

Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 154-161 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sharif H, Aghayan S. New Approaches for Gummy Smile Treatment:
A Review. J Res Dent Maxillofac Sci 2023; 8 (2) :154-161
URL: http://jrdms.dentaliau.ac.ir/article-1-368-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-368-en.html



1- Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Department of Periodontology, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,Shabnamaghayan@yahoo.com
2- Department of Periodontology, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 668 kb]
(1840 Downloads)
| Abstract (HTML) (2541 Views)
Introduction
Several parameters are involved in creation of a beautiful smile [1]. Excessive gingival display could be secondary to modified passive eruption, inadequate upper lip muscle, small upper lip, short crowns, high mobility of the upper lip, anterior dentoalveolar extrusion, bimaxillary protrusion, and vertical maxillary excess (VME) [1-3].
Factors that affect the smile include type of face, symmetry and vertical height of face, smile line, thickness, size and shape of the lips, alveolar bone thickness, type of gingiva, and height and form of the teeth that should be considered in treatment of gummy smile (GS) [3]. Mazzuco and Hexsel represented a classification based on the amount of excessive gingival exposure [4]. In a normal smile, less than 3 mm of gingiva can be seen in the anterior region [5]. Patients with anterior GS have more than 3 mm of their gingiva between their canine teeth exposed during smiling. In this situation, the levator labii superioris alaeque nasi (LLSAN) muscle is involved. Zygomatic muscles are involved in posterior GS, which is characterized by exposure of more than 3 mm of the gingiva posterior to canine teeth [4-7]. In asymmetrical GS, one of these muscles (LLSAN or zygomatic muscles) is involved and excessive gingiva is shown in one site; whereas, in mixed GS, both LLSAN and zygomatic muscles are involved and excessive gingiva can be seen in the anterior and posterior areas [4].
A wide range of techniques are available for GS treatment such as orthognathic surgery, lip repositioning procedure, surgical crown lengthening, laser application, botulinum toxin (BT) injection, micro autologous fat transplantation (MAFT) and hyaluronic acid injection according to the etiology of GS [8]. The aim of this study was to review different GS treatment options and their application methods.
Materials and Methods
This review included studies related to GS treatment. A search was conducted in PubMed, Wiley and Cochrane Library from January 2015 to August 2021. We considered all available case reports, case series, retrospective studies, prospective studies, and expert reviews.
Thorough analysis was conducted on the retrieved articles. The inclusion criteria included prospective clinical studies on patients with excessive gingival show as their chief complaint, type of treatment specified, effectiveness of treatment and reporting at least 3 months of follow-up after treatment. The exclusion criteria were no information regarding the etiology of GS, combination of more than three methods of treatments, not reporting the duration of follow-up, and follow-ups shorter than 3 months. The selected studies were reviewed regarding the amount of gingival show before and after treatment, site of GS, the required preparation and product for treatment, etiology of GS, injection point (fortreatments involving injection) and targeted muscle in treatment, satisfaction rate, improvement level, treatment duration, and short-term adverse effects.
Results
According to the eligibility criteria, a total of 41 relevant case reports were retrieved and reviewed. There are several techniques to treat GS. Esthetic crown lengthening treatment includes two types of surgeries namely gingivectomy, and osseous surgery [9].
Gingivectomy is selected when the patient has more than 3 mm of gingival tissue from bone to gingival crest, adequate bone level, and appropriate attached gingiva [8]. But, gingivectomy is contraindicated when the bone level is close to the cementoenamel junction (CEJ), because gingival attachments’ biologic width can be invaded [9].
An ideal treatment method in hyperactive upper lip cases would be the lip repositioning surgery [2]. In case selection for lip repositioning, the most important factor is the upper lip length (more than 10 mm) and the gingival display [2, 10, 11]. This procedure is contraindicated in patients with severe vertical maxillary excess and in patients with an inappropriate width of attached gingiva [3, 12].
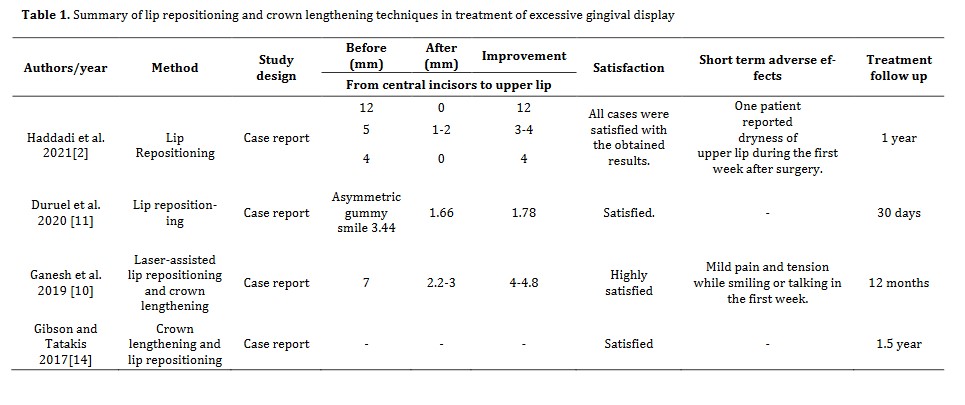
Since lasers could reduce the need for analgesics, and also decrease bleeding, the need for suturing, and postoperative discomfort, and have high patient satisfaction, they are currently considered as a convenient, fast and non-invasive treatment option. Ideal results have also been reported in gingival overgrowth and laser assisted lip repositioning [10, 13] (Table 1).
Table 1. Summary of lip repositioning and crown lengthening techniques in treatment of excessive gingival display
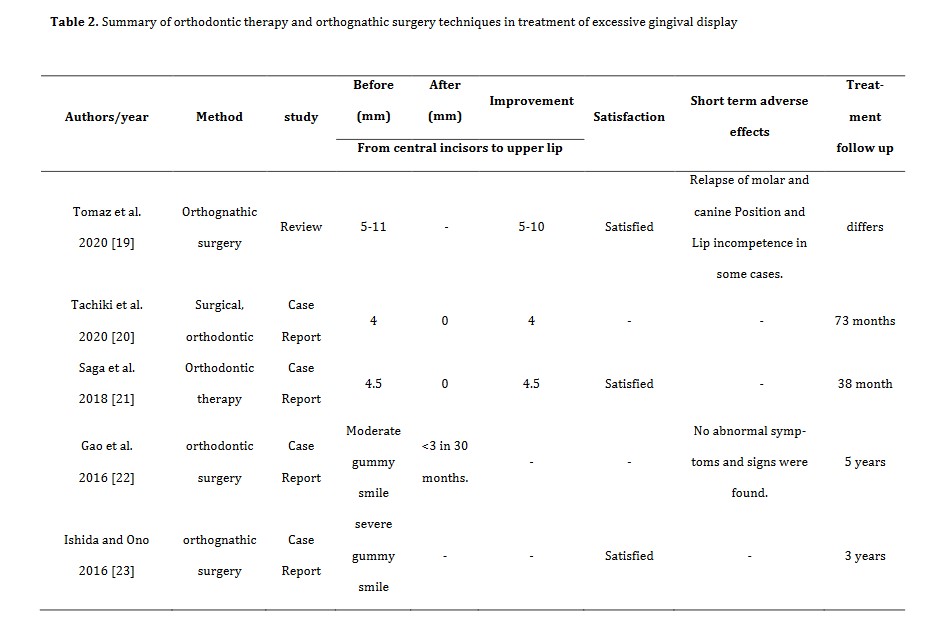
In patient with GS caused by dentoalveolar or bone problems, orthodontic therapy or orthognathic surgery is often indicated [15]. Orthodontic therapy is selected as a treatment plan when patient has dentoalveolar extrusion [9]. But if the upper third of the face is longer than the rest, the patient has VME resulting in GS. In this situation, orthognathic surgery would be the treatment of choice, which requires hospitalization [16, 17].
Swelling, pain, bruising, edema, and discomfort are among the postoperative symptoms [18] (Table 2).
Nowadays, patients prefer minimally invasive procedures to those requiring long follow-ups [24]. BT injection is a minimally invasive procedure that is recommended for patients with hyperactive lip muscle causing GS [1, 6, 9]. The onset of action of BT is between 24 to 72 hours [1]. Within 7-14 days, it reaches its maximum effect [1, 6]. Based on the dosage of BT and site of injection, the outcomes may differ. Some authors reported no relationship VME resulting in GS. In this situation, orthognathic surgery would be the treatment of choice, which requires hospitalization [16, 17].
Swelling, pain, bruising, edema, and discomfort are among the postoperative symptoms [18] (Table 2).
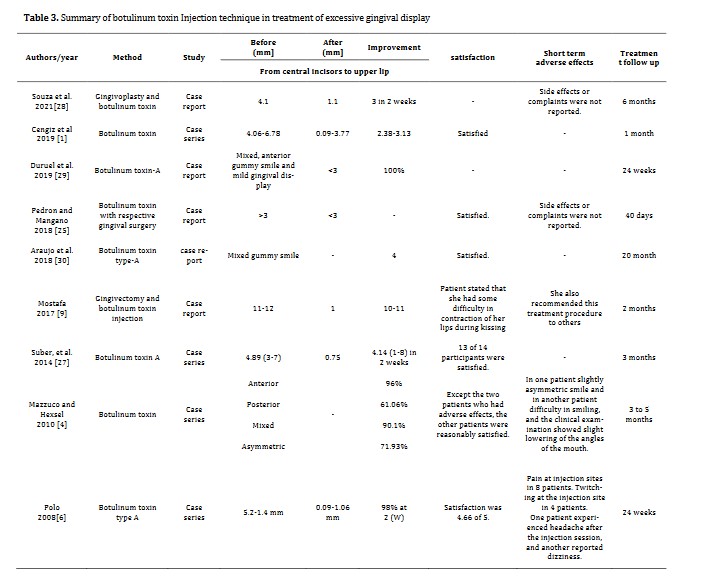
between the average percentage of improvement and number of injections at each site [8]. The durability of the results of BT injection depends on the extent of gingival exposure in smiling and the muscle movement frequency. It does not depend on the BT dosage [9]. It is a safe and effective nonsurgical therapy with high patient satisfaction which improves smile aesthetics [1, 4, 6, 8, 25-27] (Table 3).
Table 3. Summary of botulinum toxin Injection technique in treatment of excessive gingival display
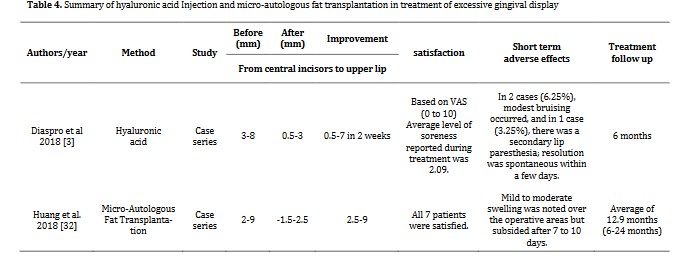
Hyaluronic acid, a novel approach, is another treatment option for GS. A small bolus dose of hyaluronic acid could be injected at the same site that BT is injected. It can inhibit movement of the deep portion of LLSAN and decrease the upper lip elevation in smiling [3]. The results of hyaluronic acid injection last much longer than BT (6 to 8 months versus 3 to 5 months). The results appear immediately and a localized volumization can be seen [31].
The short-term limited effect of BT is considered as a disadvantage which can be improved by injection of hyaluronic acid filler [24]. However, filler injection costs much more than BT [31]. Micro autologous fat transplantation (MAFT) is another reliable alternative strategy to correct a GS with optimal outcome that lasts longer [3, 32] (Table 4).
In patients with multiple occlusal problems, orthodontic treatment is often more beneficial and GS can be treated secondary to occlusal problems, and the results last a lifetime [21, 22 ,14]. However, some patients choose alternative treatment options to avoid surgery and camouflage the problem [15] (Table 4).
Discussion
Smile has an important role in facial appearance and represents kindness and confidence. Three factors that create a pleasant smile include the upper lip (levator) muscles, anterior maxillary bone, and anterior maxillary teeth. Dysfunction in each factor can lead to an unpleasant smile [33]. Das et al. suggested some preoperative examinations to help select the most appropriate treatment method. Age, height, and symmetry of the face and upper lip at rest position, lip mobility, crown-root ratio, width/length ratio of maxillary anterior region, sulcus depth, mucogingival junction position, supracrestal tissue attachment width, keratinized gingiva width, CEJ and alveolar crest are items that influence the selection of GS treatment method [34]. Moreover, patients often force the dentists to adopt less invasive methods. Thus, GS treatment techniques develop towards less invasiveness.
Alammar et al. compared two lip repositioning techniques (standard and modified) and showed that modified lip repositioning technique yielded more satisfying results, more stability, and less relapse at the 6-month follow-up in comparison with the conventional technique in patients with hypermobile lip elevator muscles or short upper lip [35].
Ganesh et al, also assessed a combination of methods (laser-assisted lip repositioning, and crown lengthening) and showed its effectiveness and stability at the 1-year follow-up in altered passive eruption Type 1A patients with hypermobile upper lip elevator muscle [10].
VME is the initial reason of GS caused by skeletal problems [36]. Graber and Salama proposed a classification based on excessive gingival display caused by VME. In VME I, gingival exposure is less than 4 mm. VME II has 4-8 mm of gingival exposure, and VME III has more than 8 mm of gingival display [37]. VME III and VME II patients need more complicated treatments, such as a combination of periodontal and orthognathic surgery, orthodontic therapy, and restorative treatments. However, VME I treatment is less invasive. But, it is important to know the source of VME. It can be in the posterior region, anterior region, or both, and can be bilateral or unilateral [38]. Bastidas evaluated class II malocclusion cases with excessive vertical growth that were treated with orthognathic surgery in his review. He concluded that Le Fort I osteotomy was not the first treatment choice, but it was the most functional treatment for other problems in some patients who were satisfied with their treatment [16].
Although orthodontic treatment has long-lasting effects and almost eliminates the problem forever, treatments with short-term effects are increasingly developed to fulfil patient demands. Souza et al. evaluated a patient with 4.1 mm GS who was treated with gingivoplasty and BT. Even though the results were acceptable, they mentioned that the patient should be aware of GS recurrence as the effect only lasts for 3 to 6 months, based on the brand of BT [28]. Cengiz et al. assessed the differences between BT injection in orbicularis oris muscle and LLSAN muscle and its recurrence over time in patients who refused to undergo orthognathic or periodontal surgery. They concluded that injection in orbicularis oris muscle reached its maximum effect 15 days sooner than LLSAN. But excessive gingival display returned after 4 months [1]. In a study by Diaspro et al, 0.2 to 0.3 mL of hyaluronic acid was injected into lateral fibers of the LLSAN muscle and immediate resolution occurred that lasted averagely for 7.1 months [3]. Huang et al. performed MAFT and showed that 16.1 ml fat only took 52 minutes to transplant and lasted averagely for 12.9 months with no significant complication [32]. As mentioned, the current novel approaches were developed to eliminate the disadvantages of BT, such as its late onset of action and short duration of results. Future psychological studies are required to find out why patients refuse to undergo orthognathic treatment and prefer to repeat the injection approximately every 6 months instead of treating their GS by orthodontic treatment.
Conclusion
Nowadays, patients prefer less invasive treatments with less postoperative complications compared with those that require hospitalization. Although orthodontic treatment could completely solve the GS problem, patients prefer methods that last shorter such as BT injection, hyaluronic acid injection, and MAFT; maybe because of low number of follow-ups and fast outcomes.
Acknowledgment
The authors declare no conflict of interests related to this review.
Full-Text: (1474 Views)
| Abstract
Background and Aim: Nowadays, facial esthetics has become the main concern for many people. Gummy smile (GS) is a common complaint that affects the esthetics and psychological status of patients. The aim of this study was to review GS treatment options. Materials and Methods: An electronic search was conducted in three databases of PubMed, Wiley and Cochrane Library from January 2015 up to August 2021. According to the eligibility criteria, a total of 41 relevant papers were retrieved and reviewed. Results: Based on the available data, several techniques have been reported for GS treatment, such as lip repositioning, crown lengthening, orthognathic surgery, laser application, botulinum toxin (BT) injection, hyaluronic acid injection, and micro autologous fat transplantation (MAFT). Combination of two or three of these techniques may yield a better result. Conclusion: A wide variety of procedures are available based on the cause of GS. The new, less invasive, faster and safer alternative techniques were shown to be feasible with a long-lasting result and minimal postoperative sequelae. Such treatment options for various types of GS can lead to significant improvement in smile esthetics with high patient satisfaction. Key Words: Botulinum Toxins; Esthetics; Gingivectomy; Lasers; Smiling; Transplantation |
Introduction
Several parameters are involved in creation of a beautiful smile [1]. Excessive gingival display could be secondary to modified passive eruption, inadequate upper lip muscle, small upper lip, short crowns, high mobility of the upper lip, anterior dentoalveolar extrusion, bimaxillary protrusion, and vertical maxillary excess (VME) [1-3].
Factors that affect the smile include type of face, symmetry and vertical height of face, smile line, thickness, size and shape of the lips, alveolar bone thickness, type of gingiva, and height and form of the teeth that should be considered in treatment of gummy smile (GS) [3]. Mazzuco and Hexsel represented a classification based on the amount of excessive gingival exposure [4]. In a normal smile, less than 3 mm of gingiva can be seen in the anterior region [5]. Patients with anterior GS have more than 3 mm of their gingiva between their canine teeth exposed during smiling. In this situation, the levator labii superioris alaeque nasi (LLSAN) muscle is involved. Zygomatic muscles are involved in posterior GS, which is characterized by exposure of more than 3 mm of the gingiva posterior to canine teeth [4-7]. In asymmetrical GS, one of these muscles (LLSAN or zygomatic muscles) is involved and excessive gingiva is shown in one site; whereas, in mixed GS, both LLSAN and zygomatic muscles are involved and excessive gingiva can be seen in the anterior and posterior areas [4].
A wide range of techniques are available for GS treatment such as orthognathic surgery, lip repositioning procedure, surgical crown lengthening, laser application, botulinum toxin (BT) injection, micro autologous fat transplantation (MAFT) and hyaluronic acid injection according to the etiology of GS [8]. The aim of this study was to review different GS treatment options and their application methods.
Materials and Methods
This review included studies related to GS treatment. A search was conducted in PubMed, Wiley and Cochrane Library from January 2015 to August 2021. We considered all available case reports, case series, retrospective studies, prospective studies, and expert reviews.
Thorough analysis was conducted on the retrieved articles. The inclusion criteria included prospective clinical studies on patients with excessive gingival show as their chief complaint, type of treatment specified, effectiveness of treatment and reporting at least 3 months of follow-up after treatment. The exclusion criteria were no information regarding the etiology of GS, combination of more than three methods of treatments, not reporting the duration of follow-up, and follow-ups shorter than 3 months. The selected studies were reviewed regarding the amount of gingival show before and after treatment, site of GS, the required preparation and product for treatment, etiology of GS, injection point (fortreatments involving injection) and targeted muscle in treatment, satisfaction rate, improvement level, treatment duration, and short-term adverse effects.
Results
According to the eligibility criteria, a total of 41 relevant case reports were retrieved and reviewed. There are several techniques to treat GS. Esthetic crown lengthening treatment includes two types of surgeries namely gingivectomy, and osseous surgery [9].
Gingivectomy is selected when the patient has more than 3 mm of gingival tissue from bone to gingival crest, adequate bone level, and appropriate attached gingiva [8]. But, gingivectomy is contraindicated when the bone level is close to the cementoenamel junction (CEJ), because gingival attachments’ biologic width can be invaded [9].
An ideal treatment method in hyperactive upper lip cases would be the lip repositioning surgery [2]. In case selection for lip repositioning, the most important factor is the upper lip length (more than 10 mm) and the gingival display [2, 10, 11]. This procedure is contraindicated in patients with severe vertical maxillary excess and in patients with an inappropriate width of attached gingiva [3, 12].
Since lasers could reduce the need for analgesics, and also decrease bleeding, the need for suturing, and postoperative discomfort, and have high patient satisfaction, they are currently considered as a convenient, fast and non-invasive treatment option. Ideal results have also been reported in gingival overgrowth and laser assisted lip repositioning [10, 13] (Table 1).
Table 1. Summary of lip repositioning and crown lengthening techniques in treatment of excessive gingival display
{kind=link}
In patient with GS caused by dentoalveolar or bone problems, orthodontic therapy or orthognathic surgery is often indicated [15]. Orthodontic therapy is selected as a treatment plan when patient has dentoalveolar extrusion [9]. But if the upper third of the face is longer than the rest, the patient has VME resulting in GS. In this situation, orthognathic surgery would be the treatment of choice, which requires hospitalization [16, 17].
Swelling, pain, bruising, edema, and discomfort are among the postoperative symptoms [18] (Table 2).
Nowadays, patients prefer minimally invasive procedures to those requiring long follow-ups [24]. BT injection is a minimally invasive procedure that is recommended for patients with hyperactive lip muscle causing GS [1, 6, 9]. The onset of action of BT is between 24 to 72 hours [1]. Within 7-14 days, it reaches its maximum effect [1, 6]. Based on the dosage of BT and site of injection, the outcomes may differ. Some authors reported no relationship VME resulting in GS. In this situation, orthognathic surgery would be the treatment of choice, which requires hospitalization [16, 17].
Swelling, pain, bruising, edema, and discomfort are among the postoperative symptoms [18] (Table 2).
{kind=link}
between the average percentage of improvement and number of injections at each site [8]. The durability of the results of BT injection depends on the extent of gingival exposure in smiling and the muscle movement frequency. It does not depend on the BT dosage [9]. It is a safe and effective nonsurgical therapy with high patient satisfaction which improves smile aesthetics [1, 4, 6, 8, 25-27] (Table 3).
Table 3. Summary of botulinum toxin Injection technique in treatment of excessive gingival display
{kind=link}
Hyaluronic acid, a novel approach, is another treatment option for GS. A small bolus dose of hyaluronic acid could be injected at the same site that BT is injected. It can inhibit movement of the deep portion of LLSAN and decrease the upper lip elevation in smiling [3]. The results of hyaluronic acid injection last much longer than BT (6 to 8 months versus 3 to 5 months). The results appear immediately and a localized volumization can be seen [31].
The short-term limited effect of BT is considered as a disadvantage which can be improved by injection of hyaluronic acid filler [24]. However, filler injection costs much more than BT [31]. Micro autologous fat transplantation (MAFT) is another reliable alternative strategy to correct a GS with optimal outcome that lasts longer [3, 32] (Table 4).
In patients with multiple occlusal problems, orthodontic treatment is often more beneficial and GS can be treated secondary to occlusal problems, and the results last a lifetime [21, 22 ,14]. However, some patients choose alternative treatment options to avoid surgery and camouflage the problem [15] (Table 4).
{kind=link}
Discussion
Smile has an important role in facial appearance and represents kindness and confidence. Three factors that create a pleasant smile include the upper lip (levator) muscles, anterior maxillary bone, and anterior maxillary teeth. Dysfunction in each factor can lead to an unpleasant smile [33]. Das et al. suggested some preoperative examinations to help select the most appropriate treatment method. Age, height, and symmetry of the face and upper lip at rest position, lip mobility, crown-root ratio, width/length ratio of maxillary anterior region, sulcus depth, mucogingival junction position, supracrestal tissue attachment width, keratinized gingiva width, CEJ and alveolar crest are items that influence the selection of GS treatment method [34]. Moreover, patients often force the dentists to adopt less invasive methods. Thus, GS treatment techniques develop towards less invasiveness.
Alammar et al. compared two lip repositioning techniques (standard and modified) and showed that modified lip repositioning technique yielded more satisfying results, more stability, and less relapse at the 6-month follow-up in comparison with the conventional technique in patients with hypermobile lip elevator muscles or short upper lip [35].
Ganesh et al, also assessed a combination of methods (laser-assisted lip repositioning, and crown lengthening) and showed its effectiveness and stability at the 1-year follow-up in altered passive eruption Type 1A patients with hypermobile upper lip elevator muscle [10].
VME is the initial reason of GS caused by skeletal problems [36]. Graber and Salama proposed a classification based on excessive gingival display caused by VME. In VME I, gingival exposure is less than 4 mm. VME II has 4-8 mm of gingival exposure, and VME III has more than 8 mm of gingival display [37]. VME III and VME II patients need more complicated treatments, such as a combination of periodontal and orthognathic surgery, orthodontic therapy, and restorative treatments. However, VME I treatment is less invasive. But, it is important to know the source of VME. It can be in the posterior region, anterior region, or both, and can be bilateral or unilateral [38]. Bastidas evaluated class II malocclusion cases with excessive vertical growth that were treated with orthognathic surgery in his review. He concluded that Le Fort I osteotomy was not the first treatment choice, but it was the most functional treatment for other problems in some patients who were satisfied with their treatment [16].
Although orthodontic treatment has long-lasting effects and almost eliminates the problem forever, treatments with short-term effects are increasingly developed to fulfil patient demands. Souza et al. evaluated a patient with 4.1 mm GS who was treated with gingivoplasty and BT. Even though the results were acceptable, they mentioned that the patient should be aware of GS recurrence as the effect only lasts for 3 to 6 months, based on the brand of BT [28]. Cengiz et al. assessed the differences between BT injection in orbicularis oris muscle and LLSAN muscle and its recurrence over time in patients who refused to undergo orthognathic or periodontal surgery. They concluded that injection in orbicularis oris muscle reached its maximum effect 15 days sooner than LLSAN. But excessive gingival display returned after 4 months [1]. In a study by Diaspro et al, 0.2 to 0.3 mL of hyaluronic acid was injected into lateral fibers of the LLSAN muscle and immediate resolution occurred that lasted averagely for 7.1 months [3]. Huang et al. performed MAFT and showed that 16.1 ml fat only took 52 minutes to transplant and lasted averagely for 12.9 months with no significant complication [32]. As mentioned, the current novel approaches were developed to eliminate the disadvantages of BT, such as its late onset of action and short duration of results. Future psychological studies are required to find out why patients refuse to undergo orthognathic treatment and prefer to repeat the injection approximately every 6 months instead of treating their GS by orthodontic treatment.
Conclusion
Nowadays, patients prefer less invasive treatments with less postoperative complications compared with those that require hospitalization. Although orthodontic treatment could completely solve the GS problem, patients prefer methods that last shorter such as BT injection, hyaluronic acid injection, and MAFT; maybe because of low number of follow-ups and fast outcomes.
Acknowledgment
The authors declare no conflict of interests related to this review.
Type of Study: Review article |
Subject:
Periodontology
References
1. Cengiz AF, Goymen M, Akcali C. Efficacy of botulinum toxin for treating a gummy smile. Am J Orthod Dentofacial Orthop. 2020 Jul;158(1):50-8. [DOI:10.1016/j.ajodo.2019.07.014] [PMID]
2. Haddadi P, Zare H, Azadikhah A. Lip Repositioning, a Solution for Gummy Smile. Front Dent. 2021 Apr 22;18:15. [DOI:10.18502/fid.v18i15.6140] [PMID] [PMCID]
3. Diaspro A, Cavallini M, Piersini P, Sito G. Gummy Smile Treat-ment: Proposal for a Novel Corrective Technique and a Review of the Literature. Aesthet Surg J. 2018 Nov 12; 38 (12):1330-8. [DOI:10.1093/asj/sjy174] [PMID]
4. Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. J Am Acad Dermatol. 2010 Dec;63(6):1042-51. [DOI:10.1016/j.jaad.2010.02.053] [PMID]
5. Mangano A, Mangano A. Current strategies in the treatment of gummy smile using botulinum toxin type A. Plast Reconstr Surg. 2012 Jun;129(6):1015e. [DOI:10.1097/PRS.0b013e31824f00a6] [PMID]
6. Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smil-ing (gummy smile). Am J Orthod Dentofacial Orthop. 2008 Feb;133(2):195-203. [DOI:10.1016/j.ajodo.2007.04.033] [PMID]
7. Rodríguez-Martínez A, Vicente-Hernández A, Bravo-González LA. Effect of posterior gingival smile on the perception of smile esthetics. Med Oral Patol Oral Cir Bucal. 2014 Jan 1;19(1):e82-7. [DOI:10.4317/medoral.19167] [PMID] [PMCID]
8. Duruel O, Ataman-Duruel ET, Berker E, Tözüm TF. Treatment of Various Types of Gummy Smile With Botulinum Toxin-A. J Craniofac Surg. 2019 May/Jun;30(3):876-8. [DOI:10.1097/SCS.0000000000005298] [PMID]
9. Mostafa D. A successful management of sever gummy smile using gingivectomy and botulinum toxin injection: A case re-port. Int J Surg Case Rep. 2018;42:169-74. [DOI:10.1016/j.ijscr.2017.11.055] [PMID] [PMCID]
10. Ganesh B, Burnice NKC, Mahendra J, Vijayalakshmi R, K AK. Laser-Assisted Lip Repositioning With Smile Elevator Muscle Containment and Crown Lengthening for Gummy Smile: A Case Report. Clin Adv Periodontics. 2019 Sep; 9(3): 135-41. [DOI:10.1002/cap.10060] [PMID]
11. Duruel O, Erduran NE, Tözüm TF. A Modification for Treat-ment of Excessive Gingival Display: Tooth-Based Lip-Repositioning Technique. Int J Periodontics Restorative Dent. 2020 May/Jun;40(3):457-61. [DOI:10.11607/prd.4465] [PMID]
12. Faus-Matoses V, Faus-Matoses I, Jorques-Zafrilla A, Faus-Llácer VJ. Lip repositioning technique. A simple surgical procedure to improve the smile harmony. J Clin Exp Dent. 2018 Apr 1;10(4):e408-e412. [DOI:10.4317/jced.54721] [PMID] [PMCID]
13. Jha N, Ryu JJ, Wahab R, Al-Khedhairy AA, Choi EH, Kaushik NK. Treatment of oral hyperpigmentation and gummy smile using lasers and role of plasma as a novel treatment technique in dentistry: An introductory review. Oncotarget. 2017 Mar 21;8(12):20496-20509. [DOI:10.18632/oncotarget.14887] [PMID] [PMCID]
14. Gibson MP, Tatakis DN. Treatment of Gummy Smile of Multi-factorial Etiology: A Case Report. Clin Adv Periodontics. 2017 Nov;7(4):167-73. [DOI:10.1902/cap.2017.160074] [PMID]
15. Izraelewicz-Djebali E, Chabre C. Gummy smile: orthodontic or surgical treatment? Journal of Dentofacial Anomalies and Orthodontics. 2015;18(1):102. [DOI:10.1051/odfen/2014036]
16. Bastidas JA. Surgical Correction of the "Gummy Smile". Oral Maxillofac Surg Clin North Am. 2021 May;33(2):197-209. [DOI:10.1016/j.coms.2021.01.005] [PMID]
17. Ramesh A, Vellayappan R, Ravi S, Gurumoorthy K. Esthetic lip repositioning: A cosmetic approach for correction of gummy smile - A case series. J Indian Soc Periodontol. 2019 May-Jun;23(3):290-4. [DOI:10.4103/jisp.jisp_548_18] [PMID] [PMCID]
18. Kim SG, Park SS. Incidence of complications and problems related to orthognathic surgery. J Oral Maxillofac Surg. 2007 Dec;65(12):2438-44. [DOI:10.1016/j.joms.2007.05.030] [PMID]
19. Tomaz AFG, Marinho LCN, de Aquino Martins ARL, Lins RDAU, de Vasconcelos Gurgel BC. Impact of orthognathic sur-gery on the treatment of gummy smile: an integrative review. Oral Maxillofac Surg. 2020 Sep;24(3):283-8. [DOI:10.1007/s10006-020-00857-4] [PMID]
20. Tachiki C, Yamamoto M, Takaki T, Nishii Y. Surgical Orthodontic Treatment in Case of Severe High Angle Skeletal Class II Malocclusion and Mandibular Retrusion. Bull Tokyo Dent Coll. 2020 Dec 16;61(4):243-53. [DOI:10.2209/tdcpublication.2020-0022] [PMID]
21. Saga AY, Araújo EA, Antelo OM, Meira TM, Tanaka OM. Non-surgical treatment of skeletal maxillary protrusion with gummy smile using headgear for growth control, mini-implants as an-chorage for maxillary incisor intrusion, and premolar extrac-tions for incisor retraction. Am J Orthod Dentofacial Orthop. 2020 Feb;157(2):245-58. [DOI:10.1016/j.ajodo.2018.09.021] [PMID]
22. Gao X, Wang T, Song J. Orthodontic and surgical management of a patient with severe skeletal Class II deformity and facial asymmetry: A case report with a 5-year follow-up. Am J Orthod Dentofacial Orthop. 2017 Apr; 151 (4):779-92. [DOI:10.1016/j.ajodo.2016.02.034] [PMID]
23. Ishida Y, Ono T. Nonsurgical treatment of an adult with a skeletal Class II gummy smile using zygomatic temporary an-chorage devices and improved superelastic nickel-titanium alloy wires. Am J Orthod Dentofacial Orthop. 2017 Nov;152(5):693-705. [DOI:10.1016/j.ajodo.2016.09.030] [PMID]
24. Mercado-García J, Rosso P, Gonzalvez-García M, Colina J, Fernández JM. Gummy Smile: Mercado-Rosso Classification System and Dynamic Restructuring with Hyaluronic Acid. Aes-thetic Plast Surg. 2021 Oct;45(5):2338-49. [DOI:10.1007/s00266-021-02169-8] [PMID] [PMCID]
25. Pedron IG, Mangano A. Gummy Smile Correction Using Botulinum Toxin With Respective Gingival Surgery. J Dent (Shi-raz). 2018 Sep;19(3):248-52.
26. Myung Y, Woo K, Kim ST. Treatment of gummy smile using botulinum toxin: a review. Journal of Dental Rehabilitation and Applied Science. 2021;37(2):61-72. [DOI:10.14368/jdras.2021.37.2.61]
27. Suber JS, Dinh TP, Prince MD, Smith PD. OnabotulinumtoxinA for the treatment of a "gummy smile". Aesthet Surg J. 2014 Mar;34(3):432-7. [DOI:10.1177/1090820X14527603] [PMID]
28. Souza FCG, da Silva SR, Neto ALSA, Shitsuka C, Pedron IG. Gingivoplasty and Botulinum Toxin Application to Improve Gummy Smile: Case Report. SVOA Dentistry. 2021;2(3):109-14.
29. Duruel O, Ataman-Duruel ET, Tözüm TF, Berker E. Ideal Dose and Injection Site for Gummy Smile Treatment with Botu-linum Toxin-A: A Systematic Review and Introduction of a Case Study. Int J Periodontics Restorative Dent. 2019 Jul/ Aug;39(4):e167-e173. [DOI:10.11607/prd.3580] [PMID]
30. Araujo JP, Cruz J, Oliveira JX, Canto AM. Botulinum Toxin Type-A as an alternative treatment for gummy smile: a case report. Dermatol Online J. 2018 Jul 15;24(7):13030/qt 75 f0h8kz. [DOI:10.5070/D3247040926] [PMID]
31. Hsien-Li Peng P, Peng JH. Treating the Gummy Smile With Hyaluronic Acid Filler Injection. Dermatol Surg. 2019 Mar;45(3):478-80. [DOI:10.1097/DSS.0000000000001563] [PMID]
32. Huang SH, Huang YH, Lin YN, Lee SS, Chou CK, Lin TY, Takahashi H, Kuo YR, Lai CS, Lin SD, Lin TM. Micro-Autologous Fat Transplantation for Treating a Gummy Smile. Aesthet Surg J. 2018 Aug 16;38(9):925-37. [DOI:10.1093/asj/sjy069] [PMID] [PMCID]
33. Mate PP, Nilesh K, Joshi A, Panda A. Clinical and electromyographic evaluation of botulinum toxin type A in the treatment of gummy smile: A prospective clinical study. J Dent Res Dent Clin Dent Prospects. 2021 Spring;15(2):122-8. [DOI:10.34172/joddd.2021.021] [PMID] [PMCID]
34. Das A, Mondal D, Chordia R, Chatterji A. Decision-making process for esthetic treatment of gummy smile: A surgical per-spective. J Indian Soc Periodontol. 2021 Nov-Dec; 25(6): 560-4. [DOI:10.4103/jisp.jisp_879_20] [PMID] [PMCID]
35. Alammar A, Heshmeh O, Mounajjed R, Goodson M, Hamadah O. A comparison between modified and conventional surgical techniques for surgical lip repositioning in the management of the gummy smile. J Esthet Restor Dent. 2018 Nov;30(6):523-31. [DOI:10.1111/jerd.12433] [PMID]
36. Waldrop TC. Gummy Smiles: The Challenge of Gingival Excess: Prevalence and Guidelines for Clinical Management. Seminars in Orthodontics. 2008;14: 260-71. [DOI:10.1053/j.sodo.2008.07.004]
37. Garber DA, Salama MA. The aesthetic smile: diagnosis and treatment. Periodontol 2000. 1996 Jun;11:18-28. [DOI:10.1111/j.1600-0757.1996.tb00179.x] [PMID]
38. Ser Yun JB, Luo M, Yin Y, Zhi Hui VL, Fang B, Han XL. Etiology-Based Treatment Strategy for Excessive Gingival Display: Liter-ature Review. World Journal of Surgery and Surgical Research. 2019; 2: 1103.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
