Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 2 (6-2026)
J Res Dent Maxillofac Sci 2026, 11(2): 126-135 |
Back to browse issues page
Ethics code: CDCRI/DEAN/ETHICSCOMMITTEE/STAFF/OMRD-01/2024
Clinical trials code: NA
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
R Patil S, Daniel S, Veeraraghavan V P, Padmashali Jayappa N, Manyam R, A Rao K. Exploring Lactate Dehydrogenase as a Biomarker for Early Detection and Monitoring of Oral Submucous Fibrosis: A Preliminary Study. J Res Dent Maxillofac Sci 2026; 11 (2) :126-135
URL: http://jrdms.dentaliau.ac.ir/article-1-969-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-969-en.html
Santosh R Patil1 
 , Shikhar Daniel *2 , Vishnu Priya Veeraraghavan3 , Nagarathna Padmashali Jayappa4 , Ravikanth Manyam5 , Krishna A Rao6
, Shikhar Daniel *2 , Vishnu Priya Veeraraghavan3 , Nagarathna Padmashali Jayappa4 , Ravikanth Manyam5 , Krishna A Rao6
, Shikhar Daniel *2 , Vishnu Priya Veeraraghavan3 , Nagarathna Padmashali Jayappa4 , Ravikanth Manyam5 , Krishna A Rao6
1- Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Chhattisgarh, India
2- Department of Oral Medicine and Radiology, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India ,shikhardaniel555@gmail.com
3- Centre of Molecular Medicine and Diagnostics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
4- Department of Pediatric Dentistry, Chhattisgarh Dental College and Research Institute, Chhattisgarh
5- Department of Oral Pathology, Vishnu Dental College, Bhimavaram
6- Department of Oral Pathology JSS Dental College & Hospital, Mysuru
2- Department of Oral Medicine and Radiology, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India ,
3- Centre of Molecular Medicine and Diagnostics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, Tamil Nadu, India
4- Department of Pediatric Dentistry, Chhattisgarh Dental College and Research Institute, Chhattisgarh
5- Department of Oral Pathology, Vishnu Dental College, Bhimavaram
6- Department of Oral Pathology JSS Dental College & Hospital, Mysuru
Full-Text [PDF 451 kb]
(5 Downloads)
| Abstract (HTML) (9 Views)
Full-Text: (1 Views)
Abstract
Background and Aim: This study compared the serum and salivary lactate dehydrogenase (LDH) levels in patients with oral submucous fibrosis (OSMF) and healthy controls, and assessed their potential as biomarkers for OSMF diagnosis, and monitoring its progression.
Materials and Methods: This case-control study involved 50 OSMF patients and 50 age- and sex-matched healthy controls. Serum and salivary LDH levels were measured using standard laboratory techniques. Clinical staging of OSMF was performed based on the severity of symptoms, and the relationship between LDH levels and disease stage was analyzed using statistical methods. Descriptive and inferential statistics including t-test, ANOVA, and correlation coefficients based on data distribution were used to assess the association between LDH levels and OSMF clinical features (alpha=0.05).
Results: OSMF patients showed significantly higher serum LDH levels (225.4±58.2 U/L) than healthy controls (187.6±42.4 U/L; P=0.0004). They also showed significantly higher salivary LDH levels (180.3±53.1 U/L) compared to controls (148.2±37.9 U/L; P=0.0006). A strong positive correlation was found between serum LDH levels and clinical stage of OSMF (r=0.65, P<0.001), while a moderate inverse correlation was observed between salivary LDH levels and mouth opening (r=-0.48, P<0.001).
Conclusion: Both serum and salivary LDH levels were significantly elevated in patients with OSMF compared to healthy controls. Salivary LDH, in particular, demonstrated a strong association with clinical severity and disease stage, supporting its potential as an effective, non-invasive biomarker for OSMF diagnosis, and monitoring its progression.
Keywords: Biomarkers; L-Lactate Dehydrogenase; Oral Submucous Fibrosis; Saliva
Introduction
Oral submucous fibrosis (OSMF) is a chronic and progressive condition of the oral mucosa, characterized by the formation of fibrous bands that restrict mouth opening, and cause other debilitating symptoms, such as pain, burning sensation, and difficulty in chewing [1]. The disease is primarily associated with the habitual use of areca nut, tobacco, and alcohol, although genetic and environmental factors also play a role in its development [2]. It is considered a premalignant disorder, with a potential for malignant transformation to oral squamous cell carcinoma in its advanced stages [3,4]. Early detection and accurate monitoring of OSMF progression are crucial for effective management and preventing malignancy. However, clinical diagnosis of OSMF often relies on subjective symptoms and clinical examination, which can be challenging in early stages of the disease [5].
Biomarkers have gained attention as potential diagnostic tools for OSMF, offering an objective and non-invasive means to assess disease severity and monitor progression. Among the various biomarkers, lactate dehydrogenase (LDH) has emerged as a promising candidate [6]. LDH is an enzyme involved in anaerobic metabolism, converting lactate to pyruvate in cells. Its elevated levels in the blood and saliva have been linked to various pathological conditions, including cancers and inflammatory diseases, due to its release during cell damage and metabolic stress [7]. LDH has been found to be a sensitive indicator of cellular injury and tissue damage, making it a valuable marker in diseases like OSMF, where inflammation and fibrosis are central to the pathogenesis [8]. Evidence shows that serum and salivary LDH levels are elevated in patients with OSMF, suggesting that LDH could serve as a potential biomarker for diagnosing and monitoring of the disease [6]. Serum LDH has been widely used to assess the severity of various diseases, including liver cirrhosis, myocardial infarction, and malignancies [9]. In OSMF, the increased LDH levels may correlate with the degree of fibrosis, tissue remodeling, and inflammation that occur as part of the disease progression. In OSMF, elevated LDH levels reflect underlying hypoxia, oxidative stress, and inflammation caused by progressive fibrosis and reduced vascularity. This leads to a metabolic shift toward anaerobic glycolysis, cellular damage, and increased membrane permeability, resulting in LDH release. Additionally, activated fibroblasts and inflammatory cytokines contribute to tissue remodeling and cell turnover, further elevating LDH as a marker of disease severity and progression [6]. Saliva, being in direct contact with oral mucosa, is an ideal medium for non-invasive sampling of biomarkers such as LDH, providing a convenient alternative to blood tests for ongoing monitoring of the disease [10]. The objective of this study was to evaluate and compare serum and salivary LDH levels in OSMF patients and healthy controls, to assess the potential of LDH as a biochemical marker for OSMF diagnosis, and monitoring of its progression. Furthermore, this study aimed to explore the relationship between LDH levels and clinical staging of OSMF, providing further insights into the potential role of LDH in tracking disease severity and progression.
Materials and Methods
Study design:
This study employed a cross-sectional, case-control design, aimed at evaluating and comparing serum and salivary LDH levels in patients clinically diagnosed with OSMF [11], and healthy controls. The study was conducted at the Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh between August 2021 and September 2024. This design allowed for a snapshot analysis of the biochemical markers (serum and salivary LDH) in both groups at a specific point in time.
Ethical considerations:
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Ethics Committee (CDCR/DEAN/ETHICSCOMMITTEE/STAFF/OMRD-01/2024). All participants provided written informed consent before enrolment, ensuring voluntary participation and confidentiality of their personal data.
Participants:
The study involved a total of 256 participants, with 128 OSMF patients (group A) and 128 healthy controls (group B). The participants were recruited from the outpatient Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh.
Inclusion criteria:
Background and Aim: This study compared the serum and salivary lactate dehydrogenase (LDH) levels in patients with oral submucous fibrosis (OSMF) and healthy controls, and assessed their potential as biomarkers for OSMF diagnosis, and monitoring its progression.
Materials and Methods: This case-control study involved 50 OSMF patients and 50 age- and sex-matched healthy controls. Serum and salivary LDH levels were measured using standard laboratory techniques. Clinical staging of OSMF was performed based on the severity of symptoms, and the relationship between LDH levels and disease stage was analyzed using statistical methods. Descriptive and inferential statistics including t-test, ANOVA, and correlation coefficients based on data distribution were used to assess the association between LDH levels and OSMF clinical features (alpha=0.05).
Results: OSMF patients showed significantly higher serum LDH levels (225.4±58.2 U/L) than healthy controls (187.6±42.4 U/L; P=0.0004). They also showed significantly higher salivary LDH levels (180.3±53.1 U/L) compared to controls (148.2±37.9 U/L; P=0.0006). A strong positive correlation was found between serum LDH levels and clinical stage of OSMF (r=0.65, P<0.001), while a moderate inverse correlation was observed between salivary LDH levels and mouth opening (r=-0.48, P<0.001).
Conclusion: Both serum and salivary LDH levels were significantly elevated in patients with OSMF compared to healthy controls. Salivary LDH, in particular, demonstrated a strong association with clinical severity and disease stage, supporting its potential as an effective, non-invasive biomarker for OSMF diagnosis, and monitoring its progression.
Keywords: Biomarkers; L-Lactate Dehydrogenase; Oral Submucous Fibrosis; Saliva
Introduction
Oral submucous fibrosis (OSMF) is a chronic and progressive condition of the oral mucosa, characterized by the formation of fibrous bands that restrict mouth opening, and cause other debilitating symptoms, such as pain, burning sensation, and difficulty in chewing [1]. The disease is primarily associated with the habitual use of areca nut, tobacco, and alcohol, although genetic and environmental factors also play a role in its development [2]. It is considered a premalignant disorder, with a potential for malignant transformation to oral squamous cell carcinoma in its advanced stages [3,4]. Early detection and accurate monitoring of OSMF progression are crucial for effective management and preventing malignancy. However, clinical diagnosis of OSMF often relies on subjective symptoms and clinical examination, which can be challenging in early stages of the disease [5].
Biomarkers have gained attention as potential diagnostic tools for OSMF, offering an objective and non-invasive means to assess disease severity and monitor progression. Among the various biomarkers, lactate dehydrogenase (LDH) has emerged as a promising candidate [6]. LDH is an enzyme involved in anaerobic metabolism, converting lactate to pyruvate in cells. Its elevated levels in the blood and saliva have been linked to various pathological conditions, including cancers and inflammatory diseases, due to its release during cell damage and metabolic stress [7]. LDH has been found to be a sensitive indicator of cellular injury and tissue damage, making it a valuable marker in diseases like OSMF, where inflammation and fibrosis are central to the pathogenesis [8]. Evidence shows that serum and salivary LDH levels are elevated in patients with OSMF, suggesting that LDH could serve as a potential biomarker for diagnosing and monitoring of the disease [6]. Serum LDH has been widely used to assess the severity of various diseases, including liver cirrhosis, myocardial infarction, and malignancies [9]. In OSMF, the increased LDH levels may correlate with the degree of fibrosis, tissue remodeling, and inflammation that occur as part of the disease progression. In OSMF, elevated LDH levels reflect underlying hypoxia, oxidative stress, and inflammation caused by progressive fibrosis and reduced vascularity. This leads to a metabolic shift toward anaerobic glycolysis, cellular damage, and increased membrane permeability, resulting in LDH release. Additionally, activated fibroblasts and inflammatory cytokines contribute to tissue remodeling and cell turnover, further elevating LDH as a marker of disease severity and progression [6]. Saliva, being in direct contact with oral mucosa, is an ideal medium for non-invasive sampling of biomarkers such as LDH, providing a convenient alternative to blood tests for ongoing monitoring of the disease [10]. The objective of this study was to evaluate and compare serum and salivary LDH levels in OSMF patients and healthy controls, to assess the potential of LDH as a biochemical marker for OSMF diagnosis, and monitoring of its progression. Furthermore, this study aimed to explore the relationship between LDH levels and clinical staging of OSMF, providing further insights into the potential role of LDH in tracking disease severity and progression.
Materials and Methods
Study design:
This study employed a cross-sectional, case-control design, aimed at evaluating and comparing serum and salivary LDH levels in patients clinically diagnosed with OSMF [11], and healthy controls. The study was conducted at the Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh between August 2021 and September 2024. This design allowed for a snapshot analysis of the biochemical markers (serum and salivary LDH) in both groups at a specific point in time.
Ethical considerations:
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Ethics Committee (CDCR/DEAN/ETHICSCOMMITTEE/STAFF/OMRD-01/2024). All participants provided written informed consent before enrolment, ensuring voluntary participation and confidentiality of their personal data.
Participants:
The study involved a total of 256 participants, with 128 OSMF patients (group A) and 128 healthy controls (group B). The participants were recruited from the outpatient Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh.
Inclusion criteria:
- Age: Participants aged between 18 and 60 years.
- Diagnosis of OSMF: Only those with a clinical diagnosis of OSMF, confirmed through a combination of clinical examinations, were included in the OSMF group.
- Healthy controls: Participants without a history of any systemic diseases, oral diseases, or malignancies were included as controls. The controls were matched for age, gender, and socio-economic status with the OSMF group.
- Informed consent: All participants provided written informed consent, indicating their voluntary participation.
Exclusion criteria:
- Participants with a history of malignancies, systemic diseases (e.g., diabetes mellitus and hypertension), or other significant oral conditions (e.g., oral cancer, lichen planus) were excluded.
- Pregnant or lactating women were excluded to avoid potential confounding factors.
- OSMF patients undergoing active treatment (e.g., corticosteroids, surgical interventions) for OSMF were excluded to maintain uniformity in disease progression.
Recruitment:
Participants were recruited from the outpatient Department of Oral medicine and Radiology, Chhattisgarh Dental College & Research Institute. OSMF patients were diagnosed based on clinical findings (e.g., mucosal blanching, restricted mouth opening) and confirmed by histopathological analysis of a biopsy specimen. Healthy controls were selected from the general population who met the inclusion criteria.
Socio-economic status was assessed and matched using the Modified Kuppuswamy Socioeconomic Scale to ensure comparability between the study groups [12].
Clinical staging of OSMF:
OSMF patients were categorized into three clinical stages based on the staging system described by Wahi et al [11]:
Group I: This stage typically presents with no symptoms related to mucosal involvement. The lesions are localized, affecting one or more commonly involved anatomical sites. These lesions are focal in nature, characterized by pallor or a whitish coloration, with wrinkling of the mucosa and minimal induration [11].
Group II: Patients in this group may report symptoms such as soreness of the mucosa or increased sensitivity to spicy foods, particularly chili. The lesions are diffuse, white, and extensive, showing signs of induration, and may involve one or more anatomical sites [11].
Group III: Symptoms in this stage are primarily related to restricted mobility, including trismus, stretching at the angles of the mouth, and altered pronunciation. Firm mucosal bands can be palpated, and the surface of the lesions may be fissured or ulcerated [11].
Each stage w::as char::acterized by specific clinical features, including the degree of mouth opening, presence of mucosal blanching, pain or burning sensations, and fibrosis.
Sample collection:
Both serum and saliva samples were collected under standardized conditions to ensure consistency and accuracy in the results.
Blood samples: The collected blood samples were allowed to clot at room temperature (approximately 22–25°C) for 30 minutes [6]. Following clotting, the samples were centrifuged using a laboratory centrifuge (Remi R-8C; Remi Elektrotechnik Ltd., Mumbai, India) at 3000 rpm for 10 minutes to obtain clear serum. The supernatant serum was carefully aspirated using sterile polypropylene pipette tips (Tarsons Products Pvt. Ltd., Kolkata, India) and transferred into sterile cryovials (Corning Inc., New York, USA). The serum samples were immediately stored at –20°C in an ultra-low temperature freezer (Haier HDF-86H series; Haier Biomedical, Qingdao, China) until further biochemical analysis.
Saliva samples: In this study, unstimulated whole saliva was collected using the spitting method. The participants were instructed to sit in a relaxed position with their head slightly tilted forward, allowing saliva to accumulate passively in the floor of the mouth. At 60-second intervals, they expectorated the saliva into a sterile, graduated 50 mL polypropylene collection tube (Tarsons Products Pvt. Ltd., Kolkata, India). To minimize contamination, all participants were advised to abstain from eating, drinking, smoking, or performing any oral hygiene procedure for at least one hour prior to saliva collection [13].
Immediately after collection, the samples were sealed and labeled, then transported in an ice-lined transport box (Thermocol Carrier Box, Cipla Ltd., Mumbai, India) to the laboratory. Upon arrival, the samples were aliquoted using sterile polypropylene micropipette tips (Eppendorf AG, Hamburg, Germany) into 1.5 mL cryovials (Corning Inc., New York, USA) and stored at –20°C in an ultra-low temperature freezer (Haier HDF-86H series; Haier Biomedical, Qingdao, China) until further biochemical analysis.
Laboratory analysis of LDH levels:
The LDH activity in both serum and salivary samples was determined using an enzymatic colorimetric assay. The analysis was conducted using the lactate dehydrogenase assay kit (Sigma-Aldrich, St. Louis, MO, USA; Catalog No. LDH-400), following the manufacturer's instructions. To eliminate potential bias, the laboratory technician performing the assay was blinded to the clinical group assignments of the participants.
LDH activity was measured in both serum and saliva samples by the enzymatic method outlined in the assay kit protocol. All procedures, including sample preparation, reagent handling, and assay execution, were carried out in accordance with the manufacturer's guidelines to ensure accuracy and consistency of the results.
The LDH activity was expressed in units per liter (U/L) for both serum and saliva samples, a standard unit for reporting enzymatic activity. These measurements were used to compare LDH levels between the study groups (OSMF patients and healthy controls), and across the different clinical stages of OSMF.
In this study, comprehensive data were collected for each participant to facilitate an in-depth analysis of the relationship between LDH levels and the clinical characteristics of OSMF. The data collected were categorized into two main types: demographic and clinical data.
Demographic Data: The demographic data included key information about the participants' age, gender, tobacco consumption status, alcohol consumption, and relevant medical history.
Participants were recruited from the outpatient Department of Oral medicine and Radiology, Chhattisgarh Dental College & Research Institute. OSMF patients were diagnosed based on clinical findings (e.g., mucosal blanching, restricted mouth opening) and confirmed by histopathological analysis of a biopsy specimen. Healthy controls were selected from the general population who met the inclusion criteria.
Socio-economic status was assessed and matched using the Modified Kuppuswamy Socioeconomic Scale to ensure comparability between the study groups [12].
Clinical staging of OSMF:
OSMF patients were categorized into three clinical stages based on the staging system described by Wahi et al [11]:
Group I: This stage typically presents with no symptoms related to mucosal involvement. The lesions are localized, affecting one or more commonly involved anatomical sites. These lesions are focal in nature, characterized by pallor or a whitish coloration, with wrinkling of the mucosa and minimal induration [11].
Group II: Patients in this group may report symptoms such as soreness of the mucosa or increased sensitivity to spicy foods, particularly chili. The lesions are diffuse, white, and extensive, showing signs of induration, and may involve one or more anatomical sites [11].
Group III: Symptoms in this stage are primarily related to restricted mobility, including trismus, stretching at the angles of the mouth, and altered pronunciation. Firm mucosal bands can be palpated, and the surface of the lesions may be fissured or ulcerated [11].
Each stage w::as char::acterized by specific clinical features, including the degree of mouth opening, presence of mucosal blanching, pain or burning sensations, and fibrosis.
Sample collection:
Both serum and saliva samples were collected under standardized conditions to ensure consistency and accuracy in the results.
Blood samples: The collected blood samples were allowed to clot at room temperature (approximately 22–25°C) for 30 minutes [6]. Following clotting, the samples were centrifuged using a laboratory centrifuge (Remi R-8C; Remi Elektrotechnik Ltd., Mumbai, India) at 3000 rpm for 10 minutes to obtain clear serum. The supernatant serum was carefully aspirated using sterile polypropylene pipette tips (Tarsons Products Pvt. Ltd., Kolkata, India) and transferred into sterile cryovials (Corning Inc., New York, USA). The serum samples were immediately stored at –20°C in an ultra-low temperature freezer (Haier HDF-86H series; Haier Biomedical, Qingdao, China) until further biochemical analysis.
Saliva samples: In this study, unstimulated whole saliva was collected using the spitting method. The participants were instructed to sit in a relaxed position with their head slightly tilted forward, allowing saliva to accumulate passively in the floor of the mouth. At 60-second intervals, they expectorated the saliva into a sterile, graduated 50 mL polypropylene collection tube (Tarsons Products Pvt. Ltd., Kolkata, India). To minimize contamination, all participants were advised to abstain from eating, drinking, smoking, or performing any oral hygiene procedure for at least one hour prior to saliva collection [13].
Immediately after collection, the samples were sealed and labeled, then transported in an ice-lined transport box (Thermocol Carrier Box, Cipla Ltd., Mumbai, India) to the laboratory. Upon arrival, the samples were aliquoted using sterile polypropylene micropipette tips (Eppendorf AG, Hamburg, Germany) into 1.5 mL cryovials (Corning Inc., New York, USA) and stored at –20°C in an ultra-low temperature freezer (Haier HDF-86H series; Haier Biomedical, Qingdao, China) until further biochemical analysis.
Laboratory analysis of LDH levels:
The LDH activity in both serum and salivary samples was determined using an enzymatic colorimetric assay. The analysis was conducted using the lactate dehydrogenase assay kit (Sigma-Aldrich, St. Louis, MO, USA; Catalog No. LDH-400), following the manufacturer's instructions. To eliminate potential bias, the laboratory technician performing the assay was blinded to the clinical group assignments of the participants.
LDH activity was measured in both serum and saliva samples by the enzymatic method outlined in the assay kit protocol. All procedures, including sample preparation, reagent handling, and assay execution, were carried out in accordance with the manufacturer's guidelines to ensure accuracy and consistency of the results.
The LDH activity was expressed in units per liter (U/L) for both serum and saliva samples, a standard unit for reporting enzymatic activity. These measurements were used to compare LDH levels between the study groups (OSMF patients and healthy controls), and across the different clinical stages of OSMF.
In this study, comprehensive data were collected for each participant to facilitate an in-depth analysis of the relationship between LDH levels and the clinical characteristics of OSMF. The data collected were categorized into two main types: demographic and clinical data.
Demographic Data: The demographic data included key information about the participants' age, gender, tobacco consumption status, alcohol consumption, and relevant medical history.
- Age and gender: These variables were recorded to assess any potential influence of age and gender on LDH levels and OSMF progression.
- Tobacco consumption status: Tobacco is a significant risk factor in the development and progression of OSMF. Tobacco consumption status was categorized as either "current user," "former user," or "non-user."
- Alcohol consumption: Alcohol consumption was also recorded, as it is known to interact with oral mucosal tissues and may exacerbate the symptoms of OSMF. The participants' alcohol consumption was categorized as either "regular drinker" or "non-drinker," and this data helped in understanding the impact of alcohol on LDH levels in OSMF patients.
- Relevant medical history: The medical history of each participant was reviewed to ensure that participants did not have any co-existing conditions (e.g., diabetes mellitus, hypertension, or other oral conditions such as lichen planus) that could confound the results. Presence of such conditions was recorded to exclude participants who might introduce bias into the study findings.
Clinical data for OSMF patients: Clinical data were collected specifically for the OSMF patients (group A), which were critical in determining the stage and severity of OSMF and its potential association with serum and salivary LDH levels.
- Clinical staging of OSMF: The patients with OSMF were classified according to the clinical staging system (grade I, II, or III) based on the extent of mucosal involvement, fibrotic changes, and symptoms [11].
- Degree of mouth opening: The ability to open the mouth is a critical clinical symptom of OSMF, and its restriction often correlates with the degree of fibrosis and disease progression. The degree of mouth opening was measured using a digital vernier caliper, and such data helped in assessing the functional impairment caused by OSMF [11].
- Presence of mucosal blanching: Mucosal blanching is a hallmark of OSMF, often associated with the initial stages of fibrosis. This clinical sign was noted for each participant to identify early-stage changes in the mucosa and determine if there was an association between mucosal changes and LDH levels [11].
- Symptoms (pain or burning sensation): Many patients with OSMF experience symptoms such as a burning sensation or pain in the oral cavity, which can be related to the extent of the disease. These symptoms were documented to assess their potential correlation with serum and salivary LDH levels. The presence or absence of symptoms was recorded as "yes" or "no," and their severity was also noted if applicable [14].
Statistical analysis:
Data were analyzed using SPSS version 26. The analysis plan included both descriptive and inferential statistics to evaluate the relationship between LDH levels and clinical characteristics of OSMF. Descriptive statistics were used to summarize continuous variables such as age and LDH levels, with means, standard deviations, and ranges calculated, while categorical variables, including gender, tobacco consumption status, and alcohol use, were summarized using frequencies and percentages. To compare serum and salivary LDH levels between OSMF patients and healthy controls, independent t-test was used. In cases where the data were not normally distributed, the Mann-Whitney U test was used. One-way ANOVA was employed to examine variations in LDH levels across different stages of OSMF, with post-hoc Tukey’s test used for pairwise comparisons between the stages. The relationship between serum and salivary LDH levels and clinical severity indicators of OSMF (such as mouth opening and mucosal blanching) was assessed using the Pearson or Spearman’s correlation coefficients, depending on data distribution. A P-value < 0.05 was considered statistically significant for all analyses.
Results
The mean age of the participants in the OSMF group was 45.2±9.1 years, while the control group had a mean age of 44.8±8.7 years. No statistically significant difference in age distribution was found between the two groups (P=0.62). Regarding gender distribution, the OSMF group had 80 males and 48 females, while the control group had 82 males and 46 females, indicating no significant gender differences between the groups (P=0.81).
Tobacco use status significantly differed between the two groups, with 76.6% of OSMF patients being smokers compared to 17.2% of healthy controls (P=0.00001). Similarly, alcohol consumption was more prevalent in the OSMF group, with 56.3% reporting alcohol use versus 11.7% in the control group (P=0.00003). These findings highlight the significantly higher prevalence of tobacco and alcohol consumption among individuals with OSMF compared to healthy controls.
The mean serum LDH level in the OSMF group was significantly higher at 225.4 ± 58.2 U/L compared to 187.6 ± 42.4 U/L in the control group (P=0.0004), indicating elevated serum LDH levels in OSMF patients. Similarly, salivary LDH levels were significantly higher in the OSMF group (180.3 ± 53.1 U/L) compared to the control group (148.2 ± 37.9 U/L) (P=0.0007). These results suggest that both serum and salivary LDH levels were significantly elevated in OSMF patients, potentially indicating tissue damage or cellular stress associated with disease progression.
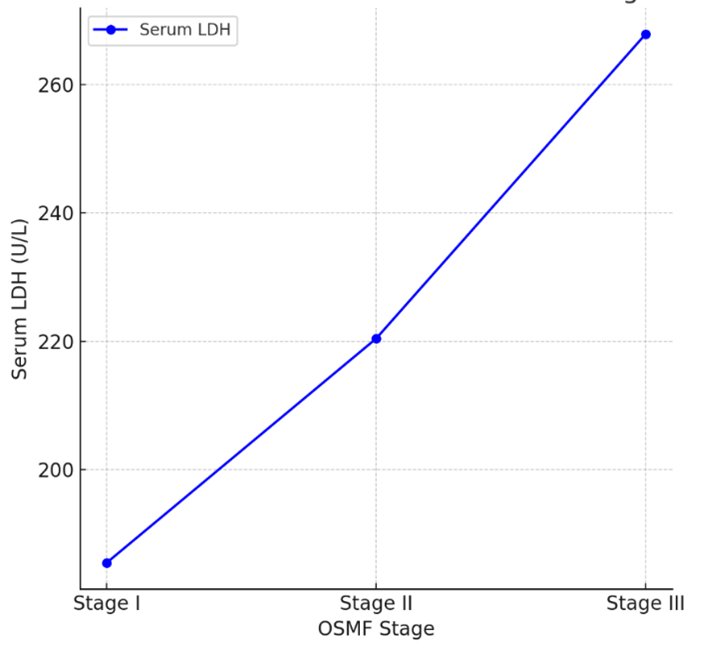
In stage I, the serum LDH level was 185.5 ± 50.3 U/L, which significantly increased to 220.4 ± 56.7 U/L in stage II (P<0.001). The highest serum LDH level was observed in stage III, with a mean of 267.8 ± 63.2 U/L, indicating a progressive increase in serum LDH levels with the advancement of OSMF.
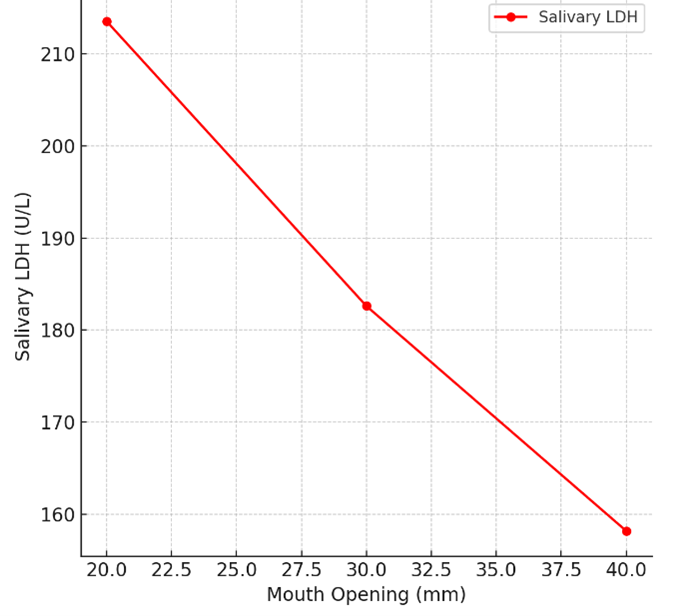
In stage I, the mean salivary LDH level was 158.2 ± 47.8 U/L, which increased to 182.6 ± 52.1 U/L in stage II, and further to 213.5 ± 56.4 U/L in stage III. The comparison revealed a statistically significant difference among the three stages (P=0.0002). Similar to serum LDH levels, salivary LDH levels increased progressively with advancing OSMF stages, suggesting that salivary LDH could serve as a useful non-invasive marker for monitoring of disease severity.
A positive correlation was observed between serum LDH levels and the clinical stage of OSMF (r=0.65, P=0.0001), indicating that higher LDH levels were associated with more advanced disease stages (Figure 1). Additionally, a negative correlation was found between salivary LDH levels and mouth opening (r=-0.48, P=0.0003), suggesting that as the severity of OSMF increased, mouth opening decreased while salivary LDH levels rose (Figure 2).
Figure 1. Correlation of serum LDH with OSMF stage
Figure 2. Correlation of salivary LDH with OSMF stage
Discussion
OSMF is a chronic, progressive, and fibrotic disorder of the oral mucosa that arises due to prolonged exposure to areca nut and tobacco, leading to excessive collagen deposition, epithelial atrophy, and vascular compromise [8]. In the present study, significantly elevated serum and salivary LDH levels were observed in OSMF patients when compared to healthy controls, suggesting that LDH may serve as a marker of tissue injury and disease progression in OSMF [15]. This can be mechanistically explained by the hypoxic and inflammatory microenvironment characteristics of OSMF. As fibrosis progresses, submucosal vascularity decreases, resulting in tissue hypoxia. Under these conditions, cells shift from aerobic to anaerobic metabolism, during which LDH plays a pivotal role in converting lactate to pyruvate, thereby increasing its expression and extracellular release [7]. Furthermore, areca nut-induced oxidative stress and chronic inflammation compromise cell membrane integrity, resulting in the passive release of cytoplasmic enzymes like LDH into extracellular fluids such as serum and saliva [16]. The elevated LDH levels observed in this study may thus reflect ongoing epithelial and stromal cell turnover, apoptosis, and necrosis as the hallmarks of OSMF tissue remodeling [17]. This is particularly significant in advanced stages of the disease, where increased fibrotic activity and persistent inflammatory responses exacerbate cellular injury. LDH, being a sensitive indicator of cell damage, has been widely studied in various fibrotic and inflammatory conditions including liver cirrhosis, myocardial infarction, and malignancies, where it correlates with disease burden and tissue destruction [18]. In the case of OSMF, chronic mucosal inflammation induced by carcinogenic alkaloids such as arecoline can activate immune cells and cytokines, promote a sustained inflammatory response and increase LDH release [19]. The observed LDH elevations in serum and saliva can thus be interpreted as a direct biochemical outcome of oxidative stress, mitochondrial dysfunction, and inflammatory cytokine-mediated cellular damage. Moreover, the symptoms typically experienced by OSMF patients, such as burning sensation, oral discomfort, and progressive trismus, are themselves clinical manifestations of underlying fibrosis and inflammation [20]. These symptoms, which indicate functional impairment, align with the biochemical findings of increased LDH, reinforcing its potential role as a non-invasive biomarker of disease activity. Therefore, the elevated LDH levels in this study are not merely associative but are biologically plausible outcomes based on the enzyme’s cellular role and the pathological processes at work in OSMF.
The present study also highlighted the significant differences in tobacco and alcohol consumption between the OSMF and control groups. Tobacco and alcohol consumption are well-established risk factors for the development and progression of OSMF. Both habits can lead to chronic irritation of the oral mucosa, which may promote the inflammatory processes and fibrotic characteristics of OSMF [21]. Tobacco, in particular, is known to induce oxidative stress and enhance inflammation, contributing to tissue damage and increased expression of enzymes like LDH [22]. Alcohol, especially when consumed regularly, may further exacerbate the mucosal damage and increase the severity of OSMF lesions. Our findings of significantly higher tobacco and alcohol consumption by OSMF patients compared to controls reinforce the known association between these factors and OSMF development [23]. In a study by Ariyawardana et al. [24], tobacco and alcohol consumption were found to be major contributors to the pathogenesis of OSMF, with smokers exhibiting a higher risk of progression to more severe stages of the disease. Additionally, evidence shows that cessation of tobacco and alcohol consumption can help reduce the severity of symptoms in OSMF patients, suggesting that these factors contribute to both the initiation and exacerbation of the disease [25]. Therefore, the elevated LDH levels in the OSMF group may also be a direct consequence of these lifestyle factors, which contribute to tissue damage and inflammation in the oral mucosa [26].
The comparison between serum and salivary LDH levels in this study is particularly noteworthy. While both serum and salivary LDH levels were significantly higher in OSMF patients, the salivary LDH levels were slightly lower than serum levels. This difference could be attributed to the fact that serum LDH levels represent systemic tissue damage; while, salivary LDH may be more reflective of local tissue damage within the oral cavity [17]. Saliva is in direct contact with the oral mucosa, and changes in the local inflammatory environment are likely to influence the levels of enzymes such as LDH [27]. Salivary biomarkers have been increasingly studied for their potential as non-invasive diagnostic tools in oral diseases, including OSMF. The use of salivary LDH as a diagnostic biomarker has the potential to offer several advantages over serum testing. Saliva collection is simple, non-invasive, and easily reproducible, making it a practical option for frequent monitoring of OSMF patients. This approach could be especially beneficial for early detection of disease progression or response to treatment. It has been demonstrated that salivary biomarkers, including LDH, may provide valuable insights into the pathogenesis of oral diseases, and could serve as a complement to clinical examination [6]. The findings of this study suggest that salivary LDH could be considered a potential biomarker for OSMF diagnosis and monitoring, although further research is needed to validate its clinical utility.
In this study, we also examined the relationship between clinical staging of OSMF and LDH levels. OSMF patients were categorized into three stages (I, II, and III) based on the severity of mucosal involvement and fibrosis. Elevated serum and salivary LDH levels were observed across all stages of OSMF, with higher levels in more advanced stages of the disease. This suggests that as the disease progresses and fibrosis becomes more severe, there is an increase in cellular damage, inflammation, and tissue remodeling, leading to higher LDH levels [18]. A similar association between disease severity and LDH levels has been reported in other studies of fibrotic diseases, such as liver cirrhosis [28]. In the present study, the significantly elevated LDH levels observed in both serum and saliva of OSMF patients can be mechanistically explained by the pathophysiological processes underlying the disease. OSMF is characterized by chronic inflammation, progressive fibrosis, and epithelial atrophy, all of which contribute to cellular stress and damage [11]. LDH, a cytoplasmic enzyme involved in anaerobic glycolysis, is released into extracellular fluids when cells undergo lysis or are subjected to hypoxia. In the context of OSMF, the fibrotic tissue restricts vascular perfusion, creating a hypoxic microenvironment that triggers anaerobic metabolic pathways and elevates LDH production [7]. Additionally, repeated irritation from areca nut and tobacco (common etiological factors in OSMF) induces oxidative stress and inflammation, compromising cell membrane integrity and promoting enzyme leakage. The direct contact of saliva with affected oral tissues allows salivary LDH to reflect localized epithelial injury, while serum LDH reflects systemic release from damaged mucosa. The positive correlation between LDH levels and disease severity, and the inverse correlation with mouth opening, further support the role of LDH as a marker of progressive tissue damage and fibrosis. These findings are not merely consistent with the existing literature but are biologically justified by the molecular and cellular changes intrinsic to OSMF progression [11].
Despite the promising results of this study, there are several limitations that must be addressed in future research. Firstly, the cross-sectional design of this study did not allow for causal inferences about the relationship between LDH levels and OSMF progression. Longitudinal studies are needed to track changes in LDH levels over time and assess their predictive value for disease progression. Additionally, while this study focused on serum and salivary LDH levels, other biomarkers of fibrosis and inflammation should be explored to gain a more comprehensive understanding of the molecular mechanisms underlying OSMF. Future studies should also investigate the potential impact of treatment interventions (e.g., corticosteroids or other anti-inflammatory drugs) on LDH levels in OSMF patients. Another limitation of this study was the relatively small sample size of 128 patients in each group. Larger cohort studies involving diverse populations are needed to confirm these findings, and validate LDH as a reliable biomarker for OSMF. Future studies should focus on validating these findings through larger, multicenter cohorts and evaluating LDH dynamics over time to establish its clinical utility in routine practice.
Conclusion
The study results showed that both serum and salivary LDH levels were significantly elevated in patients with OSMF compared to healthy controls. These elevated LDH levels are indicative of underlying cellular damage and chronic inflammation, which are central to the pathogenesis and progression of OSMF. The findings support the potential utility of LDH as a biochemical marker for assessing disease severity. In particular, salivary LDH demonstrated promise as a non-invasive, accessible diagnostic tool that could facilitate early detection and longitudinal monitoring of OSMF.
Data were analyzed using SPSS version 26. The analysis plan included both descriptive and inferential statistics to evaluate the relationship between LDH levels and clinical characteristics of OSMF. Descriptive statistics were used to summarize continuous variables such as age and LDH levels, with means, standard deviations, and ranges calculated, while categorical variables, including gender, tobacco consumption status, and alcohol use, were summarized using frequencies and percentages. To compare serum and salivary LDH levels between OSMF patients and healthy controls, independent t-test was used. In cases where the data were not normally distributed, the Mann-Whitney U test was used. One-way ANOVA was employed to examine variations in LDH levels across different stages of OSMF, with post-hoc Tukey’s test used for pairwise comparisons between the stages. The relationship between serum and salivary LDH levels and clinical severity indicators of OSMF (such as mouth opening and mucosal blanching) was assessed using the Pearson or Spearman’s correlation coefficients, depending on data distribution. A P-value < 0.05 was considered statistically significant for all analyses.
Results
The mean age of the participants in the OSMF group was 45.2±9.1 years, while the control group had a mean age of 44.8±8.7 years. No statistically significant difference in age distribution was found between the two groups (P=0.62). Regarding gender distribution, the OSMF group had 80 males and 48 females, while the control group had 82 males and 46 females, indicating no significant gender differences between the groups (P=0.81).
Tobacco use status significantly differed between the two groups, with 76.6% of OSMF patients being smokers compared to 17.2% of healthy controls (P=0.00001). Similarly, alcohol consumption was more prevalent in the OSMF group, with 56.3% reporting alcohol use versus 11.7% in the control group (P=0.00003). These findings highlight the significantly higher prevalence of tobacco and alcohol consumption among individuals with OSMF compared to healthy controls.
The mean serum LDH level in the OSMF group was significantly higher at 225.4 ± 58.2 U/L compared to 187.6 ± 42.4 U/L in the control group (P=0.0004), indicating elevated serum LDH levels in OSMF patients. Similarly, salivary LDH levels were significantly higher in the OSMF group (180.3 ± 53.1 U/L) compared to the control group (148.2 ± 37.9 U/L) (P=0.0007). These results suggest that both serum and salivary LDH levels were significantly elevated in OSMF patients, potentially indicating tissue damage or cellular stress associated with disease progression.
In stage I, the serum LDH level was 185.5 ± 50.3 U/L, which significantly increased to 220.4 ± 56.7 U/L in stage II (P<0.001). The highest serum LDH level was observed in stage III, with a mean of 267.8 ± 63.2 U/L, indicating a progressive increase in serum LDH levels with the advancement of OSMF.
In stage I, the mean salivary LDH level was 158.2 ± 47.8 U/L, which increased to 182.6 ± 52.1 U/L in stage II, and further to 213.5 ± 56.4 U/L in stage III. The comparison revealed a statistically significant difference among the three stages (P=0.0002). Similar to serum LDH levels, salivary LDH levels increased progressively with advancing OSMF stages, suggesting that salivary LDH could serve as a useful non-invasive marker for monitoring of disease severity.
A positive correlation was observed between serum LDH levels and the clinical stage of OSMF (r=0.65, P=0.0001), indicating that higher LDH levels were associated with more advanced disease stages (Figure 1). Additionally, a negative correlation was found between salivary LDH levels and mouth opening (r=-0.48, P=0.0003), suggesting that as the severity of OSMF increased, mouth opening decreased while salivary LDH levels rose (Figure 2).
Figure 1. Correlation of serum LDH with OSMF stage
{kind=link}
Figure 2. Correlation of salivary LDH with OSMF stage
{kind=link}
Discussion
OSMF is a chronic, progressive, and fibrotic disorder of the oral mucosa that arises due to prolonged exposure to areca nut and tobacco, leading to excessive collagen deposition, epithelial atrophy, and vascular compromise [8]. In the present study, significantly elevated serum and salivary LDH levels were observed in OSMF patients when compared to healthy controls, suggesting that LDH may serve as a marker of tissue injury and disease progression in OSMF [15]. This can be mechanistically explained by the hypoxic and inflammatory microenvironment characteristics of OSMF. As fibrosis progresses, submucosal vascularity decreases, resulting in tissue hypoxia. Under these conditions, cells shift from aerobic to anaerobic metabolism, during which LDH plays a pivotal role in converting lactate to pyruvate, thereby increasing its expression and extracellular release [7]. Furthermore, areca nut-induced oxidative stress and chronic inflammation compromise cell membrane integrity, resulting in the passive release of cytoplasmic enzymes like LDH into extracellular fluids such as serum and saliva [16]. The elevated LDH levels observed in this study may thus reflect ongoing epithelial and stromal cell turnover, apoptosis, and necrosis as the hallmarks of OSMF tissue remodeling [17]. This is particularly significant in advanced stages of the disease, where increased fibrotic activity and persistent inflammatory responses exacerbate cellular injury. LDH, being a sensitive indicator of cell damage, has been widely studied in various fibrotic and inflammatory conditions including liver cirrhosis, myocardial infarction, and malignancies, where it correlates with disease burden and tissue destruction [18]. In the case of OSMF, chronic mucosal inflammation induced by carcinogenic alkaloids such as arecoline can activate immune cells and cytokines, promote a sustained inflammatory response and increase LDH release [19]. The observed LDH elevations in serum and saliva can thus be interpreted as a direct biochemical outcome of oxidative stress, mitochondrial dysfunction, and inflammatory cytokine-mediated cellular damage. Moreover, the symptoms typically experienced by OSMF patients, such as burning sensation, oral discomfort, and progressive trismus, are themselves clinical manifestations of underlying fibrosis and inflammation [20]. These symptoms, which indicate functional impairment, align with the biochemical findings of increased LDH, reinforcing its potential role as a non-invasive biomarker of disease activity. Therefore, the elevated LDH levels in this study are not merely associative but are biologically plausible outcomes based on the enzyme’s cellular role and the pathological processes at work in OSMF.
The present study also highlighted the significant differences in tobacco and alcohol consumption between the OSMF and control groups. Tobacco and alcohol consumption are well-established risk factors for the development and progression of OSMF. Both habits can lead to chronic irritation of the oral mucosa, which may promote the inflammatory processes and fibrotic characteristics of OSMF [21]. Tobacco, in particular, is known to induce oxidative stress and enhance inflammation, contributing to tissue damage and increased expression of enzymes like LDH [22]. Alcohol, especially when consumed regularly, may further exacerbate the mucosal damage and increase the severity of OSMF lesions. Our findings of significantly higher tobacco and alcohol consumption by OSMF patients compared to controls reinforce the known association between these factors and OSMF development [23]. In a study by Ariyawardana et al. [24], tobacco and alcohol consumption were found to be major contributors to the pathogenesis of OSMF, with smokers exhibiting a higher risk of progression to more severe stages of the disease. Additionally, evidence shows that cessation of tobacco and alcohol consumption can help reduce the severity of symptoms in OSMF patients, suggesting that these factors contribute to both the initiation and exacerbation of the disease [25]. Therefore, the elevated LDH levels in the OSMF group may also be a direct consequence of these lifestyle factors, which contribute to tissue damage and inflammation in the oral mucosa [26].
The comparison between serum and salivary LDH levels in this study is particularly noteworthy. While both serum and salivary LDH levels were significantly higher in OSMF patients, the salivary LDH levels were slightly lower than serum levels. This difference could be attributed to the fact that serum LDH levels represent systemic tissue damage; while, salivary LDH may be more reflective of local tissue damage within the oral cavity [17]. Saliva is in direct contact with the oral mucosa, and changes in the local inflammatory environment are likely to influence the levels of enzymes such as LDH [27]. Salivary biomarkers have been increasingly studied for their potential as non-invasive diagnostic tools in oral diseases, including OSMF. The use of salivary LDH as a diagnostic biomarker has the potential to offer several advantages over serum testing. Saliva collection is simple, non-invasive, and easily reproducible, making it a practical option for frequent monitoring of OSMF patients. This approach could be especially beneficial for early detection of disease progression or response to treatment. It has been demonstrated that salivary biomarkers, including LDH, may provide valuable insights into the pathogenesis of oral diseases, and could serve as a complement to clinical examination [6]. The findings of this study suggest that salivary LDH could be considered a potential biomarker for OSMF diagnosis and monitoring, although further research is needed to validate its clinical utility.
In this study, we also examined the relationship between clinical staging of OSMF and LDH levels. OSMF patients were categorized into three stages (I, II, and III) based on the severity of mucosal involvement and fibrosis. Elevated serum and salivary LDH levels were observed across all stages of OSMF, with higher levels in more advanced stages of the disease. This suggests that as the disease progresses and fibrosis becomes more severe, there is an increase in cellular damage, inflammation, and tissue remodeling, leading to higher LDH levels [18]. A similar association between disease severity and LDH levels has been reported in other studies of fibrotic diseases, such as liver cirrhosis [28]. In the present study, the significantly elevated LDH levels observed in both serum and saliva of OSMF patients can be mechanistically explained by the pathophysiological processes underlying the disease. OSMF is characterized by chronic inflammation, progressive fibrosis, and epithelial atrophy, all of which contribute to cellular stress and damage [11]. LDH, a cytoplasmic enzyme involved in anaerobic glycolysis, is released into extracellular fluids when cells undergo lysis or are subjected to hypoxia. In the context of OSMF, the fibrotic tissue restricts vascular perfusion, creating a hypoxic microenvironment that triggers anaerobic metabolic pathways and elevates LDH production [7]. Additionally, repeated irritation from areca nut and tobacco (common etiological factors in OSMF) induces oxidative stress and inflammation, compromising cell membrane integrity and promoting enzyme leakage. The direct contact of saliva with affected oral tissues allows salivary LDH to reflect localized epithelial injury, while serum LDH reflects systemic release from damaged mucosa. The positive correlation between LDH levels and disease severity, and the inverse correlation with mouth opening, further support the role of LDH as a marker of progressive tissue damage and fibrosis. These findings are not merely consistent with the existing literature but are biologically justified by the molecular and cellular changes intrinsic to OSMF progression [11].
Despite the promising results of this study, there are several limitations that must be addressed in future research. Firstly, the cross-sectional design of this study did not allow for causal inferences about the relationship between LDH levels and OSMF progression. Longitudinal studies are needed to track changes in LDH levels over time and assess their predictive value for disease progression. Additionally, while this study focused on serum and salivary LDH levels, other biomarkers of fibrosis and inflammation should be explored to gain a more comprehensive understanding of the molecular mechanisms underlying OSMF. Future studies should also investigate the potential impact of treatment interventions (e.g., corticosteroids or other anti-inflammatory drugs) on LDH levels in OSMF patients. Another limitation of this study was the relatively small sample size of 128 patients in each group. Larger cohort studies involving diverse populations are needed to confirm these findings, and validate LDH as a reliable biomarker for OSMF. Future studies should focus on validating these findings through larger, multicenter cohorts and evaluating LDH dynamics over time to establish its clinical utility in routine practice.
Conclusion
The study results showed that both serum and salivary LDH levels were significantly elevated in patients with OSMF compared to healthy controls. These elevated LDH levels are indicative of underlying cellular damage and chronic inflammation, which are central to the pathogenesis and progression of OSMF. The findings support the potential utility of LDH as a biochemical marker for assessing disease severity. In particular, salivary LDH demonstrated promise as a non-invasive, accessible diagnostic tool that could facilitate early detection and longitudinal monitoring of OSMF.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Chhabra AK, Sune R, Reche A. Oral Submucous Fibrosis: A Review of the Current Concepts in Management. Cureus. 2023 Oct;15(10):e47259. [DOI:10.7759/cureus.47259]
2. Murthy V, Mylonas P, Carey B, Yogarajah S, Farnell D, Addison O, et al. Malignant Transformation Rate of Oral Submucous Fibrosis: A Systematic Review and Meta-Analysis. J Clin Med. 2022 Mar;11(7):1793. [DOI:10.3390/jcm11071793] [PMID] [PMCID]
3. Lorini L, Bescós Atín C, Thavaraj S, Müller-Richter U, Alberola Ferranti M, Pamias Romero J, et al. Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies. Cancers (Basel). 2021 Jul;13(15):3696. [DOI:10.3390/cancers13153696] [PMID] [PMCID]
4. Foy JP, Bertolus C, William WN Jr, Saintigny P. Oral premalignancy: the roles of early detection and chemoprevention. Otolaryngol Clin North Am. 2013 May;46(4):579-97. [DOI:10.1016/j.otc.2013.04.010] [PMID] [PMCID]
5. More CB, Jatti Patil D, Rao NR. Medicinal management of oral submucous fibrosis in the past decade- A systematic review. J Oral Biol Craniofac Res. 2020 Oct;10(4):552-68. [DOI:10.1016/j.jobcr.2020.08.004] [PMID] [PMCID]
6. Mahapatra M, Panda A, Kumar H, Barman D, Talukdar R, Dakshinakabat P. Lactate Dehydrogenase as a Biomarker in Oral Submucous Fibrosis: A Systematic Review and Meta-Analysis. Cureus. 2023 Dec;15(12):e51008. [DOI:10.7759/cureus.51008]
7. Farhana A, Lappin SL. Biochemistry, Lactate Dehydrogenase. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557536
8. Shih YH, Wang TH, Shieh TM, Tseng YH. Oral submucous fibrosis: A review on etiopathogenesis, diagnosis, and therapy. Int J Mol Sci. 2019 Jun;20(12):2940. [DOI:10.3390/ijms20122940] [PMID] [PMCID]
9. Kim J, Kim YW, Kim TY. Diagnostic value of serum lactate dehydrogenase level measured in the emergency department in predicting clinical outcome in out-of-hospital cardiac arrest: A multicenter, observational study. J Clin Med. 2023 Apr;12(8):3006. [DOI:10.3390/jcm12083006] [PMID] [PMCID]
10. Kumar P, Gupta S, Das BC. Saliva as a potential non-invasive liquid biopsy for early and easy diagnosis/prognosis of head and neck cancer. Transl Oncol. 2024 Feb;40:101827. [DOI:10.1016/j.tranon.2023.101827] [PMID] [PMCID]
11. Wahi PN, Kapur VL, Luthra UK, Srivastava MC. Submucous fibrosis of the oral cavity. 1. Clinical features. Bull World Health Organ. 1966;35(5):789-92.
12. Wani RT. Socioeconomic status scales-modified Kuppuswamy and Udai Pareekh's scale updated for 2019. J Family Med Prim Care. 2019 Jun;8(6):1846-9. [DOI:10.4103/jfmpc.jfmpc_288_19] [PMID] [PMCID]
13. Navazesh M. Methods for collecting saliva. Ann N Y Acad Sci. 1993 Sep;694(1):72-7. [DOI:10.1111/j.1749-6632.1993.tb18343.x] [PMID]
14. More CB, Gupta S, Joshi J, Varma SN. Classification system for oral submucous fibrosis. J. Indian Acad. Oral Med. Radiol. 2012;24(1):24. [DOI:10.5005/jp-journals-10011-1254]
15. Mokwatsi GG, Schutte AE, Kruger R. A biomarker of tissue damage, lactate dehydrogenase, is associated with fibulin-1 and oxidative stress in blacks: the SAfrEIC study. Biomarkers. 2016 Jan;21(1):48-55. [DOI:10.3109/1354750X.2015.1118532] [PMID]
16. Yada M, Miyazaki M, Motomura K, Masumoto A, Nakamuta M, Kohjima M, et al. The prognostic role of lactate dehydrogenase serum levels in patients with hepatocellular carcinoma who are treated with sorafenib: the influence of liver fibrosis. J Gastrointest Oncol. 2016 Aug;7(4):615-23. [DOI:10.21037/jgo.2016.03.10] [PMID] [PMCID]
17. Chen X, Chen T, Xie H, Guo J. Salivary and serum levels of lactate dehydrogenase in oral submucous fibrosis: A meta-analysis. Medicine (Baltimore). 2024 Apr;103(15):e37788. [DOI:10.1097/MD.0000000000037788] [PMID] [PMCID]
18. Gupta GS. The Lactate and the Lactate Dehydrogenase in Inflammatory Diseases and Major Risk Factors in COVID-19 Patients. Inflammation. 2022 Dec;45(6):2091-123. [DOI:10.1007/s10753-022-01680-7] [PMID] [PMCID]
19. Alonso-Bernáldez M, Cuevas-Sierra A, Micó V, Higuera-Gómez A, Ramos-Lopez O, Daimiel L, et al. An interplay between oxidative stress (lactate dehydrogenase) and inflammation (anisocytosis) mediates COVID-19 severity defined by routine clinical markers. Antioxidants (Basel). 2023 Jan;12(2):234. [DOI:10.3390/antiox12020234] [PMID] [PMCID]
20. Xu H, Lyu FY, Song JY, Xu YM, Jiang EH, Shang ZJ, et al. Research Achievements of Oral Submucous Fibrosis: Progress and Prospect. Biomed Res Int. 2021 Mar;2021:6631856. [DOI:10.1155/2021/6631856] [PMID] [PMCID]
21. Ahmed J, Puri A, Nangia R, Bhat S, Pasbola A. Oral submucous fibrosis: Histopathogenesis. Arch Dent Res. 2023;13(2):64-8. [DOI:10.18231/j.adr.2023.014]
22. Seo YS, Park JM, Kim JH, Lee MY. Cigarette smoke-induced reactive oxygen species formation: a concise review. Antioxidants. 2023 Sep;12(9):1732. [DOI:10.3390/antiox12091732] [PMID] [PMCID]
23. Hashibe M, Sankaranarayanan R, Thomas G, Kuruvilla B, Mathew B, Somanathan T, et al. Body mass index, tobacco chewing, alcohol drinking and the risk of oral submucous fibrosis in Kerala, India. Cancer Causes Control. 2002 Feb;13(1):55-64. [DOI:10.1023/A:1013991025848] [PMID]
24. Ariyawardana A, Athukorala AD, Arulanandam A. Effect of betel chewing, tobacco smoking and alcohol consumption on oral submucous fibrosis: a case-control study in Sri Lanka. J Oral Pathol Med. 2006 Apr;35(4):197-201. [DOI:10.1111/j.1600-0714.2006.00400.x] [PMID]
25. Rao NR, Villa A, More CB, Jayasinghe RD, Kerr AR, Johnson NW. Oral submucous fibrosis: a contemporary narrative review with a proposed inter-professional approach for an early diagnosis and clinical management. J Otolaryngol Head Neck Surg. 2020 Jan;49(1):3. [DOI:10.1186/s40463-020-0399-7] [PMID] [PMCID]
26. Singh AG, Roy S, Oza S, Singhavi H, Chatterjee K, Chaturvedi P. A contemporary narrative review to guide molecular epidemiology of oral submucous fibrosis. Int J Mol Epidemiol Genet. 2021 Aug;12(4):61-70.
27. Avezov K, Reznick AZ, Aizenbud D. LDH enzyme activity in human saliva: the effect of exposure to cigarette smoke and its different components. Arch Oral Biol. 2014 Feb;59(2):142-8. [DOI:10.1016/j.archoralbio.2013.11.003] [PMID]
28. Żmudka K, Jaroszewicz J, Zarębska-Michaluk D, Rogalska M, Czupryna P, Rorat M, et al. Association between liver damage and disease progression markers with mortality risk and mechanical ventilation in hospitalized COVID-19 patients: A nationwide retrospective SARSTer study. Viruses. 2024 Sep;16(10):1530. [DOI:10.3390/v16101530] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |