Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 2 (6-2024)
J Res Dent Maxillofac Sci 2024, 9(2): 94-99 |
Back to browse issues page

Ethics code: IR.TBZMED.REC.1397.434
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirmohammadi K, Fattahi S, Tavakoli F, Tashakor A. Prevalence of Dysplasia in Oral Lichen Planus Patients. J Res Dent Maxillofac Sci 2024; 9 (2) :94-99
URL: http://jrdms.dentaliau.ac.ir/article-1-531-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-531-en.html



1- Department of Orthodontics, Faculty of Dentistry, Tehran Azad University of Medical Sciences, Tehran, Iran. , Mirmohammadi_kamal@yahoo.com
2- Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran.
3- Oral and Maxillofacial Medicine Department, Faculty of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Department of Orthodontics, Faculty of Dentistry, Tehran Azad University of Medical Sciences, Tehran, Iran.
2- Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran.
3- Oral and Maxillofacial Medicine Department, Faculty of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
4- Department of Orthodontics, Faculty of Dentistry, Tehran Azad University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 314 kb]
(660 Downloads)
| Abstract (HTML) (2409 Views)
Full-Text: (817 Views)
Abstract
Background and Aim: Lichen planus (LP) is a chronic inflammatory mucocutaneous disease usually diagnosed based on clinical and histopathological findings. Prognostic evaluation of malignant transformation in LP is clinically and histologically complex. Due to the inconsistent results of previous studies regarding the prevalence of dysplastic changes in LP, this study aimed to evaluate the prevalence of dysplasia in oral lichen planus (OLP) patients.
Materials and Methods: This cross-sectional study was conducted on biopsy samples of OLP patients referred to Tabriz Dental Faculty from 2012 to 2020. The diagnosis of OLP was based on the World Health Organization criteria, which was confirmed by reassessment of the microscopic slides by a pathologist. The clinical subtype of OLP samples was specified based on the information present in patient files. Data were analyzed by the Chi-square test using SPSS 17 (alpha=0.05).
Results: The buccal mucosa was the most commonly involved area (27 out of 36 cases). The tongue ranked next (10 out of 36 cases). The most common clinical subtype was reticular form with 23 cases (63.9%). In 8 cases (21.9%), epithelial dysplasia was observed; of which, 7 cases were grade I and 1 was grade II. Among the observed dysplastic features, nuclear hyperchromatosis and enlarged nucleus had the highest incidence (11.1%).
Conclusion: The percentage of dysplasia in OLP specimens was not high in the study population. However, considering the risk of transformation to squamous cell carcinoma (SCC), accurate diagnosis of SCC based on history, and clinical and histopathological findings is critical. In case of histopathological detection of dysplasia, long-term follow-up of patients is necessary.
Keywords: Lichen Planus; Oral; Prevalence; Squamous Cell Carcinoma
Introduction
Lichen planus (LP) is a chronic mucocutaneous disease with an unknown etiology that affects the skin or mucous membranes simultaneously or individually. The oral mucosa may become infected before, at the same time, or after the development of lesions in other areas [1]. Approximately two-thirds of patients who initially develop skin lesions subsequently develop oral lesions; whereas, only one-third of patients who first show oral lesions later develop skin lesions [2]. Mucosal lesions are more chronic than skin lesions and often last for years [3]. LP more commonly affects middle-aged individuals such that 98% of the cases are older than 30 years of age. The prevalence of oral lichen planus (OLP) varies from 1% to 4% in different communities. The risk of malignant transformation of OLP is 1% to 3.5% [4]. Although the risk of malignant transformation of OLP to squamous cell carcinoma (SCC) is low, an annual follow-up has been suggested for OLP patients [5]. For patients with symptomatic OLP, malignancy testing is a part of the evaluation process of symptomatic treatment. Biopsy is essential for diagnosis and ruling out dysplasia or carcinoma. In some cases, a definite pathological diagnosis cannot be made, and conduction of direct immunofluorescence after routine histological assessment is necessary to reach a definite diagnosis [6].
In 90% of the cases, classic pathological findings including hyperkeratosis, acanthosis, elongation of rete ridges with saw-tooth, diffuse degeneration of the basal layer, and diffuse infiltration of lymphocyte strips in the underlying connective tissue are helpful criteria to reach a histopathological diagnosis [7]. The prevalence of malignancy may vary in different societies based on racial and geographical differences [8]. Early diagnosis of pre-malignant and malignant oral mucosal lesions has a pivotal role in better prognosis and longevity of patients [9]. Risk of malignant transformation of OLP is a highly controversial topic since the Hallopeau’s report in 1910 [10].
It is currently difficult to predict the risk of malignant transformation of OLP clinically or histologically. It is still unclear whether OLP is inherently malignant, or LP-like lesions with dysplasia develop into cancer [11]. Despite the contradictory results, some authors have proposed OLP as a precancerous lesion which can potentially develop into oral SCC [12]. The rate of malignant changes varies across the literature, ranging from 0.4% to 5.6% [13]. The results of a study by De Jong et al. [14] on the prevalence of epithelial dysplasia in patients with LP showed that in 25% of the cases, patients had mild to moderate dysplasia. They did not show a statistically significant relationship between the clinical subtype of LP and dysplastic changes. Also, no significant relationship was found between the age and sex of patients and prevalence of dysplasia in patients with LP. Due to the contradictory results regarding dysplastic changes of OLP, this study aimed to assess the prevalence of dysplasia in OLP patients referred to Tabriz Dental Faculty from 2012 to 2020.
Materials and Methods
This cross-sectional study was conducted on OLP specimens of patients referred to Tabriz Dental Faculty from 2012 to 2020. The study protocol was approved by the ethics committee of the dental school (IR.TBZMED.REC.1397.434). The inclusion criteria were presence of complete patient records containing demographic information and clinical diagnosis, as well as presence of sufficient amount of tissue in paraffin blocks for hematoxylin and eosin staining. Incomplete files and cases with tissue inadequacy were not included in the study. Demographic information of patients was extracted from patient files and recorded. The diagnosis of OLP had to be made according to the World Health Organization criteria. An experienced pathologist confirmed the diagnosis according to the histological findings of hematoxylin and eosin-stained slides. The clinical subtype of OLP specimens was determined according to the information in patient files. The specimens were also assessed for possible presence of epithelial dysplasia according to the 12 diagnostic criteria for epithelial dysplasia available in the literature [14]. The criteria for diagnosing epithelial dysplasia included architectural and cytological/cellular changes, and more than one of such changes were required for a diagnosis of dysplasia in the present study [15].
The grade of epithelial dysplasia refers to its severity or intensity. Mild epithelial dysplasia refers to alterations limited mainly to the basal and parabasal layers. Moderate epithelial dysplasia is defined as involvement from the basal layer to the midportion of the spinous layer.
The collected data were analyzed by descriptive statistical methods (frequency percentage) and Chi-Square test using SPSS version 17 (SPSS Inc., IL, USA). P<0.05 was considered statistically significant.
Results
This study examined 36 OLP specimens retrieved from the archives of Tabriz Dental Faculty from 2012 to 2020. The mean age of patients was 22.49±3.44 years (range 25 to 85 years). Of 36 patients, 19 (52.8%) were females, and 17 (47.2%) were males.
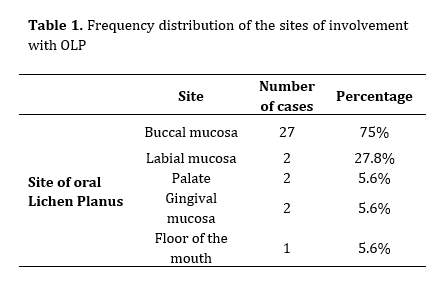
Regarding the site of involvement, the most affected area was the buccal mucosa with a significantly higher frequency of involvement compared with other sites (27 out of 36 patients). The tongue ranked next with a frequency of 10 out of 36 cases (Table 1).
Table 1. Frequency distribution of the sites of involvement with OLP
The most common clinical subtype of OLP was the reticular form with 23 cases (63.9%). The erosive form ranked second with a frequency of 33.3%. It should be noted that out of 36 cases examined, one case could not be assigned to any clinical subtype (Table 2).
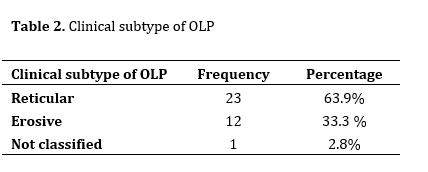
Assessment of 36 specimens for presence or absence of dysplasia revealed presence of epithelial dysplasia in 8 cases (21.9%); of which, 7 were grade I and 1 was grade II. The remaining 28 cases (77.8%) had grade 0 dysplasia (Figures 1 and 2).
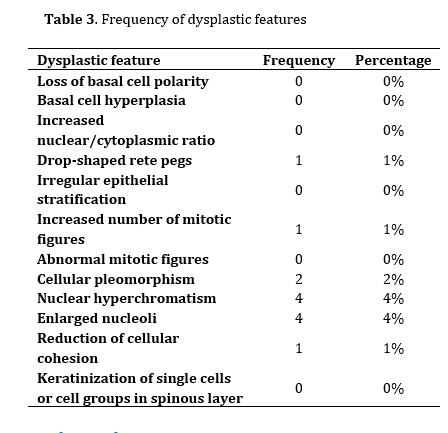
Assessment of individual dysplastic changes of the samples revealed that nuclear hyperchromatism and enlarged nuclei had the highest frequency (11.1%). Cellular pleomorphism ranked next (5.6%) (Table 3).
Table 2. Clinical subtype of OLP
Figure 1. Histopathological view of grade I dysplasia in OLP (H&E staining)
Figure 2. Frequency percentage of dysplasia grades
Table 3. Frequency of dysplastic features
Discussion
The prevalence of malignancies in different societies can vary based on racial and geographical differences [8]. Diagnosis of pre-malignant and malignant lesions of the oral mucosa has a definite role in improving the prognosis and longevity of patients [9]. The risk of malignant transformation in OLP has been one of the most debated topics since the Hallopeau’s report published in 1910 [10]. It is currently difficult to predict malignant changes in OLP clinically or histologically, and it is still unclear whether OLP is inherently malignant or whether these lesions are LP-like with dysplasia turning into cancer [11].
Mozaffari et al. [16] in their three-year study on histopathological findings in OLP conducted in the western part of Iran showed that the mean age of OLP patients was 22.49±3.44 years, and most of them were females (60.2%). According to their results, the right buccal mucosa was the most commonly involved site (38.5%). Histopathological examination showed that only 15.5% of patients had dysplasia; there was also a significant relationship between the frequency of dysplasia and age of patients. The results of their study were consistent with the results of the present study in terms of the mean age of patients and higher percentage of females with OLP. Also, in the present study, the rate of dysplasia was approximately 20%, which is close to the percentage reported in their study (15.5%). Moreover, buccal mucosa was the most commonly involved site in both studies.
Kashyap et al. [17] evaluated the dysplastic changes of OLP in 64 patients, and showed that only four patients did not have dysplasia (6.2%). Their results revealed that grade II dysplasia was the most common with 42.2% frequency, followed by grade III with 37.5% frequency. In their study, only 9 patients showed grade I dysplasia (14.1%) and the most common feature of dysplasia was basal cell hyperplasia (84.4%). Their results regarding the low frequency of grade I were contrary to the results of the present study. This difference may be due to different study populations and racial differences.
A retrospective study by Irani et al. [18] on 112 patients diagnosed with OLP showed that most patients were females (79 out of 112 cases) with a mean age of approximately 44.5 years. They reported that the erosive form was the most common type of OLP (50 cases), while the popular type was the least common with only one case. The most common site of involvement in patients was the buccal mucosa. Dysplastic changes were found in 12 cases; 5 of which were mild, and the remaining 7 were moderate. Of the studied samples, only one developed into SCC within 3 years. Their results were consistent with the results of the present study in terms of the proximity of the mean age of patients and higher percentage of females, but the dominance of the erosive form in their study was contrary to the results of the present study. Both studies showed that the buccal mucosa was the most common site of involvement. The difference between the two studies in the most common clinical subtype can be related to the larger sample size in the study by Irani et al [18]. De Jong et al. [14] in their study on the prevalence of epithelial dysplasia in patients with LP showed that in 25% of the cases, patients had mild to moderate dysplasia. They did not find a statistically significant relationship between the clinical subtype of LP and dysplastic changes. Also, no significant relationship was found between the age and sex of patients and prevalence of dysplasia in patients with LP.
In the present study, epithelial dysplasia was observed in 8 cases (21.9%), which was close to the rate reported by De Jong et al. [14], (25%). In a study conducted by Seyedmajidi et al, [19] on 26 patients with lichenoid oral mucosal lesions, 15.4% of the patients had dysplastic changes; of which, 3.8% were related to OLP. The percentage of dysplastic changes in the abovementioned study was lower than that in the present study probably due to their small sample size (26 patients). Also, in a study by Patil et al. [20] on the prevalence of lichenoid dysplasia in biopsy samples previously diagnosed with OLP, oral lichenoid lesions, and oral epithelial dysplasia, 8 cases of epithelial dysplasia were observed out of 54 OLP lesions. Also, 3 cases of epithelial dysplasia were observed out of 11 oral lichenoid lesions. Lichenoid features were also observed in 22 out of 95 cases of oral epithelial dysplasia. The results of their study showed that there was a relationship between lesions with lichenoid characteristics and epithelial dysplasia [20]. The number of cases of dysplasia observed in the abovementioned study was lower than that in the present study, which may be due to racial differences.
Conclusion
The percentage of dysplasia in OLP specimens was not high in the study population. However, considering the risk of transformation to SCC, accurate diagnosis of SCC based on history, and clinical and histopathological findings is critical. In case of histopathological detection of dysplasia, long-term follow-up of patients is necessary.
Background and Aim: Lichen planus (LP) is a chronic inflammatory mucocutaneous disease usually diagnosed based on clinical and histopathological findings. Prognostic evaluation of malignant transformation in LP is clinically and histologically complex. Due to the inconsistent results of previous studies regarding the prevalence of dysplastic changes in LP, this study aimed to evaluate the prevalence of dysplasia in oral lichen planus (OLP) patients.
Materials and Methods: This cross-sectional study was conducted on biopsy samples of OLP patients referred to Tabriz Dental Faculty from 2012 to 2020. The diagnosis of OLP was based on the World Health Organization criteria, which was confirmed by reassessment of the microscopic slides by a pathologist. The clinical subtype of OLP samples was specified based on the information present in patient files. Data were analyzed by the Chi-square test using SPSS 17 (alpha=0.05).
Results: The buccal mucosa was the most commonly involved area (27 out of 36 cases). The tongue ranked next (10 out of 36 cases). The most common clinical subtype was reticular form with 23 cases (63.9%). In 8 cases (21.9%), epithelial dysplasia was observed; of which, 7 cases were grade I and 1 was grade II. Among the observed dysplastic features, nuclear hyperchromatosis and enlarged nucleus had the highest incidence (11.1%).
Conclusion: The percentage of dysplasia in OLP specimens was not high in the study population. However, considering the risk of transformation to squamous cell carcinoma (SCC), accurate diagnosis of SCC based on history, and clinical and histopathological findings is critical. In case of histopathological detection of dysplasia, long-term follow-up of patients is necessary.
Keywords: Lichen Planus; Oral; Prevalence; Squamous Cell Carcinoma
Introduction
Lichen planus (LP) is a chronic mucocutaneous disease with an unknown etiology that affects the skin or mucous membranes simultaneously or individually. The oral mucosa may become infected before, at the same time, or after the development of lesions in other areas [1]. Approximately two-thirds of patients who initially develop skin lesions subsequently develop oral lesions; whereas, only one-third of patients who first show oral lesions later develop skin lesions [2]. Mucosal lesions are more chronic than skin lesions and often last for years [3]. LP more commonly affects middle-aged individuals such that 98% of the cases are older than 30 years of age. The prevalence of oral lichen planus (OLP) varies from 1% to 4% in different communities. The risk of malignant transformation of OLP is 1% to 3.5% [4]. Although the risk of malignant transformation of OLP to squamous cell carcinoma (SCC) is low, an annual follow-up has been suggested for OLP patients [5]. For patients with symptomatic OLP, malignancy testing is a part of the evaluation process of symptomatic treatment. Biopsy is essential for diagnosis and ruling out dysplasia or carcinoma. In some cases, a definite pathological diagnosis cannot be made, and conduction of direct immunofluorescence after routine histological assessment is necessary to reach a definite diagnosis [6].
In 90% of the cases, classic pathological findings including hyperkeratosis, acanthosis, elongation of rete ridges with saw-tooth, diffuse degeneration of the basal layer, and diffuse infiltration of lymphocyte strips in the underlying connective tissue are helpful criteria to reach a histopathological diagnosis [7]. The prevalence of malignancy may vary in different societies based on racial and geographical differences [8]. Early diagnosis of pre-malignant and malignant oral mucosal lesions has a pivotal role in better prognosis and longevity of patients [9]. Risk of malignant transformation of OLP is a highly controversial topic since the Hallopeau’s report in 1910 [10].
It is currently difficult to predict the risk of malignant transformation of OLP clinically or histologically. It is still unclear whether OLP is inherently malignant, or LP-like lesions with dysplasia develop into cancer [11]. Despite the contradictory results, some authors have proposed OLP as a precancerous lesion which can potentially develop into oral SCC [12]. The rate of malignant changes varies across the literature, ranging from 0.4% to 5.6% [13]. The results of a study by De Jong et al. [14] on the prevalence of epithelial dysplasia in patients with LP showed that in 25% of the cases, patients had mild to moderate dysplasia. They did not show a statistically significant relationship between the clinical subtype of LP and dysplastic changes. Also, no significant relationship was found between the age and sex of patients and prevalence of dysplasia in patients with LP. Due to the contradictory results regarding dysplastic changes of OLP, this study aimed to assess the prevalence of dysplasia in OLP patients referred to Tabriz Dental Faculty from 2012 to 2020.
Materials and Methods
This cross-sectional study was conducted on OLP specimens of patients referred to Tabriz Dental Faculty from 2012 to 2020. The study protocol was approved by the ethics committee of the dental school (IR.TBZMED.REC.1397.434). The inclusion criteria were presence of complete patient records containing demographic information and clinical diagnosis, as well as presence of sufficient amount of tissue in paraffin blocks for hematoxylin and eosin staining. Incomplete files and cases with tissue inadequacy were not included in the study. Demographic information of patients was extracted from patient files and recorded. The diagnosis of OLP had to be made according to the World Health Organization criteria. An experienced pathologist confirmed the diagnosis according to the histological findings of hematoxylin and eosin-stained slides. The clinical subtype of OLP specimens was determined according to the information in patient files. The specimens were also assessed for possible presence of epithelial dysplasia according to the 12 diagnostic criteria for epithelial dysplasia available in the literature [14]. The criteria for diagnosing epithelial dysplasia included architectural and cytological/cellular changes, and more than one of such changes were required for a diagnosis of dysplasia in the present study [15].
The grade of epithelial dysplasia refers to its severity or intensity. Mild epithelial dysplasia refers to alterations limited mainly to the basal and parabasal layers. Moderate epithelial dysplasia is defined as involvement from the basal layer to the midportion of the spinous layer.
The collected data were analyzed by descriptive statistical methods (frequency percentage) and Chi-Square test using SPSS version 17 (SPSS Inc., IL, USA). P<0.05 was considered statistically significant.
Results
This study examined 36 OLP specimens retrieved from the archives of Tabriz Dental Faculty from 2012 to 2020. The mean age of patients was 22.49±3.44 years (range 25 to 85 years). Of 36 patients, 19 (52.8%) were females, and 17 (47.2%) were males.
Regarding the site of involvement, the most affected area was the buccal mucosa with a significantly higher frequency of involvement compared with other sites (27 out of 36 patients). The tongue ranked next with a frequency of 10 out of 36 cases (Table 1).
Table 1. Frequency distribution of the sites of involvement with OLP
{kind=link}
The most common clinical subtype of OLP was the reticular form with 23 cases (63.9%). The erosive form ranked second with a frequency of 33.3%. It should be noted that out of 36 cases examined, one case could not be assigned to any clinical subtype (Table 2).
Assessment of 36 specimens for presence or absence of dysplasia revealed presence of epithelial dysplasia in 8 cases (21.9%); of which, 7 were grade I and 1 was grade II. The remaining 28 cases (77.8%) had grade 0 dysplasia (Figures 1 and 2).
Assessment of individual dysplastic changes of the samples revealed that nuclear hyperchromatism and enlarged nuclei had the highest frequency (11.1%). Cellular pleomorphism ranked next (5.6%) (Table 3).
Table 2. Clinical subtype of OLP
{kind=link}
Figure 1. Histopathological view of grade I dysplasia in OLP (H&E staining)
{kind=link}
Figure 2. Frequency percentage of dysplasia grades
{kind=link}
Table 3. Frequency of dysplastic features
{kind=link}
Discussion
The prevalence of malignancies in different societies can vary based on racial and geographical differences [8]. Diagnosis of pre-malignant and malignant lesions of the oral mucosa has a definite role in improving the prognosis and longevity of patients [9]. The risk of malignant transformation in OLP has been one of the most debated topics since the Hallopeau’s report published in 1910 [10]. It is currently difficult to predict malignant changes in OLP clinically or histologically, and it is still unclear whether OLP is inherently malignant or whether these lesions are LP-like with dysplasia turning into cancer [11].
Mozaffari et al. [16] in their three-year study on histopathological findings in OLP conducted in the western part of Iran showed that the mean age of OLP patients was 22.49±3.44 years, and most of them were females (60.2%). According to their results, the right buccal mucosa was the most commonly involved site (38.5%). Histopathological examination showed that only 15.5% of patients had dysplasia; there was also a significant relationship between the frequency of dysplasia and age of patients. The results of their study were consistent with the results of the present study in terms of the mean age of patients and higher percentage of females with OLP. Also, in the present study, the rate of dysplasia was approximately 20%, which is close to the percentage reported in their study (15.5%). Moreover, buccal mucosa was the most commonly involved site in both studies.
Kashyap et al. [17] evaluated the dysplastic changes of OLP in 64 patients, and showed that only four patients did not have dysplasia (6.2%). Their results revealed that grade II dysplasia was the most common with 42.2% frequency, followed by grade III with 37.5% frequency. In their study, only 9 patients showed grade I dysplasia (14.1%) and the most common feature of dysplasia was basal cell hyperplasia (84.4%). Their results regarding the low frequency of grade I were contrary to the results of the present study. This difference may be due to different study populations and racial differences.
A retrospective study by Irani et al. [18] on 112 patients diagnosed with OLP showed that most patients were females (79 out of 112 cases) with a mean age of approximately 44.5 years. They reported that the erosive form was the most common type of OLP (50 cases), while the popular type was the least common with only one case. The most common site of involvement in patients was the buccal mucosa. Dysplastic changes were found in 12 cases; 5 of which were mild, and the remaining 7 were moderate. Of the studied samples, only one developed into SCC within 3 years. Their results were consistent with the results of the present study in terms of the proximity of the mean age of patients and higher percentage of females, but the dominance of the erosive form in their study was contrary to the results of the present study. Both studies showed that the buccal mucosa was the most common site of involvement. The difference between the two studies in the most common clinical subtype can be related to the larger sample size in the study by Irani et al [18]. De Jong et al. [14] in their study on the prevalence of epithelial dysplasia in patients with LP showed that in 25% of the cases, patients had mild to moderate dysplasia. They did not find a statistically significant relationship between the clinical subtype of LP and dysplastic changes. Also, no significant relationship was found between the age and sex of patients and prevalence of dysplasia in patients with LP.
In the present study, epithelial dysplasia was observed in 8 cases (21.9%), which was close to the rate reported by De Jong et al. [14], (25%). In a study conducted by Seyedmajidi et al, [19] on 26 patients with lichenoid oral mucosal lesions, 15.4% of the patients had dysplastic changes; of which, 3.8% were related to OLP. The percentage of dysplastic changes in the abovementioned study was lower than that in the present study probably due to their small sample size (26 patients). Also, in a study by Patil et al. [20] on the prevalence of lichenoid dysplasia in biopsy samples previously diagnosed with OLP, oral lichenoid lesions, and oral epithelial dysplasia, 8 cases of epithelial dysplasia were observed out of 54 OLP lesions. Also, 3 cases of epithelial dysplasia were observed out of 11 oral lichenoid lesions. Lichenoid features were also observed in 22 out of 95 cases of oral epithelial dysplasia. The results of their study showed that there was a relationship between lesions with lichenoid characteristics and epithelial dysplasia [20]. The number of cases of dysplasia observed in the abovementioned study was lower than that in the present study, which may be due to racial differences.
Conclusion
The percentage of dysplasia in OLP specimens was not high in the study population. However, considering the risk of transformation to SCC, accurate diagnosis of SCC based on history, and clinical and histopathological findings is critical. In case of histopathological detection of dysplasia, long-term follow-up of patients is necessary.
Type of Study: Original article |
Subject:
Oral pathology
References
1. Neville BW, Damm DD, Allen CM, Chi AC. 4th ed. WB Saunders, Elsevier; Missouri: 2016. Oral and maxillofacial pathology; pp. 361.
2. Scully C, Beyli M, Ferreiro MC, Ficarra G, Gill Y, Griffiths M, Holmstrup P, Mutlu S, Porter S, Wray D. Update on oral lichen planus: etiopathogenesis and management. Crit Rev Oral Biol Med. 1998;9(1):86-122. [DOI:10.1177/10454411980090010501] [PMID]
3. Carrozzo M, Thorpe R. Oral lichen planus: a review. Minerva Stomatol. 2009 Oct;58(10):519-37.
4. Ghaem maghami SA, Taheri JB.The prevalence of coincide dermal and oral lesions of lichen planus. J Islamic Dent Assoc Iran 2003;15(45):75-87. [in persian]
5. Bornstein MM, Kalas L, Lemp S, Altermatt HJ, Rees TD, Buser D. Oral lichen planus and malignant transformation: a retrospective follow-up study of clinical and histopathologic data. Quintessence Int. 2006 Apr;37(4):261-71.
6. Boorghani M, Gholizadeh N, Taghavi Zenouz A, Vatankhah M, Mehdipour M. Oral lichen planus: clinical features, etiology, treatment and management; a review of literature. J Dent Res Dent Clin Dent Prospects. 2010 Winter;4(1):3-9.
7. Sugerman PB, Savage NW, Walsh LJ, Zhao ZZ, Zhou XJ, Khan A, Seymour GJ, Bigby M. The pathogenesis of oral lichen planus. Crit Rev Oral Biol Med. 2002;13(4):350-65. [DOI:10.1177/154411130201300405] [PMID]
8. Al-Hashimi I, Schifter M, Lockhart PB, Wray D, Brennan M, Migliorati CA, et al. Oral lichen planus and oral lichenoid lesions: diagnostic and therapeutic considerations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 Mar;103 Suppl:S25.e1-12. [DOI:10.1016/j.tripleo.2006.11.001] [PMID]
9. Rajentheran R, McLean NR, Kelly CG, Reed MF, Nolan A. Malignant transformation of oral lichen planus. Eur J Surg Oncol. 1999 Oct;25(5):520-3. [DOI:10.1053/ejso.1999.0689] [PMID]
10. Hallopeau H. Sur un cas de lichen de Wilson gingival avec neoplasie voisine dans la region maxillaire. Bull Soc Fr Dermatol Syphiligr 1910;17:32.
11. Agha-Hosseini F, Sheykhbahaei N, SadrZadeh-Afshar MS. Evaluation of Potential Risk Factors that contribute to Malignant Transformation of Oral Lichen Planus: A Literature Review. J Contemp Dent Pract. 2016 Aug 1;17(8):692-701. [DOI:10.5005/jp-journals-10024-1914] [PMID]
12. Bermejo-Fenoll A, Sanchez-Siles M, López-Jornet P, Camacho-Alonso F, Salazar-Sanchez N. Premalignant nature of oral lichen planus. A retrospective study of 550 oral lichen planus patients from south-eastern Spain. Oral Oncol. 2009 Aug;45(8):e54-6. [DOI:10.1016/j.oraloncology.2009.01.009] [PMID]
13. Fitzpatrick SG, Hirsch SA, Gordon SC. The malignant transformation of oral lichen planus and oral lichenoid lesions: a systematic review. J Am Dent Assoc. 2014 Jan;145(1):45-56. [DOI:10.14219/jada.2013.10] [PMID]
14. De Jong WF, Albrecht M, Bánóczy J, van der Waal I. Epithelial dysplasia in oral lichen planus. A preliminary report of a Dutch-Hungarian study of 100 cases. Int J Oral Surg. 1984 Jun;13(3):221-5. [DOI:10.1016/S0300-9785(84)80007-1] [PMID]
15. El-Naggar AK, Chan JK, Grandis JR, Takata T, Slootweg PJ. WHO Classification of Tumours of the Head and Neck. WHO/IARC Classification of Tumours of the Head and Neck., 4th edn Lyon: IARC Presslow. 2017.
16. Mozaffari HR, Mirbahari SG, Sadeghi M. Histopathological Findings in Oral Lichen Planus: A Three-Year Report from Western Iran, J Res Med Dent Sci. 2018;6(1):274-8
17. Kashyap B, Pallavi N, Shruthi BS, Birajdar S. Evaluation of oral epithelial dysplastic features in oral lichen planus: The diagnostic difficulties. Clin Cancer Investig J 2015;4:327-32. [DOI:10.4103/2278-0513.154038]
18. Irani S, Esfahani AM, Ghorbani A. Dysplastic change rate in cases of oral lichen planus: A retrospective study of 112 cases in an Iranian population. J Oral Maxillofac Pathol. 2016 Sep-Dec;20(3):395-9. [DOI:10.4103/0973-029X.190911] [PMID] []
19. Seyedmajidi M, Motallebnejad M, Foroughi, R, Aslani F. Clinical and Histopathological Findings in 26 Patients with Oral Lichenoid Lesions. J Babol Univ Med Sci 2010;12(3) :72-8.
20. Patil S, Rao RS, Sanketh DS, Warnakulasuriya S. Lichenoid dysplasia revisited - evidence from a review of Indian archives. J Oral Pathol Med. 2015 Aug;44(7):507-14. [DOI:10.1111/jop.12258] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |