Journal of Research in Dental
and Maxillofacial Sciences
Volume 7, Issue 3 (7-2022)
J Res Dent Maxillofac Sci 2022, 7(3): 148-154 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Veljanovski D, Stefanovikj B, Bogdanovski M, Stojkova M, Krstevski D. Effect of a Bone Replacement Material on Vertical Bone Level Alterations around Immediately Placed Mandibular Molar Implants. J Res Dent Maxillofac Sci 2022; 7 (3) :148-154
URL: http://jrdms.dentaliau.ac.ir/article-1-379-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-379-en.html



1- Clinic for Oral Surgery “Hami Optimum”, Skopje, N. Macedonia , darkoveljanovski@gmail.com
2- Dental practice “Optimum Dental”, Skopje, N. Macedonia
3- Dental practice “Molar”, Skopje, N. Macedonia
4- Dental practice “Lukanovski”, Skopje, N. Macedonia
5- Dental practice “Stela”, Skopje, N. Macedonia
2- Dental practice “Optimum Dental”, Skopje, N. Macedonia
3- Dental practice “Molar”, Skopje, N. Macedonia
4- Dental practice “Lukanovski”, Skopje, N. Macedonia
5- Dental practice “Stela”, Skopje, N. Macedonia
Full-Text [PDF 806 kb]
(1093 Downloads)
| Abstract (HTML) (2813 Views)
Full-Text: (1015 Views)
|
Abstract
Background and Aim: Immediate implant placement is a predictable therapeutic option to replace the missing teeth. However, it is technique-sensitive, and requires strict case selection criteria. Tooth extraction triggers the biologic phenomenon of bone resorption, which is not prevented with immediate implant placement. This study aimed to evaluate the influence of deproteinized bovine bone mineral (DBBM) use on vertical bone loss around immediately placed mandibular molar implants. Materials and Methods: In this non-randomized clinical study, 14 patients with immediate molar implants in the lower jaw, restored with screw-retained single crowns were evaluated. The case group (with bone material use) received DBBM in conjunction with implant placement, while no grafting was performed in the control group. The vertical bone level changes were radiographically measured at the mesial and distal implant sides as the distance between the implant shoulder and first implant-bone contact in apical direction. Measurements were made at two time points of six months postoperatively and one year post-functional loading. The acquired data were statistically analyzed using two-way ANOVA. Results: The mean values for vertical bone loss at the mesial and distal reference points were greater in the control group (without bone replacement material use) than in the case group both six months postoperatively and one-year post-functional loading. The difference was statistically significant at both time points (P<0.05). Conclusion: Within the limitation of this study, it can be concluded that the use of DBBM in immediate implants can reduce vertical bone loss. Key Words: Bone Substitutes; Therapeutic Use; Dental Implantation; Bone Resorption Introduction Immediate implant placement is a clinically proven and predictable therapeutic modality for tooth replacement. However, it is at the same time a technique-sensitive method that demands strict case selection criteria such as minimally invasive implant placement at sites with preserved bony walls, absence of acute inflammation, absence of periodontal disease and gingival recession, presence of attached gingiva with sufficient width and vertical thickness, implant placement in correct prosthetic position, and filling the gap between the implant and the inner alveolar bony walls with a bone replacement material [1-5]. Different materials have been proposed for this purpose such as deproteinized bovine bone mineral (DBBM), allografts and alloplastic materials that may also be used in mixtures with blood derivatives [6,7]. Tooth extraction results in inevitable changes of the hard tissue volume. The mean horizontal bone loss is 49% (3.8 mm) in the first 12 months, post tooth extraction [8,9]. The mean vertical bone loss is 1.2 mm at the same time point post tooth extraction [10]. Immediate implant placement does not prevent such biological phenomena, as proven by certain studies [11,12]. The distance between the immediate implants and the alveolar walls was measured in a clinical study, which concluded that bone resorption does occur, but there is also a complete marginal bone fill of the defect when immediate implants are placed without the use of a bone replacement material [13]. On the other hand, the use of bone replacement materials can reduce horizontal bone resorption in immediate implants, as shown is certain relevant clinical studies [14,15]. However, not many studies have assessed the effect of bone replacement materials on vertical bone resorption. Vertical bone resorption is a clinical phenomenon that is important in terms of esthetics and longevity of implant restorations. The aim of this study was to evaluate vertical bone level alterations around immediately placed mandibular molar implants with and without the use of a DBBM. The vertical bone level changes were radiographically measured and compared at different time points in order to reveal the influence of DBBM on vertical bone loss. Materials and Methods This was a non-randomized clinical study approved by the Ethics Committee Board for Medical and Dental Research at the Faculty of Dentistry, “Ss. Cyril and Methodius University”, Skopje, North Macedonia (reference number D23-1/2021). All patients signed informed consent forms for participation in the study. A total of 14 patients received single immediate molar implants in the lower jaw. The control group with seven patients received immediate implants without a bone replacement material. The case group with seven patients who were eligible for both treatments received immediate implant placement, as well as DBBM as a gap filler, based on the surgeon's decision. All patients received MIS Seven implants (Denstply Sirona, Charlotte, NC, USA), which are grade five titanium implants that have tapered macrogeometrical form, implant neck microrings, and no polished neck collar. All implants were placed by the same surgeon (D.V) immediately after minimally invasive tooth extraction with root separation and without raising a surgical flap. Care was taken to preserve the buccal bony plate as well the interradicular septum. All implants were placed in the middle of the preserved alveolar septum in a single stage manner (with simultaneous use of gingival formers). No provisional restorations were fabricated. The implants included in the study had a high primary stability, which was verified by resonance frequency analysis (RFA). A RFA instrument (Penguin, Gothenburg, Sweden) was used to send magnetic pulses to the peg attached to the implant and cause its vibrations; its resonance frequency was then read and translated into implant stability quotient (ISQ). The ISQ is a value on a scale that indicates the level of stability of dental implants. ISQ may range from 1 to 100, with higher values indicating greater stability. Theaccepted stability range lies between 55 and 85 ISQ. All implants in the study had primary stability (ISQ) of 70 and above. The space between the implants and the inner alveolar walls was filled with Bio-Oss (Geistlich Pharma, Wolhusen, Switzerland) bone replacement material with small size particles (0.25–1 mm). The sockets were sealed using absorbable gelatin sponges (Roeko Gelatamp, Coltene, Altstatten, Switzerland) that were stabilized to the wound margins by means of cross mattress sutures utilizing absorbable 5-0 PGA suture thread (Assut Medical, Pully-Lausanne, Switzerland). The sutures were removed 2 weeks postoperatively. The patients had to meet strict inclusion criteria which were a minimum of 18 years of age, no medical contraindications for implantation, periodontal health (full mouth plaque score < 15%, full mouth bleeding score < 15%), extracted mandibular molars for endodontic failure or root fracture, but not for periodontal issues, intact alveolar bony walls, adequate apical bone for implant stability, sockets type A and B (as per Smith and Tarnow’s classification [16]) absence of acute infection, minimal vertical soft tissue thickness of 3 mm, minimal width of attached gingiva to be 2 mm, implants placed 3-4 mm below the free gingival margin, minimal ISQ value of 70, and implants restored with screw-retained single crowns. At the prosthetic phase of the workflow, analogue implant-level impressions were made with silicone impression material (Variotime, Heraeus Kulzer, Hanau, Germany) which were subsequently digitized utilizing an in-lab scanner (Figure 1). Radiographic images were acquired using Pax-i 2D panoramic X-ray unit and EZDent-i software (Vatech, Hwaseong, South Korea). All images were obtained in a mode that allowed to reconstruct an image with allowed to reconstruct an image with autofocus to prevent errors caused by inappropriate patient positioning. Care was taken to correctly position each patient. The patients were guided to stand at the center of the equipment, the vertical frame was set such that the patients’ chin reached the chin rest, their hands holding the equipment handles tightly, chest pressed against the equipment, and both feet kept close to the inside of the base. The patients were instructed to straighten the cervical spine and stand still with balanced shoulders. They were directed to bite the groove of the bite block, close the mouth, touch the roof of the mouth with the tongue, and close the eyes. The laser beams marking the mid-sagittal plane, Frankfurt plane, and canine laser beam were set, the temple supports were tightened, and the patients were instructed to maintain their position until image acquisition was completed. The exposure settings included normal X-ray intensity with 74 kVp voltage and 12.0 mA amperage for males and 68 kVp voltage and 10.0 mA amperage for female patients. The primary outcome measure of the study was the amount of vertical bone level reduction. It was evaluated by digital measurement of the distance between certain reference points on the acquired panoramic radiographic images done six months postoperatively and one year post prosthetic restoration of the implants. The first reference point was the edge of the horizontal implant platform (implant shoulder). The second reference point was the first contact between the implant and bone in apical direction. Each implant had two mesial and two distal reference points. This distance was measured at both the mesial and the distal implant sides using the digital ruler of the software and the values were expressed in millimeters with one decimal place. The secondary outcome measures were bleeding on probing, periodontal probing depth, and plaque index, which were clinically measured. Figure 1. Clinical workflow images Results All implants were successfully integrated six months postoperatively. This was verified clinically (absence of mobility, inflammation, pain, discomfort), radiographically (absence of peri-implant radiolucency on the acquired digital panoramic images) and utilizing the Penguin RFA instrument (Penguin RFA, Gothenburg, Sweden) which showed acceptable secondary stability (ISQ values of 65 and above for all implants included in the study). The soft tissue healing was uneventful, without any sign of inflammation. The periodontal pocket depth showed no values above 7 mm and bleeding on probing was positive at only few implant sites. At the end of the prosthetic phase, screw-retained metal-ceramic single crowns were fabricated. All crowns were torqued to the implant fixtures with the recommended torque of 30 N/cm. Apart from the immediate postoperative imaging, the panoramic images were |
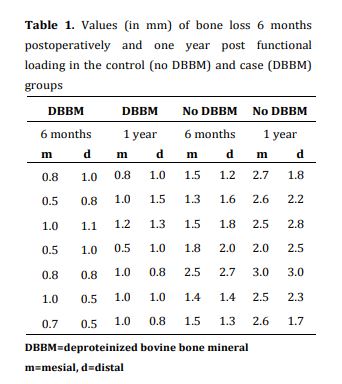
| Figure 2. Control group: no bone replacement material was used. Radiographic evaluation of the bone level at the time of implant placement, six months postoperatively and one year post functional loading acquired six months postoperatively and one year post functional loading. The distance between the previously described reference points on the images was calculated using the software of the digital panoramic system and expressed as vertical bone loss (Figures 2 and 3). The acquired data were statistically analyzed using two-way ANOVA. The results revealed that the mean and the median values of bone loss were greater in the control group (without bone replacement material) than in the case group (with bone replacement material used) six months postoperatively and one year post prosthetic restoration of implants (Table 1). The difference was statistically significant at both time points (P<0.05) |
| Figure 3. Case group: deproteinized bovine bone mineral was used. Radiographic evaluation of the bone level at the time of implant placement, six months postoperatively, and one year post functional loading Table 1. Values (in mm) of bone loss 6 months postoperatively and one year post functional loading in the control (no DBBM) and case (DBBM) groups Discussion Stable peri-implant crestal bone level is the most desired outcome in contemporary implant therapy. The most commonly reported implant bone stability criteria were defined as less than 1.5 mm of bone loss in the first year and 0.2 mm annual bone loss after the first year of loading, absence of bleeding on probing, pain, and radiolucency, and periodontal probing depth not greater than 5-7 mm. However, recent trends in implant dentistry have shifted towards absence of bone loss when defining peri-implant bone stability [17]. The success of immediate implants depends on many factors such as correct prosthetic position, adequate vertical gingival thickness, adequate width of attached gingiva, implant design, correct design of provisional and definitive restorations (screw-retained or cemented) and correct use of bone replacement materials as gap fillers [18]. The clinician should anticipate the horizontal and vertical bone resorption that occurs when placing immediate implants, which is why the implant fixtures need to be placed 3-4 mm below the free gingival margin and away from the buccal bony wall. The connection of the healing abutment (gingival former) or the temporary restoration to the implant marks the beginning of the biologic width formation. The biologic width has a protective function. It distances the implant-abutment interface from the oral microflora. In dental implants, biologic width is defined as the distance between the most apical part of the junctional epithelium and the first contact between the implant and the surrounding bone. The biologic width formation is clinically presented as bone remodeling that stops at the implant neck (the prosthetic platform). This bone remodeling is also referred to as controlled bone loss. However, if the bone remodeling continues beyond the implant neck in the apical direction, it is referred to as progressive bone loss, or simply bone loss. This is an unwanted outcome of implant therapy because it may jeopardize the future of implant restorations. Therefore, every effort should be made to minimize peri-implant bone loss. With this in mind, many authors have proposed different approaches to implant placement. The use of bone replacement materials with slow resorption rate, such as DBBM together with immediate implant placement is a well-documented method that minimizes post-extraction changes of bone volume [19]. The bovine bone mineral used in this study (Bio-Oss, Geistlich Pharma, Wolhusen, Swiss) is an osteoconductive material widely used in different procedures such as guided bone regeneration, sinus floor elevation, ridge preservation, and immediate implant placement. When used in immediate implant placement procedures, the small size particles allow for better vascularization while the slow resorption rate of the graft decreases the reduction of bone volume to a certain extent. The resorption that occurs in the vertical (apicocoronal) direction affects the long-term implant stability and may cause esthetic issues. Therefore, it is of paramount importance to decrease or prevent it, if possible. Conclusion The use of DBBM can compensate for the vertical bone level loss to a great extent and has a significant clinical implication. However, further controlled clinical studies are needed in order to draw more accurate conclusions. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Type of Study: Original article |
Subject:
Periodontology
References
1. Canullo L, Iurlaro G, Iannello G. Double-blind randomized controlled trial study on post-extraction immediately restored implants using the switching platform concept: soft tissue response. Preliminary report. Clin Oral Implants Res. 2009 Apr;20(4):414-20. [DOI:10.1111/j.1600-0501.2008.01660.x] [PMID]
2. Pieri F, Aldini NN, Marchetti C, Corinaldesi G. Influence of implant-abutment interface design on bone and soft tissue levels around immediately placed and restored single-tooth implants: a randomized controlled clinical trial. Int J Oral Maxillofac Implants. 2011 Jan-Feb;26(1): 169-78.
3. Shanelec DA, Tibbetts LS. Implant microsurgery: Immediate implant placement with implant-supported provisional. Clin. adv. periodontics. 2011 Mar;1(3):161-72. [DOI:10.1902/cap.2011.110040]
4. Degidi M, Nardi D, Daprile G, Piattelli A. Buccal bone plate in the immediately placed and restored maxillary single implant: a 7-year retrospective study using computed tomography. Implant Dent. 2012 Feb;21(1):62-6. [DOI:10.1097/ID.0b013e31823fce9f] [PMID]
5. Kinaia BM, Shah M, Neely AL, Goodis HE. Crestal bone level changes around immediately placed implants: a systematic review and meta-analyses with at least 12 months' follow-up after functional loading. J Periodontol. 2014 Nov;85(11): 1537-48. [DOI:10.1902/jop.2014.130722] [PMID]
6. Kan JY, Rungcharassaeng K, Sclar A, Lozada JL. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg. 2007 Jul; 65(7 Suppl 1):13-9. [DOI:10.1016/j.joms.2007.04.006] [PMID]
7. Saito H, Chu SJ, Reynolds MA, Tarnow DP. Provisional Restorations Used in Immediate Implant Placement Provide a Platform to Promote Peri-implant Soft Tissue Healing: A Pilot Study. Int J Periodontics Restorative Dent. 2016 Jan-Feb;36(1):47-52. [DOI:10.11607/prd.1945] [PMID]
8. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003 Aug;23(4):313-23.
9. Hämmerle CH, Araújo MG, Simion M; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:80-2. [DOI:10.1111/j.1600-0501.2011.02370.x] [PMID]
10. Weng D, Stock V, Schliephake H. Are socket and ridge preservation techniques at the day of tooth extraction efficient in maintaining the tissues of the alveolar ridge? Systematic review, consensus statements and recommendations of the 1st DGI Consensus Conference in September 2010, Eur. J. Oral Implantol. 2011 Feb;4(1): 459-66.
11. Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005 Feb;32(2):212-8. [DOI:10.1111/j.1600-051X.2005.00642.x] [PMID]
12. Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin Oral Implants Res. 2010 Jan;21(1):22-9. [DOI:10.1111/j.1600-0501.2009.01825.x] [PMID]
13. Botticelli D, Berglundh T, Lindhe J. Resolution of bone defects of varying dimension and configuration in the marginal portion of the peri-implant bone. An experimental study in the dog. J Clin Periodontol. 2004 Apr;31(4):309-17. [DOI:10.1111/j.1600-051X.2004.00502.x] [PMID]
14. Maiorana C, Beretta M, Salina S, Santoro F. Reduction of autogenous bone graft resorption by means of bio-oss coverage: a prospective study. Int J Periodontics Restorative Dent. 2005 Feb;25(1):19-25.
15. Araújo M, Linder E, Lindhe J. Effect of a xenograft on early bone formation in extraction sockets: an experimental study in dog. Clin Oral Implants Res. 2009 Jan;20(1):1-6. [DOI:10.1111/j.1600-0501.2008.01606.x] [PMID]
16. Smith RB, Tarnow DP. Classification of molar extraction sites for immediate dental implant placement: technical note. Int J Oral Maxillofac Implants. 2013 May-Jun;28(3): 911-6. [DOI:10.11607/jomi.2627] [PMID]
17. Linkevicius T. Zero Bone Loss Concepts. Illustrated ed. Batavia, IL: Quintessence Pub Co; 2019. 304 p.
18. De Angelis P, Manicone PF, Gasparini G, De Angelis S, Liguori MG, De Filippis I, et al. Influence of Immediate Implant Placement and Provisionalization with or without Soft Tissue Augmentation on Hard and Soft Tissues in the Esthetic Zone: A One-Year Retrospective Study. Biomed Res Int. 2021 Jan 5;2021:8822804. [DOI:10.1155/2021/8822804] [PMID] [PMCID]
19. Girlanda FF, Feng HS, Corrêa MG, Casati MZ, Pimentel SP, Ribeiro FV, Cirano FR. Deproteinized bovine bone derived with collagen improves soft and bone tissue outcomes in flapless immediate implant approach and immediate provisionalization: a randomized clinical trial. Clin Oral Investig. 2019 Oct;23(10):3885-93. [DOI:10.1007/s00784-019-02819-x] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |