

Volume 1, Issue 4 (12-2016)
J Res Dent Maxillofac Sci 2016, 1(4): 1-8 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salem K, Ezaani P. Radiographic Evaluation of the Developmental Stages of Second and Third Molars in 7 to 11-Year-old Children and its Implication
in the Treatment of First Molars with Poor Prognosis. J Res Dent Maxillofac Sci 2016; 1 (4) :1-8
URL: http://jrdms.dentaliau.ac.ir/article-1-135-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-135-en.html


1- Assistant professor ,Pediatric dentistry Dep, Dental Branch, Islamic Azad University, Tehran, Iran , katayoun.salem@gmail.com
2- Dentist
2- Dentist
Full-Text [PDF 422 kb]
(2826 Downloads)
| Abstract (HTML) (6291 Views)
Abstract
Background and aim: First permanent molars with poor prognosis may be candidate for timely extraction and replacement by second permanent molars. The presence of third molars should be considered in this treatment plan. The aim of the present study was to evaluate the critical developmental stages of permanent second molar and the status of third molar bud in an Iranian population.
Materials and methods: Four hundred panoramic radiographs of 7 to 11-year-old children were evaluated in this descriptive study. Data were collected from patients’ files and through phone interview with parents. The stage of tooth development in each age group was determined according to the modified Demirjian method. Statistical analysis was performed using Wilcoxon signed Rank test and Chi-Square test.
Results: Stage E (beginning of root formation) in permanent second molars had the highest prevalence among 8 and 9-year-olds in the mandible, and among 9 and 10-year-olds in the maxilla. The predominant stage of development in third molar buds was stage 0 (no evidence of bud formation) in the corresponding age groups. There was no significant difference between boys and girls in terms of developmental stages. Mandibular second and third molars were more advanced than maxillary molars in terms of development, with no gender predilection.
Conclusion: The beginning of calcification in the furcation area of permanent second molar (Stage E, between 8 to 10 years of age) is the most proper stage to coincide with first molar extraction. However, during this time period, the signs of third molar bud formation are not detectable in many individuals, especially in the maxillary arch.
Keywords: Demirjian method, permanent molar, extraction, mixed dentition
Introduction
One of the clinical hindrances in pediatric dentistry is the presence of permanent first molars with poor prognosis, which their treatment requires comprehensive evaluation of the occlusion and performing the best treatment decision. One of the treatment methods is the natural substitution of the lost first molar by second molar, which can be a successful treatment under proper conditions. The correct time for this replacement is preferably when the furcation area of second molar has been calcified (developmental stage E according to the Demirjian method), which will provide the best future positioning for this tooth especially in the mandible, although the behavior pattern of mandibular second molar is not always predictable. Maxillary second molars usually find a suitable position after extraction of first molar. (1) The other factor that affects this replacement is the presence of third molar with normal size. Retrospective studies show that extraction of first molar is accompanied by accelerated development and eruption of third molar. (1)
Considering the high prevalence of severely destructed first molars and the limited number of studies performed in this regard in pediatric dentistry, the present study aimed to evaluate the key developmental stages of permanent second molar in 7 to 11-year old children of Rasht province. The second aim of the present research was to determine the presence or absence of third molar bud and its developmental stage and to use this information in the selection of the best treatment method.
Materials and methods
This study was a single-blind descriptive analysis, so that the observer was unaware of the age and gender of the participants. Four hundred panoramic radiographs of patients that had been referred to the dental school of Rasht with the age range of 7 to 11 years were evaluated. These radiographs had been obtained by Planmeca CC panoramic unit (Helsinki, Finland). Considering that the calcification of permanent second molar bud usually begins between the ages of 2.5 and 3 years, and crown formation is complete at the age of 7 to 8 years, and the age of the beginning of hard tissue formation in third molar is between 7 to 10 years, and it has been advised by the references to extract permanent first molar with poor prognosis in the most proper time period (between 8 to 10 years of age), the age range of the evaluated individuals was selected to be between 7 to 11 years. (1)
The inclusion criteria included: 7 to 11 years of age, absence of diagnosed systemic, metabolic or genetic diseases such as thyroid disorders, growth hormone disorders, vitamin D deficiency, absence of a history of malignancy, chemotherapy and radiotherapy, and absence of mental/physical disabilities. (2)
The exclusion criteria included: panoramic radiographs with technical errors or development/fixation errors that didn’t allow the assessment of second and third molars, panoramic radiographs which showed developmental or acquired dental anomalies or specific pathologies, radiographs including missing, impaction or transposition of any kind or extracted permanent teeth, radiographs of the patients with incomplete or unavailable file information or radiographs taken with units other than Planmeca CC panoramic unit. (2)
Data collection:
The samples were collected from the pediatrics and orthodontics departments of the clinic of Rasht dental school. The study questionnaire was completed at the same time either by interviewing the parents through telephone conversation or by retrieving the patients' files from the archive of the dental school. The phone numbers registered in the files were contacted and primary patients' information was recorded. From among 1600 panoramic radiographs, 1200 radiographs were selected. About 600 samples were observed and 400 samples which met the inclusion criteria were entered into the study. If a patient's information was incomplete or the parents were uncooperative or didn’t answer the phone, the patient was excluded and replaced by another patient. Children under the age of 7 years and 6 months were placed in the lower age group (7 years) and those aged over 7 years and 6 months were placed in the higher age group (8 years).
Training and Calibration of the observer:
Prior to the study, a number of panoramic radiographs were evaluated by an experienced oral and maxillofacial radiologist and the observer based on the Demirjian method, (3,4) and the diagnostic manner was regulated through discussion and debate and the observer was trained. In the second stage, calibration was performed and 15 panoramic radiographs were evaluated separately by the oral and maxillofacial radiologist and the observer. The results of the calibration stage were assessed by a statistics expert using Cohen Kappa coefficient and the agreement between the observer and the oral and maxillofacial radiologist was determined. Ten panoramic radiographs were reevaluated by the observer two months later and the inter-observer agreement was determined using Cohen Kappa coefficient.
Method of determining the developmental stages:
In assessment and classification, the developmental stages of second and third molars on both sides of the mandible and maxilla were considered. The classification of dental calcification was performed based on the modified Demirjian method. (3,4) The Demirjian method is the most advanced, the most common and the most recommended method for evaluation of dental age, but since it does not include third molar in the classifications, Solari et al used the modified Demirjian method for the estimation of the chronologic age. They introduced 10 stages of crown and root formation for more accurate determination of the developmental stage according to Apexification,. In this classification, 8 developmental stages from A to H have been considered. Stages A to D are related to crown formation and stages E to H are related to root formation, from primary furcation to apex closure. (2) In cases with no evidence of dental bud, stage zero was considered, and if only a non-calcified dental bud existed, stage 1 was considered. (3) The two mentioned stages were used to evaluate third molar. (3,4) The Demirjian developmental stages have been more frequently used, since it is more accurate than other methods, and distinct developmental stages have been mentioned as its advantage. Moreover, this method only uses the dental anatomical specifications without measuring crown and root length. In fact, it is based on the morphology and root length ratio ad uses the relative coronal length instead of the precise length. Therefore, radiographs with shortening or elongation do not affect the exactness and quality of the evaluation. It is worth mentioning that only the dental morphology was considered in the Demirjian method to avoid the problems associated with quantitative measurements, and only if the shape of a tooth was unclear or the tooth was between two developmental stages, approximate crown and root lengths were measured and the developmental stage of that tooth was sited in a lower stage. The Demirjian method includes below stages. (Table 1, Figure 1): (4)
Table 1- Dental developmental stages according to the modified Demirjian method
Figure 1- Method of determining the dental developmental stage based on the Demirjian method
Data analysis:
Data were transferred to SPSS software version 21. The aim was to evaluate the amount of crown formation, the primary stage of furcation formation and the presence or absence of third molar bud, and their frequency in the population was determined by statistical analysis of the samples.
Wilcoxon signed Rank test was used for comparison between the left and right sides of the upper and lower jaws. Moreover, Chi Square test was employed to evaluate the correlation between the developmental stages and age groups divided by gender.
Results
Four hundred 7 to 11-year-old children including 238 girls (59.5%) and 162 boys (40.5%) participated in this study. The highest frequency belonged to the 9-year-old age group (22.5%) while the lowest frequency was related to the 8-year-old age group (17.8%).
Fifteen panoramic radiographs were evaluated independently by an oral and maxillofacial radiologist and the observer to determine the inter-observer reliability. Excellent reliability coefficient was obtained regarding second and third molars (100% and 97% respectively).
Moreover, 10 panoramic radiographs were reevaluated by the observer two months later and the intra-observer reliability was determined. This coefficient was excellent regarding second and third molars (100% and 90% respectively). The frequency distribution of each developmental stage of second and third molars divided by age and gender are presented in tables 2 and 3. No significant differences were observed between boys and girls in any of the age groups (Chi Square test).
Evaluation of the developmental stages irrespective of gender showed that in mandibular second molar, the highest frequency of stage E (beginning of furcation formation ) was detected in 8 and 9 years of age (41.1 % and 39.4% respectively). In maxillary second molar, the highest frequency of stage E was related to 9 and 10 years of age (40.4% and 28.9% respectively).
In mandibular third molar, the highest frequency at 8 and 9 years of age belonged to stage zero (absence of tooth bud) (46.5% and 36.7% respectively). In maxillary third molar, stage zero was reported at 9 years of age in 63.3% of individuals, while this value was 39.8% at 10 years of age.
The relative frequency of the developmental stages of second and third molars irrespective of gender are presented in tables 4 and 5.
Regarding the developmental stages of third molars, according to Wilcoxon signed Rank test, no significant difference was observed between the left and right sides of the jaws, (0.31
Comparison of the developmental stages between the maxilla and mandible showed that overall, mandibular second and third molars were developmentally more advanced than maxillary molars (p<0.01) (Wilcoxon signed Rank test).
Table 2- Relative frequency of each developmental stage in mandibular and maxillary second molars divided by age and gender
Table 3- Relative frequency of each developmental stage in maxillary and mandibular third molars divided by age and gender
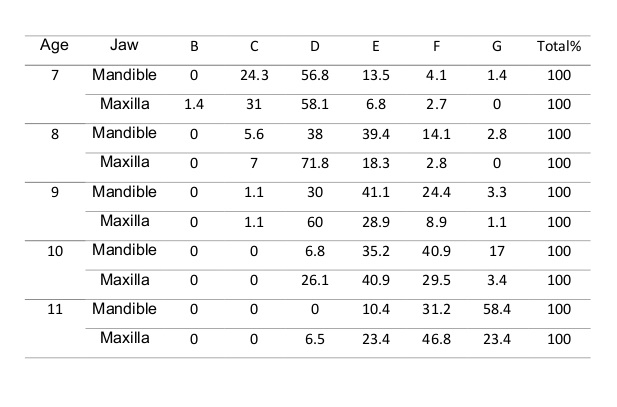
Table 4- Relative frequency of each developmental stage in maxillary and mandibular second molars based on age
Table 5- Relative frequency of each developmental stage in maxillary and mandibular third molars based on age
Discussion
The aim of the present study was the evaluation of the developmental status of permanent second molar and also the determination of the status of third molar to use this information in the selection of treatment plan for permanent molars with poor prognosis. Due to early growth and also developmental deficiencies such as molar-incisor hypoplasia and hypo mineralization, permanent first molar is predisposed to premature destruction. Although restorative and endodontic treatments can preserve teeth in children and adolescents, but the extensively-restored teeth may need extraction during the later years. Delayed extraction can leave undesired side effects on the occlusion. Upon encountering extensively-destructed teeth, early extraction during the mixed dentition phase can lead to a correct occlusion with minimum complications, provided that other conditions are suitable such as presence of third molar with normal size and class 1 occlusion with mild crowding. Assessment of the amount of development of permanent second molar (as a predictor of the manner of movement of this tooth after extraction of first molar) is of special importance. Among the developmental stages of permanent second molar, the stage of beginning of calcification in the furcation area (Stage E) is the most proper stage to coincide with first molar extraction, and can lead to proper axial angle and acceptable tooth contact and therefore, it is important in terms of tooth movement. (1,6) Untimely and early extraction of first molar can lead to distal drift of the premolar or its rotation, because the premolar lacks strong intra bone support, and the socket of first molar can be an easier path for its movement. (6) The suitable time for extraction of first molar is correlated with the developmental stage E in permanent second molar.
The results of the present study showed that the highest relative frequency of stage E in the mandible is related to 9 and 8-year-old children while in the maxilla, it is detected in 10 and 9-year-olds. The developmental stages of mandibular second molars in boys and girls preceded those of maxillary second molars. In regard to maxillary third molar, in 10 and 9 years of age respectively 3.3% and 2.3% of children showed the primary signs of the presence of third molar bud (developmental stage 1). The primary signs of formation of this tooth bud in the mandible in 8 and 9-year-olds were observed in 10% and 19.7% of the studied population. Based on a study by Orhan et al in Turkey, the first signs of formation of third molar's crypt (developmental stage 1) were reported since the 7 years of age, which is in line with our results, although in the present study the highest frequency of this stage was observed in 8-year-olds in the mandible and in 9-year-olds in the maxilla. (4) Moreover, at 11 years of age, over 11% of the subjects still were showing no signs of formation of third molar bud. Some researchers have attributed this lack of bud formation after this age to be a probable sign of the absence of third molar. (4) It can be concluded that during the proper time for first molar extraction, there is no adequate evidence of the presence of third molar in many individuals. (1)
Mandibular third molars in boys and girls preceded maxillary third molars in terms of development, so that respectively in 63.3% and 39.8% of 9 and 10-year-old individuals no signs of third molar formation were observed. In a study by Almedia et al, similar to our study, the development of mandibular third molars was more advanced than maxillary third molars, while in a study by Caldas et al no difference existed between the maxilla and mandible. (7,8) In the studies by Kasper et al and Arany et al, the development of maxillary third molars was more advanced than mandibular third molars. (9,10) Likewise, in the study by Orhan et al, maxillary third molars were more advanced in terms of development compared to mandibular third molars but the difference was not significant. (4)
In the present study, no differences were observed between boys and girls in terms of the development status of second and third molars. In the studies by Orhan, Caldas, Sisman, Kasper, Arany, Bai and Meinl et al, the development of third molar was more advanced in males. (4,8-13) But in the study by Almedia et al, the development of third molar was more advanced in females. (7) In a study by Lee et al, the development of second molar was more advanced in females and the development of third molar up to stage E in the maxilla and up to stage D in the mandible was more advanced in females. (14) Bagherian et al reported more advanced development for second molar in girls compared with that in boys. (15) These differences can be attributed to the ethnical differences among various populations or to the differences in sample size. (4,13)
In the present study, the inter/intra-observer reliability was excellent similar to the studies by Orhan, Sisman and Lee et al. (4,11,14) A reason for this excellent agreement was the access to distinct developmental stages and the absence of interstitial stages. In the present study, no significant differences were observed in comparing left and right mandibular and maxillary second molars, which is similar to the results of the study by Lee et al. (14) Also, no differences existed between left and right maxillary and mandibular third molars, which is similar to the findings of the studies by Orhan, Almedia, Arany, Meinl and Lee et al. (4,7,10,13,14) However, in the present study, significant differences were observed between left and right maxillary third molars in 11-year-old girls, and left side was developmentally delayed. This finding which was similar to the finding of Caldas et al should be considered in treatment planning. (8)
Thus far, different methods have been introduced for dental age estimation using radiographic stages of tooth development. Assessment by these methods should be accurate, noninvasive, repeatable and easy to use. The Demirjian ten-step modified method follows the above mentioned characteristics. It is easy to use and targeted. It does not require tooth measurements, therefore interventions due to personalization are omitted. This method only requires experience in panoramic interpretation. In addition, it has been used in many studies which allows comparisons with others. Indigenous individuals allowed the assessment of the developmental status in the evaluated population. Although, one of the limitations of this study was lack of a longitudinal assessment to follow up probable changes during time. The other limitation was the probable confounders such as the socio-economic status, which can affect child's growth and the observed calcification in radiography through nutrition and life style. (7)
Conclusion
The results of the present study showed that the highest relative frequency of the developmental stage E in permanent second molars in the assessed population was related to 9 and 10 years of age in the maxilla and to 8 and 9 years of age in the mandible. Nevertheless, during this time period, signs of third molar bud formation (stage 1) were not detectable in many individuals.
Full-Text: (1043 Views)
Abstract
Background and aim: First permanent molars with poor prognosis may be candidate for timely extraction and replacement by second permanent molars. The presence of third molars should be considered in this treatment plan. The aim of the present study was to evaluate the critical developmental stages of permanent second molar and the status of third molar bud in an Iranian population.
Materials and methods: Four hundred panoramic radiographs of 7 to 11-year-old children were evaluated in this descriptive study. Data were collected from patients’ files and through phone interview with parents. The stage of tooth development in each age group was determined according to the modified Demirjian method. Statistical analysis was performed using Wilcoxon signed Rank test and Chi-Square test.
Results: Stage E (beginning of root formation) in permanent second molars had the highest prevalence among 8 and 9-year-olds in the mandible, and among 9 and 10-year-olds in the maxilla. The predominant stage of development in third molar buds was stage 0 (no evidence of bud formation) in the corresponding age groups. There was no significant difference between boys and girls in terms of developmental stages. Mandibular second and third molars were more advanced than maxillary molars in terms of development, with no gender predilection.
Conclusion: The beginning of calcification in the furcation area of permanent second molar (Stage E, between 8 to 10 years of age) is the most proper stage to coincide with first molar extraction. However, during this time period, the signs of third molar bud formation are not detectable in many individuals, especially in the maxillary arch.
Keywords: Demirjian method, permanent molar, extraction, mixed dentition
Introduction
One of the clinical hindrances in pediatric dentistry is the presence of permanent first molars with poor prognosis, which their treatment requires comprehensive evaluation of the occlusion and performing the best treatment decision. One of the treatment methods is the natural substitution of the lost first molar by second molar, which can be a successful treatment under proper conditions. The correct time for this replacement is preferably when the furcation area of second molar has been calcified (developmental stage E according to the Demirjian method), which will provide the best future positioning for this tooth especially in the mandible, although the behavior pattern of mandibular second molar is not always predictable. Maxillary second molars usually find a suitable position after extraction of first molar. (1) The other factor that affects this replacement is the presence of third molar with normal size. Retrospective studies show that extraction of first molar is accompanied by accelerated development and eruption of third molar. (1)
Considering the high prevalence of severely destructed first molars and the limited number of studies performed in this regard in pediatric dentistry, the present study aimed to evaluate the key developmental stages of permanent second molar in 7 to 11-year old children of Rasht province. The second aim of the present research was to determine the presence or absence of third molar bud and its developmental stage and to use this information in the selection of the best treatment method.
Materials and methods
This study was a single-blind descriptive analysis, so that the observer was unaware of the age and gender of the participants. Four hundred panoramic radiographs of patients that had been referred to the dental school of Rasht with the age range of 7 to 11 years were evaluated. These radiographs had been obtained by Planmeca CC panoramic unit (Helsinki, Finland). Considering that the calcification of permanent second molar bud usually begins between the ages of 2.5 and 3 years, and crown formation is complete at the age of 7 to 8 years, and the age of the beginning of hard tissue formation in third molar is between 7 to 10 years, and it has been advised by the references to extract permanent first molar with poor prognosis in the most proper time period (between 8 to 10 years of age), the age range of the evaluated individuals was selected to be between 7 to 11 years. (1)
The inclusion criteria included: 7 to 11 years of age, absence of diagnosed systemic, metabolic or genetic diseases such as thyroid disorders, growth hormone disorders, vitamin D deficiency, absence of a history of malignancy, chemotherapy and radiotherapy, and absence of mental/physical disabilities. (2)
The exclusion criteria included: panoramic radiographs with technical errors or development/fixation errors that didn’t allow the assessment of second and third molars, panoramic radiographs which showed developmental or acquired dental anomalies or specific pathologies, radiographs including missing, impaction or transposition of any kind or extracted permanent teeth, radiographs of the patients with incomplete or unavailable file information or radiographs taken with units other than Planmeca CC panoramic unit. (2)
Data collection:
The samples were collected from the pediatrics and orthodontics departments of the clinic of Rasht dental school. The study questionnaire was completed at the same time either by interviewing the parents through telephone conversation or by retrieving the patients' files from the archive of the dental school. The phone numbers registered in the files were contacted and primary patients' information was recorded. From among 1600 panoramic radiographs, 1200 radiographs were selected. About 600 samples were observed and 400 samples which met the inclusion criteria were entered into the study. If a patient's information was incomplete or the parents were uncooperative or didn’t answer the phone, the patient was excluded and replaced by another patient. Children under the age of 7 years and 6 months were placed in the lower age group (7 years) and those aged over 7 years and 6 months were placed in the higher age group (8 years).
Training and Calibration of the observer:
Prior to the study, a number of panoramic radiographs were evaluated by an experienced oral and maxillofacial radiologist and the observer based on the Demirjian method, (3,4) and the diagnostic manner was regulated through discussion and debate and the observer was trained. In the second stage, calibration was performed and 15 panoramic radiographs were evaluated separately by the oral and maxillofacial radiologist and the observer. The results of the calibration stage were assessed by a statistics expert using Cohen Kappa coefficient and the agreement between the observer and the oral and maxillofacial radiologist was determined. Ten panoramic radiographs were reevaluated by the observer two months later and the inter-observer agreement was determined using Cohen Kappa coefficient.
Method of determining the developmental stages:
In assessment and classification, the developmental stages of second and third molars on both sides of the mandible and maxilla were considered. The classification of dental calcification was performed based on the modified Demirjian method. (3,4) The Demirjian method is the most advanced, the most common and the most recommended method for evaluation of dental age, but since it does not include third molar in the classifications, Solari et al used the modified Demirjian method for the estimation of the chronologic age. They introduced 10 stages of crown and root formation for more accurate determination of the developmental stage according to Apexification,. In this classification, 8 developmental stages from A to H have been considered. Stages A to D are related to crown formation and stages E to H are related to root formation, from primary furcation to apex closure. (2) In cases with no evidence of dental bud, stage zero was considered, and if only a non-calcified dental bud existed, stage 1 was considered. (3) The two mentioned stages were used to evaluate third molar. (3,4) The Demirjian developmental stages have been more frequently used, since it is more accurate than other methods, and distinct developmental stages have been mentioned as its advantage. Moreover, this method only uses the dental anatomical specifications without measuring crown and root length. In fact, it is based on the morphology and root length ratio ad uses the relative coronal length instead of the precise length. Therefore, radiographs with shortening or elongation do not affect the exactness and quality of the evaluation. It is worth mentioning that only the dental morphology was considered in the Demirjian method to avoid the problems associated with quantitative measurements, and only if the shape of a tooth was unclear or the tooth was between two developmental stages, approximate crown and root lengths were measured and the developmental stage of that tooth was sited in a lower stage. The Demirjian method includes below stages. (Table 1, Figure 1): (4)
Table 1- Dental developmental stages according to the modified Demirjian method
{kind=link}
Figure 1- Method of determining the dental developmental stage based on the Demirjian method
{kind=link}
Data analysis:
Data were transferred to SPSS software version 21. The aim was to evaluate the amount of crown formation, the primary stage of furcation formation and the presence or absence of third molar bud, and their frequency in the population was determined by statistical analysis of the samples.
Wilcoxon signed Rank test was used for comparison between the left and right sides of the upper and lower jaws. Moreover, Chi Square test was employed to evaluate the correlation between the developmental stages and age groups divided by gender.
Results
Four hundred 7 to 11-year-old children including 238 girls (59.5%) and 162 boys (40.5%) participated in this study. The highest frequency belonged to the 9-year-old age group (22.5%) while the lowest frequency was related to the 8-year-old age group (17.8%).
Fifteen panoramic radiographs were evaluated independently by an oral and maxillofacial radiologist and the observer to determine the inter-observer reliability. Excellent reliability coefficient was obtained regarding second and third molars (100% and 97% respectively).
Moreover, 10 panoramic radiographs were reevaluated by the observer two months later and the intra-observer reliability was determined. This coefficient was excellent regarding second and third molars (100% and 90% respectively). The frequency distribution of each developmental stage of second and third molars divided by age and gender are presented in tables 2 and 3. No significant differences were observed between boys and girls in any of the age groups (Chi Square test).
Evaluation of the developmental stages irrespective of gender showed that in mandibular second molar, the highest frequency of stage E (beginning of furcation formation ) was detected in 8 and 9 years of age (41.1 % and 39.4% respectively). In maxillary second molar, the highest frequency of stage E was related to 9 and 10 years of age (40.4% and 28.9% respectively).
In mandibular third molar, the highest frequency at 8 and 9 years of age belonged to stage zero (absence of tooth bud) (46.5% and 36.7% respectively). In maxillary third molar, stage zero was reported at 9 years of age in 63.3% of individuals, while this value was 39.8% at 10 years of age.
The relative frequency of the developmental stages of second and third molars irrespective of gender are presented in tables 4 and 5.
Regarding the developmental stages of third molars, according to Wilcoxon signed Rank test, no significant difference was observed between the left and right sides of the jaws, (0.31
Comparison of the developmental stages between the maxilla and mandible showed that overall, mandibular second and third molars were developmentally more advanced than maxillary molars (p<0.01) (Wilcoxon signed Rank test).
Table 2- Relative frequency of each developmental stage in mandibular and maxillary second molars divided by age and gender
{kind=link}
Table 3- Relative frequency of each developmental stage in maxillary and mandibular third molars divided by age and gender
{kind=link}
Table 4- Relative frequency of each developmental stage in maxillary and mandibular second molars based on age
{kind=link}
Table 5- Relative frequency of each developmental stage in maxillary and mandibular third molars based on age
{kind=link}
Discussion
The aim of the present study was the evaluation of the developmental status of permanent second molar and also the determination of the status of third molar to use this information in the selection of treatment plan for permanent molars with poor prognosis. Due to early growth and also developmental deficiencies such as molar-incisor hypoplasia and hypo mineralization, permanent first molar is predisposed to premature destruction. Although restorative and endodontic treatments can preserve teeth in children and adolescents, but the extensively-restored teeth may need extraction during the later years. Delayed extraction can leave undesired side effects on the occlusion. Upon encountering extensively-destructed teeth, early extraction during the mixed dentition phase can lead to a correct occlusion with minimum complications, provided that other conditions are suitable such as presence of third molar with normal size and class 1 occlusion with mild crowding. Assessment of the amount of development of permanent second molar (as a predictor of the manner of movement of this tooth after extraction of first molar) is of special importance. Among the developmental stages of permanent second molar, the stage of beginning of calcification in the furcation area (Stage E) is the most proper stage to coincide with first molar extraction, and can lead to proper axial angle and acceptable tooth contact and therefore, it is important in terms of tooth movement. (1,6) Untimely and early extraction of first molar can lead to distal drift of the premolar or its rotation, because the premolar lacks strong intra bone support, and the socket of first molar can be an easier path for its movement. (6) The suitable time for extraction of first molar is correlated with the developmental stage E in permanent second molar.
The results of the present study showed that the highest relative frequency of stage E in the mandible is related to 9 and 8-year-old children while in the maxilla, it is detected in 10 and 9-year-olds. The developmental stages of mandibular second molars in boys and girls preceded those of maxillary second molars. In regard to maxillary third molar, in 10 and 9 years of age respectively 3.3% and 2.3% of children showed the primary signs of the presence of third molar bud (developmental stage 1). The primary signs of formation of this tooth bud in the mandible in 8 and 9-year-olds were observed in 10% and 19.7% of the studied population. Based on a study by Orhan et al in Turkey, the first signs of formation of third molar's crypt (developmental stage 1) were reported since the 7 years of age, which is in line with our results, although in the present study the highest frequency of this stage was observed in 8-year-olds in the mandible and in 9-year-olds in the maxilla. (4) Moreover, at 11 years of age, over 11% of the subjects still were showing no signs of formation of third molar bud. Some researchers have attributed this lack of bud formation after this age to be a probable sign of the absence of third molar. (4) It can be concluded that during the proper time for first molar extraction, there is no adequate evidence of the presence of third molar in many individuals. (1)
Mandibular third molars in boys and girls preceded maxillary third molars in terms of development, so that respectively in 63.3% and 39.8% of 9 and 10-year-old individuals no signs of third molar formation were observed. In a study by Almedia et al, similar to our study, the development of mandibular third molars was more advanced than maxillary third molars, while in a study by Caldas et al no difference existed between the maxilla and mandible. (7,8) In the studies by Kasper et al and Arany et al, the development of maxillary third molars was more advanced than mandibular third molars. (9,10) Likewise, in the study by Orhan et al, maxillary third molars were more advanced in terms of development compared to mandibular third molars but the difference was not significant. (4)
In the present study, no differences were observed between boys and girls in terms of the development status of second and third molars. In the studies by Orhan, Caldas, Sisman, Kasper, Arany, Bai and Meinl et al, the development of third molar was more advanced in males. (4,8-13) But in the study by Almedia et al, the development of third molar was more advanced in females. (7) In a study by Lee et al, the development of second molar was more advanced in females and the development of third molar up to stage E in the maxilla and up to stage D in the mandible was more advanced in females. (14) Bagherian et al reported more advanced development for second molar in girls compared with that in boys. (15) These differences can be attributed to the ethnical differences among various populations or to the differences in sample size. (4,13)
In the present study, the inter/intra-observer reliability was excellent similar to the studies by Orhan, Sisman and Lee et al. (4,11,14) A reason for this excellent agreement was the access to distinct developmental stages and the absence of interstitial stages. In the present study, no significant differences were observed in comparing left and right mandibular and maxillary second molars, which is similar to the results of the study by Lee et al. (14) Also, no differences existed between left and right maxillary and mandibular third molars, which is similar to the findings of the studies by Orhan, Almedia, Arany, Meinl and Lee et al. (4,7,10,13,14) However, in the present study, significant differences were observed between left and right maxillary third molars in 11-year-old girls, and left side was developmentally delayed. This finding which was similar to the finding of Caldas et al should be considered in treatment planning. (8)
Thus far, different methods have been introduced for dental age estimation using radiographic stages of tooth development. Assessment by these methods should be accurate, noninvasive, repeatable and easy to use. The Demirjian ten-step modified method follows the above mentioned characteristics. It is easy to use and targeted. It does not require tooth measurements, therefore interventions due to personalization are omitted. This method only requires experience in panoramic interpretation. In addition, it has been used in many studies which allows comparisons with others. Indigenous individuals allowed the assessment of the developmental status in the evaluated population. Although, one of the limitations of this study was lack of a longitudinal assessment to follow up probable changes during time. The other limitation was the probable confounders such as the socio-economic status, which can affect child's growth and the observed calcification in radiography through nutrition and life style. (7)
Conclusion
The results of the present study showed that the highest relative frequency of the developmental stage E in permanent second molars in the assessed population was related to 9 and 10 years of age in the maxilla and to 8 and 9 years of age in the mandible. Nevertheless, during this time period, signs of third molar bud formation (stage 1) were not detectable in many individuals.
Type of Study: Original article |
Subject:
Periodontology
References
1. Cobourne MT, Williams A, Harrison M. National clinical guidelines for the extraction of first permanent molars in children. Br Dent J 2014;217(11):643-8.
2. Bagherpour A, Imanimoghaddam M, Bagherpour MR, Einolghozati M. Dental age assessment among Iranian children aged 6–13 years using the Demirjian method. Forensic Sci Int 2010;197(1-3):121.e1–4.
3. Lewis AJ, Boaz K, Nagesh KR, Srikant N, Gupta N, Nandita KP, et al. Demirjian’s method in the estimation of age: A study on human third molars. J Forensic Dent Sci 2015;7(2):153–7.
4. Orhan K, Ozer L, Orhan AI, Dogan S, Paksoy CS. Radiographic evaluation of third molar development in relation to chronological age among Turkish children and youth. Forensic Sci Int 2007;165(1):46-51.
5. Gill DS, Lee RT, Tredwindec CJ. Treatment Planning for the Loss of First Permanent Molars.Dent Update 2001;28(6):304-8.
6. Almeida MS, Pontual Ados A, Beltrao RT, Pontual ML.The chronology of second molar development in Brazilians and its application to forensic age estimation. Imaging Sci Den 2013;43(1):1-6.
7. Caldas I M, Júlio P, Simoes RJ , Matos E, Afonso A , Magalhaes T. Chronological age estimation based on third molar development in a Portuguese population. Int J Legal Med 2011;125(2):235–43.
8. Kasper KA, Austin D, Kvanli AH, Rios TR, Senn DR. Reliability of Third Molar Development for Age Estimation in a Texas Hispanic Population:A Comparison Study. J Forensic Sci 2009;54( 3):651-7.
9. Arany S, Iino M,Yoshioka N. Radiographic Survey of Third Molar Development in Relation to Chronological Age Among Japanese Juveniles. J Forensic Sci 2004;49(3):534-8.
10. Sisman Y, Uysal T, Yagmur F , Ramoglu S. Third – Molar Development in Relation to chronologic Age in Turkish children and Young Adults . Angle Orthod 2006;77(6):1040-5.
11. Bai Y, Mao J, Zhu S, Wei W.Third-Molar Development in Relation to Chronologic Age in Young Adults of Central China. J Huazhong Univ Sci Technolog Med Sci 2008;28(4):487-90.
12. Meini A, Tangl S, Huber C , Maurer B , Watzek G .The chronology of third molar mineralization in the Austrian population – a contribution to forensic age estimation .Forensic Sci Int 2007;169(2-3): 161-7.
13. Lee SS, Byun YS,Park MJ,Choi JH,Yoon CL,Shin KJ.The chronology of second and third molar mineralization in Korean population and application to forensic age estimation. Int J Legal Med 2010;124(6):659-65.
14. Bagherian A, Sadeghi M.Assessment of dental maturity of children aged 3.5 to 13.5 years using the Demirjian method in an Iranian population. J Oral Sci 2011;53(1):37-42.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
