Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 2 (6-2026)
J Res Dent Maxillofac Sci 2026, 11(2): 148-155 |
Back to browse issues page
Ethics code: IR.IAU.DENTAL.REC.1403.088
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khodabandehlou F, Zahedi Rad S, Alamdari Mahd M. Spectrophotometric Comparison of Color Change of White Spot Lesions after the Application of Two Types of Resin Infiltrants: An In Vitro Study. J Res Dent Maxillofac Sci 2026; 11 (2) :148-155
URL: http://jrdms.dentaliau.ac.ir/article-1-1330-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-1330-en.html


1- Dentist in private practice, Tehran, Iran
2- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran
3- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran ,mandanaalamdari@iau.ac.ir
2- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran
3- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 391 kb]
(6 Downloads)
| Abstract (HTML) (8 Views)
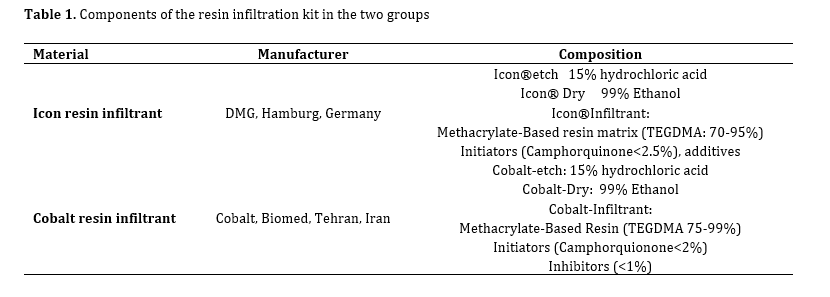
Table 1. Components of the resin infiltration kit in the two groups
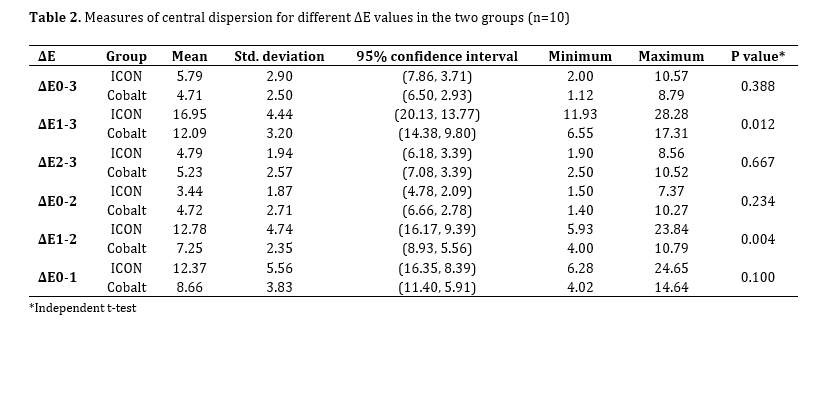
Table 2. Measures of central dispersion for different ΔE values in the two groups (n=10)
Regarding the comparison of ΔE1-0 [sound state (T0) to after the induction of WSLs (T1)], the mean ΔE was 12.37±5.57 for ICON and 3.84±8.66 for Cobalt. According to Dogra et al, [8] ΔE=3.7 is considered the threshold for clinical detection, meaning that ΔE values greater than 3.7 are clinically visible to patients and dentists, and may require color correction and restoration. Accordingly, in both study groups, WSLs were clinically visible and did not differ significantly (P=0.100).
Based on the present results, in the comparison of ΔE2-0, ICON infiltration resin with a mean ΔE value of 3.44 showed superior color coverage than Cobalt infiltration resin with a mean ΔE value of 4.73 although this difference was not statistically significant. This result was consistent with the findings of Dogra et al [8]. They compared ΔE in WSLs caused by fluorosis before and after treatment with ICON resin infiltrant using a spectrophotometer, and reported that ΔE was less than 3.7, indicating no color difference visible to the naked eye. Also, comparison of ΔE2-1 indicated significant superiority of ICON with a mean ΔE of 12.78 compared to Cobalt with a mean ΔE of 7.25; this significant superiority can be explained by the fact that after applying Cobalt, WSLs were visually visible to some extent, but after applying ICON, WSLs were not visually visible; indicating that ICON was able to create a significant color coverage compared to Cobalt. This result was somewhat consistent with the findings of Prasada et al [7]. They compared the efficacy of ICON resin infiltrant to bioactive glass and NaF to improve the esthetic appearance of WSLs. They reported that ICON caused the greatest improvement in color of WSLs compared to bioactive glass and NaF. Also, Hammad et al. [5] evaluated the ΔE and color stability of ICON in treatment of WSLs, compared to nano-hydroxyapatite toothpaste and microabrasion. They indicated the superiority of ICON over microabrasion and nano-hydroxyapatite for color improvement of WSLs. Also, Nagib et al. [1] compared the ΔE of WSLs using three treatment approaches: resin infiltration, bleaching, and microabrasion, and reported that ICON alone provided less color coverage than combined methods such as bleaching + ICON. The reason for color improvement of WSLs after bleaching with ICON is attributed to the fact that bleaching removes pigments and then the resin infiltrant blocks the pores in WSLs.
Comparison of the stability of color coverage from immediately after treatment (T2) to 4 weeks later (T3) indicated that ICON with a mean ΔE of 4.79 had a greater color stability than Cobalt with a mean ΔE of 5.24. However, this difference was not statistically significant indicating that the two resin infiltrants had a relatively similar stability during this time period. In line with the present results, Zaazou et al. [17] evaluated the effect of ICON resin infiltrant on ΔE of WSLs during the follow-up periods of 3, 6 and 12 months in a clinical study, and showed that although color coating of lesions was initially significant, there was a slight decrease in color stability over time and further evaluation is needed to investigate the durability of its long-term effects. Based on a study by Schoppmeier et al. [18], the TEGDEMA present in the composition of resin infiltrant has the potential for color change due to its tendency to absorb water. Schoppmeier et al. [18] showed that office or home bleaching led to improvement of the color of infiltrated WSLs to their baseline shade after treatment. In the present study, a significant change in color stability was not observed, probably due to the short follow-up of 4 weeks. On the other hand, the significant difference in ΔE1-3 and ΔE1-2 may be attributed to the difference in the viscosity of the etching acid between the two groups, such that the lower viscosity of the etchant in the ICON resin infiltration kit leads to better surface wettability, improved penetration into the depth of the porosities, and consequently, enhanced color and esthetic improvement of WSLs. According to a study by Al-Saeed et al. [19], the viscosity of the etchant can indeed influence the depth of penetration of resin infiltrant; lower-viscosity acids spread easily and penetrate more uniformly into the enamel surface, and penetration coefficient of resin infiltrant is strongly dependent on the permeability of the lesion surface.
Although this study was the first to assess the efficacy of Cobalt resin infiltrant for color correction of WSLs, it had some limitations as well. The study was conducted in vitro, and lacked the complexities of the oral environment (such as alterations in pH, temperature, bacterial flora, and diet), which may affect the generalizability of the results to clinical settings. Also, the 4-week follow-up period was short, and the long-term stability of color coverage was not evaluated. Clinical studies with longer follow-ups (more than 6 months) are required to investigate the stability of color coverage in real oral conditions.
Conclusion
Full-Text: (1 Views)
Abstract
Background and Aim: This study aimed to spectrophotometrically compare the color change (ΔE) of white spot lesions (WSLs) after the application of ICON and Cobalt resin infiltrants.
Materials and Methods: In this in vitro study, WSLs were artificially induced in 20 extracted sound human premolars by their 7-day immersion in a demineralizing solution with a pH of 4.4. The specimens were randomly assigned to two groups (n=10) for resin infiltration treatment with ICON and Cobalt resin infiltrants. The color parameters of the specimens were measured before the intervention (T0), after demineralization (T1), immediately after treatment (T2), and 4 weeks after treatment (T3) spectrophotometrically by using the CIEL*a*b* system. ΔE values were calculated and analyzed by independent t-test (alpha=0.05).
Results: In comparison of ΔE2-0, the difference was not statistically significant between ICON and Cobalt (P=0.234). In comparison of ΔE2-1, ICON (ΔE=12.78) showed a significantly better coverage than Cobalt (ΔE=7.25) (P=0.004). In comparison of ΔE3-2, ICON (ΔE =4.79) showed higher color stability than Cobalt (ΔE=5.24), but the difference was not significant (P=0.667).
Conclusion: The results of this study showed that both ICON and Cobalt effectively corrected the color of WSLs to match the color of sound enamel, although ICON showed a slightly superior performance. The two resin infiltrants also had a comparable color stability after 4 weeks.
Keywords: Color; Dental Caries; Dentition, Permanent; Spectrophotometry
Introduction
Materials and Methods: In this in vitro study, WSLs were artificially induced in 20 extracted sound human premolars by their 7-day immersion in a demineralizing solution with a pH of 4.4. The specimens were randomly assigned to two groups (n=10) for resin infiltration treatment with ICON and Cobalt resin infiltrants. The color parameters of the specimens were measured before the intervention (T0), after demineralization (T1), immediately after treatment (T2), and 4 weeks after treatment (T3) spectrophotometrically by using the CIEL*a*b* system. ΔE values were calculated and analyzed by independent t-test (alpha=0.05).
Results: In comparison of ΔE2-0, the difference was not statistically significant between ICON and Cobalt (P=0.234). In comparison of ΔE2-1, ICON (ΔE=12.78) showed a significantly better coverage than Cobalt (ΔE=7.25) (P=0.004). In comparison of ΔE3-2, ICON (ΔE =4.79) showed higher color stability than Cobalt (ΔE=5.24), but the difference was not significant (P=0.667).
Conclusion: The results of this study showed that both ICON and Cobalt effectively corrected the color of WSLs to match the color of sound enamel, although ICON showed a slightly superior performance. The two resin infiltrants also had a comparable color stability after 4 weeks.
Keywords: Color; Dental Caries; Dentition, Permanent; Spectrophotometry
Introduction
White spot lesions (WSLs) have a white and opaque appearance, cause cosmetic problems, reduce enamel hardness, and change enamel surface texture [1]. These lesions can be the early sign of dental caries or result from developmental enamel defects, such as enamel hypomineralization or fluorosis. They may also develop during or after orthodontic treatment [2]. The prevalence of WSLs due to developmental enamel defects varies from 3.6% to 25%, while the prevalence of WSLs after orthodontic treatment ranges from 2% to 97% [2-4]. Evidence indicates that more than 50% of patients treated with fixed orthodontic appliances (brackets) experience at least one WSL during treatment. These lesions often develop on the buccal surface of teeth, especially around the brackets, and in addition to being unsightly, they can lead to progressive caries and further destruction of tooth structure [5].
Effective prevention and treatment of WSLs are essential for maintaining dental health and restoring the esthetic appearance of the teeth in orthodontic patients [5]. From a restorative perspective, treatment of WSLs has always been challenging because these lesions are usually confined to the enamel, and invasive treatments such as veneers or composite restorations require extensive removal of sound tooth structure [5]. Therefore, minimally invasive treatment approaches that can improve the esthetic appearance and mechanical properties of enamel while preserving maximum tooth structure have received much attention. In this regard, various methods have been proposed for the treatment of WSLs, including fluoride therapy, application of casein phosphopeptide-amorphous calcium phosphate, resin infiltrants, and, more recently, treatment with nanohydroxyapatite-containing materials [2-6]. Various studies have reported optimal results regarding the treatment of WSLs with ICON resin infiltration. Prasada et al. [7], spectrophotomet-rically evaluated the efficacy of treatment of WSLs with resin infiltration (ICON®). According to their findings, resin infiltration is a micro-invasive method for treatment of WSLs that shows acceptable cosmetic results in the short term. Also, Dogra et al. [8] showed that ICON resin infiltrant can restore the color of WSLs to a clinically acceptable level. The abovementioned studies all proposed resin infiltration as a minimally invasive treatment for WSLs. This approach prevents further demineralization and shows acceptable cosmetic results in the short term by deeply penetrating the demineralized areas with a low-viscosity resin [9]. However, no study has been conducted on the efficacy of Cobalt infiltration resin for treatment of WSLs. Thus, this study aimed to spectrophotometrically compare the color change (ΔE) of WSLs after the application of ICON and Cobalt resin infiltrants. The null hypothesis of the study was that the ΔE of WSLs would not be significantly different following the application of ICON and Cobalt resin infiltrants.
Materials and Methods
Effective prevention and treatment of WSLs are essential for maintaining dental health and restoring the esthetic appearance of the teeth in orthodontic patients [5]. From a restorative perspective, treatment of WSLs has always been challenging because these lesions are usually confined to the enamel, and invasive treatments such as veneers or composite restorations require extensive removal of sound tooth structure [5]. Therefore, minimally invasive treatment approaches that can improve the esthetic appearance and mechanical properties of enamel while preserving maximum tooth structure have received much attention. In this regard, various methods have been proposed for the treatment of WSLs, including fluoride therapy, application of casein phosphopeptide-amorphous calcium phosphate, resin infiltrants, and, more recently, treatment with nanohydroxyapatite-containing materials [2-6]. Various studies have reported optimal results regarding the treatment of WSLs with ICON resin infiltration. Prasada et al. [7], spectrophotomet-rically evaluated the efficacy of treatment of WSLs with resin infiltration (ICON®). According to their findings, resin infiltration is a micro-invasive method for treatment of WSLs that shows acceptable cosmetic results in the short term. Also, Dogra et al. [8] showed that ICON resin infiltrant can restore the color of WSLs to a clinically acceptable level. The abovementioned studies all proposed resin infiltration as a minimally invasive treatment for WSLs. This approach prevents further demineralization and shows acceptable cosmetic results in the short term by deeply penetrating the demineralized areas with a low-viscosity resin [9]. However, no study has been conducted on the efficacy of Cobalt infiltration resin for treatment of WSLs. Thus, this study aimed to spectrophotometrically compare the color change (ΔE) of WSLs after the application of ICON and Cobalt resin infiltrants. The null hypothesis of the study was that the ΔE of WSLs would not be significantly different following the application of ICON and Cobalt resin infiltrants.
Materials and Methods
This in vitro experimental study was conducted on sound human premolars with intact buccal surfaces, no caries, no microcracks, no staining, no hypoplastic lesions, no enamel structural defects, and no WSLs, as ensured by inspection under a light stereomicroscope (SMZ, Nikon, Japan) at x10 magnification [10]. The teeth had been extracted for orthodontic purposes within the past 6 months. Teeth with attrition, erosion, history of root canal treatment, developmental defects, or history of treatment with chemical agents were excluded [7]. The study protocol was approved by the ethics committee of the Islamic Azad University, School of Dentistry, Tehran, Iran (IR.IAU.DENTAL.REC. 1403.088).
Sample size:
The sample size was calculated to be 10 in each group according to a study by Nagib et al, [1] and assuming α=0.05, β=0.2, and mean standard deviation of ΔE=0.72 to find a significant difference in ΔE equal to 1 unit using two-sample t-test power analysis of PASS 11.
Specimen preparation:
The collected teeth were rinsed with distilled water to eliminate soft tissue debris and blood, and were then stored in 1% thymol (Sigma Aldrich, Merck, Germany) solution for 48 hours for disinfection. They were then stored in saline until the experiment, and the solution was refreshed daily [7]. To simplify assessment of buccal surface, the teeth were vertically mounted in gypsum molds such that the entire tooth crown and 2 mm of the root below the cementoenamel junction remained exposed out of the gypsum (Type II; Asia Shimi Teb, Iran) [10]. The teeth were then polished with a white polishing cup (Tribest, China) and fluoride-free and oil-free pumice powder (Nik Darman, Iran) with a low-speed handpiece (SG20; NSK, Japan) under running water [10].
Assessment of tooth color:
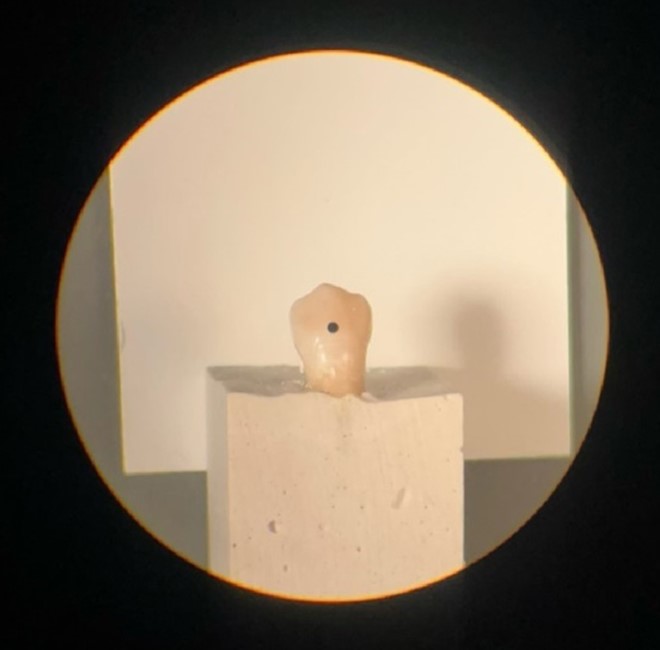
After polishing, tooth color was measured (T0) by a spectrophotometer (Model: CS-2000; Konica Minolta, Japan) using the CIEL*a*b* color system. A piece of non-fluorescent white Leneta paper (Leneta Co., USA) was used in the background as instructed by the manufacturer. The specimens were fixed on the jig, and a homogenous 20 W tungsten light source (Pars Shahab, Iran) illuminated the surface at a 45-degree angle relative to the longitudinal tooth axis. The spectrophotometer was positioned at 0-degree angle relative to the longitudinal tooth axis at 70 cm distance with 0.01-degree viewing angle. This adjustment created a circle with approximate diameter of 1.2 mm at the center of each specimen [11]. The spectrophotometer was calibrated prior to color measurement of each specimen, and the color of specimens was measured at the center of the middle third of the tooth surface at three points (Figure 1). The mean of the three values was calculated and reported.
Figure 1. Color measurement at the center of the middle third of the buccal surface at T0 (before any intervention)
Then, to standardize the experimental condi-tions, the cervical and coronal thirds of the teeth were covered with adhesive tape to create WSLs in their middle third. The specimens were then immersed in a demineralizing solution (2.2 mM CaCl2, 2.2 mM NaH2PO4, and 0.05 M acetic acid) with a pH of 4.4 for 7 days to induce WSLs [12]. This solution was stored at 4°C and brought to 37°C to simulate the oral environment before use. Also, the solution was changed every day to maintain a constant pH. The specimens were examined regularly every day until a frosty white appearance appeared [13]. After the induction of WSLs, color assessment was repeated (T1) as explained for T0. The teeth were then randomly assigned to two groups using a table of random numbers:
Group 1: Treatment with ICON resin infiltrant (DMG, Hamburg, Germany): After cleaning, the teeth were first etched with ICON Etch (DMG, Hamburg, Germany) containing 15% hydrochloric acid, for 2 minutes. After rinsing for 30 seconds and drying, Icon Dry (99% ethanol; DMG, Hamburg, Germany) was applied on the surface for 30 seconds and dried after careful visual inspection. Then, the operator light was turned off, and resin infiltrant (DMG, Hamburg, Germany) was applied for 3 minutes. After spreading the resin with air spray, the specimens were cured for 40 seconds using a LED.D curing unit (Woodpecker, China), and then resin was applied again and cured for 40 seconds. Finally, polishing was performed using Sof-Lex discs (3M, St. Paul, USA) [8].
Group 2: Treatment with Cobalt resin infiltrant (Biomed, Tehran, Iran): According to the manufacturer's instructions, the teeth were first cleaned and etched. Then, Cobalt Etch (Biomed, Tehran, Iran) was applied on the surface for 2 minutes. It was then rinsed for 30 seconds and dried with air spray. Next, Cobalt Dry (99% ethanol; Biomed, Tehran, Iran) was applied to the tooth surface for 30 seconds. If the white opaque lesions were significantly reduced, the next step was performed; otherwise, the steps were repeated from the beginning. Subsequently, Cobalt resin (Biomed, Tehran, Iran) was applied to the surface and left for 3 minutes. After spreading the resin with air spray and re-applying it, it was cured for 40 seconds using a LED.D curing unit (Woodpecker, China) and finally polished using Sof-Lex discs (3M, St. Paul, USA) [14]. The constituents of the two resin infiltrants are presented in Table 1. The color of the specimens was measured again spectrophotometrically for the third time (T2), immediately after applying the infiltration resin, as mentioned for the previous steps. After treatment, the specimens were stored for 4 weeks in artificial saliva (manufactured by Tehran University of Medical Sciences) containing 1.5 mmol/L Ca, 0.9 mmol/L P, 150 mmol/L KCl, and 0.05 mg F/mL in 0.1 mol/L Tris buffer, with a pH of 7.0 at 37°C to simulate the oral environment. The solution was changed daily [15]. The color of the specimens was then measured again for the fourth time (T3) with a spectrophotometer as explained earlier.
For each specimen, color evaluation was performed at four stages: before the intervention (T0), after demineralization (T1), immediately after treatment (T2), and 4 weeks after treatment (T3) (Figure 2). Color parameters were measured using the CIEL*a*b* color system, and ΔE was calculated according to the formula: ΔE*Lab =[(ΔL2)+(Δa2)+(Δb2)]½ [16].
In this formula, L* indicates lightness, a* indicates redness-greenness, and b* indicates yellowness-blueness [16].
Sample size:
The sample size was calculated to be 10 in each group according to a study by Nagib et al, [1] and assuming α=0.05, β=0.2, and mean standard deviation of ΔE=0.72 to find a significant difference in ΔE equal to 1 unit using two-sample t-test power analysis of PASS 11.
Specimen preparation:
The collected teeth were rinsed with distilled water to eliminate soft tissue debris and blood, and were then stored in 1% thymol (Sigma Aldrich, Merck, Germany) solution for 48 hours for disinfection. They were then stored in saline until the experiment, and the solution was refreshed daily [7]. To simplify assessment of buccal surface, the teeth were vertically mounted in gypsum molds such that the entire tooth crown and 2 mm of the root below the cementoenamel junction remained exposed out of the gypsum (Type II; Asia Shimi Teb, Iran) [10]. The teeth were then polished with a white polishing cup (Tribest, China) and fluoride-free and oil-free pumice powder (Nik Darman, Iran) with a low-speed handpiece (SG20; NSK, Japan) under running water [10].
Assessment of tooth color:
After polishing, tooth color was measured (T0) by a spectrophotometer (Model: CS-2000; Konica Minolta, Japan) using the CIEL*a*b* color system. A piece of non-fluorescent white Leneta paper (Leneta Co., USA) was used in the background as instructed by the manufacturer. The specimens were fixed on the jig, and a homogenous 20 W tungsten light source (Pars Shahab, Iran) illuminated the surface at a 45-degree angle relative to the longitudinal tooth axis. The spectrophotometer was positioned at 0-degree angle relative to the longitudinal tooth axis at 70 cm distance with 0.01-degree viewing angle. This adjustment created a circle with approximate diameter of 1.2 mm at the center of each specimen [11]. The spectrophotometer was calibrated prior to color measurement of each specimen, and the color of specimens was measured at the center of the middle third of the tooth surface at three points (Figure 1). The mean of the three values was calculated and reported.
Figure 1. Color measurement at the center of the middle third of the buccal surface at T0 (before any intervention)
{kind=link}
Then, to standardize the experimental condi-tions, the cervical and coronal thirds of the teeth were covered with adhesive tape to create WSLs in their middle third. The specimens were then immersed in a demineralizing solution (2.2 mM CaCl2, 2.2 mM NaH2PO4, and 0.05 M acetic acid) with a pH of 4.4 for 7 days to induce WSLs [12]. This solution was stored at 4°C and brought to 37°C to simulate the oral environment before use. Also, the solution was changed every day to maintain a constant pH. The specimens were examined regularly every day until a frosty white appearance appeared [13]. After the induction of WSLs, color assessment was repeated (T1) as explained for T0. The teeth were then randomly assigned to two groups using a table of random numbers:
Group 1: Treatment with ICON resin infiltrant (DMG, Hamburg, Germany): After cleaning, the teeth were first etched with ICON Etch (DMG, Hamburg, Germany) containing 15% hydrochloric acid, for 2 minutes. After rinsing for 30 seconds and drying, Icon Dry (99% ethanol; DMG, Hamburg, Germany) was applied on the surface for 30 seconds and dried after careful visual inspection. Then, the operator light was turned off, and resin infiltrant (DMG, Hamburg, Germany) was applied for 3 minutes. After spreading the resin with air spray, the specimens were cured for 40 seconds using a LED.D curing unit (Woodpecker, China), and then resin was applied again and cured for 40 seconds. Finally, polishing was performed using Sof-Lex discs (3M, St. Paul, USA) [8].
Group 2: Treatment with Cobalt resin infiltrant (Biomed, Tehran, Iran): According to the manufacturer's instructions, the teeth were first cleaned and etched. Then, Cobalt Etch (Biomed, Tehran, Iran) was applied on the surface for 2 minutes. It was then rinsed for 30 seconds and dried with air spray. Next, Cobalt Dry (99% ethanol; Biomed, Tehran, Iran) was applied to the tooth surface for 30 seconds. If the white opaque lesions were significantly reduced, the next step was performed; otherwise, the steps were repeated from the beginning. Subsequently, Cobalt resin (Biomed, Tehran, Iran) was applied to the surface and left for 3 minutes. After spreading the resin with air spray and re-applying it, it was cured for 40 seconds using a LED.D curing unit (Woodpecker, China) and finally polished using Sof-Lex discs (3M, St. Paul, USA) [14]. The constituents of the two resin infiltrants are presented in Table 1. The color of the specimens was measured again spectrophotometrically for the third time (T2), immediately after applying the infiltration resin, as mentioned for the previous steps. After treatment, the specimens were stored for 4 weeks in artificial saliva (manufactured by Tehran University of Medical Sciences) containing 1.5 mmol/L Ca, 0.9 mmol/L P, 150 mmol/L KCl, and 0.05 mg F/mL in 0.1 mol/L Tris buffer, with a pH of 7.0 at 37°C to simulate the oral environment. The solution was changed daily [15]. The color of the specimens was then measured again for the fourth time (T3) with a spectrophotometer as explained earlier.
For each specimen, color evaluation was performed at four stages: before the intervention (T0), after demineralization (T1), immediately after treatment (T2), and 4 weeks after treatment (T3) (Figure 2). Color parameters were measured using the CIEL*a*b* color system, and ΔE was calculated according to the formula: ΔE*Lab =[(ΔL2)+(Δa2)+(Δb2)]½ [16].
In this formula, L* indicates lightness, a* indicates redness-greenness, and b* indicates yellowness-blueness [16].
Figure 2. Color change during T0-T3 in the (up) Icon, and (down) cobalt groups
Statistical analysis:
To reduce measurement error, the color was measured at three points on each tooth, and the mean value was calculated. Due to the normal distribution of data as confirmed by the Shapiro-Wilk test, ΔE was compared between the two study groups at different time points using independent t-test. All statistical analyses were performed using SPSS version 24 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
{kind=link}
Statistical analysis:
To reduce measurement error, the color was measured at three points on each tooth, and the mean value was calculated. Due to the normal distribution of data as confirmed by the Shapiro-Wilk test, ΔE was compared between the two study groups at different time points using independent t-test. All statistical analyses were performed using SPSS version 24 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
Table 2 presents the measures of central dispersion for different ΔE values in the two groups. As shown, the two groups had no significant difference in ΔE1-0 (P=0.100), ΔE2-0 (P=0.234), ΔE3-0 (P=0.388), and ΔE3-2 (P=0.667). However, ΔE2-1 (P=0.004) and ΔE3-1 (P=0.012) of ICON were significantly higher than the corresponding values for Cobalt.
Discussion
Discussion
This study spectrophotometrically compared the ΔE of WSLs after the application of ICON and Cobalt resin infiltrants. The results showed that ΔE2-1 and ΔE3-1 of ICON were significantly higher than the corresponding values for Cobalt, but no other significant differences were found. Thus, the null hypothesis of the study was partially accepted and partially rejected.
Resin infiltration aims to stop the progression of WSLs and improve the appearance of the enamel. First, the hypermineralized layer is removed by etching the surface with hydrochloric acid to provide access to the demineralized area. The resin infiltrant then penetrates the porous enamel by the capillary action, and this process causes the refractive index of the demineralized area to match that of sound enamel, ultimately reducing light scattering and improving the white, opaque appearance of the lesion. This method not only improves the color and appearance of the enamel but also acts as a physical barrier against the progression of the lesion [16]. Despite the effectiveness of this method, various materials are available under different brand names, and it is important to compare their performance in various aspects (including color masking ability and color stability over time).
Resin infiltration aims to stop the progression of WSLs and improve the appearance of the enamel. First, the hypermineralized layer is removed by etching the surface with hydrochloric acid to provide access to the demineralized area. The resin infiltrant then penetrates the porous enamel by the capillary action, and this process causes the refractive index of the demineralized area to match that of sound enamel, ultimately reducing light scattering and improving the white, opaque appearance of the lesion. This method not only improves the color and appearance of the enamel but also acts as a physical barrier against the progression of the lesion [16]. Despite the effectiveness of this method, various materials are available under different brand names, and it is important to compare their performance in various aspects (including color masking ability and color stability over time).
Table 1. Components of the resin infiltration kit in the two groups
{kind=link}
Table 2. Measures of central dispersion for different ΔE values in the two groups (n=10)
{kind=link}
Regarding the comparison of ΔE1-0 [sound state (T0) to after the induction of WSLs (T1)], the mean ΔE was 12.37±5.57 for ICON and 3.84±8.66 for Cobalt. According to Dogra et al, [8] ΔE=3.7 is considered the threshold for clinical detection, meaning that ΔE values greater than 3.7 are clinically visible to patients and dentists, and may require color correction and restoration. Accordingly, in both study groups, WSLs were clinically visible and did not differ significantly (P=0.100).
Based on the present results, in the comparison of ΔE2-0, ICON infiltration resin with a mean ΔE value of 3.44 showed superior color coverage than Cobalt infiltration resin with a mean ΔE value of 4.73 although this difference was not statistically significant. This result was consistent with the findings of Dogra et al [8]. They compared ΔE in WSLs caused by fluorosis before and after treatment with ICON resin infiltrant using a spectrophotometer, and reported that ΔE was less than 3.7, indicating no color difference visible to the naked eye. Also, comparison of ΔE2-1 indicated significant superiority of ICON with a mean ΔE of 12.78 compared to Cobalt with a mean ΔE of 7.25; this significant superiority can be explained by the fact that after applying Cobalt, WSLs were visually visible to some extent, but after applying ICON, WSLs were not visually visible; indicating that ICON was able to create a significant color coverage compared to Cobalt. This result was somewhat consistent with the findings of Prasada et al [7]. They compared the efficacy of ICON resin infiltrant to bioactive glass and NaF to improve the esthetic appearance of WSLs. They reported that ICON caused the greatest improvement in color of WSLs compared to bioactive glass and NaF. Also, Hammad et al. [5] evaluated the ΔE and color stability of ICON in treatment of WSLs, compared to nano-hydroxyapatite toothpaste and microabrasion. They indicated the superiority of ICON over microabrasion and nano-hydroxyapatite for color improvement of WSLs. Also, Nagib et al. [1] compared the ΔE of WSLs using three treatment approaches: resin infiltration, bleaching, and microabrasion, and reported that ICON alone provided less color coverage than combined methods such as bleaching + ICON. The reason for color improvement of WSLs after bleaching with ICON is attributed to the fact that bleaching removes pigments and then the resin infiltrant blocks the pores in WSLs.
Comparison of the stability of color coverage from immediately after treatment (T2) to 4 weeks later (T3) indicated that ICON with a mean ΔE of 4.79 had a greater color stability than Cobalt with a mean ΔE of 5.24. However, this difference was not statistically significant indicating that the two resin infiltrants had a relatively similar stability during this time period. In line with the present results, Zaazou et al. [17] evaluated the effect of ICON resin infiltrant on ΔE of WSLs during the follow-up periods of 3, 6 and 12 months in a clinical study, and showed that although color coating of lesions was initially significant, there was a slight decrease in color stability over time and further evaluation is needed to investigate the durability of its long-term effects. Based on a study by Schoppmeier et al. [18], the TEGDEMA present in the composition of resin infiltrant has the potential for color change due to its tendency to absorb water. Schoppmeier et al. [18] showed that office or home bleaching led to improvement of the color of infiltrated WSLs to their baseline shade after treatment. In the present study, a significant change in color stability was not observed, probably due to the short follow-up of 4 weeks. On the other hand, the significant difference in ΔE1-3 and ΔE1-2 may be attributed to the difference in the viscosity of the etching acid between the two groups, such that the lower viscosity of the etchant in the ICON resin infiltration kit leads to better surface wettability, improved penetration into the depth of the porosities, and consequently, enhanced color and esthetic improvement of WSLs. According to a study by Al-Saeed et al. [19], the viscosity of the etchant can indeed influence the depth of penetration of resin infiltrant; lower-viscosity acids spread easily and penetrate more uniformly into the enamel surface, and penetration coefficient of resin infiltrant is strongly dependent on the permeability of the lesion surface.
Although this study was the first to assess the efficacy of Cobalt resin infiltrant for color correction of WSLs, it had some limitations as well. The study was conducted in vitro, and lacked the complexities of the oral environment (such as alterations in pH, temperature, bacterial flora, and diet), which may affect the generalizability of the results to clinical settings. Also, the 4-week follow-up period was short, and the long-term stability of color coverage was not evaluated. Clinical studies with longer follow-ups (more than 6 months) are required to investigate the stability of color coverage in real oral conditions.
Conclusion
The results of this study showed that both ICON and Cobalt effectively corrected the color of WSLs to match the color of sound enamel, although ICON showed a slightly superior performance. The two resin infiltrants also had a comparable color stability after 4 weeks.
Type of Study: Original article |
Subject:
pediatric
References
1. Nagib T, Yassa M, Elheeny A. Spectrophotometric evaluation of color change of white spot lesions treated with three different approaches: an in vitro study. Egypt Dent J. 2023 Oct;69:2549-54. [DOI:10.21608/edj.2023.215807.2583]
2. Aref NS, Alrasheed MK. Casein phosphopeptide amorphous calcium phosphate and universal adhesive resin as a complementary approach for management of white spot lesions: an in-vitro study. Prog Orthod. 2022 Mar;23(1):10. [DOI:10.1186/s40510-022-00404-9] [PMID] [PMCID]
3. Sulieman M. An overview of tooth discoloration: extrinsic, intrinsic and internalized stains. Dent Update. 2005 Oct;32(8):463-4, 6-8, 71. [DOI:10.12968/denu.2005.32.8.463] [PMID]
4. Khoroushi M, Kachuie M. Prevention and treatment of white spot lesions in orthodontic patients. Contemp Clin Dent. 2017 Jan;8(1):11-9. [DOI:10.4103/ccd.ccd_216_17] [PMID] [PMCID]
5. Hammad SM, El-Wassefy NA, Alsayed MA. Evaluation of color changes of white spot lesions treated with three different treatment approaches: an in-vitro study. Dent Press J Orthod. 2020;25(1):26-7. [DOI:10.1590/2177-6709.25.1.27.e1-7.onl] [PMID] [PMCID]
6. Ballard RW, Hagan JL, Phaup AN, Sarkar N, Townsend JA, Armbruster PC. Evaluation of three commercially available materials for resolution of white spot lesions. Am J Orthod Dentofacial Orthop. 2013 Apr;143(4 Suppl):S78-84. [DOI:10.1016/j.ajodo.2012.08.020] [PMID]
7. Prasada KL, Penta PK, Ramya KM. Spectrophotometric evaluation of white spot lesion treatment using novel resin infiltration material (ICON®). J Conserv Dent. 2018 Sep;21(5):531-5. [DOI:10.4103/JCD.JCD_52_18] [PMID] [PMCID]
8. Dogra S, Goyal V, Gupta A, Joshi S, Kataria V, Saini J, et al. Spectrophotometric evaluation of color change in tooth enamel defects using resin infiltrate: an in vivo study. Int J Clin Pediatr Dent. 2020 Mar;13(2):150-4. [DOI:10.5005/jp-journals-10005-1727] [PMID] [PMCID]
9. Puleio F, Fiorillo L, Gorassini F, Iandolo A, Meto A, D'Amico C, et al. Systematic review on white spot lesions treatments. Eur J Dent. 2022 Feb;16(1):41-8. [DOI:10.1055/s-0041-1731931] [PMID] [PMCID]
10. Mohamed B, Marzouk ES, Zaher AR. Spectrophotometric evaluation of different protocols of resin infiltration of white spot lesions with various depths. Egypt Orthod J. 2017 Dec;52:31-44. [DOI:10.21608/eos.2017.78356]
11. Rafiee A, Memarpour M, Benam H. Evaluation of bleaching agent effects on color and microhardness change of silver diamine fluoride-treated demineralized primary tooth enamel: An in vitro study. BMC Oral Health. 2022 Aug;22(1):1-9. [DOI:10.1186/s12903-022-02371-3] [PMID] [PMCID]
12. Ozgul BM, Orhan K, Oz FT. Micro-computed tomographic analysis of progression of artificial enamel lesions in primary and permanent teeth after resin infiltration. J Oral Sci. 2015;57(3):177-83. [DOI:10.2334/josnusd.57.177] [PMID]
13. Hannig M, Hannig C. Nanobiomaterials in preventive dentistry. In: Subramani K, Ahmed W, editors. Nanobiomaterials in Clinical Dentistry. 2nd ed. Amsterdam: Elsevier; 2019. p. 201-2. [DOI:10.1016/B978-0-12-815886-9.00008-5]
14. Instructions for using the Cobalt Infiltrant Resin Kit [Internet]. Available from: https://cobalt-biomed.ir/ifu-resin-infiltrant/
15. Alexandria AK, Vieira TI, Pithon MM, da Silva Fidalgo TK, Fonseca-Gonçalves A, Valença AMG, et al. In vitro enamel erosion and abrasion-inhibiting effect of different fluoride varnishes. Arch Oral Biol. 2017 May;77:39-43. [DOI:10.1016/j.archoralbio.2017.01.010] [PMID]
16. Gousalya V, Prabu D, Dhamodhar D, Bharathwaj VV, Sindhu R, Elakiya S. Systematic review on the efficacy of Icon resin infiltration on white spot lesions. Indian J Contemp Dent. 2023;11(1):18-24. [DOI:10.37506/ijocd.v11i1.18813]
17. Zaazou MH, Saleh RS, Hassan SN, Abdelnabi A, Zaki ZM, Hamdy TM, et al. Effectiveness of low-viscosity resin infiltration (Icon) on color change of enamel white spot lesions: 1-year follow-up clinical study. Bull Natl Res Cent. 2024 Jun;48(1):62. [DOI:10.1186/s42269-024-01219-w]
18. Schoppmeier CM, von Kohout M, Sun L, Janson M, Deeg I, Barbe AG, et al. Influence of home or in-office tooth bleaching on the color stability of white-spot lesions after resin infiltration: An in vitro comparison. J Am Dent Assoc D. 2025 Jul;156(7):517-29. [DOI:10.1016/j.adaj.2025.04.009] [PMID]
19. Al-Saeed EJ, AlMarhoon ZW, Al-Eid ZA, AlAhmari TA, AlJamed SH, AlSarhan R, et al. Properties, success, and applications of resin infiltration for minimal invasive restoration: A scoping review. Arch Pharm Pract. 2022;13(2-2022):110-5. [DOI:10.51847/nABHjPaqO7]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |