Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 2 (6-2024)
J Res Dent Maxillofac Sci 2024, 9(2): 71-79 |
Back to browse issues page

Ethics code: IR.IAU.DENTAL.REC.1397.037
Clinical trials code: IRCT20120311009260N3
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Karimi M R, Sadatmansouri S, Anoush G, Montazeri M, Taheri N. Effect of Cyanoacrylate Adhesive on Palatal Wound Healing Following Free Gingival Grafting: A Clinical Trial. J Res Dent Maxillofac Sci 2024; 9 (2) :71-79
URL: http://jrdms.dentaliau.ac.ir/article-1-485-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-485-en.html
Mohammad Reza Karimi1 
 , Saeed Sadatmansouri1
, Saeed Sadatmansouri1  , Ghazal Anoush2 , Mostafa Montazeri *3 , Nastaran Taheri2
, Ghazal Anoush2 , Mostafa Montazeri *3 , Nastaran Taheri2
, Saeed Sadatmansouri1 , Ghazal Anoush2 , Mostafa Montazeri *3 , Nastaran Taheri2
1- Department of Periodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran.
2- Private Dental Practice, Tehran, Iran.
3- Department of Periodontics, School of Dentistry, Shiraz Branch, Islamic Azad University, Shiraz, Iran. ,mosimont@gmail.com
2- Private Dental Practice, Tehran, Iran.
3- Department of Periodontics, School of Dentistry, Shiraz Branch, Islamic Azad University, Shiraz, Iran. ,
Keywords: Tissue adhesives, Wound healing, Cyanoacrylates, Transplantation, Gingiva, Pain, Postoperative
Full-Text [PDF 411 kb]
(1104 Downloads)
| Abstract (HTML) (3402 Views)
Full-Text: (1327 Views)
Abstract
Background and Aim: This study investigated the effect of applying cyanoacrylate adhesive on clinical indices involved in the healing process of the palatal wound following free gingival graft (FGG) harvesting.
Materials and Methods: In this randomized controlled clinical trial, 15 patients who required bilateral FGG harvesting were randomly assigned to two groups. In the suture group, the wound was closed by Vicryl 4-0 sutures; whereas in the control group, the wound closure and hemostasis were attained by applying a concentrated mixture of n-butyl and 2-octyl cyanoacrylate. The primary outcomes included pain according to a visual analog scale (VAS), discomfort, healing rate, early and late bleeding, ease of feeding, wound epithelization rate, and sensory disturbances within one week and three months following the surgery. Statistical analysis was performed with the Chi-square and Mann-Whitney U tests (alpha=0.05).
Results: Cyanoacrylate application on the wound was significantly faster than suturing (2.12±1.23 minutes vs. 8.42±2.24 minutes, P<0.0001). The mean postoperative pain score (P=0.015), patient discomfort (P=0.017), and healing rate (P=0.024) were significantly more favorable in the cyanoacrylate group compared to the control group during the first week after surgery. Rate of wound epithelialization showed no significant difference between the two groups (P>0.05).
Conclusion: Application of cyanoacrylate adhesive to enhance the healing of palatal donor site wound decreased pain and discomfort and enhanced healing during the first postoperative week. In general, cyanoacrylate application is comparable to suturing in palatal wound healing and may be used for faster (by 6 minutes) closure of FGG wounds.
Keywords: Tissue adhesives; Wound healing; Cyanoacrylates; Transplantation; Gingiva; Pain; Postoperative
Introduction
The palatal wound created following free gingival graft (FGG) surgery is usually accompanied by patient discomfort. The wound healing process after surgery has always been a concern for dentists. In the oral cavity, healing is considered to be more complicated due to the movement of the tongue, swallowing, and chewing [1]. With the development of prosthetic treatment options and the necessity to increase the keratinized gingiva width, periodontal plastic surgery has become more popular [2]. Nowadays, materials such as hemostatic substances (including absorbable collagen/gelatin sponge, oxidized regenerated cellulose, ferric sulfate) [3], antibiotics, mouthwashes [4], medicinal plant extracts [5], platelet concentrates [6] and more recently erythropoietin [7] are used to accelerate the healing process and reduce long-term bleeding and pain originating from palatal wounds. If the donor site is not managed correctly after graft harvesting, pain, bleeding, or infection may occur and lead to further complications for patients. Cyanoacrylate is a suitable alternative for management of extraoral wounds. Its advantages include fast application, patient comfort, resistance to infection, hemostatic properties, and no need for a second session for suture removal [8].
Cyanoacrylates, first introduced by Coover in 1959, are a group of structurally simple and inexpensive adhesives used to stabilize tissues in periodontal plastic surgery [9, 10]. Butyl cyanoacrylates have bacteriostatic and hemostatic properties, are biodegradable, have a long half-life, and have optimal biocompatibility. They have adhesive properties in humid environments, and they are also available in formulations suitable for intraoral use [11]. A study conducted in 2003 reported the hemostatic properties of cyanoacrylates in patients under treatment with warfarin [12].
There is a gap of information on the effect of cyanoacrylate adhesive on the palatal donor site for a FGG; thus, this study aimed to evaluate the effect of cyanoacrylate adhesive on clinical parameters of palatal wound healing following FGG harvesting.
Materials and Methods
Ethical approval:
This study was approved by the ethics committee of the Faculty of Dentistry, Islamic Azad University of Tehran (IR.IAU.DENTAL.REC.1397.037) and registered in the Iranian Registry of Clinical Trials (IRCT20120311009260N3).
Sample collection:
This split-mouth clinical trial was performed on patients referred to the Periodontics Department of the School of Dentistry of Islamic Azad University of Tehran in 2018-2019. All patients who required bilateral FGGs were evaluated after obtaining written informed consent from them.
A computer-generated randomization list (Excel 2016, Microsoft Co., Redmond, Washington, USA) was used to randomly assign one quadrant of each patient to the test and the other one to the control group. In the test group, cyanoacrylate adhesive (PeriAcryl®90, GluStitch Inc., BC, Canada) was applied over the donor site; whereas, conventional sutures (Vicryl 4-0 suture material; Supa Medical Devices Co., Tehran, Iran) and periodontal dressing (Coe-Pak™, GC America Inc., Chicago, IL, USA) were utilized in the control side. Acetaminophen (500 mg; Arya Pharmaceutical Co., Tehran, Iran) was prescribed for pain control before and right after the surgical procedure. The patients signed an informed consent not to take any other analgesic on the day of surgery.
Systemically healthy patients with inflammation-free periodontium, and suitable palatal vaults for bilateral FGG harvesting between 35 to 60 years of age were included in this study. The exclusion criteria were patients with significant systemic diseases affecting oral mucosa or wound healing, pregnancy, presence of painful oral conditions such as teeth requiring root canal treatment, psychiatric diseases, intake of drugs interfering with wound healing or basic metabolism, smoking and alcohol consumption, history of surgery in the past 6 months, and trauma to the head and neck region.
Surgical procedure:
The thickness of the FGG was attempted to be roughly 1.5 mm. Also, a template (10 mm × 5 mm) was employed to replicate the graft on both sides of the palate. The steps utilized in this process are shown in Figures 1 to 4.
Figure 1. Palatal donor site immediately after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right) were applied to the wound area
Figure 2. Palatal donor site one week after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right)
Figure 3. Palatal donor site one month after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right)
Figure 4. Evaluation of epithelialization by applying 3% H2O2. Presence of bubbles in the first week (left). No bubble could be seen in the first month, which indicates completion of epithelialization (right)
Background and Aim: This study investigated the effect of applying cyanoacrylate adhesive on clinical indices involved in the healing process of the palatal wound following free gingival graft (FGG) harvesting.
Materials and Methods: In this randomized controlled clinical trial, 15 patients who required bilateral FGG harvesting were randomly assigned to two groups. In the suture group, the wound was closed by Vicryl 4-0 sutures; whereas in the control group, the wound closure and hemostasis were attained by applying a concentrated mixture of n-butyl and 2-octyl cyanoacrylate. The primary outcomes included pain according to a visual analog scale (VAS), discomfort, healing rate, early and late bleeding, ease of feeding, wound epithelization rate, and sensory disturbances within one week and three months following the surgery. Statistical analysis was performed with the Chi-square and Mann-Whitney U tests (alpha=0.05).
Results: Cyanoacrylate application on the wound was significantly faster than suturing (2.12±1.23 minutes vs. 8.42±2.24 minutes, P<0.0001). The mean postoperative pain score (P=0.015), patient discomfort (P=0.017), and healing rate (P=0.024) were significantly more favorable in the cyanoacrylate group compared to the control group during the first week after surgery. Rate of wound epithelialization showed no significant difference between the two groups (P>0.05).
Conclusion: Application of cyanoacrylate adhesive to enhance the healing of palatal donor site wound decreased pain and discomfort and enhanced healing during the first postoperative week. In general, cyanoacrylate application is comparable to suturing in palatal wound healing and may be used for faster (by 6 minutes) closure of FGG wounds.
Keywords: Tissue adhesives; Wound healing; Cyanoacrylates; Transplantation; Gingiva; Pain; Postoperative
Introduction
The palatal wound created following free gingival graft (FGG) surgery is usually accompanied by patient discomfort. The wound healing process after surgery has always been a concern for dentists. In the oral cavity, healing is considered to be more complicated due to the movement of the tongue, swallowing, and chewing [1]. With the development of prosthetic treatment options and the necessity to increase the keratinized gingiva width, periodontal plastic surgery has become more popular [2]. Nowadays, materials such as hemostatic substances (including absorbable collagen/gelatin sponge, oxidized regenerated cellulose, ferric sulfate) [3], antibiotics, mouthwashes [4], medicinal plant extracts [5], platelet concentrates [6] and more recently erythropoietin [7] are used to accelerate the healing process and reduce long-term bleeding and pain originating from palatal wounds. If the donor site is not managed correctly after graft harvesting, pain, bleeding, or infection may occur and lead to further complications for patients. Cyanoacrylate is a suitable alternative for management of extraoral wounds. Its advantages include fast application, patient comfort, resistance to infection, hemostatic properties, and no need for a second session for suture removal [8].
Cyanoacrylates, first introduced by Coover in 1959, are a group of structurally simple and inexpensive adhesives used to stabilize tissues in periodontal plastic surgery [9, 10]. Butyl cyanoacrylates have bacteriostatic and hemostatic properties, are biodegradable, have a long half-life, and have optimal biocompatibility. They have adhesive properties in humid environments, and they are also available in formulations suitable for intraoral use [11]. A study conducted in 2003 reported the hemostatic properties of cyanoacrylates in patients under treatment with warfarin [12].
There is a gap of information on the effect of cyanoacrylate adhesive on the palatal donor site for a FGG; thus, this study aimed to evaluate the effect of cyanoacrylate adhesive on clinical parameters of palatal wound healing following FGG harvesting.
Materials and Methods
Ethical approval:
This study was approved by the ethics committee of the Faculty of Dentistry, Islamic Azad University of Tehran (IR.IAU.DENTAL.REC.1397.037) and registered in the Iranian Registry of Clinical Trials (IRCT20120311009260N3).
Sample collection:
This split-mouth clinical trial was performed on patients referred to the Periodontics Department of the School of Dentistry of Islamic Azad University of Tehran in 2018-2019. All patients who required bilateral FGGs were evaluated after obtaining written informed consent from them.
A computer-generated randomization list (Excel 2016, Microsoft Co., Redmond, Washington, USA) was used to randomly assign one quadrant of each patient to the test and the other one to the control group. In the test group, cyanoacrylate adhesive (PeriAcryl®90, GluStitch Inc., BC, Canada) was applied over the donor site; whereas, conventional sutures (Vicryl 4-0 suture material; Supa Medical Devices Co., Tehran, Iran) and periodontal dressing (Coe-Pak™, GC America Inc., Chicago, IL, USA) were utilized in the control side. Acetaminophen (500 mg; Arya Pharmaceutical Co., Tehran, Iran) was prescribed for pain control before and right after the surgical procedure. The patients signed an informed consent not to take any other analgesic on the day of surgery.
Systemically healthy patients with inflammation-free periodontium, and suitable palatal vaults for bilateral FGG harvesting between 35 to 60 years of age were included in this study. The exclusion criteria were patients with significant systemic diseases affecting oral mucosa or wound healing, pregnancy, presence of painful oral conditions such as teeth requiring root canal treatment, psychiatric diseases, intake of drugs interfering with wound healing or basic metabolism, smoking and alcohol consumption, history of surgery in the past 6 months, and trauma to the head and neck region.
Surgical procedure:
The thickness of the FGG was attempted to be roughly 1.5 mm. Also, a template (10 mm × 5 mm) was employed to replicate the graft on both sides of the palate. The steps utilized in this process are shown in Figures 1 to 4.
Figure 1. Palatal donor site immediately after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right) were applied to the wound area
{kind=link}
Figure 2. Palatal donor site one week after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right)
{kind=link}
Figure 3. Palatal donor site one month after surgery. Conventional sutures (left) and cyanoacrylate adhesive (right)
{kind=link}
Figure 4. Evaluation of epithelialization by applying 3% H2O2. Presence of bubbles in the first week (left). No bubble could be seen in the first month, which indicates completion of epithelialization (right)
{kind=link}
Pain was assessed by using a visual analog scale (VAS) [13]. The level of pain was marked on a 10-cm line representing a continuum between "no pain" and "the worst pain imaginable." The 10-cm VAS was used at 5 hours post-surgery and also on a daily basis for one week. The patients were contacted to be reminded to record their pain score during this time period in the checklist. During the first week, the patients were also asked to record the number of taken analgesics in a timetable. Also, the level and duration of pain were marked using the VAS ruler. The patients were recalled at 1 and 3 months postoperatively and re-evaluated for pain [13].
The discomfort of patients was also recorded using a 10-cm scale with zero indicating "no discomfort," and 10 indicating "extreme discomfort imaginable." This scale was used at 5 hours post-surgery and on a daily basis for one week. The patients were contacted to be reminded to record their discomfort. The patients marked their discomfort in the checklist daily for the first week and were re-evaluated after 1 and 3 months [14].
Healing was assessed by a five-point healing scale, graded from 1 to 5. Score 1 indicated uneventful healing, 2 indicated healing with inflammation, 3 indicated healing with clot dehiscence, 4 indicated healing with wound dehiscence, and 5 indicated no healing [15].
The epithelialization rate was assessed clinically through standardized color photography of the donor site on the day of surgery, and at 7 days, 1 month, and 3 months after surgery. One single operator (Dr. GH Anoosh) took all the photographs with a DSLR camera (Canon 600D, Canon Inc., Ota, Tokyo, Japan) coupled with a 100 mm macro lens with a flash on, and standardized settings. The photographs were taken perpendicular to the area, and to standardize the images, a 5.5 × 2 mm aluminum foil was placed next to the donor site as a reference to assess the changes in wound size (standard visual scale). The assessments were repeated by a second examiner, and the wound edges on the photograph were traced twice using a computer program (Adobe Photoshop CC 2018, Adobe Inc., San Jose, CA, USA) by both examiners [16]. The rate of epithelialization was assessed by applying 3% H2O2 over the area and observing the bubbling. In case of presence of an intact epithelial membrane, H2O2 would not penetrate into the area, and no bubbles would form. After applying 3% H2O2, absence or presence of bubbles in < ⅓ of the donor site was considered as a sign of complete epithelialization. If bubbling was spotted in more than ⅔ of the donor site, moderate epithelialization was reported, and if between ⅓ to ⅔ of the donor site contained bubbling, mild epithelialization was recorded [17].
Sensory disorders were examined by moving a periodontal probe in 4 palatal areas (coronal, apical, mesial, distal) compared to the opposite side of the palate at 1 week, 1 month, and 3 months after surgery. According to the patients’ responses, sensory loss was reported as none, mild, moderate, and severe [18].
If the patients managed to consume hard or warm foods in the first days after surgery, their eating habit was deemed normal. If the patients struggled with consumption of hard and hot foods, their eating habit was categorized as severe, and if only one of the two variables of hardness or heat was altered, it was considered moderate [18]. To avoid disrupting the patients’ eating habits, the graft harvesting surgery was carried out on for the opposite side one month later.
Statistical analysis:
The Mann-Whitney U test was used for statistical analysis of immediate and late bleeding indices, and the Chi-square test and Friedman test were applied for other indices including pain, discomfort, number of taken analgesics, healing rate, epithelialization rate, sensory disorders, normal feeding, and dimensional changes. Level of significance was set at 0.05.
Results
This study was performed on 15 patients to evaluate the effect of cyanoacrylate adhesive on clinical parameters of palatal wound healing following FGG. According to the split-mouth study design, the FGG samples consisted of 30 pieces divided into two groups of conventional suturing (without adhesive) with dressing, and cyanoacrylate adhesive.
The mean age of the patients was 47.2±1.53 years (range 37 to 58 years), and included 53% males (n=8) and 47% females (n=7). None of the samples had systemic diseases, pregnancy, smoking habits, history of trauma, or surgery in the past 6 months.
Pain: At 1 week, the pain score was significantly higher by 1.54 units (17%) in the control group than the test group (P=0.04). At 1 month, the pain score was 1.13 units (29%) lower in the case group and this difference was not statistically significant (P=0.1). At 3 months, the pain score was not significantly different between the two groups (P=0.8).
Discomfort: At 1 week, the discomfort score was significantly lower in the control group by 15.8% or 1.18 units (P<0.05). At 1 month, the discomfort score was 0.94 units (32%) lower in the test group, but the difference was not statistically significant (P=0.2). At 3 months, the difference in discomfort between the two groups was not statistically significant (P=0.9).
Number of taken analgesics: The number of taken analgesics was significantly lower in the test group by 2.12 tablets or 21% (P<0.002).
Healing rate: At 1 week, the healing rate was 0.9 units (22%) higher in the test group. This difference was statistically significant (P<0.05). At 1 month, the healing rate was 0.24 units (10.4%) lower in the test group. This difference was not statistically significant (P=0.8). At 3 months, the healing rate was not significantly different between the two groups (P=0.9).
Epithelialization rate: At 1 week, the epithelialization rate was higher in the control group by 0.27 units or 19.3% (P<0.08).
Sensory disorders: Moderate and severe degrees were not seen at any time point in any group. The difference in sensory disorders was not significant between the two groups at 1 week (P=0.8) or 1 month (P = 0.8). At 3 months, none of the patients in any group had sensory disorders.
Eating status: The difference in this parameter was not significant between the two groups at 1 week (P=0.07) or 1 month (P=0.9). In the last follow-up, the two groups showed similar results.
Dimensional changes: At 1-week, dimensional changes were significantly higher in the control group by 0.81 units or 28.9% (P<0.01). This difference was not statistically significant at 1 month (P=0.2). In the last follow-up, the two groups demonstrated similar results.
Immediate bleeding: There was no significant difference in immediate bleeding between the two groups (P>0.05).
Late bleeding: The difference in this regard was not significant between the two groups at 1 week (P = 0.7), and no further bleeding was seen in any group in the next follow-ups.
The time required for cyanoacrylate application was 2.12±1.23 minutes while the time required for suturing was 8.42±2.24 minutes, indicating significantly faster application of cyanoacrylate than suturing by 6.32 minutes (P<0.001).
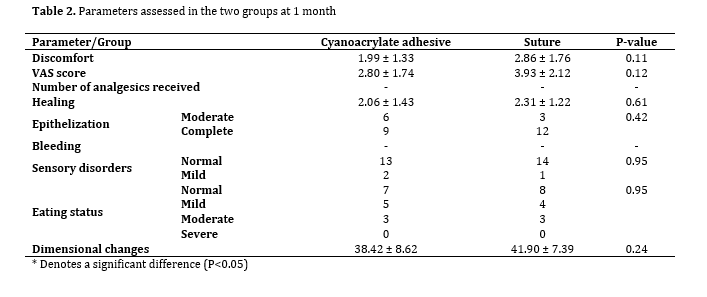
Tables 1 and 2 show the assessed parameters at 1 week and 1 month, respectively.
The discomfort of patients was also recorded using a 10-cm scale with zero indicating "no discomfort," and 10 indicating "extreme discomfort imaginable." This scale was used at 5 hours post-surgery and on a daily basis for one week. The patients were contacted to be reminded to record their discomfort. The patients marked their discomfort in the checklist daily for the first week and were re-evaluated after 1 and 3 months [14].
Healing was assessed by a five-point healing scale, graded from 1 to 5. Score 1 indicated uneventful healing, 2 indicated healing with inflammation, 3 indicated healing with clot dehiscence, 4 indicated healing with wound dehiscence, and 5 indicated no healing [15].
The epithelialization rate was assessed clinically through standardized color photography of the donor site on the day of surgery, and at 7 days, 1 month, and 3 months after surgery. One single operator (Dr. GH Anoosh) took all the photographs with a DSLR camera (Canon 600D, Canon Inc., Ota, Tokyo, Japan) coupled with a 100 mm macro lens with a flash on, and standardized settings. The photographs were taken perpendicular to the area, and to standardize the images, a 5.5 × 2 mm aluminum foil was placed next to the donor site as a reference to assess the changes in wound size (standard visual scale). The assessments were repeated by a second examiner, and the wound edges on the photograph were traced twice using a computer program (Adobe Photoshop CC 2018, Adobe Inc., San Jose, CA, USA) by both examiners [16]. The rate of epithelialization was assessed by applying 3% H2O2 over the area and observing the bubbling. In case of presence of an intact epithelial membrane, H2O2 would not penetrate into the area, and no bubbles would form. After applying 3% H2O2, absence or presence of bubbles in < ⅓ of the donor site was considered as a sign of complete epithelialization. If bubbling was spotted in more than ⅔ of the donor site, moderate epithelialization was reported, and if between ⅓ to ⅔ of the donor site contained bubbling, mild epithelialization was recorded [17].
Sensory disorders were examined by moving a periodontal probe in 4 palatal areas (coronal, apical, mesial, distal) compared to the opposite side of the palate at 1 week, 1 month, and 3 months after surgery. According to the patients’ responses, sensory loss was reported as none, mild, moderate, and severe [18].
If the patients managed to consume hard or warm foods in the first days after surgery, their eating habit was deemed normal. If the patients struggled with consumption of hard and hot foods, their eating habit was categorized as severe, and if only one of the two variables of hardness or heat was altered, it was considered moderate [18]. To avoid disrupting the patients’ eating habits, the graft harvesting surgery was carried out on for the opposite side one month later.
Statistical analysis:
The Mann-Whitney U test was used for statistical analysis of immediate and late bleeding indices, and the Chi-square test and Friedman test were applied for other indices including pain, discomfort, number of taken analgesics, healing rate, epithelialization rate, sensory disorders, normal feeding, and dimensional changes. Level of significance was set at 0.05.
Results
This study was performed on 15 patients to evaluate the effect of cyanoacrylate adhesive on clinical parameters of palatal wound healing following FGG. According to the split-mouth study design, the FGG samples consisted of 30 pieces divided into two groups of conventional suturing (without adhesive) with dressing, and cyanoacrylate adhesive.
The mean age of the patients was 47.2±1.53 years (range 37 to 58 years), and included 53% males (n=8) and 47% females (n=7). None of the samples had systemic diseases, pregnancy, smoking habits, history of trauma, or surgery in the past 6 months.
Pain: At 1 week, the pain score was significantly higher by 1.54 units (17%) in the control group than the test group (P=0.04). At 1 month, the pain score was 1.13 units (29%) lower in the case group and this difference was not statistically significant (P=0.1). At 3 months, the pain score was not significantly different between the two groups (P=0.8).
Discomfort: At 1 week, the discomfort score was significantly lower in the control group by 15.8% or 1.18 units (P<0.05). At 1 month, the discomfort score was 0.94 units (32%) lower in the test group, but the difference was not statistically significant (P=0.2). At 3 months, the difference in discomfort between the two groups was not statistically significant (P=0.9).
Number of taken analgesics: The number of taken analgesics was significantly lower in the test group by 2.12 tablets or 21% (P<0.002).
Healing rate: At 1 week, the healing rate was 0.9 units (22%) higher in the test group. This difference was statistically significant (P<0.05). At 1 month, the healing rate was 0.24 units (10.4%) lower in the test group. This difference was not statistically significant (P=0.8). At 3 months, the healing rate was not significantly different between the two groups (P=0.9).
Epithelialization rate: At 1 week, the epithelialization rate was higher in the control group by 0.27 units or 19.3% (P<0.08).
Sensory disorders: Moderate and severe degrees were not seen at any time point in any group. The difference in sensory disorders was not significant between the two groups at 1 week (P=0.8) or 1 month (P = 0.8). At 3 months, none of the patients in any group had sensory disorders.
Eating status: The difference in this parameter was not significant between the two groups at 1 week (P=0.07) or 1 month (P=0.9). In the last follow-up, the two groups showed similar results.
Dimensional changes: At 1-week, dimensional changes were significantly higher in the control group by 0.81 units or 28.9% (P<0.01). This difference was not statistically significant at 1 month (P=0.2). In the last follow-up, the two groups demonstrated similar results.
Immediate bleeding: There was no significant difference in immediate bleeding between the two groups (P>0.05).
Late bleeding: The difference in this regard was not significant between the two groups at 1 week (P = 0.7), and no further bleeding was seen in any group in the next follow-ups.
The time required for cyanoacrylate application was 2.12±1.23 minutes while the time required for suturing was 8.42±2.24 minutes, indicating significantly faster application of cyanoacrylate than suturing by 6.32 minutes (P<0.001).
Tables 1 and 2 show the assessed parameters at 1 week and 1 month, respectively.
Table 1. Parameters assessed in the two groups at 1 week
Table 2. Parameters assessed in the two groups at 1 month
Discussion
This controlled clinical trial evaluated the effect of application of cyanoacrylate adhesive compared to conventional suturing and dressing of the palatal donor site for FGG in a split-mouth design. The results revealed that the use of cyanoacrylate adhesive had a significant positive effect on some clinical parameters, such as the level of pain and discomfort experienced by patients and the healing rate.
FGG is a surgical technique that was introduced nearly 40 years ago to address the problem of keratinized tissue loss [19] and, up until now, has been the focus of considerable research [20]. Although other techniques such as subepithelial connective tissue grafting are widely used to treat gingival recessions, FGG is still a popular technique to increase the width of keratinized tissue. Due to its anatomical advantage and the possibility of harvesting tissue with ideal thickness, the palate has been recommended as an excellent site for FGG harvesting [21]. However, complications such as paresthesia, herpetic lesions, mucocele, heavy bleeding, and significant pain following FGG harvesting have been reported [22]. The area from the distal aspect of the maxillary canine to the first molar is the ideal donor site so that a safe distance could be maintained from the greater palatine artery, and also the obtained results would be comparable to those of previous investigations [23]. The ideal thickness of FGG is between 1-2 mm; In this study, standardization tools were used to ensure the average thickness of FGG to be 1.5 mm. In another study, the same thickness of FGG was used [20] while another study did not mention the thickness of harvested FGG [24].
Hemostatic agents, antiseptics, antibacterial agents, and a variety of herbal products have been proven to be effective to prevent FGG donor site complications [7], but efforts to find an ideal substance have been unsuccessful, and unwanted complications such as delayed wound healing and foreign body reaction have been reported [5-7].
Cyanoacrylate is a liquid acrylic acid derivative that, as a monomer, polymerizes when water or body secretions come in contact with it. It shapes a thin layer that holds the wound's edges together. It has a hemostatic, bacteriostatic, and slightly bactericidal effect, and its polymerization and adhesion to the living tissues create an impermeable layer against liquids and metabolites [25-27]. The effect of cyanoacrylate adhesive on FGG wound healing, and patient satisfaction has not been previously investigated. However, the positive effect of cyanoacrylate adhesive on wound healing in oral mucosal surgeries has been previously reported. Ghoreishian et al. [28] used tissue adhesives and sutures to close surgical wounds after mandibular third molar extraction, and, similar to the results of the present study, showed that the rate of postoperative healing was significantly greater in the test group than the conventional suture group.
Using cyanoacrylate to close the palatal wound took about 6 minutes less time than suturing in the present study. Similar to the findings of the present study, Soni et al. [29] found that the longer the incision length to harvest the graft, the greater the time savings when using cyanoacrylate adhesive because the cyanoacrylate application time, unlike sutures, does not increase with the length of the incision [29]. Saving time can reduce patient discomfort during surgery and increase patient compliance.
There were no significant differences between the two groups in terms of patients' age, palatal mucosal thickness, incision length, and the harvested FGG thickness. In other words, these factors were standardized in both groups in order not to have a confounding effect on the results. Also, unlike a recent study by Stavropoulou et al. [10] in which the number of females was higher, there was a balance between male and female patients in the present study.
A 10-point VAS was used to assess pain and discomfort of patients in the present study. Given the subjective nature of pain, there are constraints in documenting personal experience [30]. However, VAS seems to be a valid tool for assessment of clinical parameters, and especially postoperative pain [30]. In the present study, patients reported lower level of pain and discomfort and less analgesic consumption in the first week after surgery when cyanoacrylate adhesive was used for the donor site. Similarly, Galil et al. [31] reported that patients' acceptance of tissue adhesives was very high due to lower level of pain and less interference with chewing. Vastani and Maria [32] reported that cyanoacrylate adhesive enhanced early healing and reduced intraoperative and postoperative discomfort in patients. Khurana et al. [26] found no significant difference in pain, discomfort, burning sensation, and esthetic results between the two groups, but the rate of healing was higher in the cyanoacrylate group one week after surgery compared to the suture group. Thus, they concluded that cyanoacrylate could be helpful in early initial healing. This vital advantage of cyanoacrylate over conventional sutures can significantly affect the patients’ surgical experience and future compliance. Experiencing less pain and discomfort after surgery and saving time improve patients’ intraoperative and postoperative comfort. Also, lower level of pain and discomfort would help the patients to resume daily activities sooner.
Regarding the donor site's epithelialization rate, 13% of the areas covered with cyanoacrylate adhesive and 40% of the sutured areas showed mild epithelialization. One month after healing, 60% of the areas covered with cyanoacrylate adhesive and 80% of the areas in the conventional suture group showed complete epithelialization. Similar to the present findings, Del Pizzo et al. [33] showed standard epithelialization in only 17% of patients at the 2-week follow-up, and all patients at the 1-month follow-up after standardized FGG harvesting. Differences in imaging techniques of the palate and evaluation of epithelialization by comparing clinical images could explain the slight discrepancy observed with the current results at the 1-month follow-up. The method used in the present study is based on assessing the quality of the epithelial barrier. If the barrier is incomplete, H2O2 is released into the connective tissue, and with catalase function, bubbles form on the wound surface [34], which is more accurate and objective than the method used by Del Pizzo et al. [33]. Also, in general, rate of epithelialization in the cyanoacrylate adhesive group was significantly less than that in the suture group, which may be because the adhesive is washed out from the surface five days after surgery and its remnants are removed by phagocytes [31].
Kulkarni et al. [35] reported lower level of clinical and histological inflammation at 7 days after applying cyanoacrylate to close the periodontal flap compared with sutures, which was washed out on day 21, postoperatively, but no giant cells or histocytes were seen in any group. In contrast, Bhaskar and Cutright [36] stated that if cyanoacrylate penetrates deeply into the tissues, it can cause a giant cell reaction and phagocytosis. Therefore, in the present study, cyanoacrylate adhesive was applied topically. An aluminum foil surface was employed to prevent the entrapment of cyanoacrylate adhesive particles within the wound.
One limitation of this study was its reliance on patient satisfaction, introducing the potential for personal perceptions to influence the results. Nonetheless, the study addressed this concern through a split-mouth design, lack of selection bias, a robust sample size (15 samples), and meticulous control of variables, including anesthetics, sutures, and analgesics. These measures enhanced the validity and strength of the present investigation.
Conclusion
The results demonstrated that application of cyanoacrylate adhesive effectively reduces pain and discomfort in the first week post-surgery, along with a shortened surgical time. No significant differences were observed between the cyanoacrylate and conventional suture groups in terms of postoperative bleeding, sensory disorders, and eating habits of patients.
{kind=link}
Table 2. Parameters assessed in the two groups at 1 month
{kind=link}
Discussion
This controlled clinical trial evaluated the effect of application of cyanoacrylate adhesive compared to conventional suturing and dressing of the palatal donor site for FGG in a split-mouth design. The results revealed that the use of cyanoacrylate adhesive had a significant positive effect on some clinical parameters, such as the level of pain and discomfort experienced by patients and the healing rate.
FGG is a surgical technique that was introduced nearly 40 years ago to address the problem of keratinized tissue loss [19] and, up until now, has been the focus of considerable research [20]. Although other techniques such as subepithelial connective tissue grafting are widely used to treat gingival recessions, FGG is still a popular technique to increase the width of keratinized tissue. Due to its anatomical advantage and the possibility of harvesting tissue with ideal thickness, the palate has been recommended as an excellent site for FGG harvesting [21]. However, complications such as paresthesia, herpetic lesions, mucocele, heavy bleeding, and significant pain following FGG harvesting have been reported [22]. The area from the distal aspect of the maxillary canine to the first molar is the ideal donor site so that a safe distance could be maintained from the greater palatine artery, and also the obtained results would be comparable to those of previous investigations [23]. The ideal thickness of FGG is between 1-2 mm; In this study, standardization tools were used to ensure the average thickness of FGG to be 1.5 mm. In another study, the same thickness of FGG was used [20] while another study did not mention the thickness of harvested FGG [24].
Hemostatic agents, antiseptics, antibacterial agents, and a variety of herbal products have been proven to be effective to prevent FGG donor site complications [7], but efforts to find an ideal substance have been unsuccessful, and unwanted complications such as delayed wound healing and foreign body reaction have been reported [5-7].
Cyanoacrylate is a liquid acrylic acid derivative that, as a monomer, polymerizes when water or body secretions come in contact with it. It shapes a thin layer that holds the wound's edges together. It has a hemostatic, bacteriostatic, and slightly bactericidal effect, and its polymerization and adhesion to the living tissues create an impermeable layer against liquids and metabolites [25-27]. The effect of cyanoacrylate adhesive on FGG wound healing, and patient satisfaction has not been previously investigated. However, the positive effect of cyanoacrylate adhesive on wound healing in oral mucosal surgeries has been previously reported. Ghoreishian et al. [28] used tissue adhesives and sutures to close surgical wounds after mandibular third molar extraction, and, similar to the results of the present study, showed that the rate of postoperative healing was significantly greater in the test group than the conventional suture group.
Using cyanoacrylate to close the palatal wound took about 6 minutes less time than suturing in the present study. Similar to the findings of the present study, Soni et al. [29] found that the longer the incision length to harvest the graft, the greater the time savings when using cyanoacrylate adhesive because the cyanoacrylate application time, unlike sutures, does not increase with the length of the incision [29]. Saving time can reduce patient discomfort during surgery and increase patient compliance.
There were no significant differences between the two groups in terms of patients' age, palatal mucosal thickness, incision length, and the harvested FGG thickness. In other words, these factors were standardized in both groups in order not to have a confounding effect on the results. Also, unlike a recent study by Stavropoulou et al. [10] in which the number of females was higher, there was a balance between male and female patients in the present study.
A 10-point VAS was used to assess pain and discomfort of patients in the present study. Given the subjective nature of pain, there are constraints in documenting personal experience [30]. However, VAS seems to be a valid tool for assessment of clinical parameters, and especially postoperative pain [30]. In the present study, patients reported lower level of pain and discomfort and less analgesic consumption in the first week after surgery when cyanoacrylate adhesive was used for the donor site. Similarly, Galil et al. [31] reported that patients' acceptance of tissue adhesives was very high due to lower level of pain and less interference with chewing. Vastani and Maria [32] reported that cyanoacrylate adhesive enhanced early healing and reduced intraoperative and postoperative discomfort in patients. Khurana et al. [26] found no significant difference in pain, discomfort, burning sensation, and esthetic results between the two groups, but the rate of healing was higher in the cyanoacrylate group one week after surgery compared to the suture group. Thus, they concluded that cyanoacrylate could be helpful in early initial healing. This vital advantage of cyanoacrylate over conventional sutures can significantly affect the patients’ surgical experience and future compliance. Experiencing less pain and discomfort after surgery and saving time improve patients’ intraoperative and postoperative comfort. Also, lower level of pain and discomfort would help the patients to resume daily activities sooner.
Regarding the donor site's epithelialization rate, 13% of the areas covered with cyanoacrylate adhesive and 40% of the sutured areas showed mild epithelialization. One month after healing, 60% of the areas covered with cyanoacrylate adhesive and 80% of the areas in the conventional suture group showed complete epithelialization. Similar to the present findings, Del Pizzo et al. [33] showed standard epithelialization in only 17% of patients at the 2-week follow-up, and all patients at the 1-month follow-up after standardized FGG harvesting. Differences in imaging techniques of the palate and evaluation of epithelialization by comparing clinical images could explain the slight discrepancy observed with the current results at the 1-month follow-up. The method used in the present study is based on assessing the quality of the epithelial barrier. If the barrier is incomplete, H2O2 is released into the connective tissue, and with catalase function, bubbles form on the wound surface [34], which is more accurate and objective than the method used by Del Pizzo et al. [33]. Also, in general, rate of epithelialization in the cyanoacrylate adhesive group was significantly less than that in the suture group, which may be because the adhesive is washed out from the surface five days after surgery and its remnants are removed by phagocytes [31].
Kulkarni et al. [35] reported lower level of clinical and histological inflammation at 7 days after applying cyanoacrylate to close the periodontal flap compared with sutures, which was washed out on day 21, postoperatively, but no giant cells or histocytes were seen in any group. In contrast, Bhaskar and Cutright [36] stated that if cyanoacrylate penetrates deeply into the tissues, it can cause a giant cell reaction and phagocytosis. Therefore, in the present study, cyanoacrylate adhesive was applied topically. An aluminum foil surface was employed to prevent the entrapment of cyanoacrylate adhesive particles within the wound.
One limitation of this study was its reliance on patient satisfaction, introducing the potential for personal perceptions to influence the results. Nonetheless, the study addressed this concern through a split-mouth design, lack of selection bias, a robust sample size (15 samples), and meticulous control of variables, including anesthetics, sutures, and analgesics. These measures enhanced the validity and strength of the present investigation.
Conclusion
The results demonstrated that application of cyanoacrylate adhesive effectively reduces pain and discomfort in the first week post-surgery, along with a shortened surgical time. No significant differences were observed between the cyanoacrylate and conventional suture groups in terms of postoperative bleeding, sensory disorders, and eating habits of patients.
Type of Study: Randomized Clinical Trial |
Subject:
Periodontology
References
1. Gassner R. Wound closure materials. Oral Maxillofac Surg Clin North Am. 2002 Feb;14(1):95-104. [DOI:10.1016/S1042-3699(02)00009-2] [PMID]
2. Burkhardt R, Hämmerle CH, Lang NP; Research Group on Oral Soft Tissue Biology & Wound Healing. Self-reported pain perception of patients after mucosal graft harvesting in the palatal area. J Clin Periodontol. 2015 Mar;42(3):281-7. [DOI:10.1111/jcpe.12357] [PMID]
3. Rossmann JA, Rees TD. A comparative evaluation of hemostatic agents in the management of soft tissue graft donor site bleeding. J Periodontol. 1999 Nov;70(11):1369-75. [DOI:10.1902/jop.1999.70.11.1369] [PMID]
4. Kaigler D, Avila G, Wisner-Lynch L, Nevins ML, Nevins M, Rasperini G, Lynch SE, Giannobile WV. Platelet-derived growth factor applications in periodontal and peri-implant bone regeneration. Expert Opin Biol Ther. 2011 Mar;11(3):375-85. [DOI:10.1517/14712598.2011.554814] [PMID] []
5. Keceli HG, Aylikci BU, Koseoglu S, Dolgun A. Evaluation of palatal donor site haemostasis and wound healing after free gingival graft surgery. J Clin Periodontol. 2015 Jun;42(6):582-9. [DOI:10.1111/jcpe.12404] [PMID]
6. Yen CA, Griffin TJ, Cheung WS, Chen J. Effects of platelet concentrate on palatal wound healing after connective tissue graft harvesting. J Periodontol. 2007 Apr;78(4):601-10. [DOI:10.1902/jop.2007.060275] [PMID]
7. Yaghobee S, Rouzmeh N, Aslroosta H, Mahmoodi S, Khorsand A, Kharrazifard MJ. Effect of Topical Erythropoietin (EPO) on palatal wound healing subsequent to Free Gingival Grafting (FGG). Braz Oral Res. 2018 Jun 11;32:e55. [DOI:10.1590/1807-3107bor-2018.vol32.0055] [PMID]
8. Turkaslan T, Ozcan H, Dayicioglu D, Ozsoy Z. Use of adhesives in cleft palate surgery: a new flap fixation technique. J Craniofac Surg. 2005 Jul;16(4):719-22. [DOI:10.1097/01.SCS.0000159940.62875.95] [PMID]
9. Zumpano BJ, Jacobs LR, Hall JB, Margolis G, Sachs E Jr. Bioadhesive and histotoxic properties of ethyl-2-cyanoacrylate. Surg Neurol. 1982 Dec;18(6):452-7. [DOI:10.1016/0090-3019(82)90186-0] [PMID]
10. Stavropoulou C, Atout RN, Brownlee M, Schroth RJ, Kelekis-Cholakis A. A randomized clinical trial of cyanoacrylate tissue adhesives in donor site of connective tissue grafts. J Periodontol. 2019 Jun;90(6):608-15. [DOI:10.1002/JPER.18-0475] [PMID]
11. Gümüş P, Buduneli E. Graft stabilization with cyanoacrylate decreases shrinkage of free gingival grafts. Aust Dent J. 2014 Mar;59(1):57-64. [DOI:10.1111/adj.12149] [PMID]
12. Al-Belasy FA, Amer MZ. Hemostatic effect of n-butyl-2-cyanoacrylate (histoacryl) glue in warfarin-treated patients undergoing oral surgery. J Oral Maxillofac Surg. 2003 Dec;61(12):1405-9. [DOI:10.1016/j.joms.2002.12.001] [PMID]
13. Jung GH, Jung S, Park HJ, Oh HK, Kook MS. Factors Influencing Perception of Facial Attractiveness: Gender and Dental Education. J Craniofac Surg. 2018 Mar;29(2):e170-5. [DOI:10.1097/SCS.0000000000004241] [PMID]
14. Oteri G, De Ponte FS, Runci M, Peditto M, Marcianò A, Cicciù M. Oral-Health-Related Quality of Life After Surgical Treatment of Osteonecrosis of the Jaws. J Craniofac Surg. 2018 Mar;29(2):403-8. [DOI:10.1097/SCS.0000000000004087] [PMID]
15. Krasner D. Wound Healing Scale, version 1.0: a proposal. Adv Wound Care. 1997 Sep;10(5):82-5.
16. Sun T. Evaluation of the Effects of Two Dressing Materials: Absorbable Collagen Wound Dressings (HeliCOTE®) and Oxidized Regenerated Cellulose (Surgicel®) on Wound Healing at the Palatal Donor Site after Free Gingival Graft Surgery: A Pilot Study. [dissertation]. Boston: Tufts University School of Dental Medicine; 2015. Available from: http://hdl.handle.net/10427/011113
17. Silva CO, Ribeiro Edel P, Sallum AW, Tatakis DN. Free gingival grafts: graft shrinkage and donor-site healing in smokers and non-smokers. J Periodontol. 2010 May;81(5):692-701. [DOI:10.1902/jop.2010.090381] [PMID]
18. Ozcan M, Ucak O, Alkaya B, Keceli S, Seydaoglu G, Haytac MC. Effects of Platelet-Rich Fibrin on Palatal Wound Healing After Free Gingival Graft Harvesting: A Comparative Randomized Controlled Clinical Trial. Int J Periodontics Restorative Dent. 2017 Sep/Oct;37(5):e270-8. [DOI:10.11607/prd.3226] [PMID]
19. Pennel BM, Tabor JC, King KO, Towner JD, Fritz BD, Higgason JD. Free masticatory mucosa graft. J Periodontol. 1969 Mar;40(3):162-6. [DOI:10.1902/jop.1969.40.3.162] [PMID]
20. Hatipoğlu H, Keçeli HG, Güncü GN, Sengün D, Tözüm TF. Vertical and horizontal dimensional evaluation of free gingival grafts in the anterior mandible: a case report series. Clin Oral Investig. 2007 Jun;11(2):107-13. [DOI:10.1007/s00784-006-0084-x] [PMID]
21. Sanz M, Simion M; Working Group 3 of the European Workshop on Periodontology. Surgical techniques on periodontal plastic surgery and soft tissue regeneration: consensus report of Group 3 of the 10th European Workshop on Periodontology. J Clin Periodontol. 2014 Apr;41 Suppl 15:S92-7. [DOI:10.1111/jcpe.12215]
22. Wang HL, Bunyaratavej P, Labadie M, Shyr Y, MacNeil RL. Comparison of 2 clinical techniques for treatment of gingival recession. J Periodontol. 2001 Oct;72(10):1301-11. [DOI:10.1902/jop.2001.72.10.1301] [PMID]
23. Thoma DS, Sancho-Puchades M, Ettlin DA, Hämmerle CH, Jung RE. Impact of a collagen matrix on early healing, aesthetics and patient morbidity in oral mucosal wounds - a randomized study in humans. J Clin Periodontol. 2012 Feb;39(2):157-65. [DOI:10.1111/j.1600-051X.2011.01823.x] [PMID]
24. Wei PC, Laurell L, Geivelis M, Lingen MW, Maddalozzo D. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 1. A clinical study. J Periodontol. 2000 Aug;71(8):1297-305. [DOI:10.1902/jop.2000.71.8.1297] [PMID]
25. Collins JA, James PM, Levitsky SA, Bredenburg CE, Anderson RW, Leonard F, Hardaway RM 3rd. Cyanoacrylate adhesives as topical hemostatic aids. II. Clinical use in seven combat casualties. Surgery. 1969 Feb;65(2):260-3.
26. Khurana JV, Mali AM, Mali RS, Chaudhari AU. Comparative evaluation of healing after periodontal flap surgery using isoamyl 2-cyanoacrylate (bioadhesive material) and silk sutures: A split-mouth clinical study. J Indian Soc Periodontol. 2016 Jul-Aug;20(4):417-22. [DOI:10.4103/0972-124X.194267] [PMID] []
27. Etemadi A, Bitaraf T, Amini A, Goudarzi M, Nadafpour N. Bacterial Accumulation on Triclosan-Coated and Silk Sutures After Dental Implant Surgery. J Res Dent Maxillofac Sci 2019; 4 (3) :1-4. [DOI:10.29252/jrdms.4.3.1]
28. Ghoreishian M, Gheisari R, Fayazi M. Tissue adhesive and suturing for closure of the surgical wound after removal of impacted mandibular third molars: a comparative study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Jul;108(1):e14-6. [DOI:10.1016/j.tripleo.2009.03.001] [PMID]
29. Soni A, Narula R, Kumar A, Parmar M, Sahore M, Chandel M. Comparing cyanoacrylate tissue adhesive and conventional subcuticular skin sutures for maxillofacial incisions--a prospective randomized trial considering closure time, wound morbidity, and cosmetic outcome. J Oral Maxillofac Surg. 2013 Dec;71(12):2152.e1-8. [DOI:10.1016/j.joms.2013.08.029] [PMID]
30. Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK, Kvarstein G, Stubhaug A. Assessment of pain. Br J Anaesth. 2008 Jul;101(1):17-24. [DOI:10.1093/bja/aen103] [PMID]
31. Galil KA, Schofield ID, Wright GZ. Effect of n-butyl-2-cyanoacrylate (histoacryl blue) on the healing of skin wounds. J Can Dent Assoc. 1984 Jul;50(7):565-9.
32. Vastani A, Maria A. Healing of intraoral wounds closed using silk sutures and isoamyl 2-cyanoacrylate glue: a comparative clinical and histologic study. J Oral Maxillofac Surg. 2013 Feb;71(2):241-8. [DOI:10.1016/j.joms.2012.08.032] [PMID]
33. Del Pizzo M, Modica F, Bethaz N, Priotto P, Romagnoli R. The connective tissue graft: a comparative clinical evaluation of wound healing at the palatal donor site. A preliminary study. J Clin Periodontol. 2002 Sep;29(9):848-54. [DOI:10.1034/j.1600-051X.2002.290910.x] [PMID]
34. Marucha PT, Kiecolt-Glaser JK, Favagehi M. Mucosal wound healing is impaired by examination stress. Psychosom Med. 1998 May-Jun;60(3):362-5. [DOI:10.1097/00006842-199805000-00025] [PMID]
35. Kulkarni S, Dodwad V, Chava V. Healing of periodontal flaps when closed with silk sutures and N-butyl cyanoacrylate: a clinical and histological study. Indian J Dent Res. 2007 Apr-Jun;18(2):72-7. [DOI:10.4103/0970-9290.32424] [PMID]
36. Bhaskar SN, Cutright DE. Healing of skin wounds with butyl cyanoacrylate. J Dent Res. 1969 Mar-Apr;48(2):294-7. [DOI:10.1177/00220345690480022301] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |