Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 4 (12-2025)
J Res Dent Maxillofac Sci 2025, 10(4): 346-352 |
Back to browse issues page


Ethics code: Not applicable.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sharifzadeh S S, Mardani M, Motazedian J, Jamalpour M, Shirvani Farsani F, Entezar-e-Ghaem M et al . An Exceptionally Rare Case of Craniofacial Teratoma in A 2-Day-Old Infant: A Case Report. J Res Dent Maxillofac Sci 2025; 10 (4) :346-352
URL: http://jrdms.dentaliau.ac.ir/article-1-1115-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-1115-en.html
Seyedeh saba Sharifzadeh1 

 , Mohesen Mardani2 , Jamaledin Motazedian3 , Mahdi Jamalpour4 , Fatemeh Shirvani Farsani5 , Mahjoubeh Entezar-e-Ghaem6 , Niloofar Ghadimi *7
, Mohesen Mardani2 , Jamaledin Motazedian3 , Mahdi Jamalpour4 , Fatemeh Shirvani Farsani5 , Mahjoubeh Entezar-e-Ghaem6 , Niloofar Ghadimi *7
, Mohesen Mardani2 , Jamaledin Motazedian3 , Mahdi Jamalpour4 , Fatemeh Shirvani Farsani5 , Mahjoubeh Entezar-e-Ghaem6 , Niloofar Ghadimi *7
1- Department of Oral Medicine, TeMS.C., Islamic Azad University, Tehran, Iran
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran
3- Department of Oral and Maxillofacial Surgery, Shiraz University of Medical Sciences, Shiraz, Iran
4- Department of Pathology, Shiraz University of Medical Sciences, Shiraz, Iran
5- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Hamedan University of Medical Sciences, Hamedan, Iran
6- Department of Oral and Maxillofacial Radiology, School of Dentistry, Shahid Sadoughi, Yazd, Iran
7- Department of Oral and Maxillofacial Radiology, Medical Dental Material Research Center. Dental School, TeMS.C., Islamic Azad University, Tehran, Iran ,omfrghadimi@gmail.com
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran
3- Department of Oral and Maxillofacial Surgery, Shiraz University of Medical Sciences, Shiraz, Iran
4- Department of Pathology, Shiraz University of Medical Sciences, Shiraz, Iran
5- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Hamedan University of Medical Sciences, Hamedan, Iran
6- Department of Oral and Maxillofacial Radiology, School of Dentistry, Shahid Sadoughi, Yazd, Iran
7- Department of Oral and Maxillofacial Radiology, Medical Dental Material Research Center. Dental School, TeMS.C., Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 506 kb]
(369 Downloads)
| Abstract (HTML) (1200 Views)
Full-Text: (336 Views)
Abstract
Background and Aim: Craniofacial teratomas are exceedingly rare congenital tumors, typically presenting at birth with variable degrees of facial distortion and airway compromise.
Case Presentation: We report a rare case of a 2-day-old female neonate with a massive craniofacial teratoma affecting her left facial region, accompanied by a cleft palate and feeding difficulties. Computed tomography (CT) imaging revealed a large heterogeneous mass with destructive extension into the orbit, maxilla, mandible, and anterior and middle cranial fossae. Complete surgical excision was achieved via the Weber-Ferguson approach, and histopathological evaluation confirmed a mature teratoma.
Conclusion: This case report highlights the importance of early imaging and prompt surgical intervention in managing large craniofacial teratomas. Despite the rarity of such cases, multidisciplinary planning is essential to achieve optimal functional and cosmetic outcomes.
Keywords: Congenital; Craniofacial Abnormalities; Surgery; Teratoma
Introduction
Case Presentation: We report a rare case of a 2-day-old female neonate with a massive craniofacial teratoma affecting her left facial region, accompanied by a cleft palate and feeding difficulties. Computed tomography (CT) imaging revealed a large heterogeneous mass with destructive extension into the orbit, maxilla, mandible, and anterior and middle cranial fossae. Complete surgical excision was achieved via the Weber-Ferguson approach, and histopathological evaluation confirmed a mature teratoma.
Conclusion: This case report highlights the importance of early imaging and prompt surgical intervention in managing large craniofacial teratomas. Despite the rarity of such cases, multidisciplinary planning is essential to achieve optimal functional and cosmetic outcomes.
Keywords: Congenital; Craniofacial Abnormalities; Surgery; Teratoma
Introduction
Teratomas are germ cell tumors composed of tissues derived from more than one embryonic germ layer, which can manifest in a variety of anatomical locations. The most common sites are the sacrococcygeal region, ovaries, and testes. Craniofacial teratomas, however, represent an extremely rare subset, accounting for less than 5% of all teratomas, and are more frequently observed in females [1]. These tumors may manifest at birth with varying degrees of facial asymmetry and can be associated with congenital anomalies such as cleft lip and palate, bifid tongue, and mandibular hypoplasia [2]. Because of their complex anatomical location, they can exert pressure on vital structures, leading to airway obstruction, feeding difficulties, and significant esthetic concerns. Recent advances in prenatal ultrasonography and fetal magnetic resonance imaging (MRI) have allowed earlier detection of teratomas, often in the third trimester, enabling planned delivery and immediate airway management strategies such as the ex-utero intrapartum treatment (EXIT) procedure [3]. Postnatal imaging, especially contrast-enhanced computed tomography (CT) and MRI, is essential in delineating the full extent of the lesion, evaluating its intracranial extension, and planning a surgical intervention [4].
While mature teratomas are histologically benign, their size, growth pattern, and involvement of adjacent critical structures necessitate prompt and comprehensive management. Histologically, mature teratomas are composed of well-differentiated elements from ectodermal, mesodermal, and endodermal origins, and are rarely associated with malignant transformation [5]. Despite their benign nature, they require surgical excision to prevent complications such as airway compromise, infection, and functional deficits. Complete resection remains the definitive treatment, and early intervention improves both survival and cosmetic outcomes [1].
This report presents a rare case of a massive facial teratoma in a 2-day-old neonate, associated with a cleft palate and significant anatomical disruption. We detail the clinical presentation, radiographic findings, surgical approach, and histopathological confirmation of a mature teratoma. This case underscores the importance of multidisciplinary coordination and individualized surgical planning in managing these complex congenital tumors.
Case Presentation
While mature teratomas are histologically benign, their size, growth pattern, and involvement of adjacent critical structures necessitate prompt and comprehensive management. Histologically, mature teratomas are composed of well-differentiated elements from ectodermal, mesodermal, and endodermal origins, and are rarely associated with malignant transformation [5]. Despite their benign nature, they require surgical excision to prevent complications such as airway compromise, infection, and functional deficits. Complete resection remains the definitive treatment, and early intervention improves both survival and cosmetic outcomes [1].
This report presents a rare case of a massive facial teratoma in a 2-day-old neonate, associated with a cleft palate and significant anatomical disruption. We detail the clinical presentation, radiographic findings, surgical approach, and histopathological confirmation of a mature teratoma. This case underscores the importance of multidisciplinary coordination and individualized surgical planning in managing these complex congenital tumors.
Case Presentation
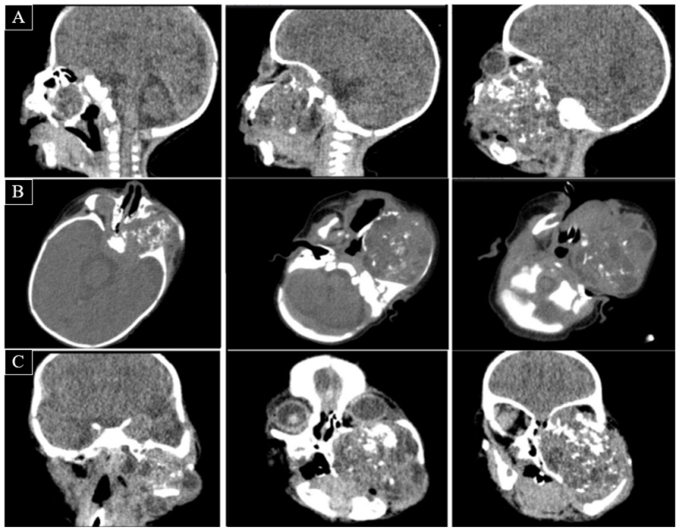
A 2-day-old female infant was brought to the Neonatal Intensive Care Unit of Namazee Hospital in Shiraz in July 2024 with the chief complaint of lateral facial swelling since birth through a cesarean section. Clinical examination revealed a large mass on the left side of her face, with a cleft in the palatal region, causing poor sucking ability. The overlying skin was normal with no neurological deficit. The CT scan revealed a giant heterogeneous mass, predominantly occupying the left side of the face, characterized by extensive expansion and destruction of adjacent structures, including the mandible, maxilla, and nasal cavity, and invasion to the orbital region, leading to displacement and compression of the eye globe. Bony erosion was severe with near-complete obliteration of normal maxillofacial architecture on the affected side. The mass showed posterior and superior extension, and evidence of invasion into the cranial fossa (anterior and middle). Airway compromise was also noted due to the effect of mass on the nasopharyngeal and oropharyngeal spaces (Figure 1).
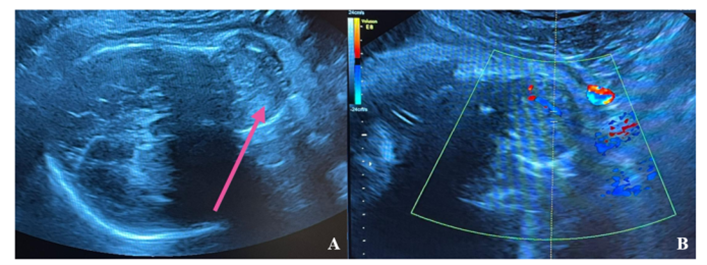
According to the parents, in ultrasonography of the fetus in the third trimester, a lobulated heterogeneous mass with some calcific foci and mild to moderate internal vascularity on color Doppler had been seen in the left part of the anterior cranial region (Figure 2).
Routine blood tests were normal, and an excisional biopsy was done by using a left Weber-Ferguson incision; a mucocutaneous flap was reflected, and the pathological lesion in the left side of the maxilla was exposed, explored, excised, and sent for histopathological analysis. After copious irrigation, a tetracycline mesh was inserted, and then the flap was repositioned and sutured in one layer with 4-0 Vicryl and 5-0 nylon sutures. A sterile dressing was then applied. After 2 days, the left maxillary sinus mesh was removed, and the area was sutured with 3-0 Vicryl sutures in a single layer (Figure 3).
Figure 1. CT scan images demonstrating a large, destructive facial mass with extensive involvement of adjacent structures: (A) sagittal, (B) axial, and (C) coronal views
Figure 2. Ultrasonography of the patient, exhibiting a heterogeneous mass with some calcific foci (A) and mild to moderate internal vascularity on color Doppler (B)
Figure 3. (A and B) Clinical view of the neonate with a lateral facial swelling; (C) a Weber-Ferguson incision; (D) teratoma; (E) mass removal; (F) flap was repositioned and sutured
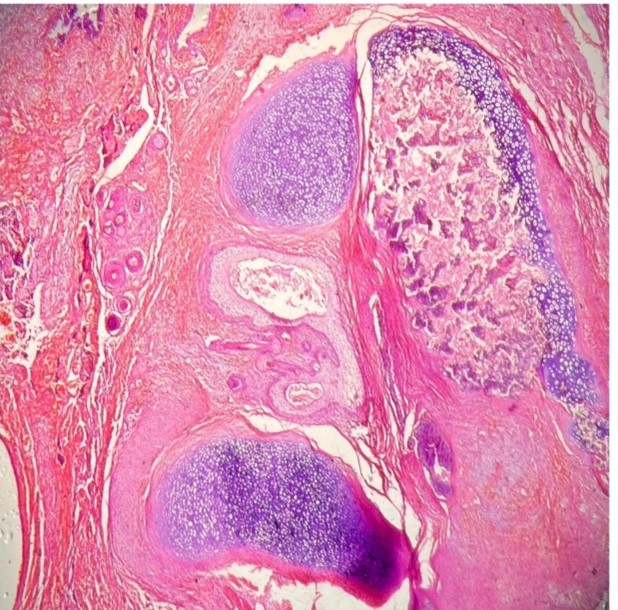
In histopathological analysis, the tumor showed a mixture of mature benign tissues, including ectodermal components like squamous epithelium and hair follicles. The mesodermal components included numerous foci of cartilage, bone, and intestinal epithelium. No foci of immature neuroepithelial tissue were identified in the serially sectioned specimen. This microscopic evidence was in favor of mature
Figure 4. Microscopic view of the mass: foci of mature cartilage, and intra-cartilaginous bone formation (H and E staining; × 40 magnification)
Discussion
According to the parents, in ultrasonography of the fetus in the third trimester, a lobulated heterogeneous mass with some calcific foci and mild to moderate internal vascularity on color Doppler had been seen in the left part of the anterior cranial region (Figure 2).
Routine blood tests were normal, and an excisional biopsy was done by using a left Weber-Ferguson incision; a mucocutaneous flap was reflected, and the pathological lesion in the left side of the maxilla was exposed, explored, excised, and sent for histopathological analysis. After copious irrigation, a tetracycline mesh was inserted, and then the flap was repositioned and sutured in one layer with 4-0 Vicryl and 5-0 nylon sutures. A sterile dressing was then applied. After 2 days, the left maxillary sinus mesh was removed, and the area was sutured with 3-0 Vicryl sutures in a single layer (Figure 3).
Figure 1. CT scan images demonstrating a large, destructive facial mass with extensive involvement of adjacent structures: (A) sagittal, (B) axial, and (C) coronal views
{kind=link}
Figure 2. Ultrasonography of the patient, exhibiting a heterogeneous mass with some calcific foci (A) and mild to moderate internal vascularity on color Doppler (B)
{kind=link}
Figure 3. (A and B) Clinical view of the neonate with a lateral facial swelling; (C) a Weber-Ferguson incision; (D) teratoma; (E) mass removal; (F) flap was repositioned and sutured
{kind=link}
In histopathological analysis, the tumor showed a mixture of mature benign tissues, including ectodermal components like squamous epithelium and hair follicles. The mesodermal components included numerous foci of cartilage, bone, and intestinal epithelium. No foci of immature neuroepithelial tissue were identified in the serially sectioned specimen. This microscopic evidence was in favor of mature
Figure 4. Microscopic view of the mass: foci of mature cartilage, and intra-cartilaginous bone formation (H and E staining; × 40 magnification)
{kind=link}
Discussion
Craniofacial teratomas, although histologically benign in most cases, pose significant clinical challenges due to their location, potential for airway compromise, and impact on facial anatomy and development. These tumors represent a rare form of congenital neoplasm, and are estimated to constitute less than 5% of all teratomas [1,5]. Their etiology remains unclear, although they are derived from pluripotent germ cells capable of differentiating into all three embryonic germ layers of ectoderm, mesoderm, and endoderm [6]. These tumors often arise along the embryonic fusion lines, suggesting an origin from mislocalized primordial cells, such as remnants of the notochord or neural crest derivatives. Some hypotheses propose that faulty differentiation of multipotent stem cells—due to genetic or epigenetic dysregulation—leads to their uncontrolled growth and heterogeneous tissue composition. The key genes involved in maintaining pluripotency, including the SOX2, OCT4, and NANOG, may play a role, alongside chromosomal abnormalities like trisomies or structural rearrangements. While the exact mechanisms remain unclear, the convergence of embryological mispatterning and genetic instability likely drives the pathogenesis of these rare lesions [7].
In the present case, a 2-day-old neonate presented with a large mature teratoma involving multiple facial and cranial compartments. This aligns with the known clinical presentations where teratomas extend into the orbit, maxilla, and cranial base, disrupting the maxillofacial structures [2]. The CT imaging revealed destructive behavior and intracranial extension, which are commonly reported in such cases, necessitating fast surgical planning [3]. Preoperative imaging, especially contrast-enhanced CT or MRI, remains essential to assess tumor boundaries, potential vascular involvement, and critical anatomical distortions [4]. Histopathologically, the majority of craniofacial teratomas in neonates are mature, as in our case, composed of well-differentiated tissues such as cartilage, bone, and squamous epithelium. However, immature teratomas with neuroepithelial tissue elements are associated with a more aggressive clinical course and potential for recurrence or malignancy [5]. A recent report by Riazi et al. [8] described a giant high-grade immature teratoma in the central nervous system of an infant, highlighting a histopathological variant that can exist, and the importance of complete resection in guiding prognosis.
Surgical excision remains the cornerstone of management. Our approach utilized a left Weber-Ferguson incision for exposure and complete resection, which is widely accepted for extensive facial tumors. Notably, Wiedermann et al. [9] emphasized the growing utility of 3D-printed models in skull base reconstructions, aiding in surgical precision for such large, complex craniofacial teratomas. In some instances, submental flaps or other reconstructive techniques may be employed depending on tissue loss and post-excision defects. In cases where airway obstruction is anticipated, especially prenatally detected tumors, an EXIT procedure may be indicated to establish a secure airway before complete delivery. Although not needed in this case, the EXIT is increasingly utilized since the advent of reliable fetal MRI [3]. The key indications for the EXIT procedure include: 1) imaging evidence of tumor mass effect (e.g., tracheolaryngeal compression, or neck hyperextension on MRI or ultrasound), 2) polyhydramnios (suggesting impaired fetal swallowing due to obstruction), or 3) tumor size > 5 cm encroaching on the oropharynx or trachea. The EXIT strategy prioritizes airway control while maintaining uteroplacental circulation, allowing time for fetal intubation, tracheostomy, or even partial tumor resection before umbilical cord clamping [10]. Postoperative management and follow-up are essential to monitor potential recurrence. The presence of immature components is a known risk factor for recurrence [4]. However, in mature teratomas with clear surgical margins, long-term outcomes are generally favorable. A multidisciplinary approach involving pediatric surgeons, anesthetists, otolaryngologists, and pathologists is critical for comprehensive perioperative care. Genetic considerations also play a role in some craniofacial teratomas, especially when associated with syndromic anomalies [11]. Acosta-Fernández et al. [12] reported a case involving a novel EFNB1 mutation linked to craniofrontonasal syndrome, reinforcing the need for genetic consultation in cases where craniofacial teratomas coexist with midline or systemic anomalies. This case enriches the literature by contributing detailed anatomical, surgical, and histological insights into a rare mature craniofacial teratoma, and emphasizes the importance of early imaging, timely surgery, and coordinated multidisciplinary management.
Conclusion
In the present case, a 2-day-old neonate presented with a large mature teratoma involving multiple facial and cranial compartments. This aligns with the known clinical presentations where teratomas extend into the orbit, maxilla, and cranial base, disrupting the maxillofacial structures [2]. The CT imaging revealed destructive behavior and intracranial extension, which are commonly reported in such cases, necessitating fast surgical planning [3]. Preoperative imaging, especially contrast-enhanced CT or MRI, remains essential to assess tumor boundaries, potential vascular involvement, and critical anatomical distortions [4]. Histopathologically, the majority of craniofacial teratomas in neonates are mature, as in our case, composed of well-differentiated tissues such as cartilage, bone, and squamous epithelium. However, immature teratomas with neuroepithelial tissue elements are associated with a more aggressive clinical course and potential for recurrence or malignancy [5]. A recent report by Riazi et al. [8] described a giant high-grade immature teratoma in the central nervous system of an infant, highlighting a histopathological variant that can exist, and the importance of complete resection in guiding prognosis.
Surgical excision remains the cornerstone of management. Our approach utilized a left Weber-Ferguson incision for exposure and complete resection, which is widely accepted for extensive facial tumors. Notably, Wiedermann et al. [9] emphasized the growing utility of 3D-printed models in skull base reconstructions, aiding in surgical precision for such large, complex craniofacial teratomas. In some instances, submental flaps or other reconstructive techniques may be employed depending on tissue loss and post-excision defects. In cases where airway obstruction is anticipated, especially prenatally detected tumors, an EXIT procedure may be indicated to establish a secure airway before complete delivery. Although not needed in this case, the EXIT is increasingly utilized since the advent of reliable fetal MRI [3]. The key indications for the EXIT procedure include: 1) imaging evidence of tumor mass effect (e.g., tracheolaryngeal compression, or neck hyperextension on MRI or ultrasound), 2) polyhydramnios (suggesting impaired fetal swallowing due to obstruction), or 3) tumor size > 5 cm encroaching on the oropharynx or trachea. The EXIT strategy prioritizes airway control while maintaining uteroplacental circulation, allowing time for fetal intubation, tracheostomy, or even partial tumor resection before umbilical cord clamping [10]. Postoperative management and follow-up are essential to monitor potential recurrence. The presence of immature components is a known risk factor for recurrence [4]. However, in mature teratomas with clear surgical margins, long-term outcomes are generally favorable. A multidisciplinary approach involving pediatric surgeons, anesthetists, otolaryngologists, and pathologists is critical for comprehensive perioperative care. Genetic considerations also play a role in some craniofacial teratomas, especially when associated with syndromic anomalies [11]. Acosta-Fernández et al. [12] reported a case involving a novel EFNB1 mutation linked to craniofrontonasal syndrome, reinforcing the need for genetic consultation in cases where craniofacial teratomas coexist with midline or systemic anomalies. This case enriches the literature by contributing detailed anatomical, surgical, and histological insights into a rare mature craniofacial teratoma, and emphasizes the importance of early imaging, timely surgery, and coordinated multidisciplinary management.
Conclusion
Although teratomas are among the more common tumors during the infancy and childhood, craniofacial teratomas remain exceptionally rare. Accurate diagnosis relies on advanced imaging (MRI or CT) to delineate tumor extent, and guide surgical planning. Complete excision with meticulous preservation of the surrounding vital structures is critical to achieve optimal outcomes. However, successful management requires a multidisciplinary approach, involving pediatric surgeons, otolaryngologists, oral/maxillofacial specialists, anesthetists, and pathologists, to address both functional and cosmetic challenges. Long-term follow-up is essential to monitor for recurrence, ensure normal craniofacial development, and address any psychosocial or reconstructive needs. This holistic strategy maximizes not only the survival but also the quality of life of affected individuals.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate consent forms from the patient’s parents for publication of this case report.
Conflict of Interests: There is no conflict of interest to declare.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate consent forms from the patient’s parents for publication of this case report.
Conflict of Interests: There is no conflict of interest to declare.
Type of Study: Case report |
Subject:
Oral & maxillofacial surgery
References
1. Brodsky JR, Irace AL, Didas A, Watters K, Estroff JA, Barnewolt CE, et al. Teratoma of the neonatal head and neck: A 41-year experience. Int J Pediatr Otorhinolaryngol. 2017 Jun;97:66-71. [DOI:10.1016/j.ijporl.2017.02.011] [PMID]
2. Yhoshu E, Chaudhary G, Ahmed I, Gupta MK. Congenital lateral facial teratoma: A case report and review of literature. Afr J Paediatr Surg. 2021 Apr-Jun;18(2):99-103. [DOI:10.4103/ajps.AJPS_77_20] [PMID] []
3. Alexander VR, Manjaly JG, Pepper CM, Ifeacho SN, Hewitt RJ, Hartley BE. Head and neck teratomas in children--A series of 23 cases at Great Ormond Street Hospital. Int J Pediatr Otorhinolaryngol. 2015 Dec;79(12):2008-14. [DOI:10.1016/j.ijporl.2015.07.042] [PMID]
4. Dharmarajan H, Rouillard-Bazinet N, Chandy BM. Mature and immature pediatric head and neck teratomas: A 15-year review at a large tertiary center. Int J Pediatr Otorhinolaryngol. 2018 Feb;105:43-7. [DOI:10.1016/j.ijporl.2017.11.031] [PMID]
5. da Silva Freitas R, Bernert BF, Guarezi Nasser IJ, Lupion FG, Angeli-Freitas E, Grande CV. Congenital teratoma of the oral cavity - the largest personal series of cases. Oral Maxillofac Surg. 2024 Nov;29(1):13. [DOI:10.1007/s10006-024-01307-1] [PMID]
6. Fasfoos A, Amro O, Heeh S, Zighan W, Manasrah A, Bakri S, et al. Multidisciplinary management of a neonate with oropharyngeal teratoma and bilateral cleft lip and palate: a rare congenital presentation. J Surg Case Rep. 2025 May;2025(5):rjaf293. [DOI:10.1093/jscr/rjaf293] [PMID] []
7. Adachi K, Suemori H, Yasuda SY, Nakatsuji N, Kawase E. Role of SOX2 in maintaining pluripotency of human embryonic stem cells. Genes Cells. 2010 May;15(5):455-70. [DOI:10.1111/j.1365-2443.2010.01400.x] [PMID]
8. Riazi A, Larry M, Mokhtari A, Abdali H, Asfia M, Bagherieh S. Giant high-grade immature teratoma of the central nervous system (CNS) in an infant: A case report. Am J Case Rep. 2021 Dec 24;22:e932752. [DOI:10.12659/AJCR.932752] [PMID] []
9. Wiedermann JP, Joshi AS, Jamshidi A, Conchenour C, Preciado D. Utilization of a submental island flap and 3D printed model for skull base reconstruction: Infantile giant cranio-cervicofacial teratoma. Int J Pediatr Otorhinolaryngol. 2017 Jan;92:143-5.
10. Spiers A, Legendre G, Biquard F, Descamps P, Corroenne R. Ex utero intrapartum technique (EXIT): Indications, procedure methods and materno-fetal complications - A literature review. J Gynecol Obstet Hum Reprod. 2022 Jan;51(1):102252. [DOI:10.1016/j.ijporl.2016.11.014] [PMID]
10. Oommen J, Mohammed H, Ayyappan Kutty S, Mammen A, Kalathingal K, Vellani Thamunni C, et al. Neonatal teratoma: Craniofacial treatment. J Craniofac Surg. 2019 Jan;30(1):e17-9. [DOI:10.1097/SCS.0000000000004906] [PMID]
11. Acosta-Fernández E, Zenteno JC, Chacón-Camacho OF, Peña-Padilla C, Bobadilla-Morales L, Corona-Rivera A, et al. Extracranial midline defects in a patient with craniofrontonasal syndrome with a novel EFNB1 mutation. Am J Med Genet A. 2020 May;182(5):1223-9. [DOI:10.1002/ajmg.a.61506] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |