Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 2 (6-2024)
J Res Dent Maxillofac Sci 2024, 9(2): 117-123 |
Back to browse issues page

Ethics code: IR.KMUS.REC.1400.836.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mafi S, Ghahremani F, Rahmani M, Alaee A. Validity and Reliability of the Persian Version of the Graded Chronic Pain Scale 2.0 for Determination of TMJ Pain. J Res Dent Maxillofac Sci 2024; 9 (2) :117-123
URL: http://jrdms.dentaliau.ac.ir/article-1-543-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-543-en.html



1- Oral Medicine Department, Islamic Azad University, Dental Branch, Tehran Iran.
2- Private Dentistry Practice, Kermanshah, Iran.
3- Oral Medicine Specialist, Kermanshah, Iran.
4- Oral Medicine Department, Dental Material Research Center, Islamic Azad University, Dental Branch, Tehran Iran. ,arezoo.alaee@yahoo.com
2- Private Dentistry Practice, Kermanshah, Iran.
3- Oral Medicine Specialist, Kermanshah, Iran.
4- Oral Medicine Department, Dental Material Research Center, Islamic Azad University, Dental Branch, Tehran Iran. ,
Keywords: Chronic pain, Facial pain, Pain measurement, Temporomandibular joint disorders, Reproducibility of results
Full-Text [PDF 323 kb]
(909 Downloads)
| Abstract (HTML) (2541 Views)
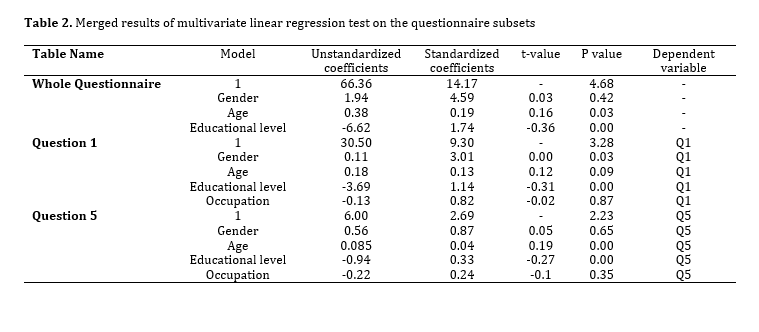
Table 2. Merged results of multivariate linear regression test on the questionnaire subsets
Hietaharju et al. [8] compared the suitability of GCPS versions 1.0 and 2.0 for biopsychosocial screening and subtyping of Finnish tertiary care referral patients with TMD pain. They reported that the distribution of TMD patients in both the questionnaire groups was the same, and the GCPS 2.0 could be regarded as a suitable initial screening tool for adjunct personalized or comprehensive multidisciplinary assessment.
Tanti and colleagues [4] examined the validity of GCPS 2.0 in an Indonesian population and found that it had appropriate validity, similar to its Persian version. The questionnaire was also investigated for validity in some other studies and found to have excellent validity, comparable to its Persian version [12,13].
Tanti and colleagues [4] reported an ICC of 0.79. The ICC value was 0.96 in a study by González and colleagues [14], and 0.81 in a study by Ferrer-Peña and colleagues [10]. These results indicate the appropriate reliability of this questionnaire in various studies.
Von Korff et al. [15] showed that due to easy use and speed, the number of questions can be reduced to 5 (questions 2 to 6) with sufficient validity and reliability, making it a modified version. Tedin et al. [16] showed the optimal validity and reliability of the Malay version of this questionnaire. In terms of validity in the present study, the KMO test result was 0.85, indicating adequacy of the sample size, and the significant result of the Bartlett test showed that the data in this study had the potential to become a factor [16]. These results were consistent with those of Ferrer-Peña and colleagues [10]. In their study, the KMO was 0.82, and the Bartlett test result was significant [10].
In the present study, after examining the correlation between the questions, it was found that questions 2 to 4, and 6 to 8 were correlated and placed in one factor, but questions 1 and 5 were different from other questions. After removing these two questions from the questionnaire, the questionnaire with the remaining 6 questions showed relatively high reliability and a higher Cronbach's alpha coefficient. However, since questions 1 and 5 have been added to the questionnaire to evaluate pain persistence and disability levels in past assessments, they cannot be removed from the questionnaire and should be examined separately from other questions. Similar conditions were reported by Ferrer-Peña et al. [10]. In their study, questions 2 to 4 were placed in one factor, questions 5 to 8 were placed in another factor, and question 1 did not appear in any of the main factors. According to the authors, question 1 had been added to the original questionnaire (English version) to evaluate pain persistence in past studies; thus, it should not be removed from the questionnaire. The Spanish version of this questionnaire also has 8 questions, similar to the original version [10].
The present study found that educational level had a significant direct correlation with the questionnaire score. The questionnaire score was also found to have a significant correlation with age. However, age was only significantly associated with the number of disability episodes. The questionnaire score was lower in males than females, but this difference was not statistically significant. These results were consistent with those of Salaffi and colleagues [17]. Age was only significantly associated with disability due to pain. In their study, the pain score was also reported to be lower in males than females, but this difference was significant. This difference may be attributed to the sample size and the reported location of pain.
Agha-Hosseini et al. [7] evaluated the correlation of bruxism with lumbar pain in an Iranian population. The patients were provided with instructions on how to discontinue their parafunctional habits including clenching and bruxism. The Helkimo and Rolland Morris questionnaires were used to assess TMDs and lower back pain in their study. The mean severity score of TMD significantly decreased after the intervention. Following treatment of TMDs, the mean severity score of lumbar pain significantly decreased from 8 to 2 [7]. The questionnaire used in their study was different from that used in the present study.
Gębska et al. [3] evaluated the prevalence of headache in TMD patients, using the Research Diagnostic Criteria for TMDs while the standardized short-form of the McGill Pain Questionnaire was used to qualitatively and quantitatively assess headaches. The participants with TMD reported the occurrence of headache significantly more than others, and it was associated with a pressing pain in the majority of patients (r = 0.82) and a cutting pain in a small percentage of patients (r=0.30). Neck and shoulder girdle pain and clenching and/or grinding of teeth were significantly more common among those who declared headache than those without headache. The results obtained so far may indicate a significant relationship between headache and TMDs [3].
This study was conducted on a homogeneous population in terms of social and educational status. Also, this study was the first to translate GCPS 2.0 to Persian for clinical applications.
Conclusion
The Persian version of the GCPS 2.0 with omission of questions 1 and 5 can be used to assess chronic pain in the TMJ area in the Iranian population.
Full-Text: (880 Views)
Abstract
Background and Aim: The Graded Chronic Pain Scale version 2.0 (GCPS 2.0) has no Persian version for use on the Iranian population. Thus, this study aimed to validate the Persian version of this scale.
Materials and Methods: The cross-sectional study was conducted on 160 patients with chronic pain who filled out the GCPS 2.0. The 8-item self-report GCPS 2.0 was first translated to Persian. The validity of its Persian version was examined by a group of 7 expert specialists and calculation of the content validity index. The test-retest method was used to measure the reliability of the Persian version of GCPS 2.0. The Bartlett's test, KMO index, and exploratory factor analysis were used to confirm its construct validity. The internal consistency of the questions was analyzed by calculation of Cronbach's alpha coefficient and item-scale correlation coefficient, and retesting. The relationship between the questionnaire score and demographic information of the participants was analyzed (alpha=0.05).
Results: The content validity coefficient was 0.98. The test-retest coefficient was 0.98, indicating high reliability of the questionnaire. The mean age of the participants was 38 years, and 81 (50.6%) were males. Education was found to have a significant correlation with the total questionnaire score (P<0.05) but age had no such correlation (P>0.05).
Conclusion: The Persian version of the GCPS 2.0 with the omission of questions 1 and 5 may be used for assessment of chronic pain in the temporomandibular joint (TMJ) area in the Iranian population.
Keywords: Chronic pain; Facial pain; Pain measurement; Temporomandibular joint disorders; Reproducibility of results
Introduction
Chronic orofacial pain disorders manifest a complex of non-specific symptoms such as dental pain or temporomandibular disorders (TMDs). Patients with such disorders often seek dental consultation at first and resultantly, may undergo unnecessary dental procedures. Patients that seek medical consultation from medical practitioners and neurosurgical services are also often misdiagnosed. Delay in achieving an accurate diagnosis and effective treatment increases the healthcare costs and negatively affects the quality of life of patients [1].
The temporomandibular joint (TMJ) plays an important role in dental occlusion and the neuromuscular system [2]. TMDs include a wide range of clinical symptoms [1,3,4]. Based on a report by the World Health Organization, TMDs are the 3rd most common dental conditions after dental caries and periodontal disease. TMDs affect 5% to 12% of the world’s population. Some studies have reported a higher prevalence rate of up to 25% and 33–40% in the general population [4-7]. TMDs include a series of signs and symptoms in the TMJ or the muscles of mastication, causing discomfort and concerns for patients [4-7].
The Diagnostic Criteria for TMDs Axis I and II were developed to identify both physical and psychosocial factors that may contribute to patient symptoms [4,6,8-11]. Graded Chronic Pain Scale 2.0 (GCPS 2.0), is an 8-item scale that evaluates the severity of chronic pain, presence of persistent pain, and degree of disability. It is an initial screening tool for adjunct personalized or comprehensive multidisciplinary assessment [4,9]. The aim of this study was to translate the GCPS 2.0 into Persian and assess the validity and reliability of the Persian version of this questionnaire for use on the Iranian population.
Materials and Methods
The population of this cross-sectional study included all patients presenting to Kermanshah Dental School complaining of chronic pain. A sample size of 160 individuals was selected based on calculation of 20 individuals per each item of the questionnaire. The sampling method was non-probability convenience sampling. This study was approved by the ethics committee of Kermanshah University of Medical Sciences (IR.KMUS.REC.1400.836). Written informed consent was obtained from all participants.
The inclusion criteria were Iranians with Persian as their native language, age between 18 to 70 years, suffering from chronic pain in the TMJ or head and face region for more than 3 months, and willingness for participation in the study [9].
The standard English version of GCPS 2.0 was used [6]. It has 8 questions. Questions 1 to 6 estimate the severity of chronic pain and questions 7 and 8 estimate the level of disability using a Likert scale. It was translated to Persian and then the translated version was back-translated to English by an expert English translator who was unaware of the research objectives. Finally, the final version was prepared in Persian.
To validate the content validity of the questionnaire, the content validity index was calculated. A group of 7 experts reviewed the questionnaire by rating the appropriateness of each question using a four-part scale: irrelevant, needs fundamental revision, relevant but needs revision, completely relevant. The number of experts who selected options 3 and 4 was divided by the total number of experts. The content validity index was calculated to be 98.0, which was acceptable. Next, the questionnaire was completed by 30 patients twice with a 2-week interval, and the intraclass correlation coefficient (ICC) was calculated. The ICC in test-retest reliability analysis showed very good reliability (98.0).
The Bartlett's test, the KMO index, and the principal axis factoring were used to confirm the structural validity of the questionnaire. The closer the KMO value to one, the more desirable it would be. In the Bartlett’s test, if the P value is less than 0.05, the data's suitability for factor transformation is confirmed. The internal consistency of the questions was also analyzed using the Cronbach's alpha coefficient, item-scale correlation coefficient, and test-retest analysis.
Questions 2, 3, 4, 6, 7, and 8 were scored between 0 and 10. Questions 1 and 5, which indicate the number of days, could receive any score. The total score of the questionnaire was the sum of all scores given to the questions. The internal consistency and exploratory factor analysis revealed P=0.07 for questions 1 and 2 and P=0.00 for all other questions.
The Q square test and t-test were used to assess the relationship between the questionnaire scores and demographic information. Linear regression analysis was applied for data analysis using SPSS version 26 with a significance level of 0.05.
Results
The results showed that most of the questions had a correlation between 0.3 and 0.9 except questions 1 and 2. In addition, all P values were significant (P<0.05), except for questions 1 and 2 (P = 0.072). A KMO value of 0.6 was weak but acceptable as a factor suitability index.
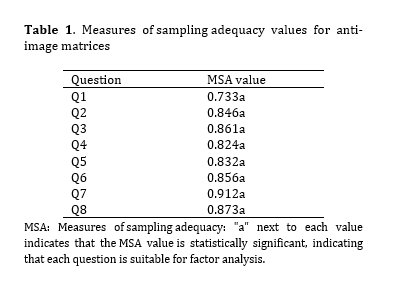
The Kaiser-Meyer-Olkin sample suitability index was 0.85. Also, for the Bartlett statistic, the value was 1008.574 (P<0.05). Table 1 shows the sample adequacy measures of the correlation matrix. All measures were greater than 0.6, indicating good correlation between all questions.
It was determined that the questionnaire was factorable, and all coefficients were greater than 0.25. In fact, the commonality of each variable, which represents the proportion of variance in each variable accounted for by the common factors, was calculated. In the next stage, questions were entered into the analysis without assumptions, and the software considered two factors. Based on the extracted eigenvalues of two factors, the first factor alone accounted for 59.7% of the variance, and the second factor accounted for 9.1% of the variance. The total extracted factors accounted for 69.0% of the variance. According to the factor coefficients, the first factor was identified as the most important factor with a coefficient of 0.65, and the second factor was 0.57.
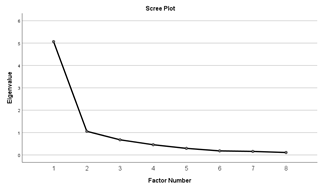
In Figure 1, the eigenvalues for each factor are shown in the scree plot. This plot displays the eigenvalue of each extracted component, starting from the largest eigenvalue, and is always a descending plot.
Table 1. Measures of sampling adequacy values for anti-image matrices
Figure 1. Scree plot for the 8 items of the Persian version of GCPS 2.0
Each question that had a higher correlation with one of the factors was placed in the respective factor. Among the 8 questions, questions 1 and 5 were placed in a separate factor from the other questions, even though they did not have a significant correlation with the first factor. This indicates the difference between these two questions compared to other questions.
The questionnaire was first examined as one factor with all questions. Then, the first factor (excluding questions 1 and 5) and finally, the second factor (questions 1 and 5) were examined separately. The Cronbach's alpha coefficient was calculated for the entire questionnaire (0.60), the first factor (0.91), and the second factor (0.52). It was concluded that the translated version of the questionnaire was valid and reliable after removing questions 1 and 5, and these questions had to be examined separately. Therefore, in this questionnaire, questions 1 and 5 had to be removed, and the remaining 6 questions had to be used as a tool for measuring the chronic pain.
The mean and standard deviation of the total questionnaire score were 30.01±1.56. However, the mean score of the questionnaire after removing questions 1 and 5 was 11.60±28.60.
Demographic data:
Of the participants, 81 (50.6%) were males and 79 (49.4%) were females. Also, 69 individuals (43.1%) had a high-school diploma or lower level of education and 91 individuals (56.9%) had a higher educational degree. The age of the participants in this study ranged from 11 to 68 years, with a mean age of 38 years. The t-test showed that gender of the participants had no significant relationship with chronic pain score (P>0.05). Evaluation of the participants in two groups based on their educational level i.e., higher than high-school diploma and high-school diploma or lower, showed a significant relationship between the educational level and chronic pain score (P<0.05). Age of the participants also had a significant relationship with chronic pain score (P<0.05).
A multiple linear regression test was then performed. Analysis of the questionnaire data after removing questions 1 and 5 showed a significant relationship between the educational level and chronic pain score (P=0.00). It means that the higher the educational level of individuals, the lower their chronic pain score was.
As shown in Table 2, a multiple linear regression test was performed for all questionnaire items and it was shown that in addition to education, age also had a significant relationship with chronic pain score (P<0.05). To investigate this correlation, a regression test was separately performed for question 1 and question 5. The results showed that only educational level had a significant relationship with chronic pain score for question 1 (P<0.05), but for question 5, in addition to education, age also had a significant relationship with chronic pain score (P<0.05). It means that the effect of question 5 on the total score of the questionnaire caused age to also have a significant relationship with chronic pain score.
Discussion
The results showed that after omission of questions 1 and 5, the GCPS 2.0 questionnaire showed appropriate validity and reliability for the Iranian population. This questionnaire showed a completely suitable content validity (content validity index=0.98). According to the suggestion of one of the experts, the phrase "pain in the jaw and/or face area" was added to the word "facial pain" to prevent misinterpretation by individuals.
Background and Aim: The Graded Chronic Pain Scale version 2.0 (GCPS 2.0) has no Persian version for use on the Iranian population. Thus, this study aimed to validate the Persian version of this scale.
Materials and Methods: The cross-sectional study was conducted on 160 patients with chronic pain who filled out the GCPS 2.0. The 8-item self-report GCPS 2.0 was first translated to Persian. The validity of its Persian version was examined by a group of 7 expert specialists and calculation of the content validity index. The test-retest method was used to measure the reliability of the Persian version of GCPS 2.0. The Bartlett's test, KMO index, and exploratory factor analysis were used to confirm its construct validity. The internal consistency of the questions was analyzed by calculation of Cronbach's alpha coefficient and item-scale correlation coefficient, and retesting. The relationship between the questionnaire score and demographic information of the participants was analyzed (alpha=0.05).
Results: The content validity coefficient was 0.98. The test-retest coefficient was 0.98, indicating high reliability of the questionnaire. The mean age of the participants was 38 years, and 81 (50.6%) were males. Education was found to have a significant correlation with the total questionnaire score (P<0.05) but age had no such correlation (P>0.05).
Conclusion: The Persian version of the GCPS 2.0 with the omission of questions 1 and 5 may be used for assessment of chronic pain in the temporomandibular joint (TMJ) area in the Iranian population.
Keywords: Chronic pain; Facial pain; Pain measurement; Temporomandibular joint disorders; Reproducibility of results
Introduction
Chronic orofacial pain disorders manifest a complex of non-specific symptoms such as dental pain or temporomandibular disorders (TMDs). Patients with such disorders often seek dental consultation at first and resultantly, may undergo unnecessary dental procedures. Patients that seek medical consultation from medical practitioners and neurosurgical services are also often misdiagnosed. Delay in achieving an accurate diagnosis and effective treatment increases the healthcare costs and negatively affects the quality of life of patients [1].
The temporomandibular joint (TMJ) plays an important role in dental occlusion and the neuromuscular system [2]. TMDs include a wide range of clinical symptoms [1,3,4]. Based on a report by the World Health Organization, TMDs are the 3rd most common dental conditions after dental caries and periodontal disease. TMDs affect 5% to 12% of the world’s population. Some studies have reported a higher prevalence rate of up to 25% and 33–40% in the general population [4-7]. TMDs include a series of signs and symptoms in the TMJ or the muscles of mastication, causing discomfort and concerns for patients [4-7].
The Diagnostic Criteria for TMDs Axis I and II were developed to identify both physical and psychosocial factors that may contribute to patient symptoms [4,6,8-11]. Graded Chronic Pain Scale 2.0 (GCPS 2.0), is an 8-item scale that evaluates the severity of chronic pain, presence of persistent pain, and degree of disability. It is an initial screening tool for adjunct personalized or comprehensive multidisciplinary assessment [4,9]. The aim of this study was to translate the GCPS 2.0 into Persian and assess the validity and reliability of the Persian version of this questionnaire for use on the Iranian population.
Materials and Methods
The population of this cross-sectional study included all patients presenting to Kermanshah Dental School complaining of chronic pain. A sample size of 160 individuals was selected based on calculation of 20 individuals per each item of the questionnaire. The sampling method was non-probability convenience sampling. This study was approved by the ethics committee of Kermanshah University of Medical Sciences (IR.KMUS.REC.1400.836). Written informed consent was obtained from all participants.
The inclusion criteria were Iranians with Persian as their native language, age between 18 to 70 years, suffering from chronic pain in the TMJ or head and face region for more than 3 months, and willingness for participation in the study [9].
The standard English version of GCPS 2.0 was used [6]. It has 8 questions. Questions 1 to 6 estimate the severity of chronic pain and questions 7 and 8 estimate the level of disability using a Likert scale. It was translated to Persian and then the translated version was back-translated to English by an expert English translator who was unaware of the research objectives. Finally, the final version was prepared in Persian.
To validate the content validity of the questionnaire, the content validity index was calculated. A group of 7 experts reviewed the questionnaire by rating the appropriateness of each question using a four-part scale: irrelevant, needs fundamental revision, relevant but needs revision, completely relevant. The number of experts who selected options 3 and 4 was divided by the total number of experts. The content validity index was calculated to be 98.0, which was acceptable. Next, the questionnaire was completed by 30 patients twice with a 2-week interval, and the intraclass correlation coefficient (ICC) was calculated. The ICC in test-retest reliability analysis showed very good reliability (98.0).
The Bartlett's test, the KMO index, and the principal axis factoring were used to confirm the structural validity of the questionnaire. The closer the KMO value to one, the more desirable it would be. In the Bartlett’s test, if the P value is less than 0.05, the data's suitability for factor transformation is confirmed. The internal consistency of the questions was also analyzed using the Cronbach's alpha coefficient, item-scale correlation coefficient, and test-retest analysis.
Questions 2, 3, 4, 6, 7, and 8 were scored between 0 and 10. Questions 1 and 5, which indicate the number of days, could receive any score. The total score of the questionnaire was the sum of all scores given to the questions. The internal consistency and exploratory factor analysis revealed P=0.07 for questions 1 and 2 and P=0.00 for all other questions.
The Q square test and t-test were used to assess the relationship between the questionnaire scores and demographic information. Linear regression analysis was applied for data analysis using SPSS version 26 with a significance level of 0.05.
Results
The results showed that most of the questions had a correlation between 0.3 and 0.9 except questions 1 and 2. In addition, all P values were significant (P<0.05), except for questions 1 and 2 (P = 0.072). A KMO value of 0.6 was weak but acceptable as a factor suitability index.
The Kaiser-Meyer-Olkin sample suitability index was 0.85. Also, for the Bartlett statistic, the value was 1008.574 (P<0.05). Table 1 shows the sample adequacy measures of the correlation matrix. All measures were greater than 0.6, indicating good correlation between all questions.
It was determined that the questionnaire was factorable, and all coefficients were greater than 0.25. In fact, the commonality of each variable, which represents the proportion of variance in each variable accounted for by the common factors, was calculated. In the next stage, questions were entered into the analysis without assumptions, and the software considered two factors. Based on the extracted eigenvalues of two factors, the first factor alone accounted for 59.7% of the variance, and the second factor accounted for 9.1% of the variance. The total extracted factors accounted for 69.0% of the variance. According to the factor coefficients, the first factor was identified as the most important factor with a coefficient of 0.65, and the second factor was 0.57.
In Figure 1, the eigenvalues for each factor are shown in the scree plot. This plot displays the eigenvalue of each extracted component, starting from the largest eigenvalue, and is always a descending plot.
Table 1. Measures of sampling adequacy values for anti-image matrices
{kind=link}
Figure 1. Scree plot for the 8 items of the Persian version of GCPS 2.0
{kind=link}
Each question that had a higher correlation with one of the factors was placed in the respective factor. Among the 8 questions, questions 1 and 5 were placed in a separate factor from the other questions, even though they did not have a significant correlation with the first factor. This indicates the difference between these two questions compared to other questions.
The questionnaire was first examined as one factor with all questions. Then, the first factor (excluding questions 1 and 5) and finally, the second factor (questions 1 and 5) were examined separately. The Cronbach's alpha coefficient was calculated for the entire questionnaire (0.60), the first factor (0.91), and the second factor (0.52). It was concluded that the translated version of the questionnaire was valid and reliable after removing questions 1 and 5, and these questions had to be examined separately. Therefore, in this questionnaire, questions 1 and 5 had to be removed, and the remaining 6 questions had to be used as a tool for measuring the chronic pain.
The mean and standard deviation of the total questionnaire score were 30.01±1.56. However, the mean score of the questionnaire after removing questions 1 and 5 was 11.60±28.60.
Demographic data:
Of the participants, 81 (50.6%) were males and 79 (49.4%) were females. Also, 69 individuals (43.1%) had a high-school diploma or lower level of education and 91 individuals (56.9%) had a higher educational degree. The age of the participants in this study ranged from 11 to 68 years, with a mean age of 38 years. The t-test showed that gender of the participants had no significant relationship with chronic pain score (P>0.05). Evaluation of the participants in two groups based on their educational level i.e., higher than high-school diploma and high-school diploma or lower, showed a significant relationship between the educational level and chronic pain score (P<0.05). Age of the participants also had a significant relationship with chronic pain score (P<0.05).
A multiple linear regression test was then performed. Analysis of the questionnaire data after removing questions 1 and 5 showed a significant relationship between the educational level and chronic pain score (P=0.00). It means that the higher the educational level of individuals, the lower their chronic pain score was.
As shown in Table 2, a multiple linear regression test was performed for all questionnaire items and it was shown that in addition to education, age also had a significant relationship with chronic pain score (P<0.05). To investigate this correlation, a regression test was separately performed for question 1 and question 5. The results showed that only educational level had a significant relationship with chronic pain score for question 1 (P<0.05), but for question 5, in addition to education, age also had a significant relationship with chronic pain score (P<0.05). It means that the effect of question 5 on the total score of the questionnaire caused age to also have a significant relationship with chronic pain score.
Discussion
The results showed that after omission of questions 1 and 5, the GCPS 2.0 questionnaire showed appropriate validity and reliability for the Iranian population. This questionnaire showed a completely suitable content validity (content validity index=0.98). According to the suggestion of one of the experts, the phrase "pain in the jaw and/or face area" was added to the word "facial pain" to prevent misinterpretation by individuals.
Table 2. Merged results of multivariate linear regression test on the questionnaire subsets
{kind=link}
Hietaharju et al. [8] compared the suitability of GCPS versions 1.0 and 2.0 for biopsychosocial screening and subtyping of Finnish tertiary care referral patients with TMD pain. They reported that the distribution of TMD patients in both the questionnaire groups was the same, and the GCPS 2.0 could be regarded as a suitable initial screening tool for adjunct personalized or comprehensive multidisciplinary assessment.
Tanti and colleagues [4] examined the validity of GCPS 2.0 in an Indonesian population and found that it had appropriate validity, similar to its Persian version. The questionnaire was also investigated for validity in some other studies and found to have excellent validity, comparable to its Persian version [12,13].
Tanti and colleagues [4] reported an ICC of 0.79. The ICC value was 0.96 in a study by González and colleagues [14], and 0.81 in a study by Ferrer-Peña and colleagues [10]. These results indicate the appropriate reliability of this questionnaire in various studies.
Von Korff et al. [15] showed that due to easy use and speed, the number of questions can be reduced to 5 (questions 2 to 6) with sufficient validity and reliability, making it a modified version. Tedin et al. [16] showed the optimal validity and reliability of the Malay version of this questionnaire. In terms of validity in the present study, the KMO test result was 0.85, indicating adequacy of the sample size, and the significant result of the Bartlett test showed that the data in this study had the potential to become a factor [16]. These results were consistent with those of Ferrer-Peña and colleagues [10]. In their study, the KMO was 0.82, and the Bartlett test result was significant [10].
In the present study, after examining the correlation between the questions, it was found that questions 2 to 4, and 6 to 8 were correlated and placed in one factor, but questions 1 and 5 were different from other questions. After removing these two questions from the questionnaire, the questionnaire with the remaining 6 questions showed relatively high reliability and a higher Cronbach's alpha coefficient. However, since questions 1 and 5 have been added to the questionnaire to evaluate pain persistence and disability levels in past assessments, they cannot be removed from the questionnaire and should be examined separately from other questions. Similar conditions were reported by Ferrer-Peña et al. [10]. In their study, questions 2 to 4 were placed in one factor, questions 5 to 8 were placed in another factor, and question 1 did not appear in any of the main factors. According to the authors, question 1 had been added to the original questionnaire (English version) to evaluate pain persistence in past studies; thus, it should not be removed from the questionnaire. The Spanish version of this questionnaire also has 8 questions, similar to the original version [10].
The present study found that educational level had a significant direct correlation with the questionnaire score. The questionnaire score was also found to have a significant correlation with age. However, age was only significantly associated with the number of disability episodes. The questionnaire score was lower in males than females, but this difference was not statistically significant. These results were consistent with those of Salaffi and colleagues [17]. Age was only significantly associated with disability due to pain. In their study, the pain score was also reported to be lower in males than females, but this difference was significant. This difference may be attributed to the sample size and the reported location of pain.
Agha-Hosseini et al. [7] evaluated the correlation of bruxism with lumbar pain in an Iranian population. The patients were provided with instructions on how to discontinue their parafunctional habits including clenching and bruxism. The Helkimo and Rolland Morris questionnaires were used to assess TMDs and lower back pain in their study. The mean severity score of TMD significantly decreased after the intervention. Following treatment of TMDs, the mean severity score of lumbar pain significantly decreased from 8 to 2 [7]. The questionnaire used in their study was different from that used in the present study.
Gębska et al. [3] evaluated the prevalence of headache in TMD patients, using the Research Diagnostic Criteria for TMDs while the standardized short-form of the McGill Pain Questionnaire was used to qualitatively and quantitatively assess headaches. The participants with TMD reported the occurrence of headache significantly more than others, and it was associated with a pressing pain in the majority of patients (r = 0.82) and a cutting pain in a small percentage of patients (r=0.30). Neck and shoulder girdle pain and clenching and/or grinding of teeth were significantly more common among those who declared headache than those without headache. The results obtained so far may indicate a significant relationship between headache and TMDs [3].
This study was conducted on a homogeneous population in terms of social and educational status. Also, this study was the first to translate GCPS 2.0 to Persian for clinical applications.
Conclusion
The Persian version of the GCPS 2.0 with omission of questions 1 and 5 can be used to assess chronic pain in the TMJ area in the Iranian population.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Teshima T, Zakrzewska JM, Potter R. A systematic review of screening diagnostic tools for trigeminal neuralgia. Br J Pain. 2023 Jun;17(3):255-66. [DOI:10.1177/20494637221146854] [PMID] []
2. Chang CL, Wang DH, Yang MC, Hsu WE, Hsu ML. Functional disorders of the temporomandibular joints: Internal derangement of the temporomandibular joint. Kaohsiung J Med Sci. 2018 Apr;34(4):223-30. [DOI:10.1016/j.kjms.2018.01.004] [PMID]
3. Gębska M, Frąszczak M, Dalewski B, Kołodziej Ł. Qualitative and quantitative assessment of headaches in people with temporomandibular joint disorders: A pilot study. Adv Clin Exp Med. 2023 Oct;32(10):1193-9. [DOI:10.17219/acem/171821] [PMID]
4. Tanti I, Wira VVW, Pragustine Y, Himawan LS, Ariani N. Validation of the Indonesian version of the graded chronic pain scale 2.0 in pain-related temporomandibular disorders. Med J Indones. 2020 Mar;29(1):42-6. [DOI:10.13181/mji.oa.191790]
5. Gil-Martínez A, Paris-Alemany A, López-de-Uralde-Villanueva I, La Touche R. Management of pain in patients with temporomandibular disorder (TMD): challenges and solutions. J Pain Res. 2018 Mar 16;11:571-87. [DOI:10.2147/JPR.S127950] [PMID] []
6. Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. 2014 Winter;28(1):6-27. [DOI:10.11607/jop.1151] [PMID] []
7. Agha-Hosseini F, Mirzaii-Dizgah I, Shirazian S, Javaheri-Mahd M. Treating Parafunctional Habits for Alleviating Temporomandibular Disorder and Lower Back Pain: A Phase II Clinical Trial. Front Dent. 2023 May 2;20:11. [DOI:10.18502/fid.v20i11.12657] [PMID] []
8. Hietaharju M, Näpänkangas R, Sipilä K, et al. Importance of the Graded Chronic Pain Scale as a Biopsychosocial Screening Instrument in TMD Pain Patient Subtyping. J Oral Facial Pain Headache. 2021 Fall;35(4):303-16. [DOI:10.11607/ofph.2983] [PMID]
9. Whitten CE, Cristobal K. Chronic Pain is a Chronic Condition, Not Just a Symptom. Perm J. 2005 Summer;9(3):43-51. [DOI:10.7812/TPP/04-139]
10. Ferrer-Peña R, Gil-Martínez A, Pardo-Montero J, Jiménez-Penick V, Gallego-Izquierdo T, La Touche R. Adaptation and validation of the Spanish version of the graded chronic pain scale. Reumatol Clin. 2016 May-Jun;12(3):130-8. [DOI:10.1016/j.reumae.2015.07.003]
11. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017 May;11(Suppl 1):S80-9. [DOI:10.4103/sja.SJA_203_17] [PMID] []
12. Ahmadi Tehrani E, Naimi SS, Khademi Kalantari KH, Akbarzadeh Baghebani A, Tavakolizadeh S. Cultural Adaptation and Content Validation of the Persian Version of the Diagnostic Criteria for Temporomandibular Disorders Axis I. J Rehab Med. 2018; 7(3): 133-40.
13. González Yoly, Miranda-Rivera Yaritza, Espinosa Irene. cross-cultural adaptation of research diagnostic criteria for temporomandibular disorders( (RDC/TMD). Rev Fac Odontol Univ Antioq. 2023;25(1):11-25.
14. Salaffi F, Stancati A, Grassi W. Reliability and validity of the Italian version of the Chronic Pain Grade questionnaire in patients with musculoskeletal disorders. Clin Rheumatol. 2006 Sep;25(5):619-31. [DOI:10.1007/s10067-005-0140-y] [PMID]
15. Von Korff M, DeBar LL, Krebs EE, Kerns RD, Deyo RA, Keefe FJ. Graded chronic pain scale revised: mild, bothersome, and high-impact chronic pain. Pain. 2020 Mar;161(3):651-61. [DOI:10.1097/j.pain.0000000000001758] [PMID] []
16. Tedin Ng FN, Kadir K, Yusof ZYM. Reliability and Validity of the Malaysian English Version of the Diagnostic Criteria for Temporomandibular Disorder (M-English DC/TMD). Healthcare (Basel). 2022 Feb 9;10(2):329. [DOI:10.3390/healthcare10020329] [PMID] []
17. Salaffi F, Sarzi-Puttini P, Atzeni F. How to measure chronic pain: New concepts. Best Pract Res Clin Rheumatol. 2015 Feb;29(1):164-86. [DOI:10.1016/j.berh.2015.04.023] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |