Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 1 (3-2024)
J Res Dent Maxillofac Sci 2024, 9(1): 43-48 |
Back to browse issues page


Ethics code: IR.MEDILAM.REC1400.053
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abdal K, Yari A, Bonyadi M, Shafiei E. Predictive Role of Ectopic Calcifications on Digital Panoramic Radiographs in the West of Iran. J Res Dent Maxillofac Sci 2024; 9 (1) :43-48
URL: http://jrdms.dentaliau.ac.ir/article-1-435-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-435-en.html



1- Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Ilam University of Medical Sciences, Ilam, Iran
2- Faculty of Dentistry, Ilam University of Medical Sciences, Ilam, Iran
3- Non-Communicable Diseases Research Center, Ilam University of Medical Sciences,Ilam,Iran
4- Clinical Research Development Unit, Ayatollah Taleghani Hospital, Ilam University of Medical Sciences, Ilam, Iran ,shafiei-e@medilam.ac.ir
2- Faculty of Dentistry, Ilam University of Medical Sciences, Ilam, Iran
3- Non-Communicable Diseases Research Center, Ilam University of Medical Sciences,Ilam,Iran
4- Clinical Research Development Unit, Ayatollah Taleghani Hospital, Ilam University of Medical Sciences, Ilam, Iran ,
Full-Text [PDF 245 kb]
(702 Downloads)
| Abstract (HTML) (2569 Views)
Full-Text: (753 Views)
Abstract
Background and Aim: Although soft tissue calcifications are relatively common and are commonly seen on panoramic radiographs, few studies have reported their causes. Therefore, the present study was conducted to investigate the relationship between systemic diseases and ectopic calcifications.
Materials and Methods: In this descriptive study, the study population included patients referred to the Radiology Department of two specialized dental clinics in Ilam and Kermanshah cities from 2020-2021. A total of 1000 participants were voluntarily examined. The collected data were analyzed using the correlation and logistic regression tests.
Results: The prevalence of calcifications was 39.4% in Ilam and 27.6% in Kermanshah. Also, the results showed that there was a significant relationship between systemic diseases and calcifications (P<0.05). The correlation coefficient between systemic diseases and calcifications was r=0.76 (P=0.02) in Ilam, and r=0.84 (P=0.00) in Kermanshah. Age and sex could not predict calcifications (P>0.05).
Conclusion: Based on the findings, calcifications on panoramic radiographs may serve as a predictor for presence of systemic diseases.
Key Words: Prevalence; Calcification, Physiologic; Calcinosis; Radiography, Panoramic; Iran
Materials and Methods: In this descriptive study, the study population included patients referred to the Radiology Department of two specialized dental clinics in Ilam and Kermanshah cities from 2020-2021. A total of 1000 participants were voluntarily examined. The collected data were analyzed using the correlation and logistic regression tests.
Results: The prevalence of calcifications was 39.4% in Ilam and 27.6% in Kermanshah. Also, the results showed that there was a significant relationship between systemic diseases and calcifications (P<0.05). The correlation coefficient between systemic diseases and calcifications was r=0.76 (P=0.02) in Ilam, and r=0.84 (P=0.00) in Kermanshah. Age and sex could not predict calcifications (P>0.05).
Conclusion: Based on the findings, calcifications on panoramic radiographs may serve as a predictor for presence of systemic diseases.
Key Words: Prevalence; Calcification, Physiologic; Calcinosis; Radiography, Panoramic; Iran
Introduction
Deposition of calcium salts, mainly calcium phosphate, usually occurs in bones. However, if it occurs in the soft tissue in an unorganized manner, it is called heterotopic calcification. Soft tissue calcifications are common in the maxillofacial region [1], and include calcifications of the lymph nodes, ossification of the stylohyoid complex, calcification of the tonsils, rhinolith, enterolith, calcification of the carotid bifurcation area, sialolith, myositis ossificans, and otomycosis [2]. These calcifications may occur in arteries, ligaments, and glandular tissues with chronic inflammation and scarring [3]. Presence of the-se calcifications may be due to various factors such as age, sex, place of residence, and systemic diseases [4-6].
Stroke is the third leading cause of death in different countries. Carotid artery calcification is also common in patients at risk of stroke, which is seen on panoramic radiographs approximately between the C3 and C4 vertebrae near the hyoid bone [7]. Therefore, presence of carotid artery plaque on panoramic images can indicate a risk of future cardiovascular events. As a result of early diagnosis, it will be possible to benefit from early intervention and reduce mortality and complications [7-9]. Arzani and Ahmadi showed that the highest prevalence of soft tis-sue calcifications was related to the stylohyoid ligament [10]. Typically, calcified areas do not cause any specific signs or symptoms or have nonspecific symptoms such as tonsillitis that can cause a foreign body sensation, dysphagia, earache, and unstimulated cough.
In general, soft tissue calcifications are common and are usually 4% visible on panoramic images. They are usually identified as random findings during routine radiographic examinations. Some of these calcifications do not require any intervention or long-term care, while others may be life-threatening and the existing underlying cause needs to be investigated and treated [11]. What is important for a dentist is the ability to differentiate between anatomical calcified bone structures and calcification of the aorta, thyroid cartilage, lymph nodes, submandibular glands and tonsils, and phleboliths [12].
Panoramic radiography is inexpensive for patients and can be used to examine the jaw and teeth in most dental treatments. On the other hand, on most of these radiographs, misplaced soft tissue calcifications can be seen to some extent. Therefore, dentists should be careful not to ignore any unusual finding and contribute to reducing the burden of more serious complications of diseases by timely referral of patients to a physician.
In order to make a correct diagnosis and prevent incorrect unnecessary treatments, it is necessary to know the prevalence of soft tissue calcifications in different geographical regions. On the other hand, due to the small number of studies on the correlation of systemic diseases and soft tissue calcifications in Iran, and lack of such studies in the west of Iran (Ilam and Kermanshah Provinces), this study aimed to investigate the relationship between systemic diseases and soft tissue calcifications detectable on panoramic radiographs in a population in the western Iran.
Materials and Methods
The present descriptive analytical study was conducted in 2020-2021 in two specialized dental clinics in Ilam and Kermanshah cities. A total of 1600 people referred to the radiology department of two specialized dental clinics in Ilam and Kermanshah, for whom panoramic radiography had been requested for various reasons not related to this study were selected and enrolled by convenience sampling. Of all, 335 people had different types of calcifications.The exclusion criteria were radiographs showing pathologies, history of maxillofacial or bone surgeries, and poor-quality radiographs. The inclusion criterion was presence of soft tissue calcifications. All participants were informed about the study and its objectives, and their rights including the right to withdraw from the study and the confidentiality of their information. Verbal and informed consent was obtained from all participants. The study was approved by the ethics research committee of Ilam University of Medical Sciences (IR.MEDILAM.REC1400.053). All radiographs had been taken by Planmeca PM 2002 CC
Proline Panoramic X-ray device (Planmeca, Helsinki, Finland) with no technical or processing errors. The maximum voltage was 80 kV, amperage was 12 mA, and scanning time was 18 seconds, which could change depending on patient conditions.
Demographic characteristics (sex, age, underlying conditions, history of heart disease, hypertension and smoking, smoking duration, and frequency, etc.) of all participants were recorded. All radiographs were accurately examined by an independent radiologist. The evaluations were conducted two times, and an intra-class correlation coefficient of more than 0.85 was deemed to be a sign of excellent intra-examiner reliability. The radiologist assessed the calcifications in various locations of the head and neck, determining their quantity and category by using the diagnostic criteria.
After collecting the data, the Kolmogorov-Smirnov test was used to assess the normal distribution of data. Due to the type of data and non-normal distribution of some variables, the Kendall correlation test was used to investigate the relationship between the research variables. In addition, the odds ratios were calculated. Multiple logistic regression test was used for predictions. Significance level was considered at 0.05. All analyses were performed using SPSS version 19 (SPSS Inc., Chicago, USA).
Results
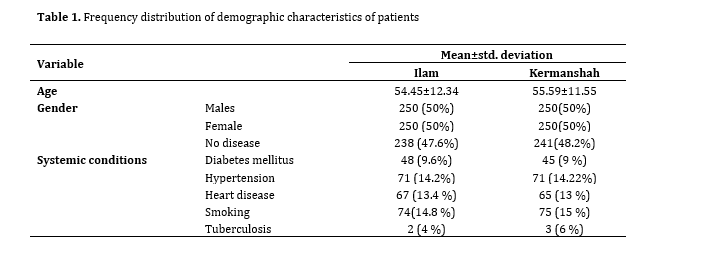
A total of 1000 radiographs were evaluated. The mean age was 54.45±12.34 years in Ilam and 55.59±11.55 years in Kermanshah (range 30-70 years), and the study population included 250 males and 250 females in each province. Among the study samples, it was found that 47.6% of individuals in Ilam and 48.2% of individuals in Kermanshah had no disease. The most commonly observed conditions in the study samples were smoking and hypertension (Table 1).
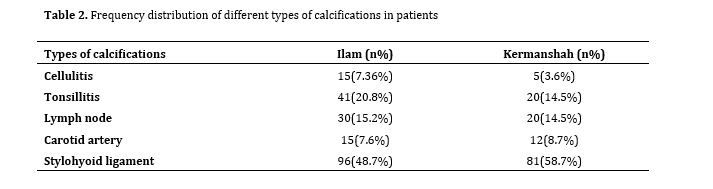
A total of 197 calcifications were found in the participants from Ilam and 138 calcifications were found in the participants from Kermanshah. The stylohyoid ligament calcification had the highest prevalence in Ilam (n=96, 48.7%) and also in Kermanshah (n=81, 58.7%). Cellulitis had the lowest prevalence in Ilam (n=15, 7.6%), and also in Kermanshah (n=5, 3.6%). The frequency and prevalence of other types of calcifications are listed in Table 2.
The highest frequency of calcifications was found in males in the age group of over 40 years. In addition, among the individuals over the age of 40 years, the most commonly observed ligament calcification was the stylohyoid ligament calcification, which was seen in 70.7% of males and 29.3% of females in Ilam Province, and 38.9% of males and 61.1% of females in Kermanshah Province. According to the Chi-square test, there was no significant relationship between age and calcification in the two provinces. Also, based on Fisher's exact test, no significant relationship was found between sex and calcifications in the two provinces (Table 3).
The results showed that in both groups, there was a significant relationship between systemic diseases and calcifications.
The correlation coefficient between systemic diseases and calcifications was r=0.76 (P=0.02) in Ilam, and r=0.84 (P=0.00) in Kermanshah.
Deposition of calcium salts, mainly calcium phosphate, usually occurs in bones. However, if it occurs in the soft tissue in an unorganized manner, it is called heterotopic calcification. Soft tissue calcifications are common in the maxillofacial region [1], and include calcifications of the lymph nodes, ossification of the stylohyoid complex, calcification of the tonsils, rhinolith, enterolith, calcification of the carotid bifurcation area, sialolith, myositis ossificans, and otomycosis [2]. These calcifications may occur in arteries, ligaments, and glandular tissues with chronic inflammation and scarring [3]. Presence of the-se calcifications may be due to various factors such as age, sex, place of residence, and systemic diseases [4-6].
Stroke is the third leading cause of death in different countries. Carotid artery calcification is also common in patients at risk of stroke, which is seen on panoramic radiographs approximately between the C3 and C4 vertebrae near the hyoid bone [7]. Therefore, presence of carotid artery plaque on panoramic images can indicate a risk of future cardiovascular events. As a result of early diagnosis, it will be possible to benefit from early intervention and reduce mortality and complications [7-9]. Arzani and Ahmadi showed that the highest prevalence of soft tis-sue calcifications was related to the stylohyoid ligament [10]. Typically, calcified areas do not cause any specific signs or symptoms or have nonspecific symptoms such as tonsillitis that can cause a foreign body sensation, dysphagia, earache, and unstimulated cough.
In general, soft tissue calcifications are common and are usually 4% visible on panoramic images. They are usually identified as random findings during routine radiographic examinations. Some of these calcifications do not require any intervention or long-term care, while others may be life-threatening and the existing underlying cause needs to be investigated and treated [11]. What is important for a dentist is the ability to differentiate between anatomical calcified bone structures and calcification of the aorta, thyroid cartilage, lymph nodes, submandibular glands and tonsils, and phleboliths [12].
Panoramic radiography is inexpensive for patients and can be used to examine the jaw and teeth in most dental treatments. On the other hand, on most of these radiographs, misplaced soft tissue calcifications can be seen to some extent. Therefore, dentists should be careful not to ignore any unusual finding and contribute to reducing the burden of more serious complications of diseases by timely referral of patients to a physician.
In order to make a correct diagnosis and prevent incorrect unnecessary treatments, it is necessary to know the prevalence of soft tissue calcifications in different geographical regions. On the other hand, due to the small number of studies on the correlation of systemic diseases and soft tissue calcifications in Iran, and lack of such studies in the west of Iran (Ilam and Kermanshah Provinces), this study aimed to investigate the relationship between systemic diseases and soft tissue calcifications detectable on panoramic radiographs in a population in the western Iran.
Materials and Methods
The present descriptive analytical study was conducted in 2020-2021 in two specialized dental clinics in Ilam and Kermanshah cities. A total of 1600 people referred to the radiology department of two specialized dental clinics in Ilam and Kermanshah, for whom panoramic radiography had been requested for various reasons not related to this study were selected and enrolled by convenience sampling. Of all, 335 people had different types of calcifications.The exclusion criteria were radiographs showing pathologies, history of maxillofacial or bone surgeries, and poor-quality radiographs. The inclusion criterion was presence of soft tissue calcifications. All participants were informed about the study and its objectives, and their rights including the right to withdraw from the study and the confidentiality of their information. Verbal and informed consent was obtained from all participants. The study was approved by the ethics research committee of Ilam University of Medical Sciences (IR.MEDILAM.REC1400.053). All radiographs had been taken by Planmeca PM 2002 CC
Proline Panoramic X-ray device (Planmeca, Helsinki, Finland) with no technical or processing errors. The maximum voltage was 80 kV, amperage was 12 mA, and scanning time was 18 seconds, which could change depending on patient conditions.
Demographic characteristics (sex, age, underlying conditions, history of heart disease, hypertension and smoking, smoking duration, and frequency, etc.) of all participants were recorded. All radiographs were accurately examined by an independent radiologist. The evaluations were conducted two times, and an intra-class correlation coefficient of more than 0.85 was deemed to be a sign of excellent intra-examiner reliability. The radiologist assessed the calcifications in various locations of the head and neck, determining their quantity and category by using the diagnostic criteria.
After collecting the data, the Kolmogorov-Smirnov test was used to assess the normal distribution of data. Due to the type of data and non-normal distribution of some variables, the Kendall correlation test was used to investigate the relationship between the research variables. In addition, the odds ratios were calculated. Multiple logistic regression test was used for predictions. Significance level was considered at 0.05. All analyses were performed using SPSS version 19 (SPSS Inc., Chicago, USA).
Results
A total of 1000 radiographs were evaluated. The mean age was 54.45±12.34 years in Ilam and 55.59±11.55 years in Kermanshah (range 30-70 years), and the study population included 250 males and 250 females in each province. Among the study samples, it was found that 47.6% of individuals in Ilam and 48.2% of individuals in Kermanshah had no disease. The most commonly observed conditions in the study samples were smoking and hypertension (Table 1).
A total of 197 calcifications were found in the participants from Ilam and 138 calcifications were found in the participants from Kermanshah. The stylohyoid ligament calcification had the highest prevalence in Ilam (n=96, 48.7%) and also in Kermanshah (n=81, 58.7%). Cellulitis had the lowest prevalence in Ilam (n=15, 7.6%), and also in Kermanshah (n=5, 3.6%). The frequency and prevalence of other types of calcifications are listed in Table 2.
The highest frequency of calcifications was found in males in the age group of over 40 years. In addition, among the individuals over the age of 40 years, the most commonly observed ligament calcification was the stylohyoid ligament calcification, which was seen in 70.7% of males and 29.3% of females in Ilam Province, and 38.9% of males and 61.1% of females in Kermanshah Province. According to the Chi-square test, there was no significant relationship between age and calcification in the two provinces. Also, based on Fisher's exact test, no significant relationship was found between sex and calcifications in the two provinces (Table 3).
The results showed that in both groups, there was a significant relationship between systemic diseases and calcifications.
The correlation coefficient between systemic diseases and calcifications was r=0.76 (P=0.02) in Ilam, and r=0.84 (P=0.00) in Kermanshah.
Table 1. Frequency distribution of demographic characteristics of patients
Table 2. Frequency distribution of different types of calcifications in patients
Table 3. Frequency distribution of different types of calcifications based on age and sex of patients
Discussion
Since soft tissue calcifications can be affected by lifestyle or even racial and ethnic differences, and considering the scarcity of studies on soft tissue radiopacities and their importance in Iran, the present study aimed to investigate the relationship between systemic diseases and ectopic calcifications on digital panoramic radiographs in the west of Iran.
In this study, the prevalence of calcifications were 39.4% in Ilam and 27.6 % in Kermanshah. While in the study by Ezoddini-Ardakani et al., the prevalence of soft tissue calcifications was 29.2% [13]. This value was 6.4% in the study by Icoz and Akgunlu. [14] and 6.4% in the study by ImaniMoghaddam et al. [15] which was con-sistent with the present results. The variation in prevalence rates reported in the studies mentioned above may be due to the fact that stylohyoid calcification was not taken into consideration, or some cases were not included in the analysis. The prevalence of stylohyoid calcification varies from 2% to 30% in the literature [16]. Variations in the reported rates can be due to different sample selections and differences in radiographic indices for detection of calcifications. In the present study, the rate of calcification in different soft tissue areas significantly increased with age, but ImaniMoghaddam et al. [15] reported an increase in stylohyoid ligament length with age. Also, Watanabe et al. showed that the prevalence of calcifications increased with age, and the highest prevalence of calcified stylohyoid ligament was observed between 50 and 69 years of age [17].
The most common type of calcification was stylohyoid ligament calcification in Ilam (48.7%) and also in Kermanshah (58.7%), and the least common calcification was cellulitis in Ilam (7.36%) and also in Kermanshah (3.6%). Ezoddini-Ardakani et al. [13] reported the highest prevalence for stylohyoid ligament calcification (54%).
Ribeiro et al. [18] reported a prevalence of 66%, and Watanabe et al. [17] reported a prevalence of 18% for stylohyoid ligament calcification. Omami considered this type of calcification to be a common finding on panoramic radiographs [19]. After stylohyoid ligament calcification, tonsillitis and lymph node calcification had the highest frequency in Kermanshah and Ilam, which was almost consistent with the results of studies by ImaniMoghaddam et al. [15] and Ezoddini-Ardakani et al. [13] in Iran. In a study by Sutter et al. [20], the prevalence of calcification was reported to be 3.6% in southern Austria.
The highest frequency of calcifications was in males in the age group of over 40 years. In a study by Shakibaei et al., [16] a high prevalence of stylohyoid ligament calcification in the age group of 20 to 40 years and without any relationship with gender was reported. No significant relationship was reported between age and sex with calcification. According to the results obtained in the study by Icoz and Akgunlu, the mean age of the study population could not be considered as a good predictor of the prevalence of soft tissue calcifications [14]. In a study of Bamgbose et al. [21], tonsillitis did not have a significant relationship with gender. It should also be noted that in their study, only the prevalence of tonsillitis in the United States was studied [21], which is consistent with the present study. In the present study, the lowest observed frequency was related to sialolith. In some other similar studies, the frequency of sialolith was lower than other soft tissue calcifications [14,16,18,22].
In the present study, carotid calcification was seen in males over 40 years of age, and according to Guimarães Henriques et al. [23], the process of vascular calcification begins at an early age and manifests after 45 years. The prevalence of carotid calcification was reported to be 7.6% in Ilam and 8.7% in Kermanshah. Vengalath et al. [22] estimated this rate to be between 2-11%, which was not much different from the present result.
In both provinces, a significant relationship was reported between systemic diseases and calcifications. The most frequently observed systemic conditions in Ilam and Kermanshah were smoking, hypertension, and heart disease. However, according to Haghighat et al, [24] heart disease and hypertension had the highest prevalence. Ezoddini-Ardakani et al. [13] showed that hypertension increased the risk of calcification by 7 times. The results of the present study showed that tobacco consumption increased the risk of calcification by 2.3 times.
It is important to note that the sample size of this study was much higher than that of previous studies. Due to the fact that in this study, panoramic radiographs of dental clinics were used, there were no special restrictions.
Conclusion
The study revealed a significant association between systemic diseases and calcifications, indicating that systemic diseases increase the likelihood of calcifications. However, age and sex were not found to be predictive factors for calcifications.
Acknowledgement
We would like to thank our co-workers in dental clinics of Ilam, Iran.
Funding
This study was supported by the Deputy of Research of Ilam University of Medical Sciences.
Availability of data and materials
The datasets used and/or analyzed in the current study can be obtained from the corresponding author on reasonable request.
Competing interests
The authors declare no conflict of interests.
{kind=link}
Table 2. Frequency distribution of different types of calcifications in patients
{kind=link}
Table 3. Frequency distribution of different types of calcifications based on age and sex of patients
{kind=link}
Discussion
Since soft tissue calcifications can be affected by lifestyle or even racial and ethnic differences, and considering the scarcity of studies on soft tissue radiopacities and their importance in Iran, the present study aimed to investigate the relationship between systemic diseases and ectopic calcifications on digital panoramic radiographs in the west of Iran.
In this study, the prevalence of calcifications were 39.4% in Ilam and 27.6 % in Kermanshah. While in the study by Ezoddini-Ardakani et al., the prevalence of soft tissue calcifications was 29.2% [13]. This value was 6.4% in the study by Icoz and Akgunlu. [14] and 6.4% in the study by ImaniMoghaddam et al. [15] which was con-sistent with the present results. The variation in prevalence rates reported in the studies mentioned above may be due to the fact that stylohyoid calcification was not taken into consideration, or some cases were not included in the analysis. The prevalence of stylohyoid calcification varies from 2% to 30% in the literature [16]. Variations in the reported rates can be due to different sample selections and differences in radiographic indices for detection of calcifications. In the present study, the rate of calcification in different soft tissue areas significantly increased with age, but ImaniMoghaddam et al. [15] reported an increase in stylohyoid ligament length with age. Also, Watanabe et al. showed that the prevalence of calcifications increased with age, and the highest prevalence of calcified stylohyoid ligament was observed between 50 and 69 years of age [17].
The most common type of calcification was stylohyoid ligament calcification in Ilam (48.7%) and also in Kermanshah (58.7%), and the least common calcification was cellulitis in Ilam (7.36%) and also in Kermanshah (3.6%). Ezoddini-Ardakani et al. [13] reported the highest prevalence for stylohyoid ligament calcification (54%).
Ribeiro et al. [18] reported a prevalence of 66%, and Watanabe et al. [17] reported a prevalence of 18% for stylohyoid ligament calcification. Omami considered this type of calcification to be a common finding on panoramic radiographs [19]. After stylohyoid ligament calcification, tonsillitis and lymph node calcification had the highest frequency in Kermanshah and Ilam, which was almost consistent with the results of studies by ImaniMoghaddam et al. [15] and Ezoddini-Ardakani et al. [13] in Iran. In a study by Sutter et al. [20], the prevalence of calcification was reported to be 3.6% in southern Austria.
The highest frequency of calcifications was in males in the age group of over 40 years. In a study by Shakibaei et al., [16] a high prevalence of stylohyoid ligament calcification in the age group of 20 to 40 years and without any relationship with gender was reported. No significant relationship was reported between age and sex with calcification. According to the results obtained in the study by Icoz and Akgunlu, the mean age of the study population could not be considered as a good predictor of the prevalence of soft tissue calcifications [14]. In a study of Bamgbose et al. [21], tonsillitis did not have a significant relationship with gender. It should also be noted that in their study, only the prevalence of tonsillitis in the United States was studied [21], which is consistent with the present study. In the present study, the lowest observed frequency was related to sialolith. In some other similar studies, the frequency of sialolith was lower than other soft tissue calcifications [14,16,18,22].
In the present study, carotid calcification was seen in males over 40 years of age, and according to Guimarães Henriques et al. [23], the process of vascular calcification begins at an early age and manifests after 45 years. The prevalence of carotid calcification was reported to be 7.6% in Ilam and 8.7% in Kermanshah. Vengalath et al. [22] estimated this rate to be between 2-11%, which was not much different from the present result.
In both provinces, a significant relationship was reported between systemic diseases and calcifications. The most frequently observed systemic conditions in Ilam and Kermanshah were smoking, hypertension, and heart disease. However, according to Haghighat et al, [24] heart disease and hypertension had the highest prevalence. Ezoddini-Ardakani et al. [13] showed that hypertension increased the risk of calcification by 7 times. The results of the present study showed that tobacco consumption increased the risk of calcification by 2.3 times.
It is important to note that the sample size of this study was much higher than that of previous studies. Due to the fact that in this study, panoramic radiographs of dental clinics were used, there were no special restrictions.
Conclusion
The study revealed a significant association between systemic diseases and calcifications, indicating that systemic diseases increase the likelihood of calcifications. However, age and sex were not found to be predictive factors for calcifications.
Acknowledgement
We would like to thank our co-workers in dental clinics of Ilam, Iran.
Funding
This study was supported by the Deputy of Research of Ilam University of Medical Sciences.
Availability of data and materials
The datasets used and/or analyzed in the current study can be obtained from the corresponding author on reasonable request.
Competing interests
The authors declare no conflict of interests.
Type of Study: Original article |
Subject:
Radiology
References
1. Alkhatib SG, Shah KA, Abrams KJ. Imaging of Calcifying and Ossifying Disorders of the Spine. Neurographics 2021; 11 (1):49-58. [DOI:10.3174/ng.2000051]
2. Maia PRL, Tomaz AFG, Maia EFT, Lima KC, Oliveira PT. Prevalence of soft tissue calcifications in panoramic radiographs of the maxillofacial region of older adults. Gerodontology. 2021 Jun 24. [DOI:10.1111/ger.12578] [PMID]
3. Withana T, Maheshwari N, Ng A, Syed A. A pictorial review of soft tissue calcifications in the head and neck region. In: The 23rd International Congress of DentoMaxilloFacial Radiology (ICDMFR). 2021: Gwangju, South Korea.
4. Birudaraju D, Cherukuri L, Pranesh S, Budoff MJ. Current methods to assess mitral annular calcification and its risk factors. Expert Rev Cardiovasc Ther. 2021 Sep;19(9):787-800. [DOI:10.1080/14779072.2021.1964361] [PMID]
5. Raggi P, Bellasi A. Prevalence and Progression of Cardiovascular Calcification in the General Population and Patients with Chronic Kidney Disease. In: McCullough PA, Ronco C, editors. Textbook of Cardiorenal Medicine. Cham: Springer International Publishing; 2021. p. 7-18. [DOI:10.1007/978-3-030-57460-4_2] []
6. Leow K, Szulc P, Schousboe JT, Kiel DP, Teixeira-Pinto A, Shaikh H, Sawang M, Sim M, Bondonno N, Hodgson JM, Sharma A, Thompson PL, Prince RL, Craig JC, Lim WH, Wong G, Lewis JR. Prognostic Value of Abdominal Aortic Calcification: A Systematic Review and Meta-Analysis of Observational Studies. J Am Heart Assoc. 2021 Jan 19;10(2): e017205. [DOI:10.1161/JAHA.120.017205] [PMID] []
7. Sinjab AZ, Soman C, Sahab LA. Prevalence of carotid artery calcifications in Riyadh from digital panoramic radiographs and its relationship with cardiovascular disorders: A retrospective cross-sectional study. Saudi J Oral Sci 2021; 8: 28-32. [DOI:10.4103/sjos.SJOralSci_78_20]
8. de Onofre NML, Vizzotto MB, Wanzeler AMV, da Silveira Tiecher PF, Arús NA, Guillén LEA, et al. Association between internal carotid artery calcifications detected as incidental findings and clinical characteristics associated with atherosclerosis: A dental volumetric tomography study. European Journal of Radiology. 2021;145:110045. [DOI:10.1016/j.ejrad.2021.110045] [PMID]
9. Kermanshah H, Geramy A, Ebrahimi SF, Bitaraf T. IPS-Empress II inlay-retained fixed partial denture reinforced with zirconia bar: three-dimensional finite element and in-vitro studies. Acta Odontol Scand. 2012 Dec;70(6):569-76. [DOI:10.3109/00016357.2011.640283] [PMID]
10. Arzani V, Ahmadi P. Evaluation of Stylohyoid Complex Patterns on Digital Panoramic Radiographs in the Local Population in Ilam, Iran. AJDR 2021;13(1):23-7. [DOI:10.34172/ajdr.2021.05]
11. Arya N, Ranjbar F, Mohamadi S, Keyhan AM. Evaluation of Prevalence of Ectopic Calcification in Digital Panoramic Radiography in Patients Referred To Radiology Department of Bushehr Dental School During 2018. Journal of Mashhad Dental School. 2019;43(3):217-26.
12. Imanimoghaddam M, Tohidi E, Yazdi AA, Nikbakhsh E, Goudarzi F. Incidental Findings in Digital Panoramic Radiography of Patients Referred to Mashhad Dental School. Journal of Kerman University of Medical Sciences. 2021; 28 (1):43-55.
13. Ezoddini-Ardakani F, Kheirollahi Kh, Kheirollahi H. A prevalence study on ectopic calcification in digital panoramic radiographs in Shahid Sadoughi Dental School of Yazd in 2012-2013. J Shahid Sadoughi Univ Med Sci 2013; 21(3 Suppl): 384-94.
14. Icoz D, Akgunlu F. Prevalence of detected soft tissue calcifications on digital panoramic radiographs. SRM J Res Dent Sci 2019;10(1):21-5. [DOI:10.4103/srmjrds.srmjrds_60_18]
15. ImaniMoghaddam M, JavadzadehBluori A, AhmadianYazdi A, Daneshvar F. A One Year Prevalence Study on Soft Tissue Opacities in Panorarnic Radiography in Patients Referred to Radiology Department of Mashhad Dental School. Journal of Mashhad Dental School. 2010; 34 (4):271-80.
16. Shakibaei Z, Tohidi E, Salemi F, Saati S. Prevalence of Stylohyoid Ligament Calcification on Panoramic Radiographs in an Iranian Population. J Dent Mater Tech 2015; 4(1): 21-8.
17. Watanabe PC, Dias FC, Issa JP, Monteiro SA, de Paula FJ, Tiossi R. Elongated styloid process and atheroma in panoramic radiography and its relationship with systemic osteoporosis and osteopenia. Osteoporos Int. 2010 May; 21 (5):831-6. [DOI:10.1007/s00198-009-1022-y] [PMID]
18. Ribeiro A, Keat R, Khalid S, Ariyaratnam S, Makwana M, do Pranto M, Albuquerque R, Monteiro L. Prevalence of calcifications in soft tissues visible on a dental pantomogram: A retrospective analysis. J Stomatol Oral Maxillofac Surg. 2018 Nov;119(5):369-74. [DOI:10.1016/j.jormas.2018.04.014] [PMID]
19. Omami G. Soft tissue calcification in oral and maxillofacial imaging: a pictorial review. Int J Dentistry Oral Sci 2016;3(4):219-24. [DOI:10.19070/2377-8075-1600046]
20. Sutter W, Berger S, Meier M, Kropp A, Kielbassa AM, Turhani D. Cross-sectional study on the prevalence of carotid artery calcifications, tonsilloliths, calcified submandibular lymph nodes, sialoliths of the submandibular gland, and idiopathic osteosclerosis using digital panoramic radiography in a Lower Austrian subpopulation. Quintessence Int. 2018 Jan 22:231-42.
21. Bamgbose BO, Ruprecht A, Hellstein J, Timmons S, Qian F. The prevalence of tonsilloliths and other soft tissue calcifications in patients attending oral and maxillofacial radiology clinic of the university of iowa. ISRN Dent. 2014 Jan 22;2014:839635. [DOI:10.1155/2014/839635] [PMID] []
22. Vengalath J, Puttabuddi JH, Rajkumar B, Shivakumar GC. Prevalence of soft tissue calcifications on digital panoramic radiographs: A retrospective study. J Indian Acad Oral Med Radiol 2014;26(4):385-89. [DOI:10.4103/0972-1363.155676]
23. Guimarães Henriques JC, Kreich EM, Helena Baldani M, Luciano M, Cezar de Melo Castilho J, Cesar de Moraes L. Panoramic radiography in the diagnosis of carotid artery atheromas and the associated risk factors. Open Dent J. 2011;5:79-83. [DOI:10.2174/1874210601105010079] [PMID] []
24. Haghighat ASJ, Nikbin A, Sajedikia S. Prevalence of Soft Tissue Calcifications in Panoramic Radiographs of Patients Referred to Guilan School of Dentistry Within 1 Year and its Relationship With Systemic Diseases. Avicenna J Dent Res. 2019;11(1):15-20. [DOI:10.34172/ajdr.2019.03]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |