Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 3 (8-2023)
J Res Dent Maxillofac Sci 2023, 8(3): 221-225 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Masannan Mozaffari P, Saeedi N, Mohtasham M, Khosravi F, Farjami F. Giant Cell Fibroma of the Oral Cavity: Case Series and Literature Review. J Res Dent Maxillofac Sci 2023; 8 (3) :221-225
URL: http://jrdms.dentaliau.ac.ir/article-1-439-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-439-en.html
Pegah Masannan Mozaffari1 

 , Nooshin Saeedi *2 , Mahdi Mohtasham3 , Farzaneh Khosravi4 , Fatane Farjami5
, Nooshin Saeedi *2 , Mahdi Mohtasham3 , Farzaneh Khosravi4 , Fatane Farjami5
, Nooshin Saeedi *2 , Mahdi Mohtasham3 , Farzaneh Khosravi4 , Fatane Farjami5
1- Oral & Maxillofacial Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
2- Oral & Maxillofacial Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran ,mahdi__sa1993@yahoo.com
3- Department of Oral and Maxillofacial Pathology, Mashhad University of Medical Sciences, Mashhad, Iran
4- Department of Cosmetic Medicine and Restorative Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
5- Department of Orofacial medicine, Borås Hospital, Sweden
2- Oral & Maxillofacial Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran ,
3- Department of Oral and Maxillofacial Pathology, Mashhad University of Medical Sciences, Mashhad, Iran
4- Department of Cosmetic Medicine and Restorative Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
5- Department of Orofacial medicine, Borås Hospital, Sweden
Full-Text [PDF 673 kb]
(1242 Downloads)
| Abstract (HTML) (2980 Views)
Introduction
Oral giant cell fibroma (GCF), a benign fibrous tumor, is an asymptomatic, sessile or pedunculated exophytic lesion smaller than 1 cm with a smooth or papillary surface and the same color as the oral mucosa [1].Weathers and Callihan [2] were the first to identify GCF in 1974 as an unprecedented fibrous hyperplastic soft tissue lesion, characterized by large, stellate, and mononucleated or multinucleated giant cells. Out of over 2,000 fibrous hyperplasia specimens, 108 cases met the criteria for a new lesion, which they termed GCF. GCF is more common in the second and third decades of life and has a slightly higher incidence in women, according to studies [1, 2].
Apparently, GCF is not associated with chronic irritation [3, 4]. However, one study suggested trauma or chronic irritation as the causative factor [5]. In 2016, de Oliviera et al. [4] showed that metalloproteinase-1 is involved in the pathogenesis of GCF. The most common site of involvement is the mandibular gingiva, followed by the maxillary gingiva, tongue and palate [6]. Conservative surgical excision is the treatment of choice for GCF, and recurrence is not common [1]; however, some studies have favored laser excision in children [7, 8].
To the best of the authors’ knowledge, there has been only one case report of GCF in Iran [7]. The present study reports GCF lesions in the buccal mucosa of Iranian patients, which is not common in the literature.
Case Presentation
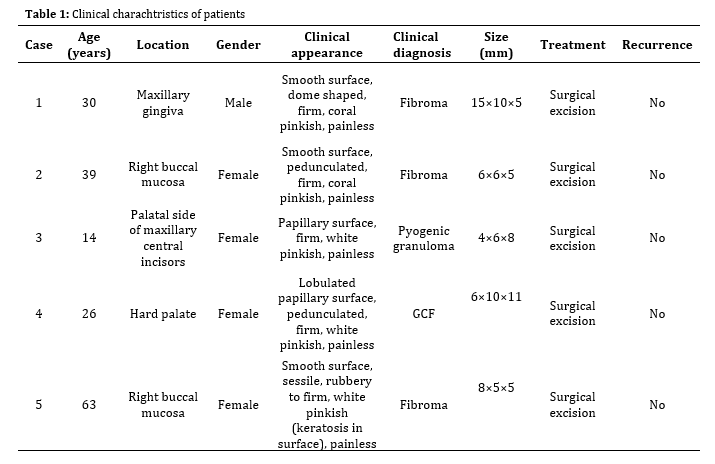
In this case series, records of five patients with GCF were extracted from the archives of the Department of Oral Medicine at the Faculty of Dentistry of Mashhad University of Medical Sciences, Iran and Shahab Dental Clinic in Mashhad city, Iran from December 2018 to December 2021. Demographic information of patients, clinical features, and histopathological characteristics of the lesions were extracted. Table 1 shows the clinical characteristics of patients. All patients signed informed consent forms.
Case 1: A 30-year-old male was referred to the Department of Oral Medicine with a slow-growing, painless growth on the palatal aspect of the maxillary central incisor region. According to the patient, there was a similar lesion in this area 10 years earlier, which was removed. However, the result of the biopsy was unknown to us. Examination revealed an approximately 15×10×5 mm, coral pinkish, smooth, and dome-shaped lesion with a firm consistency. The patient reported no pain during the examination. The clinical diagnosis of fibroma was made.
Although GCF lesions are usually smaller than 1 cm, this lesion was larger than average. Histological examination showed the presence of specific giant stellate fibroblasts and therefore the diagnosis of GCF was made.
Case 2: A 39-year-old female was referred to Shahab Dental Clinic with a pedunculated lesion in her right buccal mucosa from 18 months earlier that affected her mastication and caused discomfort. On clinical examination, the lesion was nontender, polypoid, and coral pinkish in color. However, it had a firmer consistency than a classic fibroma. Excisional biopsy of the lesion was compatible with GCF despite its rarity in the buccal mucosa.
Case 3: A 14-year-old girl was referred to the Department of Oral Medicine with a six-month history of a swelling on the palatal aspect of her upper central incisors. Clinical examination revealed an exophytic polypoid lesion with a firm consistency and a papillary surface and white-pinkish color. There was no specific stimulatory factor, such as calculus, in the area. The clinical diagnosis was pyogenic granuloma, although microscopic evidence confirmed GCF.
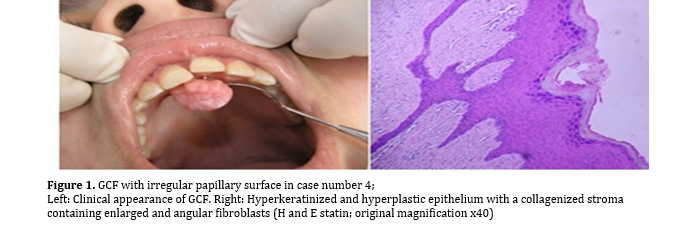
Case 4: A healthy 26-year-old female was referred to the Department of Oral Medicine with an exophytic lesion on the anterior aspect of the palate. According to the patient, the lesion had developed around 4 months earlier. The lesion appeared in a polypoid form with an irregularly lobulated papillary surface and a white-pinkish color and was firm in consistency. The lesion was not fluctuating, did not blanch on pressure, and was not tender. Due to its overgrowth, deformation of the palatal surface of the incisors was evident in the labial surface of the lesion (Fig. 1). Due to its lobulated surface, the clinical diagnosis of GCF was confirmed after histopathological examination.
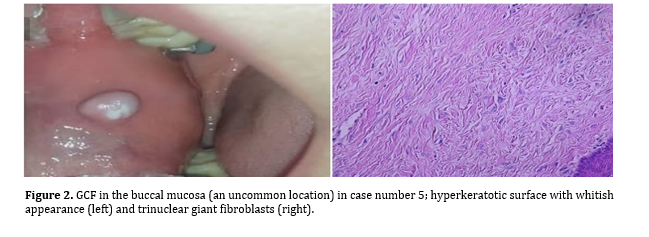
Case 5: A 63-year-old woman was referred to Shahab Dental Clinic, complaining of a swollen lesion on her right buccal mucosa for about 6 months. There was a small swelling in the buccal area which gradually increased in size and on examination, the lesion had been traumatized by occlusion. The exophytic pedunculated lesion had a rubbery to firm consistency. The overlying mucosa was pinkish in color and firm in consistency.
A hyperkeratotic surface with a white appearance was observed at the interference of the lesion and the occlusal line (Fig. 2), but the remaining surface was smooth. The lesion was not compressible.
Table 1: Clinical charachtristics of patients
Figure 1. GCF with irregular papillary surface in case number 4; Left: Clinical appearance of GCF. Right: Hyperkeratinized and hyperplastic epithelium with a collagenized stroma containing enlarged and angular fibroblasts (H and E statin; original magnification x40)
Figure 2. GCF in the buccal mucosa (an uncommon location) in case number 5; hyperkeratotic surface with whitish appearance (left) and trinuclear giant fibroblasts (right).
The clinical diagnosis of fibroma was made. Due to the unusual location of the lesion, GCF was not the first differential diagnosis, although histopathological assessment confirmed GCF. It measured approximately 5 mm laterally and 8 mm in anteroposterior direction, and had 5 mm thickness.
Discussion
Although irritation fibroma, a reactive lesion, is common in adults, its histopathological variant, known as GCF, is rare [9]. GCF has some features that distinguish it from fibroma. It usually occurs in the gingiva, tongue and palate. There are only a limited number of reports about GCF in the buccal mucosa. GCF lesions are usually smaller than 1 cm. The role of trauma in development of GCF has been contradictory. In addition, reports of GCF formation in trauma-prone areas, for instance, the buccal mucosa, are increasing. Reports of GCF in Iranians are rare [7]. Although there is no specific preponderance with regard to gender of patients, there were four females and one male patient in the present study. All patients had exophytic lesions with coral to white pink color but in case number 5, there was a white area on the lesion that appeared to be due to chronic contact with the teeth. The age range of patients was 14 to 63 years old. The smallest diameter of the lesions was 4 mm and the largest diameter was 15 mm; they were often firm in consistency.
Based on the clinical appearance of the lesion, the differential diagnosis mainly includes reactive and benign neoplastic lesions, such as irritable fibroma, pyogenic granuloma, and peripheral giant cell granuloma [6]. However, some clinical criteria such as color, size, surface appearance, localization, base, and presence of stimulating factors can aid in diagnosis [5]. Kuo et al. [10] showed that GCF resembles a fibroma or papilloma and is difficult to diagnose at first glance. At first sight, a differential diagnosis of GCF was unexpected in our cases due to its unusual location.
Full-Text: (2422 Views)
| Abstract
Background and Aim: Oral giant cell fibroma (GCF) is a benign fibrous tumor that is histologically characterized by large, stellate, and mono- or multinucleated giant cells. GCF is an asymptomatic, sessile, or pedunculated exophytic lesion, usually smaller than 1 cm, with a smooth or papillary surface and the same color as the oral mucosa. The role of trauma in development of GCF has been contradictory. Knowledge about the characteristics of this lesion can help in diagnosis, treatment and follow-up of patients. Case Presentation: This article describes five cases of GCF in Iranian patients, two of which were found in an uncommon location (buccal mucosa). Two were larger than usual (> 1 cm) and one had clinical manifestations resembling pyogenic granuloma. Patients were selected from two oral medicine centers. Conclusion: To distinguish GCF from other types of irritation fibroma, size, location, and presence or absence of stimulating factors should not preclude diagnosis. The diagnosis is confirmed by detection of giant cells in histological examination. Key Words: Fibroma; Mouth; Oral Medicine |
Introduction
Oral giant cell fibroma (GCF), a benign fibrous tumor, is an asymptomatic, sessile or pedunculated exophytic lesion smaller than 1 cm with a smooth or papillary surface and the same color as the oral mucosa [1].Weathers and Callihan [2] were the first to identify GCF in 1974 as an unprecedented fibrous hyperplastic soft tissue lesion, characterized by large, stellate, and mononucleated or multinucleated giant cells. Out of over 2,000 fibrous hyperplasia specimens, 108 cases met the criteria for a new lesion, which they termed GCF. GCF is more common in the second and third decades of life and has a slightly higher incidence in women, according to studies [1, 2].
Apparently, GCF is not associated with chronic irritation [3, 4]. However, one study suggested trauma or chronic irritation as the causative factor [5]. In 2016, de Oliviera et al. [4] showed that metalloproteinase-1 is involved in the pathogenesis of GCF. The most common site of involvement is the mandibular gingiva, followed by the maxillary gingiva, tongue and palate [6]. Conservative surgical excision is the treatment of choice for GCF, and recurrence is not common [1]; however, some studies have favored laser excision in children [7, 8].
To the best of the authors’ knowledge, there has been only one case report of GCF in Iran [7]. The present study reports GCF lesions in the buccal mucosa of Iranian patients, which is not common in the literature.
Case Presentation
In this case series, records of five patients with GCF were extracted from the archives of the Department of Oral Medicine at the Faculty of Dentistry of Mashhad University of Medical Sciences, Iran and Shahab Dental Clinic in Mashhad city, Iran from December 2018 to December 2021. Demographic information of patients, clinical features, and histopathological characteristics of the lesions were extracted. Table 1 shows the clinical characteristics of patients. All patients signed informed consent forms.
Case 1: A 30-year-old male was referred to the Department of Oral Medicine with a slow-growing, painless growth on the palatal aspect of the maxillary central incisor region. According to the patient, there was a similar lesion in this area 10 years earlier, which was removed. However, the result of the biopsy was unknown to us. Examination revealed an approximately 15×10×5 mm, coral pinkish, smooth, and dome-shaped lesion with a firm consistency. The patient reported no pain during the examination. The clinical diagnosis of fibroma was made.
Although GCF lesions are usually smaller than 1 cm, this lesion was larger than average. Histological examination showed the presence of specific giant stellate fibroblasts and therefore the diagnosis of GCF was made.
Case 2: A 39-year-old female was referred to Shahab Dental Clinic with a pedunculated lesion in her right buccal mucosa from 18 months earlier that affected her mastication and caused discomfort. On clinical examination, the lesion was nontender, polypoid, and coral pinkish in color. However, it had a firmer consistency than a classic fibroma. Excisional biopsy of the lesion was compatible with GCF despite its rarity in the buccal mucosa.
Case 3: A 14-year-old girl was referred to the Department of Oral Medicine with a six-month history of a swelling on the palatal aspect of her upper central incisors. Clinical examination revealed an exophytic polypoid lesion with a firm consistency and a papillary surface and white-pinkish color. There was no specific stimulatory factor, such as calculus, in the area. The clinical diagnosis was pyogenic granuloma, although microscopic evidence confirmed GCF.
Case 4: A healthy 26-year-old female was referred to the Department of Oral Medicine with an exophytic lesion on the anterior aspect of the palate. According to the patient, the lesion had developed around 4 months earlier. The lesion appeared in a polypoid form with an irregularly lobulated papillary surface and a white-pinkish color and was firm in consistency. The lesion was not fluctuating, did not blanch on pressure, and was not tender. Due to its overgrowth, deformation of the palatal surface of the incisors was evident in the labial surface of the lesion (Fig. 1). Due to its lobulated surface, the clinical diagnosis of GCF was confirmed after histopathological examination.
Case 5: A 63-year-old woman was referred to Shahab Dental Clinic, complaining of a swollen lesion on her right buccal mucosa for about 6 months. There was a small swelling in the buccal area which gradually increased in size and on examination, the lesion had been traumatized by occlusion. The exophytic pedunculated lesion had a rubbery to firm consistency. The overlying mucosa was pinkish in color and firm in consistency.
A hyperkeratotic surface with a white appearance was observed at the interference of the lesion and the occlusal line (Fig. 2), but the remaining surface was smooth. The lesion was not compressible.
Table 1: Clinical charachtristics of patients
{kind=link}
Figure 1. GCF with irregular papillary surface in case number 4; Left: Clinical appearance of GCF. Right: Hyperkeratinized and hyperplastic epithelium with a collagenized stroma containing enlarged and angular fibroblasts (H and E statin; original magnification x40)
{kind=link}
Figure 2. GCF in the buccal mucosa (an uncommon location) in case number 5; hyperkeratotic surface with whitish appearance (left) and trinuclear giant fibroblasts (right).
{kind=link}
The clinical diagnosis of fibroma was made. Due to the unusual location of the lesion, GCF was not the first differential diagnosis, although histopathological assessment confirmed GCF. It measured approximately 5 mm laterally and 8 mm in anteroposterior direction, and had 5 mm thickness.
Discussion
Although irritation fibroma, a reactive lesion, is common in adults, its histopathological variant, known as GCF, is rare [9]. GCF has some features that distinguish it from fibroma. It usually occurs in the gingiva, tongue and palate. There are only a limited number of reports about GCF in the buccal mucosa. GCF lesions are usually smaller than 1 cm. The role of trauma in development of GCF has been contradictory. In addition, reports of GCF formation in trauma-prone areas, for instance, the buccal mucosa, are increasing. Reports of GCF in Iranians are rare [7]. Although there is no specific preponderance with regard to gender of patients, there were four females and one male patient in the present study. All patients had exophytic lesions with coral to white pink color but in case number 5, there was a white area on the lesion that appeared to be due to chronic contact with the teeth. The age range of patients was 14 to 63 years old. The smallest diameter of the lesions was 4 mm and the largest diameter was 15 mm; they were often firm in consistency.
Based on the clinical appearance of the lesion, the differential diagnosis mainly includes reactive and benign neoplastic lesions, such as irritable fibroma, pyogenic granuloma, and peripheral giant cell granuloma [6]. However, some clinical criteria such as color, size, surface appearance, localization, base, and presence of stimulating factors can aid in diagnosis [5]. Kuo et al. [10] showed that GCF resembles a fibroma or papilloma and is difficult to diagnose at first glance. At first sight, a differential diagnosis of GCF was unexpected in our cases due to its unusual location.
The histological differential diagnosis also includes lesions of melanocytic or Langerhans cell origin that, unlike GCF, stain positive for S-100, or lesions of endothelial or myofibroblastic origin that stain positive for alpha smooth muscle actin [9, 11]. In GCF, epithelial hyperplasia forms spiky rete ridges. Also, giant, stellate, multinucleated fibroblast-like cells are seen that sometimes show cytoplasmic positivity for smooth muscle actin, suggesting differentiation towards myofibroblasts, and keloid-like dense collagen. Mast cells are often present similar to fibrous papules of the nose [12].
In the present study, based on the classic microscopic view of giant stellate fibroblasts, no further investigation was needed, including S100 and SMA, to confirm GCF, and the pathologic diagnosis of all cases was GCF.
The ultrastructural study of oral GCF by Weathers and Callihan [10] suggested that characteristic cells in GCF are atypical fibroblasts. The most characteristic feature was presence of a few mono-, bi- and multinucleated stellate giant cells in the subepithelial fibrous connective tissue.
Additional histopathological features include the presence of squamous epithelium at various stages of keratinization (hyperparakeratotic or hyperorthokeratotic) [13], hyperplasia, immature connective tissue with large stellate fibroblasts, and lack of granulation tissue. The presence of inflammatory cells typical of GFC supports the idea that fibroblastic differentiation might be induced by recurrent inflammation. It could also be a response to low-intensity trauma after lesion development [14].
In only two of our cases (numbers 2 and 5), with the lesion in buccal mucosa, trauma could be considered as the cause of lesions, while the remaining lesions were not exposed to trauma. Although GCF is rare, it is likely to become more common if we consider retrocuspid papilla as its subtype.
Retrocuspid papilla is a small fibrous nodule located on the gingiva, lingual to the mandibular cuspid, is usually bilateral, and affects children [11]. Retrocuspid papilla is quite common and has been reported in 25-99% of children and young adults. Its prevalence in older adults decreases to 6-19%, suggesting that the it is a normal anatomical variation that disappears with age [1].
In this study, we reported five cases of oral GCF on the maxillary gingiva, hard palate, and buccal mucosa in Iranian patients. Surgical excision was performed with a surgical blade and no recurrence of the lesions was reported in the cases in the present study.
Very few studies on GCF are available in the Iranian population. According to this case report, GCF can be considered in the list of differential diagnosis of exophytic lesions even if they have an unusual size or location.
Conclusion
GCF should be considered in the list of differential diagnosis of any exophytic lesion resembling a fibroma with unknown origin of irritation even in nontraumatic areas.
Acknowledgement
The authors would like to thank colleagues at Mashhad Dental School who provided insight and expertise. We would also like to express our gratitude to Shahab Oral Medicine and Special Care Dental Clinic. We also appreciate the patients who consented to publish their report.
In the present study, based on the classic microscopic view of giant stellate fibroblasts, no further investigation was needed, including S100 and SMA, to confirm GCF, and the pathologic diagnosis of all cases was GCF.
The ultrastructural study of oral GCF by Weathers and Callihan [10] suggested that characteristic cells in GCF are atypical fibroblasts. The most characteristic feature was presence of a few mono-, bi- and multinucleated stellate giant cells in the subepithelial fibrous connective tissue.
Additional histopathological features include the presence of squamous epithelium at various stages of keratinization (hyperparakeratotic or hyperorthokeratotic) [13], hyperplasia, immature connective tissue with large stellate fibroblasts, and lack of granulation tissue. The presence of inflammatory cells typical of GFC supports the idea that fibroblastic differentiation might be induced by recurrent inflammation. It could also be a response to low-intensity trauma after lesion development [14].
In only two of our cases (numbers 2 and 5), with the lesion in buccal mucosa, trauma could be considered as the cause of lesions, while the remaining lesions were not exposed to trauma. Although GCF is rare, it is likely to become more common if we consider retrocuspid papilla as its subtype.
Retrocuspid papilla is a small fibrous nodule located on the gingiva, lingual to the mandibular cuspid, is usually bilateral, and affects children [11]. Retrocuspid papilla is quite common and has been reported in 25-99% of children and young adults. Its prevalence in older adults decreases to 6-19%, suggesting that the it is a normal anatomical variation that disappears with age [1].
In this study, we reported five cases of oral GCF on the maxillary gingiva, hard palate, and buccal mucosa in Iranian patients. Surgical excision was performed with a surgical blade and no recurrence of the lesions was reported in the cases in the present study.
Very few studies on GCF are available in the Iranian population. According to this case report, GCF can be considered in the list of differential diagnosis of exophytic lesions even if they have an unusual size or location.
Conclusion
GCF should be considered in the list of differential diagnosis of any exophytic lesion resembling a fibroma with unknown origin of irritation even in nontraumatic areas.
Acknowledgement
The authors would like to thank colleagues at Mashhad Dental School who provided insight and expertise. We would also like to express our gratitude to Shahab Oral Medicine and Special Care Dental Clinic. We also appreciate the patients who consented to publish their report.
Type of Study: Review article |
Subject:
Oral medicine
References
1. Brad W. Neville D, Douglas D. Damm D, Carl M. Allen DDSMSD, Angela C. Chi D. Oral and Maxillofacial Pathology. United States: Elsevier Health Sciences; 2015. 873 p.
2. Weathers DR, Callihan MD. Giant-cell fibroma. Oral Surg Oral Med Oral Pathol. 1974 Mar;37(3):374-84. [DOI:10.1016/0030-4220(74)90110-8] [PMID]
3. Schmidt MJ, Tschoeke A, Noronha L, Moraes RS, Mesquita RA, Grégio AM, Alanis LR, Ignácio SA, Santos JN, Lima AA, Luiz TS, Michels AC, Aguiar MC, Johann AC. Histochemical analysis of collagen fibers in giant cell fibroma and inflammatory fibrous hyperplasia. Acta Histochem. 2016 Jun; 118 (5):451-5. [DOI:10.1016/j.acthis.2016.04.007] [PMID]
4. de Oliveira HC, Tschoeke A, da Cruz GC, Noronha L, de Moraes RS, Mesquita RA, de Aguiar MC, Caldeira PC, de Oliveira Ribas M, Grégio AM, Alanis LR, Ignácio SA, Dos Santos JN, de Lima AA, Johann AC. MMP-1 and MMP-8 expression in giant-cell fibroma and inflammatory fibrous hy-perplasia. Pathol Res Pract. 2016 Dec;212(12):1108-12. [DOI:10.1016/j.prp.2016.10.002] [PMID]
5. Mello-Moura ACV, Santos AMA, Bonini GAVC, Del Conte Zardetto CG, Moura-Netto C, Wanderley MT. Giant Cell Fibroma in a Two-Year-Old Child. Case Reports in Dentistry. 2016; 2016:7058356. [DOI:10.1155/2016/7058356] [PMID] [PMCID]
6. Sivapathasundharam B. Shafer's Textbook of Oral Pathology. 8th ed. India: Elsevier; 2016. 794 p.
7. Bagheri F, Rahmani S, Azimi S, Taheri JB. Giant cell fibroma of the buccal mucosa with laser excision: Report of unusual case. Iran J Pathol. 2015;10(4):314-7.
8. Sabarinath B, Sivaramakrishnan M, Sivapathasundharam B. Giant cell fibroma: A clinicopathological study. J Oral Maxillofac Pathol. 2012 Sep;16(3):359-62. [DOI:10.4103/0973-029X.102485] [PMID] [PMCID]
9. Sonalika WG, Sahu A, Deogade SC, Gupta P, Naitam D, Chansoria H, Agarwal J, Katoch S. Giant cell fibroma of tongue: understand-ing the nature of an unusual histopathological entity. Case Rep Dent. 2014;2014:864512. [DOI:10.1155/2014/864512] [PMID] [PMCID]
10. Kuo RC, Wang YP, Chen HM, Sun A, Liu BY, Kuo YS. Clinicopathological study of oral giant cell fibromas. J Formos Med Assoc. 2009 Sep;108(9):725-9. [DOI:10.1016/S0929-6646(09)60396-X] [PMID]
11. Shapira M, Akrish S. A 6-year-old girl with a lesion on the tongue. Giant cell fibroma of tongue. Pediatr Ann. 2011 Feb;40(2):71-4. [DOI:10.3928/00904481-20110117-05] [PMID]
12. Woo SB. Oral Pathology: A Comprehensive Atlas and Text. 2nd ed; Philadelphia, PA: Elsevier; 2016. 536 p.
13. Kuo YH, Hwang MJ, Lee YP, Chiang CP. Oral giant cell fibroma: A report of three cases. J Dent Sci. 2021 Jan; 16(1): 552-4. [DOI:10.1016/j.jds.2020.09.001] [PMID] [PMCID]
14. Braga MM, Carvalho AL, Vasconcelos MC, Braz-Silva PH, Pinheiro SL. Giant cell fibroma: a case report. J Clin Pediatr Dent. 2006 Spring;30(3):261-4. [DOI:10.17796/jcpd.30.3.j784203n931w3x6j] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |