Keywords: Composite Resins, Fracture Strengths, Onlays
Introduction
Premolars are more likely than molars to be subjected to lateral forces of more detrimental nature; therefore, fracture is a concern, particularly in maxillary premolars because their anatomy somehow eases separation of the cusps during mastication. (1,2) Fractures in unsupported tooth structure, especially after MOD restorations, can lead to replacement of the restoration and even extraction if the tooth is unrestorable. (3,4)
Cavity preparation design and the type of restorative material are among the important items influencing the fracture resistance of restored teeth. (5,6) The fracture mainly occurs when the marginal ridge is thin or totally removed. (7)
Numerous studies have revealed the importance of residual dental structure in increasing fracture strength. Generally, the wider the involvement by caries or cavity preparations, the weaker the teeth. (8,9)
Despite the successful use of amalgam in crown-root restorations and build-ups after root canal treatments in posterior teeth, new dental materials such as composite resins offer many advantages over amalgam, and because of their more appealing appearance, they have higher general acceptance. (9) In addition, resin composites with good bonding ability transmit and distribute functional stresses and have the potential to reinforce weakened dental structures. (10) Moreover, resin composites show good clinical survival rates (90% after two years and 55.1%-89.7% after 10 years), even when they are used for restoration of extensive cavities in posterior teeth. (11,12) In large cavities, cusp coverage with direct or indirect composite restoration seems to be a safe approach. (13,14) This procedure takes the restoration margins to the axial surfaces and protects the adhesive interface from early marginal misfits under loading. (13) In the past, cavity preparation the same as conventional cavity preparation for amalgam was suggested for posterior composite restorations, but nowadays, researchers have suggested a more conservative approach, and because the retention is provided through the bonding to the tooth, cavity preparation becomes easier and shallower and with less tooth structure removal. (15)
The most important issue in operative dentistry is to adhere to conservative principles. Restoring carious lesions or small dental defects with composite is more conservative compared to restoration with amalgam. (16,17) Therefore, it has always been a question that whether we can keep the intact but unsupported enamel to maintain aesthetics in addition to having sufficient strength against occlusal forces.
Numerous surveys have been conducted in this field with some successful results. (18-24). However, some failures in the reinforcement of weakened dental tissue with composite bonding have also been observed.
This study is a comparative evaluation of the fracture strength of cusp coverage with composite resin versus unsupported enamel reinforced with composite resin in posterior dental restorations.
Materials and Methods
This in-vitro experimental study was performed on 36 intact maxillary premolars without caries or visible fracture lines that had been extracted for orthodontic purposes. (13)
The teeth were disinfected in 0.5% chloramine-T solution and were kept in this solution at room temperature till the beginning of the experiment. The teeth were almost the same in mesiodistal and buccolingual widths (with a 0.5-mm error rate) as measured by a digital caliper (GUANGLU, Alberta, Canada). Teeth surfaces were debrided by scaling hand instruments and were polished with a rubber cup and pumice paste.
Then, the teeth were randomly divided into three groups of 12 specimens each:
Group 1) intact teeth,
Group 2) teeth with MOD cavities without cusp reduction,
Group 3) teeth with MOD cavities with cusp reduction.
Before cavity preparation, an over-impression was made for all teeth using bleaching shields (Easy-Vac Gasket, Korea) and a vacuum machine (Easy-Vac Gasket, Korea). (25) The impressions were cut 1mm below the cementoenamel junction (CEJ) as a reference for reconstruction of margins and coronal structure. Using this method, the teeth were reconstructed according to their baseline size and morphology.
Cavity preparation:
An MOD cavity was prepared using a high-speed handpiece with cooling air and water system using a 1.0-mm diameter cylindrical bur (Diaswiss, Geneva, Switzerland). A new bur was used after every five cavity preparations.
The characteristics of the cavity were as follows:
The buccolingual width of the cavity: the cavity was prepared such that only 1 mm of enamel remained intact at margins. In order to ensure the absence of dentin at margins, we used both visual examination and measurement with the digital caliper. We placed sliding jaws of the caliper against marginal walls and opened it slightly to match and fit the shape, then, turned the lock screw; the value we measured was approximately 1 mm in all marginal wall length. As the width was not more than 1 mm, we could assure that there was no dentin left.
Pulpal depth from the cavosurface: 3 mm
The dimensions of proximal boxes were as follows:
Gingival floor width: the gingival floor of the cavity was prepared such that only 1 mm of enamel remained intact in buccal and lingual walls.
Gingival floor depth: 1 mm above the CEJ (Figure 1-A).
The same cavity preparation process was followed for the next group in addition to 2 mm cusp reduction for lingual and 1.5 mm cusp reduction for buccal enamel walls in order to strengthen unsupported enamel walls in both functional and non-functional cusps (Figure 1-B).
Afterwards, a thin layer (1 mm) of light-cure glass ionomer cement (GC Fuji II LC, Tokyo, Japan) was applied to the whole gingival floor of the cavity as stress breaker and light cured with energy density of 600 mW/cm2 (Astralis 7, Ivoclar Vivadent, Lichtenstein, Switzerland) for 40 seconds. Then, the specimens were etched with 37% phosphoric acid (MORVABON, Tehran, Iran) for 15 seconds. The process was followed by rinsing with water for 10 seconds and air-drying using air spray. Then, Single Bond (3M ESPE, St Paul, MN, USA) was applied to the cavity floor and to the inner surface of dental walls and was dried for three seconds. The second layer of bonding was applied and light cured for 20 seconds using the light-curing unit. Filtek P60 composite resin (3M ESPE, St Paul, MN, USA) was applied to the cavity in 2-mm-thick increments and cured for 40 seconds. The final increment was cured along with the bleaching shield over-impression to contour the restoration the same as an intact tooth.
Testing procedure:
After one week of storage in normal saline, the specimens were mounted in cubic-shaped acrylic resin in order to be put in a universal testing machine (Zwick-Roell, Ulm, Germany).
The specimens were subjected to a compressive force at a crosshead speed of 1 mm/minute. The force was applied by an 8-mm-diameter round metal bar positioned parallel to the long axes of the teeth, in contact with the occlusal slopes of the buccal and lingual cusps (Figure 2). The peak fracture load was recorded in Newton (N) for each tooth. Data were analyzed using one-way analysis of variance (ANOVA) and Tukey’s test with a 95% confidence interval (CI).
Figure 1. (A) Gingival floor depth is 1 mm above the cementoenamel junction (CEJ). (B) Two mm cusp reduction for lingual and 1.5 mm cusp reduction for buccal enamel walls.
Figure 2. The force was applied by an 8-mm-diameter round metal bar positioned parallel to the long axes of the teeth, in contact with the occlusal slopes of the buccal and lingual cusps.
Results
In the present study, the use of overlay direct resin composite provided 66% of the fracture resistance of sound teeth according to the following formula (Table 1):
Table 1. The mean±standard deviation (SD) of fracture load (N) in the studied groups
The mean±standard deviation (SD) of fracture load was 1834.62±104.04 N in group 1 (intact teeth), 750.34±147.46 N in group 2 (no cusp coverage), and 1211.30±210.85 N in group 3 (buccal and palatal cusp coverage; Table1).
One-way ANOVA revealed significant differences between all three groups (P=0.001).
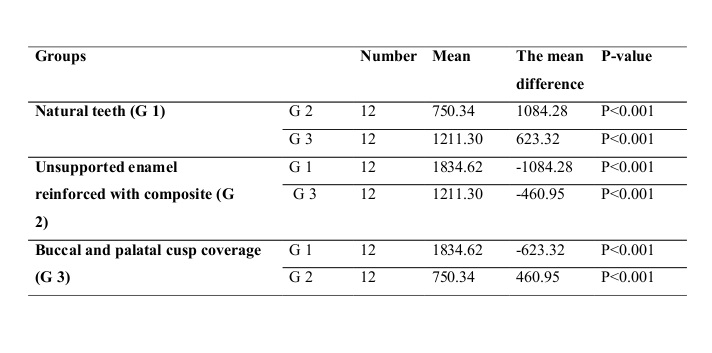
Tukey’s test was used for pairwise comparisons and showed that the difference between the three groups was statistically significant (P=0.001; Table 2). Group 1 had the highest fracture strength in comparison with the other groups, and the fracture strength of group 3 was higher than that of group 2 that had the lowest fracture strength.
Table 2. Comparison of the studied groups according to Tukey’s test
Discussion
Nowadays, one of the most important issues discussed in operative dentistry is the ability to maintain and strengthen weakened tooth structure and to adhere to conservative principles. Amalgam does not have the ability to strengthen weakened enamel structures, and cusp coverage is more recommended in non-bonded restorations than in bonded ones. (17,21) Because of the role of enamel in aesthetics and as anterior teeth are not under severe occlusal forces, unsupported weakened enamel is preserved in these teeth. (22) The question is whether it is possible to prevent removing unsupported enamel walls due to the bond of resin materials to the dental structure in posterior teeth as well and whether composite resin can strengthen unsupported enamel in such teeth to avoid or postpone fractures.
Sometimes, due to various reasons, the resistance is decreased to the level that the tooth is no longer able to tolerate masticatory loads or even smaller forces. (23) Fracture resistance of teeth is influenced by several factors, of which, some are controllable and some are not. These factors include high compressive forces, unfavorable occlusal contacts in the centric occlusion, restorative problems, steep cusps, caries, etc. (24)
In the present study, it has been shown that the fracture resistance of MOD restorations could be more improved by direct composite full coverage design compared to inlay composite restoration, which was in agreement with the results reported by Mondelli et al, Panahandeh and Johar, and Soares et al, (13,25,26) but still was significantly lower than that of intact teeth. The results of the present study do not agree with those of previous studies that reported the fracture resistance of weakened teeth restored with resin composite without cusp coverage to be similar to that of sound teeth; (5,18,20,27-29) this is probably due to the cavity size evaluated in the present study, which was larger than those examined in the mentioned studies.
Some other researchers have stated that cusp coverage may decrease the fracture resistance of teeth. In the mentioned studies, similar cavities were prepared in teeth, and specimens were evaluated in terms of cusp coverage. (30,31) This difference can be explained by the fact that in the mentioned studies, a large volume (two-thirds) of the occlusogingival cusp was removed for coverage, and fracture resistance decreased due to significant tooth reduction (and not because of cusp coverage).
Our study results did not confirm this finding and showed that cusp coverage increases the fracture resistance of teeth; this can be explained as follows:
The overall results of our study showed that using composite resin in restoring teeth with unsupported enamel walls must be combined with cusp coverage in order to increase the fracture strength of such teeth. Cusp coverage in premolars reinforces the remaining tooth structure and significantly increases the fracture strength of these teeth; even if a fracture occurs, it is going to be less severe.
Full-Text: (2443 Views)
Abstract
Background and aim: Efficient bonding techniques should be employed for strengthening tooth structure. Whether to preserve intact dental tissue or to sacrifice some undermined parts can still be challenging. We aimed to evaluate the fracture strength of cusp coverage with composite versus unsupported enamel reinforced with composite in posterior restorations.
Materials and methods: In this in-vitro study, over-impressions were made from 36 sound human maxillary premolars using bleaching shields. The teeth were randomly divided into three groups (n=12): group 1) intact teeth, group 2) teeth with MOD cavities without cusp coverage, and group 3) teeth with MOD cavities and 1.5 mm of buccal and palatal cusp coverage. Wide MOD cavities were prepared such that only 1 mm of intact enamel was left unsupported at margins. The cavities were restored using light-cure glass ionomer and P60 composite using the over-impressions to achieve the normal tooth anatomy. The teeth were stored in water at 37°C for a week, and their fracture resistance was assessed using a universal testing machine. The load at fracture was recorded in Newton (N). Data were analyzed using one-way analysis of variance (ANOVA) and Tukey’s test with a 95% confidence interval (CI).
Results: The mean±standard deviation (SD) of fracture load was 1834.62±104.04 N in group 1, 750.34±147.46 N in group 2, and 1211.30±210.85 N in group 3. One-way ANOVA revealed significant differences between the groups (P=0.001). Likewise, Tukey’s test showed that the difference between the groups was statistically significant (P<0.05).
Conclusion: Using composite in restoring unsupported enamel must be combined with cusp coverage to increase fracture strength.
Keywords: Composite Resins, Fracture Strengths, Onlays
Introduction
Premolars are more likely than molars to be subjected to lateral forces of more detrimental nature; therefore, fracture is a concern, particularly in maxillary premolars because their anatomy somehow eases separation of the cusps during mastication. (1,2) Fractures in unsupported tooth structure, especially after MOD restorations, can lead to replacement of the restoration and even extraction if the tooth is unrestorable. (3,4)
Cavity preparation design and the type of restorative material are among the important items influencing the fracture resistance of restored teeth. (5,6) The fracture mainly occurs when the marginal ridge is thin or totally removed. (7)
Numerous studies have revealed the importance of residual dental structure in increasing fracture strength. Generally, the wider the involvement by caries or cavity preparations, the weaker the teeth. (8,9)
Despite the successful use of amalgam in crown-root restorations and build-ups after root canal treatments in posterior teeth, new dental materials such as composite resins offer many advantages over amalgam, and because of their more appealing appearance, they have higher general acceptance. (9) In addition, resin composites with good bonding ability transmit and distribute functional stresses and have the potential to reinforce weakened dental structures. (10) Moreover, resin composites show good clinical survival rates (90% after two years and 55.1%-89.7% after 10 years), even when they are used for restoration of extensive cavities in posterior teeth. (11,12) In large cavities, cusp coverage with direct or indirect composite restoration seems to be a safe approach. (13,14) This procedure takes the restoration margins to the axial surfaces and protects the adhesive interface from early marginal misfits under loading. (13) In the past, cavity preparation the same as conventional cavity preparation for amalgam was suggested for posterior composite restorations, but nowadays, researchers have suggested a more conservative approach, and because the retention is provided through the bonding to the tooth, cavity preparation becomes easier and shallower and with less tooth structure removal. (15)
The most important issue in operative dentistry is to adhere to conservative principles. Restoring carious lesions or small dental defects with composite is more conservative compared to restoration with amalgam. (16,17) Therefore, it has always been a question that whether we can keep the intact but unsupported enamel to maintain aesthetics in addition to having sufficient strength against occlusal forces.
Numerous surveys have been conducted in this field with some successful results. (18-24). However, some failures in the reinforcement of weakened dental tissue with composite bonding have also been observed.
This study is a comparative evaluation of the fracture strength of cusp coverage with composite resin versus unsupported enamel reinforced with composite resin in posterior dental restorations.
Materials and Methods
This in-vitro experimental study was performed on 36 intact maxillary premolars without caries or visible fracture lines that had been extracted for orthodontic purposes. (13)
The teeth were disinfected in 0.5% chloramine-T solution and were kept in this solution at room temperature till the beginning of the experiment. The teeth were almost the same in mesiodistal and buccolingual widths (with a 0.5-mm error rate) as measured by a digital caliper (GUANGLU, Alberta, Canada). Teeth surfaces were debrided by scaling hand instruments and were polished with a rubber cup and pumice paste.
Then, the teeth were randomly divided into three groups of 12 specimens each:
Group 1) intact teeth,
Group 2) teeth with MOD cavities without cusp reduction,
Group 3) teeth with MOD cavities with cusp reduction.
Before cavity preparation, an over-impression was made for all teeth using bleaching shields (Easy-Vac Gasket, Korea) and a vacuum machine (Easy-Vac Gasket, Korea). (25) The impressions were cut 1mm below the cementoenamel junction (CEJ) as a reference for reconstruction of margins and coronal structure. Using this method, the teeth were reconstructed according to their baseline size and morphology.
Cavity preparation:
An MOD cavity was prepared using a high-speed handpiece with cooling air and water system using a 1.0-mm diameter cylindrical bur (Diaswiss, Geneva, Switzerland). A new bur was used after every five cavity preparations.
The characteristics of the cavity were as follows:
The buccolingual width of the cavity: the cavity was prepared such that only 1 mm of enamel remained intact at margins. In order to ensure the absence of dentin at margins, we used both visual examination and measurement with the digital caliper. We placed sliding jaws of the caliper against marginal walls and opened it slightly to match and fit the shape, then, turned the lock screw; the value we measured was approximately 1 mm in all marginal wall length. As the width was not more than 1 mm, we could assure that there was no dentin left.
Pulpal depth from the cavosurface: 3 mm
The dimensions of proximal boxes were as follows:
Gingival floor width: the gingival floor of the cavity was prepared such that only 1 mm of enamel remained intact in buccal and lingual walls.
Gingival floor depth: 1 mm above the CEJ (Figure 1-A).
The same cavity preparation process was followed for the next group in addition to 2 mm cusp reduction for lingual and 1.5 mm cusp reduction for buccal enamel walls in order to strengthen unsupported enamel walls in both functional and non-functional cusps (Figure 1-B).
Afterwards, a thin layer (1 mm) of light-cure glass ionomer cement (GC Fuji II LC, Tokyo, Japan) was applied to the whole gingival floor of the cavity as stress breaker and light cured with energy density of 600 mW/cm2 (Astralis 7, Ivoclar Vivadent, Lichtenstein, Switzerland) for 40 seconds. Then, the specimens were etched with 37% phosphoric acid (MORVABON, Tehran, Iran) for 15 seconds. The process was followed by rinsing with water for 10 seconds and air-drying using air spray. Then, Single Bond (3M ESPE, St Paul, MN, USA) was applied to the cavity floor and to the inner surface of dental walls and was dried for three seconds. The second layer of bonding was applied and light cured for 20 seconds using the light-curing unit. Filtek P60 composite resin (3M ESPE, St Paul, MN, USA) was applied to the cavity in 2-mm-thick increments and cured for 40 seconds. The final increment was cured along with the bleaching shield over-impression to contour the restoration the same as an intact tooth.
Testing procedure:
After one week of storage in normal saline, the specimens were mounted in cubic-shaped acrylic resin in order to be put in a universal testing machine (Zwick-Roell, Ulm, Germany).
The specimens were subjected to a compressive force at a crosshead speed of 1 mm/minute. The force was applied by an 8-mm-diameter round metal bar positioned parallel to the long axes of the teeth, in contact with the occlusal slopes of the buccal and lingual cusps (Figure 2). The peak fracture load was recorded in Newton (N) for each tooth. Data were analyzed using one-way analysis of variance (ANOVA) and Tukey’s test with a 95% confidence interval (CI).
Figure 1. (A) Gingival floor depth is 1 mm above the cementoenamel junction (CEJ). (B) Two mm cusp reduction for lingual and 1.5 mm cusp reduction for buccal enamel walls.
{kind=link}
Figure 2. The force was applied by an 8-mm-diameter round metal bar positioned parallel to the long axes of the teeth, in contact with the occlusal slopes of the buccal and lingual cusps.
{kind=link}
Results
In the present study, the use of overlay direct resin composite provided 66% of the fracture resistance of sound teeth according to the following formula (Table 1):
Table 1. The mean±standard deviation (SD) of fracture load (N) in the studied groups
{kind=link}
The mean±standard deviation (SD) of fracture load was 1834.62±104.04 N in group 1 (intact teeth), 750.34±147.46 N in group 2 (no cusp coverage), and 1211.30±210.85 N in group 3 (buccal and palatal cusp coverage; Table1).
One-way ANOVA revealed significant differences between all three groups (P=0.001).
Tukey’s test was used for pairwise comparisons and showed that the difference between the three groups was statistically significant (P=0.001; Table 2). Group 1 had the highest fracture strength in comparison with the other groups, and the fracture strength of group 3 was higher than that of group 2 that had the lowest fracture strength.
Table 2. Comparison of the studied groups according to Tukey’s test
{kind=link}
Discussion
Nowadays, one of the most important issues discussed in operative dentistry is the ability to maintain and strengthen weakened tooth structure and to adhere to conservative principles. Amalgam does not have the ability to strengthen weakened enamel structures, and cusp coverage is more recommended in non-bonded restorations than in bonded ones. (17,21) Because of the role of enamel in aesthetics and as anterior teeth are not under severe occlusal forces, unsupported weakened enamel is preserved in these teeth. (22) The question is whether it is possible to prevent removing unsupported enamel walls due to the bond of resin materials to the dental structure in posterior teeth as well and whether composite resin can strengthen unsupported enamel in such teeth to avoid or postpone fractures.
Sometimes, due to various reasons, the resistance is decreased to the level that the tooth is no longer able to tolerate masticatory loads or even smaller forces. (23) Fracture resistance of teeth is influenced by several factors, of which, some are controllable and some are not. These factors include high compressive forces, unfavorable occlusal contacts in the centric occlusion, restorative problems, steep cusps, caries, etc. (24)
In the present study, it has been shown that the fracture resistance of MOD restorations could be more improved by direct composite full coverage design compared to inlay composite restoration, which was in agreement with the results reported by Mondelli et al, Panahandeh and Johar, and Soares et al, (13,25,26) but still was significantly lower than that of intact teeth. The results of the present study do not agree with those of previous studies that reported the fracture resistance of weakened teeth restored with resin composite without cusp coverage to be similar to that of sound teeth; (5,18,20,27-29) this is probably due to the cavity size evaluated in the present study, which was larger than those examined in the mentioned studies.
Some other researchers have stated that cusp coverage may decrease the fracture resistance of teeth. In the mentioned studies, similar cavities were prepared in teeth, and specimens were evaluated in terms of cusp coverage. (30,31) This difference can be explained by the fact that in the mentioned studies, a large volume (two-thirds) of the occlusogingival cusp was removed for coverage, and fracture resistance decreased due to significant tooth reduction (and not because of cusp coverage).
Our study results did not confirm this finding and showed that cusp coverage increases the fracture resistance of teeth; this can be explained as follows:
- Since the orientation of enamel rods varies in different parts of enamel, the bond strength differs from place to place. The best adhesion is achieved when the end (terminal part) of the enamel rod is etched. In case that the inner surface of enamel is etched, the tags will have amorphous shapes and will not be able to establish a firm connection between the resin and the inner surface of enamel. (32) Therefore, the composite cannot be strongly fused to enamel as a result of a weaker bond and cannot strengthen the unsupported enamel. On the other hand, since the orientation of enamel rods in the occlusal one-third of the external surface of enamel is more appropriate for a successful etching pattern, a stronger bond can be obtained; the head of etched enamel rods provides the highest amount of porosity and the best etching pattern in enamel. Therefore, the produced tags have better shapes and sizes and can strengthen enamel walls through a higher bond to the resin.
- Cusp coverage, similar to that in onlay restorations, provides the possibility of better force distribution and lower fracture rate. (32) Splinting the cusps together preserves the integrity of tooth structure, provides a single unit and leads to strengthening the weakened walls.
- The anchorage promoted by the resin composite, protecting the buccal and lingual cusps of group 3 specimens, rendered a fracture resistance similar to that of sound teeth. The adhesive procedure was clearly not the only factor responsible for this resistance, and cusp protection that avoided the separation in consequence of the wedge effect caused by cusp elongation also plays a major role in this respect. (13)
Therefore, composite restoration with cusp coverage reinforces unsupported or weakened dental walls and increases tooth resistance against fracture. It should be considered that, in the clinic, we may rarely encounter teeth with only 1 mm of unsupported enamel, comparable to our tested specimens. Similar to all laboratory studies, there were some limitations in the present study; for example, the intraoral aging factors were not taken into consideration. This laboratory study also did not completely mimic the occlusal forces during mastication.
Conclusion
Conclusion
The overall results of our study showed that using composite resin in restoring teeth with unsupported enamel walls must be combined with cusp coverage in order to increase the fracture strength of such teeth. Cusp coverage in premolars reinforces the remaining tooth structure and significantly increases the fracture strength of these teeth; even if a fracture occurs, it is going to be less severe.
Type of Study: Original article |
Subject:
Oral & maxillofacial surgery
References
1. 1. Zahed Pasha Y, Esmaeili Dooki M, Haji Ahmadi M, Asgardon G, Ghadimi R, Baleghi M, et al. Effect of Risk Factors on Low Birth
2. Weight Neonates. JBUMS. 2004;6(2):18-24. [DOI:10.7748/ns.18.18.24.s37]
3. Michalowicz BS, Gustafsson A Thumbigere- Math V, Buhlin K. The effects of periodontal treatment on pregnancy outcomes.
4. J Periodontol. 2013 Apr;84(4Suppl):S195-208.
5. Rajapakse PS, Nagarathne M, Chandrasekra KB, Dasanayake AP. Periodontal disease and prematurity among non-smoking
6. Sri Lankan women. J Dent Res. 2005 Mar;84(3):274-7. [DOI:10.1177/154405910508400313] [PMID]
7. Agueda A, Ramón JM, Manau C, Guerrero A, Echeverría JJ. Periodontal disease as a risk factor for adverse pregnancy outcomes: a prospective cohort study. J Clin Periodontol. 2008 Jan;35(1):16-22.
8. Gomes-Filho IS, Cruz SS, Rezende EJ, Dos Santos CA, Soledade KR, Magalhães MA, et al. Exposure measurement in the association between periodontal disease and prematurity/low birth weight. J Clin Periodontol. 2007 Nov;34(11):957-63. [DOI:10.1111/j.1600-051X.2007.01141.x] [PMID]
9. Baccaglini L. A meta-analysis of randomized controlled trials shows no evidence that periodontal treatment during pregnancy
10. prevents adverse pregnancy outcomes. J Am Dent Assoc. 2011 Oct;142(10):1192-3. [DOI:10.14219/jada.archive.2011.0089] [PMID]
11. Al-Habashneh R, Aljundi SH, Alwaeli HA. Survey of medical doctors' attitudes and knowledge of the association between oral
12. health and pregnancy outcomes. Int J Dent Hyg. 2008 Aug;6(3):214-20.
13. Chang HH1, Larson J, Blencowe H, Spong CY, Howson CP, Cairns-Smith S, et al. Preventing preterm births: analysis of trends and potential reductions with interventions in 39 countries with very high human development index.Lancet. 2013 Jan 19;381(9862):223-34. [DOI:10.1016/S0140-6736(12)61856-X]
14. Emrich LJ, Shlossman M, Genco RJ. Periodontal disease in non-insulin-dependent diabetes mellitus. J Periodontol. 1991 Feb;62(2):123-31. [DOI:10.1902/jop.1991.62.2.123] [PMID]
15. Boggess KA, Urlaub DM, Massey KE, Moos MK, Matheson MB, Lorenz C. Oral hygiene practices and dental service utilization
16. among pregnant women. J Am Dent Assoc. 2010 May;141(5):553-61.
17. Vergnes JN, Pastor-Harper D, Constantin D, Bedos C, Kaminski M, Nabet C, et al. [Perceived oral health and use of dental
18. services during pregnancy: the MaterniDent study]. [Article in French]. Sante Publique. 2013 May-Jun;25(3):281-92. [DOI:10.3917/spub.253.0281] [PMID]
19. Wilder R, Robinson C, Jared HL, Lieff S, Boggess K. Obstetricians' knowledge and practice behaviors concerning periodontal
20. health and preterm delivery and low birth weight. J Dent Hyg. 2007 Fall;81(4):81.
21. Morgan MA, Crall J, Goldenberg RL, Schulkin J. Oral health during pregnancy. J Matern Fetal Neonatal Med. 2009 Sep;22(9):733-9. [DOI:10.3109/14767050902926954] [PMID]
22. Tarannum F, Prasad S; Muzammil, Vivekananda L, Jayanthi D, Faizuddin M. Awareness of the association between periodontal disease and pre-term births among general dentists, general medical practitioners and gynecologists. Indian J Public Health. 2013 Apr-Jun;57(2):92-5. [DOI:10.4103/0019-557X.114992] [PMID]
23. Zanata RL, Fernandes KB, Navarro PS. Prenatal dental care: evaluation of professional knowledge of obstetricians and dentists in the cities of Londrina/PR and Bauru/ SP, Brazil, 2004. J Appl Oral Sci. 2008 May-Jun;16(3):194-200. [DOI:10.1590/S1678-77572008000300006] [PMID] [PMCID]
24. Ishikawa I, Sasaki KM, Aoki A, Watanabe H. Effects of Er:YAG laser on peri- odontal therapy. J Int Acad Periodontol. 2003 Jan;5(1):23-8.
25. Offenbacher S. Periodontal diseases: pathogenesis. Ann Periodontol. 1996 Nov;1(1):821-78. [DOI:10.1902/annals.1996.1.1.821] [PMID]
26. Sanz M, Kornman K; working group 3 of the joint EFP/AAP workshop. Periodontitis and adverse pregnancy outcomes: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Disease. J Periodontol. 2013 Apr;84(4 Suppl):S164-9. [DOI:10.1902/jop.2013.1340016] [PMID]
27. Oppermann RV, Weidlich P, Musskopf ML. Periodontal disease and systemic complications. Braz Oral Res. 2012;26 Suppl [DOI:10.1590/S1806-83242012000700007] [PMID]
28. 1:39-47.
29. Jeffcoat MK, Geurs NC, Reddy MS, Cliver SP, Goldenberg RL, Hauth JC. Periodontal infection and preterm birth: results of
30. a prospective study. J Am Dent Assoc. 2001 Jul;132(7):875-80.
31. López NJ, Smith PC, Gutierrez J. Higher risk of preterm birth and low birth weight in women with periodontal disease. J Dent Res. 2002 Jan;81(1):58-63. [DOI:10.1177/002203450208100113] [PMID]
32. Offenbacher S, Lieff S, Boggess KA, Murtha AP, Madianos PN, Champagne CM, et al. Maternal periodontitis and prematurity.
33. Part 1: Obstetric outcome of prematurity and growth restriction. Ann Periodontol. 2001 Dec;6(1):164-74. [DOI:10.1902/annals.2001.6.1.164] [PMID]
34. Moreu G, Téllez L, González-Jaranay M. Relationship between maternal periodontal disease and low-birth-weight pre-term infants. J Clin Periodontol. 2005 Jun;32(6):622-7. [DOI:10.1111/j.1600-051X.2005.00722.x] [PMID]
35. Jeffcoat MK, Geurs NC, Reddy MS, Goldenberg RL, Hauth JC. Current evidence regarding periodontal disease as a risk factor
36. in preterm birth. Ann Periodontol. 2001 Dec;6(1):183-8.
37. Marin C, Segura-Egea JJ, Martínez-Sahuquillo A, Bullón P. Correlation between infant birth weight and mother's periodontal status. J Clin Periodontol. 2005 Mar;32(3):299-304. [DOI:10.1111/j.1600-051X.2005.00661.x] [PMID]
38. Nutalapati R, Ramisetti A, Mutthineni RB, Jampani ND, Kasagani SK. Awareness of association between periodontitis and
39. PLBW among selected population of practicing gynecologists in Andhra Pradesh. Indian J Dent Res. 2011 Sep-Oct;22(5):735. [DOI:10.4103/0970-9290.93474] [PMID]
40. Shanthi V, Vanka A, Bhambal A, Saxena V, Saxena S, Kumar SS. Association of pregnant women periodontal status to preterm and low-birth weight babies: A systematic and evidence- based review. Dent Res J (Isfahan). 2012 Jul;9(4):368-80.
41. Lewis CW, Grossman DC, Domoto PK, Deyo RA. The role of the pediatrician in the oral health of children: A national survey. Pediatrics. 2000 Dec;106(6):E84. [DOI:10.1542/peds.106.6.e84] [PMID]
42. Roberts MW, Keels MA, Sharp MC, Lewis JL Jr. Fluoride supplement prescribing and dental referral patterns among academic pediatricians. Pediatrics. 1998 Jan;101(1):E6. [DOI:10.1542/peds.101.1.e6] [PMID]
43. Shenoy RP, Nayak DG, Sequeira PS. Periodontal disease as a risk factor in pre-term low birth weight--an assessment of gynecologists' knowledge: a pilot study. Indian J Dent Res 2009 Jan-Mar;20(1):13-6. [DOI:10.4103/0970-9290.49049] [PMID]
44. Patil SN, Kalburgi NB, Koregol AC, Warad SB, Patil S, Ugale MS. Female sex hormones and periodontal health-awareness among gynecologists - A questionnaire survey. Saudi Dent J. 2012 Apr;24(2):99-104. [DOI:10.1016/j.sdentj.2011.12.001] [PMID] [PMCID]
45. Strafford KE, Shellhaas C, Hade EM. Provider and patient perceptions about dental care during pregnancy. J Matern Fetal Neonatal Med. 2008 Jan;21(1):63-71. [DOI:10.1080/14767050701796681] [PMID]
46. Cohen L, Schaeffer M, Davideau JL, Tenenbaum H, Huck O. Obstetric Knowledge, Attitude, and Behavior Concerning Periodontal Diseases and Treatment Needs in Pregnancy: Influencing Factors in France. J Periodontol. 2015 Mar;86(3):398-405. [DOI:10.1902/jop.2014.140371] [PMID]
47. Rocha JM, Chaves VR, Urbanetz AA, Baldissera Rdos S, Rösing CK. Obstetricians' knowledge of periodontal disease as a potential risk factor for preterm delivery and low birth weight. Braz Oral Res. 2011 May-Jun;25(3):248-54. [DOI:10.1590/S1806-83242011000300010] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |