Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 1 (3-2026)
J Res Dent Maxillofac Sci 2026, 11(1): 8-21 |
Back to browse issues page
Ethics code: IRCT20101204005305N22
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shahbazpey S, Mohammadi M, Lashkarizadeh N. Comparative Efficacy of Acellular Dermal Matrix with and without Injectable Platelet-Rich Fibrin, and Free Gingival Graft for Enhancement of Peri-Implant Keratinized Gingiva Width: A Randomized Controlled Clinical Trial. J Res Dent Maxillofac Sci 2026; 11 (1) :8-21
URL: http://jrdms.dentaliau.ac.ir/article-1-1274-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-1274-en.html


1- Department of Periodontics, School of Dentistry, Kerman University of Medical Sciences, Shafa St, Kerman, 7616913555, Iran
2- Department of Periodontics, School of Dentistry, Kerman University of Medical Sciences, Shafa St, Kerman, 7616913555, Iran ,Mmohammadi28@yahoo.com
2- Department of Periodontics, School of Dentistry, Kerman University of Medical Sciences, Shafa St, Kerman, 7616913555, Iran ,
Full-Text [PDF 408 kb]
(40 Downloads)
| Abstract (HTML) (65 Views)
Introduction
Table 1. Mean KGW (mm) in the three groups before and after treatment
Table 2. Mean PPD (mm) in the three groups before and after treatment
Table 3. Mean graft height (mm), length (mm), and surface area (mm2) in the three groups before and after treatment
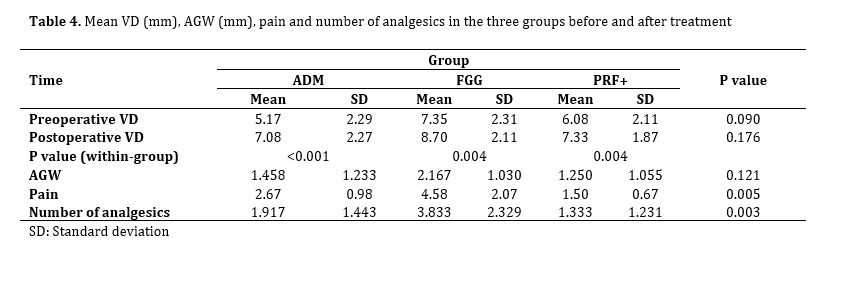
Table 4. Mean VD (mm), AGW (mm), pain and number of analgesics in the three groups before and after treatment
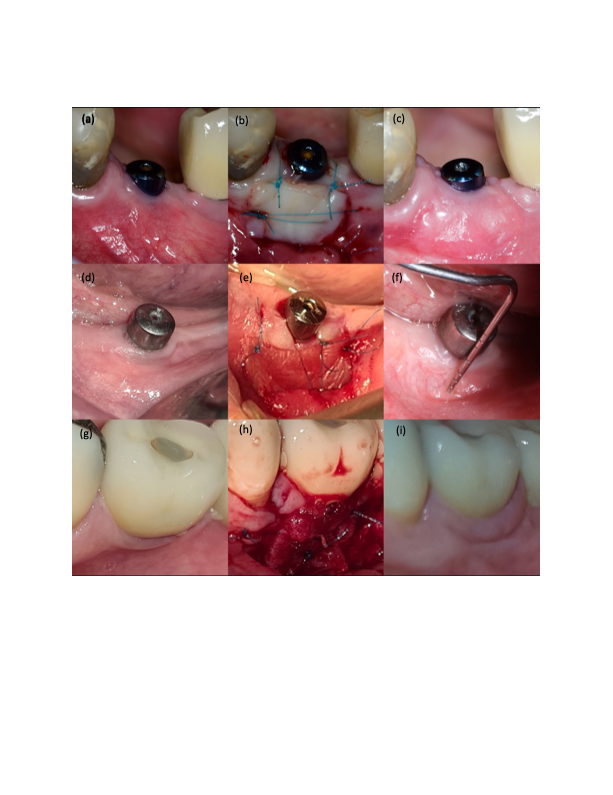
Figure 1. Clinical photographs illustrating three different surgical approaches for increasing peri-implant keratinized gingiva width.
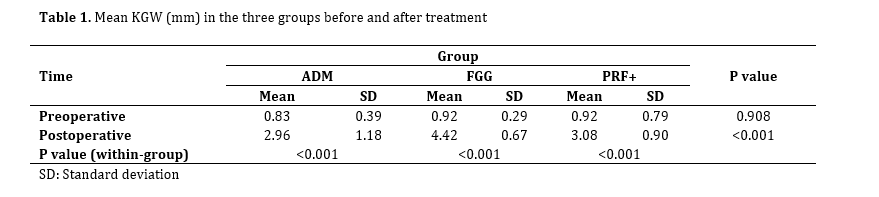
The present study compared iPRF-impregnated ADM, iPRF-free ADM, and FGG for enhancement of peri-implant KGW. The results showed a significant increase in KGW in all three groups 3 months after treatment. The gain in KGW was 2.16 mm in the ADM, 3.5 mm in the FGG, and 2.19 mm in the ADM/iPRF group.
Ramanauskaite et al. [27] compared three-dimensional changes of porcine-derived collagen matrix and FGG for increasing the KGW around dental implants over a 6-month period and concluded that FGG produced a wider keratinized band compared to the collagen matrix. Basegmez et al. [28] conducted a clinical trial comparing the effectiveness of ADM versus FGG for augmentation of peri-implant keratinized gingiva, and showed that although ADM allografts were able to increase peri-implant KGW, FGGs appeared to be more effective, which was in line with the present findings. Also, Han et al. [29] evaluated the changes in KGW in molar areas after FGG before implant placement and showed its favorable results, such that KGW increased by 2.9 mm, which was less than that in the present study (3.5 mm in the FGG group). Park [20] investigated the clinical effectiveness of ADM to increase peri-implant keratinized mucosa and reported that peri-implant KGW increased by an average of 2.4 mm over 3 months, which was slightly greater than the value obtained in the present study. It seems that the synergy of three factors namely heterogeneity of surgical techniques in soft tissue manipulation, variability in the host biological response to residual antigens in ADM, and finally differences in postoperative protocols might be responsible for the difference in the results between the current study and previous investigations.
PRF induces new angiogenesis, accelerates wound closure, and speeds up cicatricial tissue remodeling. Since PRF is produced without using any additives, fibrin polymerization occurs in a physiological manner, resulting in a fibrin network similar to that formed during natural healing. However, in the present study, we expected the PRF to improve KGW more than other products, but this trend was not observed.
Also, the findings of the current study indicated a significant decrease in graft height after treatment in all three groups, and the mixed linear model confirmed a significant interaction between group and time. These findings indicate that the treatment results differed depending on the method used. It is noteworthy that the FGG group showed a greater graft height after treatment than the other groups. Also, the results showed that the mean graft length in the three groups did not differ significantly after treatment compared with before. These two factors were used to measure the changes in the graft surface area in the three groups, and the results indicated that the graft surface area decreased significantly after treatment in all groups. Also, FGG showed a larger graft surface area than the other groups after treatment. In the present study, the purpose of measuring the graft surface area was to evaluate the percentage of graft shrinkage, which was reported to be 52.55% ± 11.23% in the FGG group, lower than the value in the other two groups. Excessive shrinkage is one of the problems that may limit the use of ADM [18]. Agarwal et al. [30] compared FGG and AlloDerm® in increasing the KGW in a clinical study. They indicated that KGW significantly increased after both treatments, but this increase was relatively less in the ADM allograft group. The ADM site had significantly more shrinkage (76.6%) than the FGG site (49.7%), which was consistent with the present study.
Also, in another study, the efficacy of ADM allograft was clinically evaluated to increase AGW. The results showed that ADM allograft was less effective and predictable than FGG for this purpose due to significant shrinkage and unstable quality of the obtained attached gingiva, but the cosmetic results with ADM allograft were better than those with FGG [18]. Lorenzo et al. [14] used a type of ADM for soft tissue augmentation around dental implants and achieved a 2.9 mm increase in KGW after 6 months, which was comparable to the 2.8 mm increase in the control group (connective tissue graft), and the mean shrinkage of ADM was about 60%, which was in line with the present study.
Temmerman et al. [31] evaluated the efficacy of PRF for the enhancement of KGW around dental implants. They examined the percentage of shrinkage and concluded that the shrinkage rate after 6 weeks was 32.1% in the PRF group and 23.6% in the control group (FGG). However, this difference was not statistically significant. A systematic review conducted by Giammarinaro et al. [32] on whether PRF improves soft tissue outcomes around implants showed the superiority of FGG to PRF, which was consistent with the present results. Autogenous grafts have better dimensional stability than acellular dermal matrices due to their inherent biological properties and vascularization potential. Lower shrinkage of the FGG is also consistent with the well-known clinical phenomenon that autogenous tissues retain their volume better during the healing process, while AlloDerm undergoes greater resorption and deformation. However, despite the favorable shrinkage rate, the use of FGG is associated with more patient complications, including discomfort at the graft site and prolonged healing, which may limit its widespread use.
In the present study, the mean PPD was not significantly different among the three groups. This was in line with the results of Zheng et al. [33], who evaluated the clinical outcomes and soft tissue changes after implant treatment in groups with and without FGG. They demonstrated no significant difference in PPD between the FGG and the control groups. Also, Papi et al. [34] investigated the clinical changes in mucosal thickness after treatment with ADM, and reported that the mean recorded PPD did not increase significantly, which was also similar to the present study.
Pain is an important patient-reported criterion that determines the quality of patient's surgical experience. The present results showed that patients treated with ADM/iPRF experienced significantly lower postoperative pain than patients who received FGG as the standard treatment or ADM alone. This finding highlights the potential benefit of combining PRF with ADM in reducing postoperative discomfort in periodontal grafts or oral surgeries. This finding was consistent with the existing literature on the biological properties of PRF. PRF is initially composed of fibrinogen and thrombin, which are gradually converted to fibrin and form a blood clot after approximately 15 minutes. The fibrin network contains a large number of platelets and leukocytes, which secrete high concentrations of growth factors, including PDGF, insulin-like growth factor-1, VEGF, and TGF-β1, for up to 10 days [35].
IPRF enhances the migration, proliferation, and expansion of gingival fibroblasts, as well as the expression of messenger RNA of genes involved in regeneration (PDGF, TGF-β1, and collagen 1). Thus, PRF acts as a reservoir with long-term secretion of growth factors (PDGF, TGF-β, VEGF) and cytokines that actively modulate inflammation, promote angiogenesis, and accelerate soft tissue healing [36].
Gupta and Agarwal [37] evaluated the effect of advanced PRF compared to natural healing on extraction sockets and assessed pain, edema, and soft tissue healing. They showed that there was a significant reduction in pain and improvement of soft tissue healing at PRF-treated sites compared to control sites on days 3 and 7 after tooth extraction, which was attributed to the anti-inflammatory properties of PRF, which releases growth factors and enhances wound healing. Also, Yang et al. [38] evaluated the clinical and biochemical outcomes after mandibular third molar extraction surgery using ALB-PRF on one side and PRF on the other. They measured pain, socket closure, infection, and swelling. Their results showed that both PRFs effectively reduced postoperative pain. Fu et al. [39] compared patient-reported and clinical outcomes after augmentation with xenogeneic collagen matrix or FGG at different postoperative stages. Their results showed that FGG was associated with greater intensity and duration of pain after augmentation of keratinized gingiva in the early stages of healing compared with xenogeneic collagen matrix. These findings may allow surgeons to better inform patients about postoperative pain for better decision-making [38].
Also, in the present study, the pain intensity in the FGG group was significantly higher than that in ADM alone. In a systematic review, Thoma et al. [40] examined patient-reported outcomes after soft tissue augmentation in dental implants. They reported a significant reduction in pain after soft tissue augmentation with ADM compared with autologous FGG. The authors attributed this to lack of a donor site, as harvesting soft tissue grafts from the palate leads to excessive bleeding, numbness, and other complications such as tissue necrosis, which increase pain. Agarwal et al. [30] in their clinical study compared FGG and AlloDerm®, and concluded that ADM had minimal postoperative pain, with no adverse effects, compared to FGG for gingival augmentation procedures.
However, Harris [19] compared ADM, FGG, and subepithelial connective tissue grafts and reported no difference in pain scores between patients treated with ADM or FGG, which was in contrast to the current results. Differences in pain score can be explained by the healing process of mucosal wounds. At the recipient site, the initial healing phase, up to 3 days, involves the survival of the graft tissue through plasma circulation from the recipient bed. However, in the FGG group, the higher pain level during the initial phase can be attributed to the healing process at the donor site proceeding with secondary intention. Therefore, specific measures to minimize the patient's postoperative pain perception are necessary to increase patient tolerance to soft tissue grafting procedures.
It is worth noting that some limitations should be considered. The specific surgical procedure, demographic characteristics of patients, and the exact time points of pain assessment require explicit description to fully understand the findings. In addition, the exact mechanism of pain reduction in the ADM/iPRF group compared to FGG, whether it is the elimination of graft site problems, the improvement of recipient site healing by PRF, or a combination of both, requires further investigation. Future studies will provide deeper insights by employing standardized pain assessment tools at specific time intervals, histological analysis of the healing site, and comparison with other methods such as connective tissue grafts combined with PRF. Nevertheless, these findings provide valuable clinical evidence supporting PRF+ADM as a promising strategy to reduce postoperative pain burden compared with conventional FGG techniques, which could lead to increased patient comfort and improved adherence to postoperative care protocols.
The present findings indicated a statistically significant difference in postoperative analgesic consumption among the three groups. Analgesic consumption in the FGG group was significantly higher than that in both the ADM and PRF+ADM groups. This observation is consistent with the data on postoperative pain in the present study and the existing evidence of higher morbidity with FGG-based procedures. The higher analgesic consumption in the FGG group can be directly attributed to problems with the palatal graft site. Secondary ulceration in the palatal region is a known source of significant pain and requires stronger pharmacological management. In contrast, lower analgesic requirement in the PRF+ADM group is likely due to the intrinsic anti-inflammatory and analgesic effects of PRF. PRF reduces the need for analgesics by modulating the secretion of proinflammatory cytokines (such as IL-6 and tumor necrosis factor-α) and increasing the secretion of anti-inflammatory interleukin-10.
Of note, there was no statistically significant difference in analgesic consumption between the ADM and PRF+ADM groups in this study. This finding suggests that elimination of the secondary graft site (which was achieved in both the ADM and PRF+ADM groups) is a key factor in reducing the need for analgesics compared to FGG, as the need for a second surgery can lead to postoperative pain and increased patient discomfort. Despite the importance of these findings, there are limitations, including lack of accurate recording of analgesic consumption by patients based on standard prescription of 400 mg ibuprofen, and lack of monitoring of analgesic consumption over short time periods (e.g., 24, 48, and 72 hours). Also, the impact of individual variables, such as patients' pain perception threshold on analgesic consumption was not assessed. However, the present objective data on higher analgesic consumption in the FGG group provide strong evidence that this method has a higher drug burden than ADM-based techniques (alone or augmented with PRF). The reduction in the need for analgesics not only indicates improved patient comfort but also may reduce the risk of drug side effects and treatment costs. Future studies could contribute to a more comprehensive understanding of this important aspect of postoperative care by designing standardized protocols for more accurate quantitative monitoring of medication consumption and considering psychological variables affecting pain perception.
Conclusion
Full-Text: (14 Views)
Abstract
Background and Aim: This study compared the efficacy of acellular dermal matrix (ADM) with and without injectable platelet-rich fibrin (iPRF) and free gingival graft (FGG) for the enhancement of peri-implant keratinized gingiva width (KGW).
Materials and Methods: In this randomized controlled clinical trial, 36 dental implants with KGW<2 mm were randomly assigned to 3 groups (n=12) for enhancement of KGW with FGG alone (control group), ADM alone (AlloDerm), and iPRF-impregnated ADM (AlloDerm). KGW, pain by using a visual analog scale (VAS), and graft shrinkage percentage (reduction in height and surface area of the graft) were assessed 3 months after surgery, and compared by one-way ANOVA and Sidak test (alpha=0.05).
Results: A significant increase in peri-implant KGW was observed after treatment in all three groups (P<0.001). FGG caused a significantly greater increase in KGW than the other two groups (P<0.001). Graft shrinkage was significantly lower in the FGG group than other groups (P<0.05). Postoperative pain was significantly lower in the ADM/iPRF than the FGG (P<0.001) and ADM (P=0.002) groups. Postoperative pain in the ADM group was significantly lower than that in the FGG group (P=0.008). No other significant differences were found (P>0.05).
Conclusion: All three tested methods significantly increased the peri-implant KGW. Although FGG was the most effective for the enhancement of KGW, it was associated with the highest postoperative pain level. IPRF-impregnated ADM may be considered as an acceptable, less invasive, and less painful approach for patients not consenting to FGG, although it had no significant difference with ADM alone.
Keywords: Acellular Dermis; Alloderm; Dental Implants; Platelet-Rich Fibrin
Materials and Methods: In this randomized controlled clinical trial, 36 dental implants with KGW<2 mm were randomly assigned to 3 groups (n=12) for enhancement of KGW with FGG alone (control group), ADM alone (AlloDerm), and iPRF-impregnated ADM (AlloDerm). KGW, pain by using a visual analog scale (VAS), and graft shrinkage percentage (reduction in height and surface area of the graft) were assessed 3 months after surgery, and compared by one-way ANOVA and Sidak test (alpha=0.05).
Results: A significant increase in peri-implant KGW was observed after treatment in all three groups (P<0.001). FGG caused a significantly greater increase in KGW than the other two groups (P<0.001). Graft shrinkage was significantly lower in the FGG group than other groups (P<0.05). Postoperative pain was significantly lower in the ADM/iPRF than the FGG (P<0.001) and ADM (P=0.002) groups. Postoperative pain in the ADM group was significantly lower than that in the FGG group (P=0.008). No other significant differences were found (P>0.05).
Conclusion: All three tested methods significantly increased the peri-implant KGW. Although FGG was the most effective for the enhancement of KGW, it was associated with the highest postoperative pain level. IPRF-impregnated ADM may be considered as an acceptable, less invasive, and less painful approach for patients not consenting to FGG, although it had no significant difference with ADM alone.
Keywords: Acellular Dermis; Alloderm; Dental Implants; Platelet-Rich Fibrin
Introduction
Keratinized gingiva extends from the gingival margin to the mucogingival junction, and encompasses both the attached and free gingiva [1]. After tooth extraction, significant changes occur in the soft and hard tissues that decrease the keratinized gingiva width (KGW) [2,3]. Keratinized gingiva has been shown to resist mechanical damage to oral soft tissues and reduce the incidence of gingivitis around dental implants. Therefore, success of dental implants depends not only on the bone integrity, but also on integration of the surrounding soft tissue [4]. KGW around dental implants may be considered as a fundamental aspect of the peri-implant soft tissue status [4,5].
Greater KGW is associated with healthier supporting tissues, less bone loss, and lower rate of inflammation. Studies also show that KGW is associated with various immunological factors [3,6]. Thus, when reduced KGW coincides with pathological changes in the peri-implant mucosa, surgical interventions aimed at increasing the peri-implant KGW should be considered [7]. It has been shown that keratinized tissue enhancement at implant sites with deficient or decreased KGW results in significant improvements in mucosal and plaque indices, as well as more stable marginal bone levels compared to non-augmented sites [8].
KGW augmentation can be performed at different stages of implant treatment, including before implant surgery, during implant surgery, during the second-stage surgical phase, or after implant loading. The first three stages of soft tissue augmentation have shown promising clinical results. However, the second stage is associated with risks of peri-implant infections and graft failure [9]. A new era in keratinized tissue augmentation began with the use of apically-positioned flap (APF). However, contraction can be reduced by adding an autograft rather than using APF alone [10]. Hence, APF often serves as a recipient substrate for autologous soft tissue [11,12].
APF, along with an autologous free gingival graft (FGG) harvested from the palatal mucosa, is considered the gold standard due to its optimal clinical efficacy and predictability [13]. Although this technique shows a high degree of predictability in achieving a satisfactory outcome, it has certain disadvantages, such as the need for additional surgical site preparation at the donor site, limited availability of donor tissue, and creation of a significant wound at the donor site of the palate that heals secondarily and causes postoperative pain. Similarly, at the recipient site, FGG may be associated with cosmetic problems due to color and texture differences between the healed graft and the surrounding mucosa, as well as a bulky appearance. These disadvantages of FGG prompted researchers to seek a better alternative to gingival grafting [14,15].
Acellular dermal matrix (ADM) allograft was recently introduced in periodontics as an alternative to FGG to increase KGW around teeth and implants [16], and also for treatment of gingival recession [17]. Although there is research on the use of ADM allografts around natural teeth [18,19], there are very few studies demonstrating the effectiveness of ADM in reinforcing keratinized mucosa around dental implants [20,21].
The use of platelet concentrates has gained popularity in regenerative dentistry due to their ability to accelerate healing by promoting neovascularization. Platelet-rich fibrin (PRF) forms a three-dimensional fibrin matrix that may act as a barrier membrane in guided bone and tissue regeneration procedures, and as a scaffold for tissue regeneration while simultaneously containing a number of growth factors responsible for wound healing [22]. Recent advances in tissue engineering led to the development of new PRF formulations such as injectable PRF (iPRF) aiming to increase the growth factor concentration, and offering superior regenerative potential compared to the conventional PRF [23]. IPRF contains various growth factors such as transforming growth factor-β1 (TGF-β1), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF), which contribute to cell proliferation, migration, and vascularization required for tissue regeneration [22].
Considering the importance of presence of sufficient keratinized mucosa around dental implants, and the need for methods with high efficacy and fewer complications, the present study was designed to compare iPRF-impregnated ADM. iPRF-free ADM, and FGG for enhancement of peri-implant KGW.
Materials and Methods
Greater KGW is associated with healthier supporting tissues, less bone loss, and lower rate of inflammation. Studies also show that KGW is associated with various immunological factors [3,6]. Thus, when reduced KGW coincides with pathological changes in the peri-implant mucosa, surgical interventions aimed at increasing the peri-implant KGW should be considered [7]. It has been shown that keratinized tissue enhancement at implant sites with deficient or decreased KGW results in significant improvements in mucosal and plaque indices, as well as more stable marginal bone levels compared to non-augmented sites [8].
KGW augmentation can be performed at different stages of implant treatment, including before implant surgery, during implant surgery, during the second-stage surgical phase, or after implant loading. The first three stages of soft tissue augmentation have shown promising clinical results. However, the second stage is associated with risks of peri-implant infections and graft failure [9]. A new era in keratinized tissue augmentation began with the use of apically-positioned flap (APF). However, contraction can be reduced by adding an autograft rather than using APF alone [10]. Hence, APF often serves as a recipient substrate for autologous soft tissue [11,12].
APF, along with an autologous free gingival graft (FGG) harvested from the palatal mucosa, is considered the gold standard due to its optimal clinical efficacy and predictability [13]. Although this technique shows a high degree of predictability in achieving a satisfactory outcome, it has certain disadvantages, such as the need for additional surgical site preparation at the donor site, limited availability of donor tissue, and creation of a significant wound at the donor site of the palate that heals secondarily and causes postoperative pain. Similarly, at the recipient site, FGG may be associated with cosmetic problems due to color and texture differences between the healed graft and the surrounding mucosa, as well as a bulky appearance. These disadvantages of FGG prompted researchers to seek a better alternative to gingival grafting [14,15].
Acellular dermal matrix (ADM) allograft was recently introduced in periodontics as an alternative to FGG to increase KGW around teeth and implants [16], and also for treatment of gingival recession [17]. Although there is research on the use of ADM allografts around natural teeth [18,19], there are very few studies demonstrating the effectiveness of ADM in reinforcing keratinized mucosa around dental implants [20,21].
The use of platelet concentrates has gained popularity in regenerative dentistry due to their ability to accelerate healing by promoting neovascularization. Platelet-rich fibrin (PRF) forms a three-dimensional fibrin matrix that may act as a barrier membrane in guided bone and tissue regeneration procedures, and as a scaffold for tissue regeneration while simultaneously containing a number of growth factors responsible for wound healing [22]. Recent advances in tissue engineering led to the development of new PRF formulations such as injectable PRF (iPRF) aiming to increase the growth factor concentration, and offering superior regenerative potential compared to the conventional PRF [23]. IPRF contains various growth factors such as transforming growth factor-β1 (TGF-β1), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF), which contribute to cell proliferation, migration, and vascularization required for tissue regeneration [22].
Considering the importance of presence of sufficient keratinized mucosa around dental implants, and the need for methods with high efficacy and fewer complications, the present study was designed to compare iPRF-impregnated ADM. iPRF-free ADM, and FGG for enhancement of peri-implant KGW.
Materials and Methods
This study was conducted at the Periodontics Department of Kerman University of Medical Sciences in 2024. It was approved by the ethics committee of the university (IR.KMU.REC.1403.238) and registered in the Iranian Registry of Clinical Trials (IRCT20101204005305N22).
Trial design:
A randomized controlled clinical trial with three parallel arms was designed in which the two experimental groups received either PRF-free or PRF-impregnated ADM while the control group received FGG for peri-implant KGW enhancement. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings
The inclusion criteria were age over 18 years, KGW < 2 mm, clinical peri-implant tissue health, plaque index < 20%, and optimal general health status.
The exclusion criteria were smoking > 10 cigarettes/day or alcohol consumption, systemic diseases affecting healing (such as uncontrolled diabetes mellitus), consumption of bisphosphonates, history of jaw radiotherapy, moderate to severe periodontitis, and pregnancy or nursing.
The sample consisted of 36 patients presenting to the Periodontics Department for dental implant treatment or follow-up, who were selected by consecutive sampling.
Interventions
Before the study onset, written informed consent was obtained from all the participants. The patients' personal and clinical information was kept confidential, and the patients were assured that they could withdraw from the study at any stage.
Preoperative assessment: It included measurement of KGW, pocket probing depth (PPD), and vestibular depth (VD). KGW (distance from the gingival margin to the mucogingival junction) and PPD were both measured at the mid-buccal area by a periodontist using a Williams probe with an accuracy of 1 mm. Attached gingival width (AGW) in the mid-buccal area was calculated by subtracting the PPD from the KGW. It should be noted that all pre- and post-surgical measurements were made by one observer (periodontist) who was blinded to the group allocations.
Preparation of iPRF: During the surgical session, a few minutes before the onset of the surgery, approximately 10 cc of blood was taken from the patient by an expert nurse, and collected in a sterile test tube specific for iPRF preparation. The tubes were centrifuged for 3 minutes at 700 rpm. The blood was divided into 3 layers. The middle layer (iPRF) was collected using a syringe, and poured into a container [22].
Surgical protocol: Initial periodontal therapy included scaling and root planing, and oral hygiene instructions. Surgery was performed only when satisfactory plaque control was achieved, and the selected surgical site was completely free of any inflammation. Preoperative disinfection included disinfecting the perioral area with 2% betadine (Behvazan Co., Rasht, Iran) and mouth rinsing with 0.2% chlorhexidine (Shahid Ghazi Pharmaceutical Co., Tabriz, Iran) for one minute. The graft bed preparation technique was the same in all 3 groups, as follows: First, local anesthesia was administered by injection of lidocaine plus 1:80,000 epinephrine (Persocaine-E®, Darou Pakhsh Pharmaceutical Co., Tehran, Iran) at the recipient site. The graft bed was prepared by making a coronal incision at the mucogingival junction (submarginal incision) while preserving the existing gingival margin, and two vertical incisions were made at 10 mm distance at both ends of the horizontal incision. A partial-thickness flap was elevated, the muscle fibers and connective tissue connections were separated, and an immobile bed was created. Next, the flap was sutured apically to the apical periosteum of the recipient site with periosteal sutures using 5-0 Vicryl thread (Supa, Tehran, Iran). After preparation, the recipient site was randomly assigned to the experimental or control group [24,25].
Control group (FGG): A FGG with 1 to 1.5 mm thickness was harvested from the hard palate, in the premolar area, at 2 mm distance from the gingival margin, with dimensions of approximately 10 x 7 mm. After graft harvesting from the palate, the donor site was pressed with a gauze. The palatal area was covered with a periodontal pack (Coe-Pak®, GC America, USA). Then, the adipose tissue and glands on the graft were removed using a No. 15 surgical scalpel. Next, the graft was placed over the recipient site and fixed with two simple sutures in the mesial and distal directions in the coronal part. For better adaptation of the graft to the recipient bed, a circumferential periosteal suture was made with 5-0 nonabsorbable nylon suture thread (Supa, Iran). Gentle pressure was applied for 3 to 5 minutes to maintain the graft in close contact with the underlying periosteum. The graft surface was covered with a periodontal pack [11].
PRF-free ADM: ADM (AlloDerm; Faravardeh Baft Iranian, Tehran, Iran) with a thickness of 1-1.8 mm and dimensions of 10 × 10 mm was prepared. For preparation, the membrane was first hydrated in 50 mL of sterile saline (Samen Co., Mashhad, Iran) for 5 minutes, then cut into pieces of approximately 7 × 10 mm, and then placed on the recipient site. The allograft was placed in such a way that the connective tissue surface faced the recipient bed, and the basement membrane surface faced outside. Graft fixation at the site was performed using the same technique as in the first group [26].
ADM + iPRF: IPRF was prepared as mentioned earlier, poured into a container, and the AlloDerm was cut into 7 x 10 mm pieces, mixed with iPRF in a container, and immersed for 5 minutes. Then, the impregnated graft was sutured and fixed at the recipient site in the same way as in the previous group [23]. The three surgical procedures performed in the study groups of FGG, ADM, and ADM+iPRF are illustrated in Figure 1a–i.
Postoperative instructions: Rinsing with 0.12% chlorhexidine mouthwash twice a day for 2 weeks was recommended. Ibuprofen (400 mg) was prescribed as needed. Amoxicillin (500 mg, three times a day, for 7 days) was prescribed to prevent infection. The sutures were removed 2 weeks, and the dressing was removed one week after surgery [24].
Postoperative measurements: Three months after surgery, all measurements were made again by the same examiner using a Williams probe. The measurements included PPD at the mid-buccal region around the dental implant, KGW (distance between the gingival margin and mucogingival junction), also at the mid-buccal, VD (from the gingival margin to the border of the mobile mucosa), number of analgesics taken after surgery, and postoperative pain score using a visual analog scale (by asking the patients).
Graft height was also measured as the difference between preoperative and postoperative KGW. Graft length was measured as the distance between the mesial and distal parts of the graft. Graft surface area was calculated by multiplying graft height and graft length, and percentage of graft shrinkage was calculated by subtracting the final surface area after surgery from the initial surface area, divided by the initial surface area, and multiplied by 100.
Outcomes (primary and secondary)
KGW was the primary outcome while PPD, VD, graft height, graft length, graft surface area, graft shrinkage, number of analgesics taken after surgery, and postoperative pain were the secondary outcomes.
Sample size calculation
The required sample size for each group was calculated to be 12 (a total of 36), assuming a study power of 80%, 5% level of significance, and minimum clinically significant difference of 1 mm in KGW between the two groups, using G*Power software.
Interim analyses and stopping guidelines
None.
Randomization
Randomization was performed by block randomization. Three blocks of 12 with letters A, B, and C, representing the three treatment groups, were generated using the random number function of Excel. Participants were assigned equally to the three groups based on the order of study enrollment and the generated pattern.
Blinding
The outcome assessor, who was a periodontist, was unaware of the type of intervention in each group (single-blind design).
Statistical analysis
Data were analyzed by SPSS version 23 (SPSS Inc., IL, USA). The KGW, PPD, graft height, graft length, graft surface area, and VD were compared among the three groups before and after treatment using mixed linear modeling. Generalized Linear Mixed Model was applied to compare AGW, postoperative pain, and number of analgesics taken among the three groups across time. The Sidak’s multiple comparisons test was applied for pairwise comparison of the groups regarding KGW, graft height, and graft surface area at each time point, and also for before-after comparisons of KGW, PPD, and graft height within each group. P<0.05 was considered statistically significant.
Results
Trial design:
A randomized controlled clinical trial with three parallel arms was designed in which the two experimental groups received either PRF-free or PRF-impregnated ADM while the control group received FGG for peri-implant KGW enhancement. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings
The inclusion criteria were age over 18 years, KGW < 2 mm, clinical peri-implant tissue health, plaque index < 20%, and optimal general health status.
The exclusion criteria were smoking > 10 cigarettes/day or alcohol consumption, systemic diseases affecting healing (such as uncontrolled diabetes mellitus), consumption of bisphosphonates, history of jaw radiotherapy, moderate to severe periodontitis, and pregnancy or nursing.
The sample consisted of 36 patients presenting to the Periodontics Department for dental implant treatment or follow-up, who were selected by consecutive sampling.
Interventions
Before the study onset, written informed consent was obtained from all the participants. The patients' personal and clinical information was kept confidential, and the patients were assured that they could withdraw from the study at any stage.
Preoperative assessment: It included measurement of KGW, pocket probing depth (PPD), and vestibular depth (VD). KGW (distance from the gingival margin to the mucogingival junction) and PPD were both measured at the mid-buccal area by a periodontist using a Williams probe with an accuracy of 1 mm. Attached gingival width (AGW) in the mid-buccal area was calculated by subtracting the PPD from the KGW. It should be noted that all pre- and post-surgical measurements were made by one observer (periodontist) who was blinded to the group allocations.
Preparation of iPRF: During the surgical session, a few minutes before the onset of the surgery, approximately 10 cc of blood was taken from the patient by an expert nurse, and collected in a sterile test tube specific for iPRF preparation. The tubes were centrifuged for 3 minutes at 700 rpm. The blood was divided into 3 layers. The middle layer (iPRF) was collected using a syringe, and poured into a container [22].
Surgical protocol: Initial periodontal therapy included scaling and root planing, and oral hygiene instructions. Surgery was performed only when satisfactory plaque control was achieved, and the selected surgical site was completely free of any inflammation. Preoperative disinfection included disinfecting the perioral area with 2% betadine (Behvazan Co., Rasht, Iran) and mouth rinsing with 0.2% chlorhexidine (Shahid Ghazi Pharmaceutical Co., Tabriz, Iran) for one minute. The graft bed preparation technique was the same in all 3 groups, as follows: First, local anesthesia was administered by injection of lidocaine plus 1:80,000 epinephrine (Persocaine-E®, Darou Pakhsh Pharmaceutical Co., Tehran, Iran) at the recipient site. The graft bed was prepared by making a coronal incision at the mucogingival junction (submarginal incision) while preserving the existing gingival margin, and two vertical incisions were made at 10 mm distance at both ends of the horizontal incision. A partial-thickness flap was elevated, the muscle fibers and connective tissue connections were separated, and an immobile bed was created. Next, the flap was sutured apically to the apical periosteum of the recipient site with periosteal sutures using 5-0 Vicryl thread (Supa, Tehran, Iran). After preparation, the recipient site was randomly assigned to the experimental or control group [24,25].
Control group (FGG): A FGG with 1 to 1.5 mm thickness was harvested from the hard palate, in the premolar area, at 2 mm distance from the gingival margin, with dimensions of approximately 10 x 7 mm. After graft harvesting from the palate, the donor site was pressed with a gauze. The palatal area was covered with a periodontal pack (Coe-Pak®, GC America, USA). Then, the adipose tissue and glands on the graft were removed using a No. 15 surgical scalpel. Next, the graft was placed over the recipient site and fixed with two simple sutures in the mesial and distal directions in the coronal part. For better adaptation of the graft to the recipient bed, a circumferential periosteal suture was made with 5-0 nonabsorbable nylon suture thread (Supa, Iran). Gentle pressure was applied for 3 to 5 minutes to maintain the graft in close contact with the underlying periosteum. The graft surface was covered with a periodontal pack [11].
PRF-free ADM: ADM (AlloDerm; Faravardeh Baft Iranian, Tehran, Iran) with a thickness of 1-1.8 mm and dimensions of 10 × 10 mm was prepared. For preparation, the membrane was first hydrated in 50 mL of sterile saline (Samen Co., Mashhad, Iran) for 5 minutes, then cut into pieces of approximately 7 × 10 mm, and then placed on the recipient site. The allograft was placed in such a way that the connective tissue surface faced the recipient bed, and the basement membrane surface faced outside. Graft fixation at the site was performed using the same technique as in the first group [26].
ADM + iPRF: IPRF was prepared as mentioned earlier, poured into a container, and the AlloDerm was cut into 7 x 10 mm pieces, mixed with iPRF in a container, and immersed for 5 minutes. Then, the impregnated graft was sutured and fixed at the recipient site in the same way as in the previous group [23]. The three surgical procedures performed in the study groups of FGG, ADM, and ADM+iPRF are illustrated in Figure 1a–i.
Postoperative instructions: Rinsing with 0.12% chlorhexidine mouthwash twice a day for 2 weeks was recommended. Ibuprofen (400 mg) was prescribed as needed. Amoxicillin (500 mg, three times a day, for 7 days) was prescribed to prevent infection. The sutures were removed 2 weeks, and the dressing was removed one week after surgery [24].
Postoperative measurements: Three months after surgery, all measurements were made again by the same examiner using a Williams probe. The measurements included PPD at the mid-buccal region around the dental implant, KGW (distance between the gingival margin and mucogingival junction), also at the mid-buccal, VD (from the gingival margin to the border of the mobile mucosa), number of analgesics taken after surgery, and postoperative pain score using a visual analog scale (by asking the patients).
Graft height was also measured as the difference between preoperative and postoperative KGW. Graft length was measured as the distance between the mesial and distal parts of the graft. Graft surface area was calculated by multiplying graft height and graft length, and percentage of graft shrinkage was calculated by subtracting the final surface area after surgery from the initial surface area, divided by the initial surface area, and multiplied by 100.
Outcomes (primary and secondary)
KGW was the primary outcome while PPD, VD, graft height, graft length, graft surface area, graft shrinkage, number of analgesics taken after surgery, and postoperative pain were the secondary outcomes.
Sample size calculation
The required sample size for each group was calculated to be 12 (a total of 36), assuming a study power of 80%, 5% level of significance, and minimum clinically significant difference of 1 mm in KGW between the two groups, using G*Power software.
Interim analyses and stopping guidelines
None.
Randomization
Randomization was performed by block randomization. Three blocks of 12 with letters A, B, and C, representing the three treatment groups, were generated using the random number function of Excel. Participants were assigned equally to the three groups based on the order of study enrollment and the generated pattern.
Blinding
The outcome assessor, who was a periodontist, was unaware of the type of intervention in each group (single-blind design).
Statistical analysis
Data were analyzed by SPSS version 23 (SPSS Inc., IL, USA). The KGW, PPD, graft height, graft length, graft surface area, and VD were compared among the three groups before and after treatment using mixed linear modeling. Generalized Linear Mixed Model was applied to compare AGW, postoperative pain, and number of analgesics taken among the three groups across time. The Sidak’s multiple comparisons test was applied for pairwise comparison of the groups regarding KGW, graft height, and graft surface area at each time point, and also for before-after comparisons of KGW, PPD, and graft height within each group. P<0.05 was considered statistically significant.
Results
Participant flow
The sample consisted of 36 patients (12 in each group). The mean age was 54.58±12.29 years in the ADM group, 54.50±9.05 years in the FGG group, and 51.08±11.92 years in the ADM/iPRF group. In terms of gender, there were 4 females (21.1%) and 8 males (47.1%) in the ADM group, 7 females (36.8%) and 5 males (29.4%) in the FGG group, and 8 females (42.1%) and 4 males (23.5%) in the ADM/iPRF group. There was no significant difference in the mean age or gender distribution among the study groups (P>0.05). The CONSORT flow diagram of patient selection and allocation is shown in Figure 2.
Harms
No patients were harmed during the study.
Subgroup analyses
Primary outcome
KGW: Table 1 shows the mean KGW in the three groups before and after treatment. The interaction effect of group and time on KGW was significant (P<0.001), indicating that the trend of change in the mean KGW of the study groups after treatment compared with baseline was not the same in the three groups. Pairwise comparisons by the Sidak test showed that the mean KGW in all three groups significantly increased after treatment (P<0.001 for all three). At baseline (before the treatment), no significant difference was observed among the three groups in KGW (P=0.908), but after the treatment, the FGG group had a significantly higher mean KGW compared to the ADM (P<0.001) and ADM/iPRF groups (P<0.001, Figure 3a).
Secondary outcomes
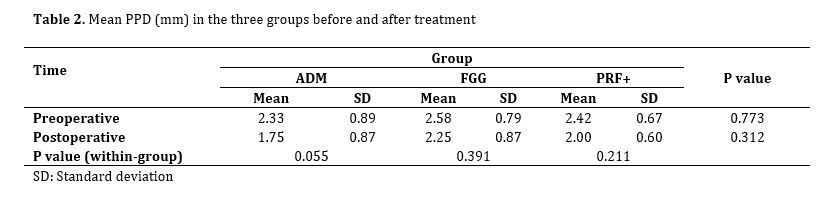
PPD: Table 2 shows the mean PPD in the three groups before and after treatment. The interaction effect of group and time was not significant on PPD (P>0.05), indicating that the trend of change in the mean PPD after treatment compared with baseline was the same in all three groups. The results also showed that the mean PPD in the three groups was not significantly different neither before nor after the treatment (P>0.05).
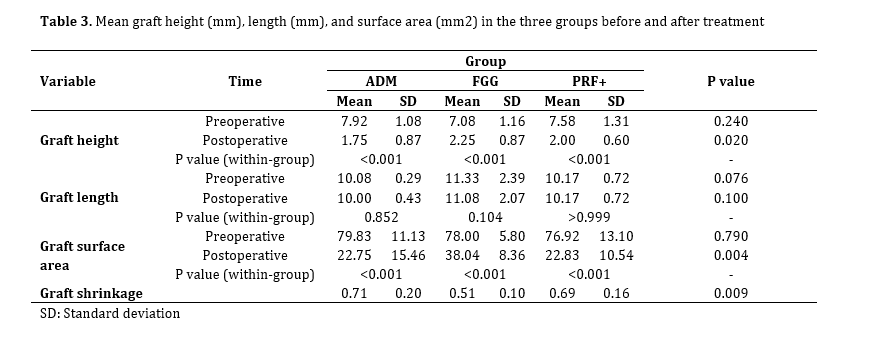
Graft height: Table 3 shows the mean graft height in the three groups before and after treatment. The interaction effect of group and time on graft height was significant (P<0.001) indicating that the trend of change in the mean graft height after treatment compared with before was not the same in the three groups. Pairwise comparisons showed that the mean graft height decreased significantly after treatment in all three groups (P<0.001 for all). Also, graft height in the FGG group was significantly higher than that in the ADM (P=0.044) and ADM/iPRF (P=0.035) groups after treatment (Figure 3b).
Graft length: Table 3 also shows the mean graft length in the three groups before and after treatment. The interaction effect of group and time was not significant (P>0.05) indicating that the trend of change in the mean graft length after treatment was the same in all three groups. The results showed that the mean graft length was not significantly different among the three groups, neither before nor after treatment (P>0.05). Also, the change in graft length was not significant in any group after treatment compared with before (P>0.05).
Graft surface area: Table 3 also shows the mean graft surface area in the three groups before and after treatment. The interaction effect of group and time on graft surface area was significant (P<0.001) indicating that the trend of change in the mean graft surface area after treatment compared with before was not the same among the three groups. Pairwise comparisons showed that the mean graft area in all three groups significantly decreased after treatment (P<0.001 in all). No significant difference was observed among the groups in this regard before treatment (P>0.05). After treatment, the graft surface area in the FGG group was significantly greater than that in the ADM (P=0.044) and ADM/iPRF (P=0.035) groups (Figure 3c).
Postoperative pain: As shown in Table 4, postoperative pain was significantly different among the three groups (P=0.005). Pairwise comparisons (Figure 3d) showed that postoperative pain was significantly lower in the ADM/iPRF than the FGG (P<0.001) and ADM (P=0.002) groups. Postoperative pain in the ADM group was also significantly lower than that in the FGG group (P=0.008).
Number of analgesics taken: As shown in Table 4, the three groups had a significant difference in the number of analgesics taken after treatment (P=0.003). Pairwise comparisons showed significantly higher number of taken analgesics in the FGG group than the ADM (P=0.028) and ADM/iPRF (P=0.003) groups (Figure 3e).
Graft shrinkage: The three groups had a significant difference in graft shrinkage (P=0.009). Pairwise comparisons showed that graft shrinkage percentage in the FGG group was significantly lower than that in the ADM (P=0.014) and ADM/iPRF (P=0.029) groups (Figure 3f).
VD: Table 4 shows the mean VD in the three groups before and after treatment. The interaction effect of group and time on VD was not significant (P>0.05), indicating that the trend of change in the mean VD after treatment compared with before was the same in all three groups. Pairwise comparisons showed that the mean VD significantly decreased after treatment in all three groups (P< 0.001, P=0.004, P=0.004). However, no significant difference was observed among the groups, neither before nor after the treatment (P>0.05).
AGW: As shown in Table 4, AGW was not significantly different among the three groups after treatment (P>0.999).
The sample consisted of 36 patients (12 in each group). The mean age was 54.58±12.29 years in the ADM group, 54.50±9.05 years in the FGG group, and 51.08±11.92 years in the ADM/iPRF group. In terms of gender, there were 4 females (21.1%) and 8 males (47.1%) in the ADM group, 7 females (36.8%) and 5 males (29.4%) in the FGG group, and 8 females (42.1%) and 4 males (23.5%) in the ADM/iPRF group. There was no significant difference in the mean age or gender distribution among the study groups (P>0.05). The CONSORT flow diagram of patient selection and allocation is shown in Figure 2.
Harms
No patients were harmed during the study.
Subgroup analyses
Primary outcome
KGW: Table 1 shows the mean KGW in the three groups before and after treatment. The interaction effect of group and time on KGW was significant (P<0.001), indicating that the trend of change in the mean KGW of the study groups after treatment compared with baseline was not the same in the three groups. Pairwise comparisons by the Sidak test showed that the mean KGW in all three groups significantly increased after treatment (P<0.001 for all three). At baseline (before the treatment), no significant difference was observed among the three groups in KGW (P=0.908), but after the treatment, the FGG group had a significantly higher mean KGW compared to the ADM (P<0.001) and ADM/iPRF groups (P<0.001, Figure 3a).
Secondary outcomes
PPD: Table 2 shows the mean PPD in the three groups before and after treatment. The interaction effect of group and time was not significant on PPD (P>0.05), indicating that the trend of change in the mean PPD after treatment compared with baseline was the same in all three groups. The results also showed that the mean PPD in the three groups was not significantly different neither before nor after the treatment (P>0.05).
Graft height: Table 3 shows the mean graft height in the three groups before and after treatment. The interaction effect of group and time on graft height was significant (P<0.001) indicating that the trend of change in the mean graft height after treatment compared with before was not the same in the three groups. Pairwise comparisons showed that the mean graft height decreased significantly after treatment in all three groups (P<0.001 for all). Also, graft height in the FGG group was significantly higher than that in the ADM (P=0.044) and ADM/iPRF (P=0.035) groups after treatment (Figure 3b).
Graft length: Table 3 also shows the mean graft length in the three groups before and after treatment. The interaction effect of group and time was not significant (P>0.05) indicating that the trend of change in the mean graft length after treatment was the same in all three groups. The results showed that the mean graft length was not significantly different among the three groups, neither before nor after treatment (P>0.05). Also, the change in graft length was not significant in any group after treatment compared with before (P>0.05).
Graft surface area: Table 3 also shows the mean graft surface area in the three groups before and after treatment. The interaction effect of group and time on graft surface area was significant (P<0.001) indicating that the trend of change in the mean graft surface area after treatment compared with before was not the same among the three groups. Pairwise comparisons showed that the mean graft area in all three groups significantly decreased after treatment (P<0.001 in all). No significant difference was observed among the groups in this regard before treatment (P>0.05). After treatment, the graft surface area in the FGG group was significantly greater than that in the ADM (P=0.044) and ADM/iPRF (P=0.035) groups (Figure 3c).
Postoperative pain: As shown in Table 4, postoperative pain was significantly different among the three groups (P=0.005). Pairwise comparisons (Figure 3d) showed that postoperative pain was significantly lower in the ADM/iPRF than the FGG (P<0.001) and ADM (P=0.002) groups. Postoperative pain in the ADM group was also significantly lower than that in the FGG group (P=0.008).
Number of analgesics taken: As shown in Table 4, the three groups had a significant difference in the number of analgesics taken after treatment (P=0.003). Pairwise comparisons showed significantly higher number of taken analgesics in the FGG group than the ADM (P=0.028) and ADM/iPRF (P=0.003) groups (Figure 3e).
Graft shrinkage: The three groups had a significant difference in graft shrinkage (P=0.009). Pairwise comparisons showed that graft shrinkage percentage in the FGG group was significantly lower than that in the ADM (P=0.014) and ADM/iPRF (P=0.029) groups (Figure 3f).
VD: Table 4 shows the mean VD in the three groups before and after treatment. The interaction effect of group and time on VD was not significant (P>0.05), indicating that the trend of change in the mean VD after treatment compared with before was the same in all three groups. Pairwise comparisons showed that the mean VD significantly decreased after treatment in all three groups (P< 0.001, P=0.004, P=0.004). However, no significant difference was observed among the groups, neither before nor after the treatment (P>0.05).
AGW: As shown in Table 4, AGW was not significantly different among the three groups after treatment (P>0.999).
Table 1. Mean KGW (mm) in the three groups before and after treatment
{kind=link}
Table 2. Mean PPD (mm) in the three groups before and after treatment
{kind=link}
Table 3. Mean graft height (mm), length (mm), and surface area (mm2) in the three groups before and after treatment
{kind=link}
Table 4. Mean VD (mm), AGW (mm), pain and number of analgesics in the three groups before and after treatment
{kind=link}
Figure 1. Clinical photographs illustrating three different surgical approaches for increasing peri-implant keratinized gingiva width.
{kind=link}
Discussion
The present study compared iPRF-impregnated ADM, iPRF-free ADM, and FGG for enhancement of peri-implant KGW. The results showed a significant increase in KGW in all three groups 3 months after treatment. The gain in KGW was 2.16 mm in the ADM, 3.5 mm in the FGG, and 2.19 mm in the ADM/iPRF group.
Ramanauskaite et al. [27] compared three-dimensional changes of porcine-derived collagen matrix and FGG for increasing the KGW around dental implants over a 6-month period and concluded that FGG produced a wider keratinized band compared to the collagen matrix. Basegmez et al. [28] conducted a clinical trial comparing the effectiveness of ADM versus FGG for augmentation of peri-implant keratinized gingiva, and showed that although ADM allografts were able to increase peri-implant KGW, FGGs appeared to be more effective, which was in line with the present findings. Also, Han et al. [29] evaluated the changes in KGW in molar areas after FGG before implant placement and showed its favorable results, such that KGW increased by 2.9 mm, which was less than that in the present study (3.5 mm in the FGG group). Park [20] investigated the clinical effectiveness of ADM to increase peri-implant keratinized mucosa and reported that peri-implant KGW increased by an average of 2.4 mm over 3 months, which was slightly greater than the value obtained in the present study. It seems that the synergy of three factors namely heterogeneity of surgical techniques in soft tissue manipulation, variability in the host biological response to residual antigens in ADM, and finally differences in postoperative protocols might be responsible for the difference in the results between the current study and previous investigations.
PRF induces new angiogenesis, accelerates wound closure, and speeds up cicatricial tissue remodeling. Since PRF is produced without using any additives, fibrin polymerization occurs in a physiological manner, resulting in a fibrin network similar to that formed during natural healing. However, in the present study, we expected the PRF to improve KGW more than other products, but this trend was not observed.
Also, the findings of the current study indicated a significant decrease in graft height after treatment in all three groups, and the mixed linear model confirmed a significant interaction between group and time. These findings indicate that the treatment results differed depending on the method used. It is noteworthy that the FGG group showed a greater graft height after treatment than the other groups. Also, the results showed that the mean graft length in the three groups did not differ significantly after treatment compared with before. These two factors were used to measure the changes in the graft surface area in the three groups, and the results indicated that the graft surface area decreased significantly after treatment in all groups. Also, FGG showed a larger graft surface area than the other groups after treatment. In the present study, the purpose of measuring the graft surface area was to evaluate the percentage of graft shrinkage, which was reported to be 52.55% ± 11.23% in the FGG group, lower than the value in the other two groups. Excessive shrinkage is one of the problems that may limit the use of ADM [18]. Agarwal et al. [30] compared FGG and AlloDerm® in increasing the KGW in a clinical study. They indicated that KGW significantly increased after both treatments, but this increase was relatively less in the ADM allograft group. The ADM site had significantly more shrinkage (76.6%) than the FGG site (49.7%), which was consistent with the present study.
Also, in another study, the efficacy of ADM allograft was clinically evaluated to increase AGW. The results showed that ADM allograft was less effective and predictable than FGG for this purpose due to significant shrinkage and unstable quality of the obtained attached gingiva, but the cosmetic results with ADM allograft were better than those with FGG [18]. Lorenzo et al. [14] used a type of ADM for soft tissue augmentation around dental implants and achieved a 2.9 mm increase in KGW after 6 months, which was comparable to the 2.8 mm increase in the control group (connective tissue graft), and the mean shrinkage of ADM was about 60%, which was in line with the present study.
Temmerman et al. [31] evaluated the efficacy of PRF for the enhancement of KGW around dental implants. They examined the percentage of shrinkage and concluded that the shrinkage rate after 6 weeks was 32.1% in the PRF group and 23.6% in the control group (FGG). However, this difference was not statistically significant. A systematic review conducted by Giammarinaro et al. [32] on whether PRF improves soft tissue outcomes around implants showed the superiority of FGG to PRF, which was consistent with the present results. Autogenous grafts have better dimensional stability than acellular dermal matrices due to their inherent biological properties and vascularization potential. Lower shrinkage of the FGG is also consistent with the well-known clinical phenomenon that autogenous tissues retain their volume better during the healing process, while AlloDerm undergoes greater resorption and deformation. However, despite the favorable shrinkage rate, the use of FGG is associated with more patient complications, including discomfort at the graft site and prolonged healing, which may limit its widespread use.
In the present study, the mean PPD was not significantly different among the three groups. This was in line with the results of Zheng et al. [33], who evaluated the clinical outcomes and soft tissue changes after implant treatment in groups with and without FGG. They demonstrated no significant difference in PPD between the FGG and the control groups. Also, Papi et al. [34] investigated the clinical changes in mucosal thickness after treatment with ADM, and reported that the mean recorded PPD did not increase significantly, which was also similar to the present study.
Pain is an important patient-reported criterion that determines the quality of patient's surgical experience. The present results showed that patients treated with ADM/iPRF experienced significantly lower postoperative pain than patients who received FGG as the standard treatment or ADM alone. This finding highlights the potential benefit of combining PRF with ADM in reducing postoperative discomfort in periodontal grafts or oral surgeries. This finding was consistent with the existing literature on the biological properties of PRF. PRF is initially composed of fibrinogen and thrombin, which are gradually converted to fibrin and form a blood clot after approximately 15 minutes. The fibrin network contains a large number of platelets and leukocytes, which secrete high concentrations of growth factors, including PDGF, insulin-like growth factor-1, VEGF, and TGF-β1, for up to 10 days [35].
IPRF enhances the migration, proliferation, and expansion of gingival fibroblasts, as well as the expression of messenger RNA of genes involved in regeneration (PDGF, TGF-β1, and collagen 1). Thus, PRF acts as a reservoir with long-term secretion of growth factors (PDGF, TGF-β, VEGF) and cytokines that actively modulate inflammation, promote angiogenesis, and accelerate soft tissue healing [36].
Gupta and Agarwal [37] evaluated the effect of advanced PRF compared to natural healing on extraction sockets and assessed pain, edema, and soft tissue healing. They showed that there was a significant reduction in pain and improvement of soft tissue healing at PRF-treated sites compared to control sites on days 3 and 7 after tooth extraction, which was attributed to the anti-inflammatory properties of PRF, which releases growth factors and enhances wound healing. Also, Yang et al. [38] evaluated the clinical and biochemical outcomes after mandibular third molar extraction surgery using ALB-PRF on one side and PRF on the other. They measured pain, socket closure, infection, and swelling. Their results showed that both PRFs effectively reduced postoperative pain. Fu et al. [39] compared patient-reported and clinical outcomes after augmentation with xenogeneic collagen matrix or FGG at different postoperative stages. Their results showed that FGG was associated with greater intensity and duration of pain after augmentation of keratinized gingiva in the early stages of healing compared with xenogeneic collagen matrix. These findings may allow surgeons to better inform patients about postoperative pain for better decision-making [38].
Also, in the present study, the pain intensity in the FGG group was significantly higher than that in ADM alone. In a systematic review, Thoma et al. [40] examined patient-reported outcomes after soft tissue augmentation in dental implants. They reported a significant reduction in pain after soft tissue augmentation with ADM compared with autologous FGG. The authors attributed this to lack of a donor site, as harvesting soft tissue grafts from the palate leads to excessive bleeding, numbness, and other complications such as tissue necrosis, which increase pain. Agarwal et al. [30] in their clinical study compared FGG and AlloDerm®, and concluded that ADM had minimal postoperative pain, with no adverse effects, compared to FGG for gingival augmentation procedures.
However, Harris [19] compared ADM, FGG, and subepithelial connective tissue grafts and reported no difference in pain scores between patients treated with ADM or FGG, which was in contrast to the current results. Differences in pain score can be explained by the healing process of mucosal wounds. At the recipient site, the initial healing phase, up to 3 days, involves the survival of the graft tissue through plasma circulation from the recipient bed. However, in the FGG group, the higher pain level during the initial phase can be attributed to the healing process at the donor site proceeding with secondary intention. Therefore, specific measures to minimize the patient's postoperative pain perception are necessary to increase patient tolerance to soft tissue grafting procedures.
It is worth noting that some limitations should be considered. The specific surgical procedure, demographic characteristics of patients, and the exact time points of pain assessment require explicit description to fully understand the findings. In addition, the exact mechanism of pain reduction in the ADM/iPRF group compared to FGG, whether it is the elimination of graft site problems, the improvement of recipient site healing by PRF, or a combination of both, requires further investigation. Future studies will provide deeper insights by employing standardized pain assessment tools at specific time intervals, histological analysis of the healing site, and comparison with other methods such as connective tissue grafts combined with PRF. Nevertheless, these findings provide valuable clinical evidence supporting PRF+ADM as a promising strategy to reduce postoperative pain burden compared with conventional FGG techniques, which could lead to increased patient comfort and improved adherence to postoperative care protocols.
The present findings indicated a statistically significant difference in postoperative analgesic consumption among the three groups. Analgesic consumption in the FGG group was significantly higher than that in both the ADM and PRF+ADM groups. This observation is consistent with the data on postoperative pain in the present study and the existing evidence of higher morbidity with FGG-based procedures. The higher analgesic consumption in the FGG group can be directly attributed to problems with the palatal graft site. Secondary ulceration in the palatal region is a known source of significant pain and requires stronger pharmacological management. In contrast, lower analgesic requirement in the PRF+ADM group is likely due to the intrinsic anti-inflammatory and analgesic effects of PRF. PRF reduces the need for analgesics by modulating the secretion of proinflammatory cytokines (such as IL-6 and tumor necrosis factor-α) and increasing the secretion of anti-inflammatory interleukin-10.
Of note, there was no statistically significant difference in analgesic consumption between the ADM and PRF+ADM groups in this study. This finding suggests that elimination of the secondary graft site (which was achieved in both the ADM and PRF+ADM groups) is a key factor in reducing the need for analgesics compared to FGG, as the need for a second surgery can lead to postoperative pain and increased patient discomfort. Despite the importance of these findings, there are limitations, including lack of accurate recording of analgesic consumption by patients based on standard prescription of 400 mg ibuprofen, and lack of monitoring of analgesic consumption over short time periods (e.g., 24, 48, and 72 hours). Also, the impact of individual variables, such as patients' pain perception threshold on analgesic consumption was not assessed. However, the present objective data on higher analgesic consumption in the FGG group provide strong evidence that this method has a higher drug burden than ADM-based techniques (alone or augmented with PRF). The reduction in the need for analgesics not only indicates improved patient comfort but also may reduce the risk of drug side effects and treatment costs. Future studies could contribute to a more comprehensive understanding of this important aspect of postoperative care by designing standardized protocols for more accurate quantitative monitoring of medication consumption and considering psychological variables affecting pain perception.
Conclusion
All three tested methods significantly increased the peri-implant KGW. Although FGG was the most effective for enhancement of KGW, it was associated with the highest postoperative pain level. IPRF-impregnated ADM may be considered as an acceptable, less invasive, and less painful approach for patients not consenting to FGG, although it had no significant difference with ADM alone.
Type of Study: Original article |
Subject:
Periodontology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |