Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 119-127 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zolfagharloo F, Nasr N, Tavakkol O, Momayezinejad M. Effect of Crown Dimensions on Stress Distribution in Implant Abutment Screw: A 3D Finite Element
Analysis. J Res Dent Maxillofac Sci 2023; 8 (2) :119-127
URL: http://jrdms.dentaliau.ac.ir/article-1-400-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-400-en.html



1- Private Dentistry Practice, Shiraz, Iran
2- Department of Periodontics, School of Dentistry, Shiraz Islamic Azad University, Shiraz, Iran
3- Department of Prosthodontics, School of Dentistry, Shiraz Islamic Azad University, Shiraz, Iran ,omidtavakkol@yahoo.com
2- Department of Periodontics, School of Dentistry, Shiraz Islamic Azad University, Shiraz, Iran
3- Department of Prosthodontics, School of Dentistry, Shiraz Islamic Azad University, Shiraz, Iran ,
Keywords: Dental Implants, Dental Prosthesis Design, Dental Stress Analysis, Finite Element Analysis
Full-Text [PDF 1056 kb]
(2278 Downloads)
| Abstract (HTML) (3191 Views)
Introduction
Dental implant is the best option for replacement of the lost teeth, aiming to replace the lost tissue and restore function, comfort, esthetics, speech, and tissue health. The main reason for selection of dental implant for replacement of the lost teeth is to preserve the alveolar bone [1]. Intraosseous dental implants are alloplastic materials that are surgically inserted in the residual alveolar ridge to serve as a prosthetic abutment [2,3]. Stresses above the normal level can cause complications and damage the implant components [4].
Abutment is part of the implant that maintains the prosthetic part or the suprastructure [1]. The suprastructure is a metal framework that is connected to the abutment and provides retention for removable prostheses (e.g., the cast metal bar of overdenture) and forms the metal framework of fixed partial dentures [5].
Abutment screw is the easiest, most reliable, and most efficient component for fixation of prosthetic components to the implant body. Abutment screw provides easy retention in a small scale [1,6,7].
High stress levels can cause microcracks in bone and lead to bone resorption or mechanical failure of implant or prosthetic components such as porcelain fracture, abutment screw loosening, and abutment screw fracture [8,9].
Unlike the reversible signs and symptoms shown by the natural teeth, bone resorption around dental implants or restoration loosening may occur with no alarming sign/symptom. Abutment screw loosening is a sign of presence of biomechanical stresses exceeding the tolerance threshold of the
assembly. Implant crowns rarely show clinical signs and symptoms other than fatigue and fracture. Resultantly, dental clinicians have little or no diagnostic evidence to decrease the level of stress applied to the supporting system [10].
Prosthetic screw fracture occurs in both fixed partial and complete dentures with a mean prevalence rate of 4% (range 0% to 19%). Abutment screw fracture occurs less commonly than prosthetic screw fracture due to having a larger diameter. Abutment screw loosening averagely occurs in 6% of implant prostheses [11]. The higher the level of stress applied to prosthesis, the higher the risk of abutment screw loosening would be.
Cantilevers increase the risk of screw loosening because increasing the loads applied to the implant assembly has a direct correlation with the cantilever length. The higher the crown height attached to the abutment, the higher the load applied to the screw and the risk of screw loosening (or fracture) would be [12].
Single-unit crowns show the highest rate of abutment screw loosening. Screw loosening has significant complications. A loose screw can cause crestal bone loss [13]. Abutment screw loosening in a cement-retained restoration necessitates perforation of crown to access the abutment screw. Chronic screw loosening can be costly and time-consuming. Evidence shows that 6% to 20% of maxillary prostheses show screw loosening at least once in their first year of function [14,15].
Any occlusal imbalance, poor adaptation of casting, or unequal forces can cause vibration of crown under function and lead to screw loosening or fracture (when the applied load is too high or the metal dimensions are too small) [16]. External forces that are exerted to the abutment screw significantly increase the risk of screw loosening. Such forces are referred to as detach or detorque forces if cause screw loosening. Such forces are considered as risk factors for implant fracture, crestal bone loss, and component fracture. When the screws are tightened and subjected to occlusal forces with no detaching force, they remain tightened for long. However, if the external detach forces exceed the screw tightening forces (known as the interlocking forces), screw loosening occurs [17]. Thus, external forces caused by parafunction, crown height, mastication dynamics, position in dental arch, and opposing teeth are factors that highly increase the stresses applied to the implant and screw [18]. Also, predictors of such conditions such as cantilevers, angulated forces, and poor occlusal schemes should be taken into account [16].
This study aimed to assess the effect of vertical and horizontal dimensions of the crown on stress distribution in the abutment screw upon load application by three-dimensional (3D) finite element analysis (FEA).
Materials and Methods
A computed tomography (CT) scan of a patient obtained in Namazi Hospital, Shiraz was randomly selected and used in this study. Implants with 11.5-, 10-, and 8.5-mm height and 4-mm diameter (AnyRidge, MegaGen, Daegu, Korea) and straight abutments underwent 3D scanning by a 3D scanner composed of an industrial camera and a light source, and the data regarding the mandible, fixture, crown and abutment geometry were transferred to a software.
For 3D designing of the teeth, some cases were randomly selected according to the following criteria:
-CT scan of patients between 18 to 40 years
-Absence of systemic diseases
-Absence of bone diseases
-No smoking
-No use of alcoholic beverages
CT scan of a 20-year-old female was finally selected. Materialise Mimics Research version 21 (Materialise Interactive Medical) was used for 3D designing of the mandible, gingiva, and teeth. After importing the files, evaluation of sections and their modifications, the first mask for the bony segment (HU1) was obtained with 226 to 3071 Hounsfield units (bone threshold).
To decrease the processing volume and due to insignificant effect of other parts, all designs were limited to the maxilla and mandible, and the surrounding areas were omitted. The artifacts and noises were also eliminated. After editing of the slides, the data were transferred to 3-Matic Research version 13 to improve the quality of the design. The final models were obtained after finishing and fitting of teeth with the jaw and gingiva.
The designed bone had D2 density and comprised of a cortical and a cancellous part.
Since the aim of this study was to assess the effect of loads applied to dental implant system on the implant-abutment interface and abutment screw loosening by FEA, Megagen implants were used for modeling. Since the precise geometric details of this implant system were not available, the implant, abutment screw, and abutment were scanned by a 3D scanner (PTS-S400, Shenzen, China), composed of an industrial camera and a light source.
According to the files obtained from the 3D scanner, and the information disclosed by the manufacturer, FANIHX4011C implant with 4-mm diameter and 11.5-, 10-, and 8.5-mm heights, and Post EZ abutment were modeled by 6R2017-V5 P3 CATIA software. In this design, the implant-abutment contact area which is the location of accumulation of microorganisms was beveled inward by 0.5 mm. Accordingly, the implant had 0.5-mm distance from the bone crest all-around.
Cement-retained prosthesis was also designed. A metal-ceramic coping with 0.7-mm occlusal thickness and 1.2-mm porcelain in the occlusal surface was designed for teeth #6 and #7 for placement over the implant using Materialise Mimics Research version 21 (Materialise Interactive Medical Image Control System).
After editing of each slide, the designs were refined using 3-Matic Research version 13. Considering the study variables, the crowns were designed in six forms of horizontal and vertical cantilevers.
The models were designed using Mimics, 3-Matic, Catia and ANSYS software programs. All models were transferred to ANSYS R2 2020 for meshing. The designed models averagely had 12,000,000 nodes and 12,500,000 elements (Figure 1A)
Figure 1. Meshed models (A); site of load application (B)
To ensure correct modeling, changes were made in meshing such that stress change reached < 1%. Two different cantilever lengths and three different heights for an implant with 4-mm diameter and 11.5-mm height in a mandible with D2 bone were subjected to static loading. Finally, 6 finite element models were analyzed. The apical part of bone and the buccal and lingual surfaces were fixed before loading. After designing of the models, the physical properties of materials were added to the models (Table 1). The interaction effect of 120 N and 20 N loads along the Y and Z axes on the implant and implant crown at the site of first molar, and the interaction effect of 150 N and 25 N loads along the Y and Z axes on the cantilever at the site of second molar were assessed. The preload was 875 N (Figure 1B)
Table 1. Modulus of elasticity and Poisson’s ratio for the materials used for modeling
Results
The maximum von Mises stress value was calculated during the masticatory cycle. Axial load was applied on the prosthesis and crowns with vertical and horizontal cantilevers. After modeling, data were analyzed. Warm colors indicated high-stress and cold colors indicated low-stress areas. Stress was reported in Pascals (Pa). Analysis of the images revealed that the stress in all implant components was lower than the yield strength of titanium (1020 MPa). Thus, static degradation or plastic deformation of implant system was prevented. According to the results, maximum stress distribution was recorded at the fixture neck.
Due to the application of preload, the abutment screw provides optimal mechanical connection between the implant and abutment. In the present study, in all abutment screws, irrespective of crown geometry, maximum stress was recorded in the screw body and interface of abutment screw body and screw access hole, and also abutment screw threads.
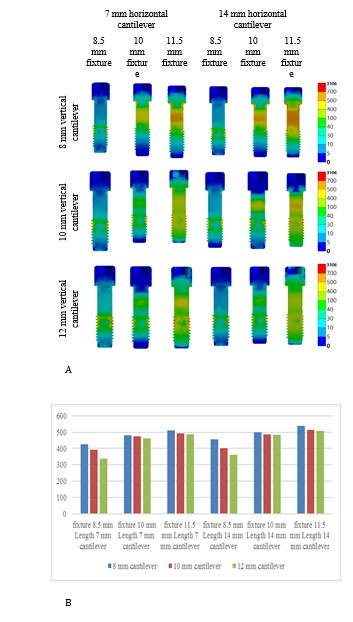
In all three implants with fixture heights of 8.5, 10, and 11.5 mm and in presence of each vertical cantilever (8, 10, 12 mm), by an increase in horizontal cantilever length, stress in abutment screw increased. In all fixture heights of 8.5, 10, and 11.5 mm and in presence of 7- and 14-mm horizontal cantilevers, stress decreased in abutment screw by an increase in vertical cantilever. In implants with 7- and 14-mm horizontal cantilever and with 8-, 10-, and 12-mm vertical cantilever, by an increase in fixture height, stress in abutment screw increased (Figures 2A and 2B).
Figure 2. Distribution of von Mises stress in the abutment screw:(A), histogram of the comparison of von Mises stress in the abutment screw (B)
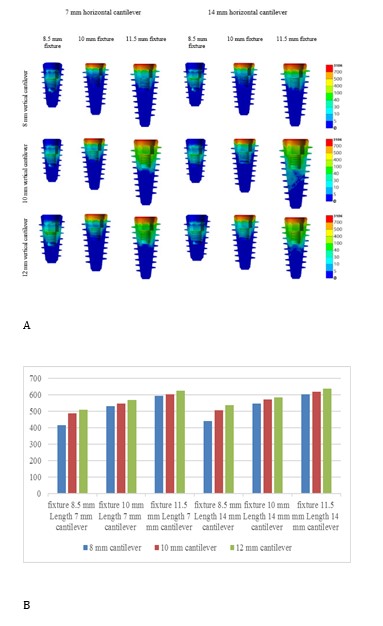
Fixture is responsible for load transfer from the implant system to bone. In order to do this, it should be completely bonded to bone. Higher stress distribution was noted in the fixture neck, and attachment of screw and fixture, creating a relatively round pattern of stress distribution in the cross-sectional view. In all three fixture heights (8.5, 10, and 11.5 mm) and all three vertical cantilevers (8,10,12 mm), by an increase in horizontal cantilever, stress in fixture increased. In all three fixture heights (8.5, 10, and 11.5 mm) and 7- and 14-mm horizontal cantilevers, by an increase in
vertical cantilever, stress in fixture increased. In implants with 7- and 14-mm horizontal cantilevers and 8-, 10-, and 12-mm vertical cantilevers, by an increase in fixture height, stress in fixture increased (Figures 3A and 3B).
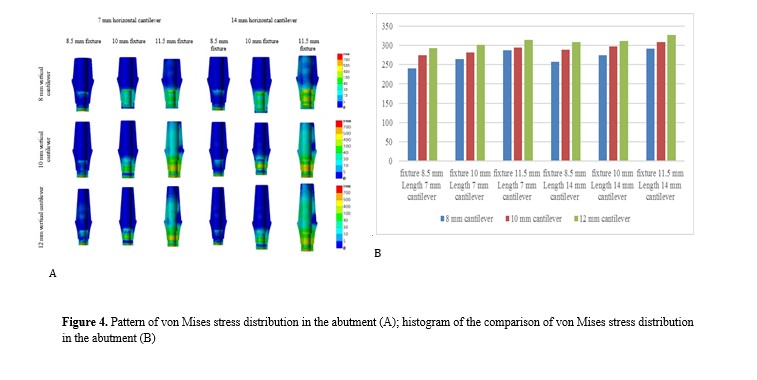
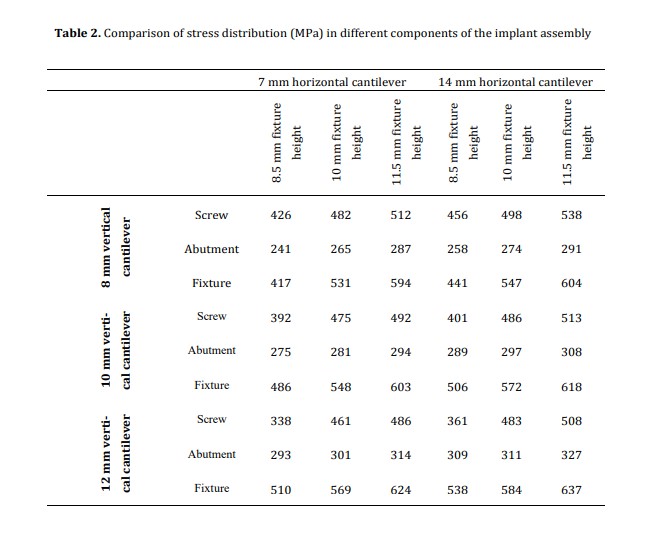
The abutment should be resistant to variable masticatory forces. In all abutments, maximum stress was observed at the abutment-fixture interface, and at the internal contact with the screw. In all three fixture heights (8.5, 10, 11.5 mm) and all three vertical cantilevers (8, 10, and 12 mm), by an increase in horizontal cantilever, stress in abutment increased. In all three fixture heights (8.5, 10, 11.5 mm) and 7- and 14-mm horizontal cantilevers, by an increase in vertical cantilever, stress in abutment increased. In implants with 7- and 14-mm horizontal cantilevers and 8-, 10-, and 12-mm vertical cantilevers, by an increase in fixture length, stress in abutment increased (Figures 4A and 4B). Table 2 compares stress distribution in different components of the implant assembly.
Figure 3. Pattern of von Mises stress distribution in the fixture (A); histogram of the comparison of von Mises stress distribution in the fixture (B)
Figure 4. Pattern of von Mises stress distribution in the abutment (A); histogram of the comparison of von Mises stress distribution in the abutment (B)
Table 2. Comparison of stress distribution (MPa) in different components of the implant assembly
Discussion
Bone loss following dental implant treatment can cause problems. Reduction in available bone does not allow placement of implants with optimal height and diameter. On the other hand, systemic diseases, old age, and financial issues may not allow conduction of complex surgical procedures for bone grafting. Thus, dental implants may be inserted with vertical and horizontal cantilevers for such cases to avoid advanced removable prosthetic or surgical treatments. Nonetheless, increased vertical and horizontal cantilevers apply greater stress to the fixture and can cause crestal bone loss and prosthetic problems such as screw fracture and loosening, causing problems for both patient and dental clinician. Thus, it is important to identify the contributing factors, the resultant complications, and strategies to prevent them.
Success of implant treatment depends not only on osseointegration but also on biomechanical aspects [19]. The geometry of implant assembly and also the magnitude of vertical and horizontal cantilever can affect the magnitude of stress applied to the implant and the supporting bone through the lever mechanism [20]. Moreover, larger crown dimensions with shorter implants may cause greater stress [21]. A shorter implant, compared with a longer implant with similar crown height has a larger crown/implant height ratio. Thus, biomechanical complications in short implants should be predicted. Nonetheless, a previous study showed that short implants are clinically successful irrespective of their crown/implant height ratio [22].
The abutment screw material can also affect the preload. The tensile and yield strength values of gold alloy screws are higher than those of conventional titanium screws. Thus, a higher preload may be achieved in gold alloy screws [23].
Therefore, in the present study, the same type of screw was used in all three implant heights with different vertical and horizontal cantilever lengths.
FEA is a cost-effective method for assessment of stress distribution in implant system components. It is a simple method for assessment of complex biomechanical systems. However, for a reliable modeling, several parameters should be taken into account including the precise mechanical properties of the implant system, implant system geometry, preloading of abutment screw, and reverse engin eering.
Effect of horizontal cantilever:
The results showed that in all three fixture heights (8.5, 10, 11.5 mm) and in presence of each vertical cantilever (8, 10, 12 mm), by an increase in horizontal cantilever, stress increased in the abutment screw (in the screw body, interface of screw body and screw hole, and abutment screw threads), abutment (at the abutment-fixture contact and at the internal contact with the screw), and fixture (around the fixture neck and at the contact of screw and fixture).
Effect of vertical cantilever:
The results showed that in all three fixture heights (8.5, 10, 11.5 mm) and in presence of 7- and 14-mm horizontal cantilevers, by an increase in vertical cantilever, the stress in abutment screw (in the screw body and contact of screw and abutment) decreased, and the stress in abutment (at the abutment-fixture contact and at the internal contact with the screw) and fixture (around the fixture neck and at the contact of screw and fixture) increased.
Effect of fixture height:
Upon load application, in implants with 7- and 14-mm horizontal cantilevers and in presence of 8, 10, and 12 mm vertical cantilevers, by an increase in fixture height, stress in the screw (in the screw body and contact area of screw body and screw hole, and in the screw threads), abutment (at the abutment-fixture contact and at the internal contact with the screw) and fixture (around the fixture neck and at the contact of screw and fixture) increased. In general, it may be concluded that minimum screw stress was recorded in implants with 8.5 mm fixture height, 7 mm horizontal cantilever, and 12 mm vertical cantilever. Also, maximum screw stress was noted in implants with 11.5 mm fixture height, 14 mm horizontal cantilever, and 8 mm vertical cantilever.
Oyar et al. [24] concluded that length of horizontal cantilever and posterior implant inclination affected the load distribution pattern. Increasing the
horizontal cantilever decreased stress in posterior implants with a distal inclination, which was not in agreement with the present results regarding the effect of horizontal cantilever on stress distribution in implant component. Variations in the results may be due to different methodologies, study designs, implant brands with different shapes, angles, and difficulty levels, different load application angles, and the role of other parameters in stress generation.
Conclusion
In the present study, maximum stress in the implant system was recorded in the fixture neck. Maximum stress in the screw was recorded in the screw body, contact of screw body and screw hole, and screw threads. By a change in vertical and horizontal cantilevers, the abutment screw undergoes fatigue, causing screw loosening and affecting the contact of screw and abutment. Upon load application, stress is accumulated in the fixture-abutment, fixture-screw, and abutment-screw interfaces. The abutment screw in single crowns has higher stress tolerance than that in crowns with two teeth.
Full-Text: (1922 Views)
| Abstract
Background and Aim: This study assessed the effect of crown dimensions on stress distribution in the abutment screw upon loading using three-dimensional (3D) finite element analysis (FEA). Materials and Methods: Eighteen finite element models were designed using Mimics, 3D-Matic, Catia, and ANSYS software programs. Implant models were designed with 8.5-, 10- and 11.5-mm fixture heights, three different vertical cantilever heights of 8, 10, and 12 mm, and two horizontal cantilever lengths of 7 and 14 mm for the mandibular first and second molars. The interaction effect of of 120 N and 20 N loads on the implant and implant crown at the site of first molar, and the interaction effect of 150 N and 25 N loads on the cantilever at the site of second molar were analyzed. Results: By an increase in horizontal cantilever length, stress in the abutment screw, abutment, and fixture increased in all models. Stress decreased in the abutment screw and increased in the abutment and fixture by an increase in vertical cantilever. Minimum screw stress was recorded in implants with 8.5 mm fixture height, 7 mm horizontal cantilever, and 12 mm vertical cantilever. Maximum screw stress was noted in implants with 11.5 mm fixture height, 14 mm horizontal cantilever, and 8 mm vertical cantilever. Conclusion: According to FEA, increasing the horizontal and vertical cantilever length may result in an increased risk of screw loosening and fatigue fracture due to increased stress values in the screw or in other components (abutment and fixture), respectively. Key Words: Dental Implants; Dental Prosthesis Design; Dental Stress Analysis; Finite Element Analysis |
Introduction
Dental implant is the best option for replacement of the lost teeth, aiming to replace the lost tissue and restore function, comfort, esthetics, speech, and tissue health. The main reason for selection of dental implant for replacement of the lost teeth is to preserve the alveolar bone [1]. Intraosseous dental implants are alloplastic materials that are surgically inserted in the residual alveolar ridge to serve as a prosthetic abutment [2,3]. Stresses above the normal level can cause complications and damage the implant components [4].
Abutment is part of the implant that maintains the prosthetic part or the suprastructure [1]. The suprastructure is a metal framework that is connected to the abutment and provides retention for removable prostheses (e.g., the cast metal bar of overdenture) and forms the metal framework of fixed partial dentures [5].
Abutment screw is the easiest, most reliable, and most efficient component for fixation of prosthetic components to the implant body. Abutment screw provides easy retention in a small scale [1,6,7].
High stress levels can cause microcracks in bone and lead to bone resorption or mechanical failure of implant or prosthetic components such as porcelain fracture, abutment screw loosening, and abutment screw fracture [8,9].
Unlike the reversible signs and symptoms shown by the natural teeth, bone resorption around dental implants or restoration loosening may occur with no alarming sign/symptom. Abutment screw loosening is a sign of presence of biomechanical stresses exceeding the tolerance threshold of the
assembly. Implant crowns rarely show clinical signs and symptoms other than fatigue and fracture. Resultantly, dental clinicians have little or no diagnostic evidence to decrease the level of stress applied to the supporting system [10].
Prosthetic screw fracture occurs in both fixed partial and complete dentures with a mean prevalence rate of 4% (range 0% to 19%). Abutment screw fracture occurs less commonly than prosthetic screw fracture due to having a larger diameter. Abutment screw loosening averagely occurs in 6% of implant prostheses [11]. The higher the level of stress applied to prosthesis, the higher the risk of abutment screw loosening would be.
Cantilevers increase the risk of screw loosening because increasing the loads applied to the implant assembly has a direct correlation with the cantilever length. The higher the crown height attached to the abutment, the higher the load applied to the screw and the risk of screw loosening (or fracture) would be [12].
Single-unit crowns show the highest rate of abutment screw loosening. Screw loosening has significant complications. A loose screw can cause crestal bone loss [13]. Abutment screw loosening in a cement-retained restoration necessitates perforation of crown to access the abutment screw. Chronic screw loosening can be costly and time-consuming. Evidence shows that 6% to 20% of maxillary prostheses show screw loosening at least once in their first year of function [14,15].
Any occlusal imbalance, poor adaptation of casting, or unequal forces can cause vibration of crown under function and lead to screw loosening or fracture (when the applied load is too high or the metal dimensions are too small) [16]. External forces that are exerted to the abutment screw significantly increase the risk of screw loosening. Such forces are referred to as detach or detorque forces if cause screw loosening. Such forces are considered as risk factors for implant fracture, crestal bone loss, and component fracture. When the screws are tightened and subjected to occlusal forces with no detaching force, they remain tightened for long. However, if the external detach forces exceed the screw tightening forces (known as the interlocking forces), screw loosening occurs [17]. Thus, external forces caused by parafunction, crown height, mastication dynamics, position in dental arch, and opposing teeth are factors that highly increase the stresses applied to the implant and screw [18]. Also, predictors of such conditions such as cantilevers, angulated forces, and poor occlusal schemes should be taken into account [16].
This study aimed to assess the effect of vertical and horizontal dimensions of the crown on stress distribution in the abutment screw upon load application by three-dimensional (3D) finite element analysis (FEA).
Materials and Methods
A computed tomography (CT) scan of a patient obtained in Namazi Hospital, Shiraz was randomly selected and used in this study. Implants with 11.5-, 10-, and 8.5-mm height and 4-mm diameter (AnyRidge, MegaGen, Daegu, Korea) and straight abutments underwent 3D scanning by a 3D scanner composed of an industrial camera and a light source, and the data regarding the mandible, fixture, crown and abutment geometry were transferred to a software.
For 3D designing of the teeth, some cases were randomly selected according to the following criteria:
-CT scan of patients between 18 to 40 years
-Absence of systemic diseases
-Absence of bone diseases
-No smoking
-No use of alcoholic beverages
CT scan of a 20-year-old female was finally selected. Materialise Mimics Research version 21 (Materialise Interactive Medical) was used for 3D designing of the mandible, gingiva, and teeth. After importing the files, evaluation of sections and their modifications, the first mask for the bony segment (HU1) was obtained with 226 to 3071 Hounsfield units (bone threshold).
To decrease the processing volume and due to insignificant effect of other parts, all designs were limited to the maxilla and mandible, and the surrounding areas were omitted. The artifacts and noises were also eliminated. After editing of the slides, the data were transferred to 3-Matic Research version 13 to improve the quality of the design. The final models were obtained after finishing and fitting of teeth with the jaw and gingiva.
The designed bone had D2 density and comprised of a cortical and a cancellous part.
Since the aim of this study was to assess the effect of loads applied to dental implant system on the implant-abutment interface and abutment screw loosening by FEA, Megagen implants were used for modeling. Since the precise geometric details of this implant system were not available, the implant, abutment screw, and abutment were scanned by a 3D scanner (PTS-S400, Shenzen, China), composed of an industrial camera and a light source.
According to the files obtained from the 3D scanner, and the information disclosed by the manufacturer, FANIHX4011C implant with 4-mm diameter and 11.5-, 10-, and 8.5-mm heights, and Post EZ abutment were modeled by 6R2017-V5 P3 CATIA software. In this design, the implant-abutment contact area which is the location of accumulation of microorganisms was beveled inward by 0.5 mm. Accordingly, the implant had 0.5-mm distance from the bone crest all-around.
Cement-retained prosthesis was also designed. A metal-ceramic coping with 0.7-mm occlusal thickness and 1.2-mm porcelain in the occlusal surface was designed for teeth #6 and #7 for placement over the implant using Materialise Mimics Research version 21 (Materialise Interactive Medical Image Control System).
After editing of each slide, the designs were refined using 3-Matic Research version 13. Considering the study variables, the crowns were designed in six forms of horizontal and vertical cantilevers.
The models were designed using Mimics, 3-Matic, Catia and ANSYS software programs. All models were transferred to ANSYS R2 2020 for meshing. The designed models averagely had 12,000,000 nodes and 12,500,000 elements (Figure 1A)
Figure 1. Meshed models (A); site of load application (B)
{kind=link}
To ensure correct modeling, changes were made in meshing such that stress change reached < 1%. Two different cantilever lengths and three different heights for an implant with 4-mm diameter and 11.5-mm height in a mandible with D2 bone were subjected to static loading. Finally, 6 finite element models were analyzed. The apical part of bone and the buccal and lingual surfaces were fixed before loading. After designing of the models, the physical properties of materials were added to the models (Table 1). The interaction effect of 120 N and 20 N loads along the Y and Z axes on the implant and implant crown at the site of first molar, and the interaction effect of 150 N and 25 N loads along the Y and Z axes on the cantilever at the site of second molar were assessed. The preload was 875 N (Figure 1B)
Table 1. Modulus of elasticity and Poisson’s ratio for the materials used for modeling
{kind=link}
Results
The maximum von Mises stress value was calculated during the masticatory cycle. Axial load was applied on the prosthesis and crowns with vertical and horizontal cantilevers. After modeling, data were analyzed. Warm colors indicated high-stress and cold colors indicated low-stress areas. Stress was reported in Pascals (Pa). Analysis of the images revealed that the stress in all implant components was lower than the yield strength of titanium (1020 MPa). Thus, static degradation or plastic deformation of implant system was prevented. According to the results, maximum stress distribution was recorded at the fixture neck.
Due to the application of preload, the abutment screw provides optimal mechanical connection between the implant and abutment. In the present study, in all abutment screws, irrespective of crown geometry, maximum stress was recorded in the screw body and interface of abutment screw body and screw access hole, and also abutment screw threads.
In all three implants with fixture heights of 8.5, 10, and 11.5 mm and in presence of each vertical cantilever (8, 10, 12 mm), by an increase in horizontal cantilever length, stress in abutment screw increased. In all fixture heights of 8.5, 10, and 11.5 mm and in presence of 7- and 14-mm horizontal cantilevers, stress decreased in abutment screw by an increase in vertical cantilever. In implants with 7- and 14-mm horizontal cantilever and with 8-, 10-, and 12-mm vertical cantilever, by an increase in fixture height, stress in abutment screw increased (Figures 2A and 2B).
Figure 2. Distribution of von Mises stress in the abutment screw:(A), histogram of the comparison of von Mises stress in the abutment screw (B)
{kind=link}
Fixture is responsible for load transfer from the implant system to bone. In order to do this, it should be completely bonded to bone. Higher stress distribution was noted in the fixture neck, and attachment of screw and fixture, creating a relatively round pattern of stress distribution in the cross-sectional view. In all three fixture heights (8.5, 10, and 11.5 mm) and all three vertical cantilevers (8,10,12 mm), by an increase in horizontal cantilever, stress in fixture increased. In all three fixture heights (8.5, 10, and 11.5 mm) and 7- and 14-mm horizontal cantilevers, by an increase in
vertical cantilever, stress in fixture increased. In implants with 7- and 14-mm horizontal cantilevers and 8-, 10-, and 12-mm vertical cantilevers, by an increase in fixture height, stress in fixture increased (Figures 3A and 3B).
The abutment should be resistant to variable masticatory forces. In all abutments, maximum stress was observed at the abutment-fixture interface, and at the internal contact with the screw. In all three fixture heights (8.5, 10, 11.5 mm) and all three vertical cantilevers (8, 10, and 12 mm), by an increase in horizontal cantilever, stress in abutment increased. In all three fixture heights (8.5, 10, 11.5 mm) and 7- and 14-mm horizontal cantilevers, by an increase in vertical cantilever, stress in abutment increased. In implants with 7- and 14-mm horizontal cantilevers and 8-, 10-, and 12-mm vertical cantilevers, by an increase in fixture length, stress in abutment increased (Figures 4A and 4B). Table 2 compares stress distribution in different components of the implant assembly.
Figure 3. Pattern of von Mises stress distribution in the fixture (A); histogram of the comparison of von Mises stress distribution in the fixture (B)
{kind=link}
Figure 4. Pattern of von Mises stress distribution in the abutment (A); histogram of the comparison of von Mises stress distribution in the abutment (B)
{kind=link}
Table 2. Comparison of stress distribution (MPa) in different components of the implant assembly
{kind=link}
Discussion
Bone loss following dental implant treatment can cause problems. Reduction in available bone does not allow placement of implants with optimal height and diameter. On the other hand, systemic diseases, old age, and financial issues may not allow conduction of complex surgical procedures for bone grafting. Thus, dental implants may be inserted with vertical and horizontal cantilevers for such cases to avoid advanced removable prosthetic or surgical treatments. Nonetheless, increased vertical and horizontal cantilevers apply greater stress to the fixture and can cause crestal bone loss and prosthetic problems such as screw fracture and loosening, causing problems for both patient and dental clinician. Thus, it is important to identify the contributing factors, the resultant complications, and strategies to prevent them.
Success of implant treatment depends not only on osseointegration but also on biomechanical aspects [19]. The geometry of implant assembly and also the magnitude of vertical and horizontal cantilever can affect the magnitude of stress applied to the implant and the supporting bone through the lever mechanism [20]. Moreover, larger crown dimensions with shorter implants may cause greater stress [21]. A shorter implant, compared with a longer implant with similar crown height has a larger crown/implant height ratio. Thus, biomechanical complications in short implants should be predicted. Nonetheless, a previous study showed that short implants are clinically successful irrespective of their crown/implant height ratio [22].
The abutment screw material can also affect the preload. The tensile and yield strength values of gold alloy screws are higher than those of conventional titanium screws. Thus, a higher preload may be achieved in gold alloy screws [23].
Therefore, in the present study, the same type of screw was used in all three implant heights with different vertical and horizontal cantilever lengths.
FEA is a cost-effective method for assessment of stress distribution in implant system components. It is a simple method for assessment of complex biomechanical systems. However, for a reliable modeling, several parameters should be taken into account including the precise mechanical properties of the implant system, implant system geometry, preloading of abutment screw, and reverse engin eering.
Effect of horizontal cantilever:
The results showed that in all three fixture heights (8.5, 10, 11.5 mm) and in presence of each vertical cantilever (8, 10, 12 mm), by an increase in horizontal cantilever, stress increased in the abutment screw (in the screw body, interface of screw body and screw hole, and abutment screw threads), abutment (at the abutment-fixture contact and at the internal contact with the screw), and fixture (around the fixture neck and at the contact of screw and fixture).
Effect of vertical cantilever:
The results showed that in all three fixture heights (8.5, 10, 11.5 mm) and in presence of 7- and 14-mm horizontal cantilevers, by an increase in vertical cantilever, the stress in abutment screw (in the screw body and contact of screw and abutment) decreased, and the stress in abutment (at the abutment-fixture contact and at the internal contact with the screw) and fixture (around the fixture neck and at the contact of screw and fixture) increased.
Effect of fixture height:
Upon load application, in implants with 7- and 14-mm horizontal cantilevers and in presence of 8, 10, and 12 mm vertical cantilevers, by an increase in fixture height, stress in the screw (in the screw body and contact area of screw body and screw hole, and in the screw threads), abutment (at the abutment-fixture contact and at the internal contact with the screw) and fixture (around the fixture neck and at the contact of screw and fixture) increased. In general, it may be concluded that minimum screw stress was recorded in implants with 8.5 mm fixture height, 7 mm horizontal cantilever, and 12 mm vertical cantilever. Also, maximum screw stress was noted in implants with 11.5 mm fixture height, 14 mm horizontal cantilever, and 8 mm vertical cantilever.
Oyar et al. [24] concluded that length of horizontal cantilever and posterior implant inclination affected the load distribution pattern. Increasing the
horizontal cantilever decreased stress in posterior implants with a distal inclination, which was not in agreement with the present results regarding the effect of horizontal cantilever on stress distribution in implant component. Variations in the results may be due to different methodologies, study designs, implant brands with different shapes, angles, and difficulty levels, different load application angles, and the role of other parameters in stress generation.
Conclusion
In the present study, maximum stress in the implant system was recorded in the fixture neck. Maximum stress in the screw was recorded in the screw body, contact of screw body and screw hole, and screw threads. By a change in vertical and horizontal cantilevers, the abutment screw undergoes fatigue, causing screw loosening and affecting the contact of screw and abutment. Upon load application, stress is accumulated in the fixture-abutment, fixture-screw, and abutment-screw interfaces. The abutment screw in single crowns has higher stress tolerance than that in crowns with two teeth.
Type of Study: Original article |
Subject:
Prosthodontics
References
1. Resnik RR, Misch CE. Diagnostic Casts, Surgical Templates, and Provisionalization. In: Misch CE, editor. Dental Implant Pros-thetics (Second Edition). St. Louis: Mosby; 2015. 1264p. [DOI:10.1016/B978-0-323-07845-0.00018-X]
2. Misch CE. ARABIC-Contemporary Implant Dentistry. 3rd ed. Elsevier Health Sciences; 2007. 1120 p.
3. Oral implantology. Glossary of implant terms. J Oral Implantol. 2007;Suppl 1:2-14.
4. Meffert RM, Langer B, Fritz ME. Dental implants: a review. J Periodontol. 1992 Nov;63(11):859-70. [DOI:10.1902/jop.1992.63.11.859] [PMID]
5. Mazurat RD, Love WB. Direct assembly of implant suprastructures. J Prosthet Dent. 1993 Aug;70(2):172-5. [DOI:10.1016/0022-3913(93)90014-F] [PMID]
6. Lee KY, Shin KS, Jung JH, Cho HW, Kwon KH, Kim YL. Clinical study on screw loosening in dental implant prostheses: a 6-year retrospective study. J Korean Assoc Oral Maxillofac Surg. 2020 Apr 30;46(2):133-42. [DOI:10.5125/jkaoms.2020.46.2.133] [PMID] [PMCID]
7. Lee JH, Cha HS. Screw loosening and changes in removal torque relative to abutment screw length in a dental implant with external abutment connection after oblique cyclic loading. J Adv Prosthodont. 2018 Dec;10(6):415-21. [DOI:10.4047/jap.2018.10.6.415] [PMID] [PMCID]
8. Agustín-Panadero R, Orozco-Varo A, Domínguez-Cardoso P, Bernabeu-Mira JC, Soto-Peñaloza D, Peñarrocha-Oltra D. Biome-chanics and Occlusion in Immediate Loading. In: Peñarrocha-Diago M, Covani U, Cuadrado L, eds. Atlas of Imme-diate Dental Implant Loading. Cham: Springer International Publishing; 2019. p. 49-67. [DOI:10.1097/01.BMSAS.0000558124.96675.8f]
9. Liu M, Li C, Liu L, Ye Y, Dastan D, Garmestani H. Inhibition of stress corrosion cracking in 304 stainless steel through titani-um ion implantation. Materials Science and Technology. 2020;36(3):284-92. [DOI:10.1080/02670836.2019.1704527]
10. De Marco G, Di Francesco F, Lanza A. Analysis and management of implant-prosthetic complications: Description of a diagnostic and therapeutic algorithm with a clinical case. J Prosthodont Res. 2018;62(3):386-90. [DOI:10.1016/j.jpor.2017.08.001] [PMID]
11. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003 Aug;90(2):121-32. [DOI:10.1016/S0022-3913(03)00212-9] [PMID]
12. Nissan J, Ghelfan O, Gross O, Priel I, Gross M, Chaushu G. The effect of crown/implant ratio and crown height space on stress distribution in unsplinted implant supporting restorations. J Oral Maxillofac Surg. 2011 Jul;69(7):1934-9. [DOI:10.1016/j.joms.2011.01.036] [PMID]
13. Kourtis S, Damanaki M, Kaitatzidou S, Kaitatzidou A, Rous-sou V. Loosening of the fixing screw in single implant crowns: predisposing factors, prevention and treatment options. J Esthet Restor Dent. 2017 Jul 8;29(4):233-46. [DOI:10.1111/jerd.12303] [PMID]
14. Kallus T, Bessing C. Loose gold screws frequently occur in full-arch fixed prostheses supported by osseointegrated im-plants after 5 years. Int J Oral Maxillofac Implants. 1994 Mar-Apr;9(2):169-78.
15. Goodacre CJ, Kan JY, Rungcharassaeng K. Clinical complications of osseointegrated implants. J Prosthet Dent. 1999 May;81(5):537-52. [DOI:10.1016/S0022-3913(99)70208-8] [PMID]
16. Huang Y, Wang J. Mechanism of and factors associated with the loosening of the implant abutment screw: A review. J Esthet Restor Dent. 2019 Jul;31(4):338-45. [DOI:10.1111/jerd.12494] [PMID]
17. Alnasser AH, Wadhwani CPK, Schoenbaum TR, Kattadiyil MT. Evaluation of implant abutment screw tightening protocols on reverse tightening values: An in vitro study. J Prosthet Dent. 2021 Mar;125(3):486-90. [DOI:10.1016/j.prosdent.2020.02.035] [PMID]
18. Kirov D, Stoichkov B. Factors affecting the abutment screw loosening. J of IMAB. 2017 Jan-Mar;23(1):1505-9. [DOI:10.5272/jimab.2017231.1505]
19. Moraes SLDd, Verri FR, Junior JFS, Almeida DAdF, Mello CCd, Pellizzer EP. A 3-D finite element study of the influence of crown-implant ratio on stress distribution. Braz Dent J. 2013 Nov-Dec;24(6):635-41. [DOI:10.1590/0103-6440201302287] [PMID]
20. Moraes SL, Pellizzer EP, Verri FR, Santiago JF Jr, Silva JV. Three-dimensional finite element analysis of stress distribution in retention screws of different crown-implant ratios. Comput Methods Biomech Biomed Engin. 2015;18 (7):689-96. [DOI:10.1080/10255842.2013.820719] [PMID]
21. Himmlová L, Dostálová T, Kácovský A, Konvicková S. Influ-ence of implant length and diameter on stress distribution: a finite element analysis. J Prosthet Dent. 2004 Jan;91(1):20-5. [DOI:10.1016/j.prosdent.2003.08.008] [PMID]
22. Tawil G, Aboujaoude N, Younan R. Influence of prosthetic parameters on the survival and complication rates of short implants. Int J Oral Maxillofac Implants. 2006 Mar-Apr;21 (2):275-82.
23. Khraisat A, Hashimoto A, Nomura S, Miyakawa O. Effect of lateral cyclic loading on abutment screw loosening of an exter-nal hexagon implant system. J Prosthet Dent. 2004 Apr;91(4):326-34. [DOI:10.1016/j.prosdent.2004.01.001] [PMID]
24. Oyar P, Durkan R, Deste G. The effect of the design of a man-dibular implant-supported zirconia prosthesis on stress distri-bution. J Prosthet Dent. 2021 Mar;125(3):502.e1-502.e11. [DOI:10.1016/j.prosdent.2020.05.027] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |