Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 2 (6-2026)
J Res Dent Maxillofac Sci 2026, 11(2): 97-106 |
Back to browse issues page

Ethics code: IR.MUBABOL.HRI.REC.1400.053
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Razian F, Daryaei F, Mahmoudi E, Moudi E, Saeidi A, Gholinia H et al . Efficacy of ProTaper, M3, and Edge Endo Rotary Files for Removal of Root Canal Filling Materials: An Ex Vivo Study Using CBCT. J Res Dent Maxillofac Sci 2026; 11 (2) :97-106
URL: http://jrdms.dentaliau.ac.ir/article-1-924-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-924-en.html
Fatemeh Razian1 
 , Fatemeh Daryaei1 , Elham Mahmoudi *2 , Ehsan Moudi3 , Akam Saeidi4 , Hemmat Gholinia5 , Zahra Sadat Madani4
, Fatemeh Daryaei1 , Elham Mahmoudi *2 , Ehsan Moudi3 , Akam Saeidi4 , Hemmat Gholinia5 , Zahra Sadat Madani4
, Fatemeh Daryaei1 , Elham Mahmoudi *2 , Ehsan Moudi3 , Akam Saeidi4 , Hemmat Gholinia5 , Zahra Sadat Madani4
1- Student Research Committee, Babol University of Medical Sciences, Babol, Iran.
2- Dental Materials Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,dr.elhammahmoodi@yahoo.com
3- Oral Health and Hygiene Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
4- Dental Materials Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
5- Health Research Institute, Babol University of Medical Sciences, Babol, Iran
2- Dental Materials Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,
3- Oral Health and Hygiene Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
4- Dental Materials Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
5- Health Research Institute, Babol University of Medical Sciences, Babol, Iran
Keywords: Cone-Beam Computed Tomography, Gutta-Percha, Molar, Root Canal Obturation, Root Canal Therapy
Full-Text [PDF 404 kb]
(6 Downloads)
| Abstract (HTML) (7 Views)
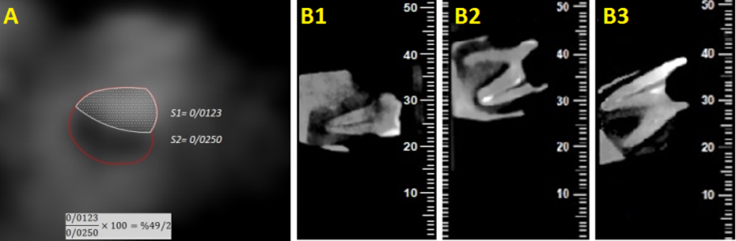
Figure 1. CBCT cross-sections: (A) Calculation of the surface area, (B1, B2, and B3) sagittal views for qualitative scoring
Statistical analysis:
Data were analyzed using SPSS version 26. Given that the data did not have a normal distribution based on the Shapiro-Wilk test result, the Kruskal-Wallis test followed by the Mann-Whitney test were used to compare the remaining filling material across the study groups. The Chi-square test was employed to assess the differences in the frequency of file fractures among the groups. A P value < 0.05 was considered statistically significant.
Results
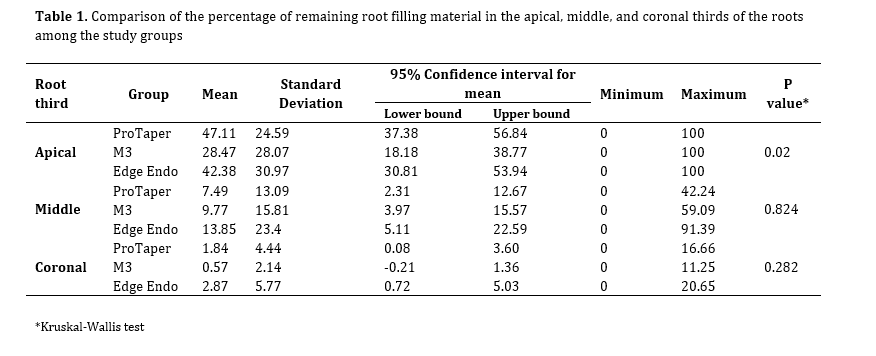
The amount of remaining filling material in the apical, middle, and coronal thirds of the root in each group is presented in Table 1.
Full-Text: (1 Views)
Abstract
Background and Aim: Previous studies have reported inconsistent findings on the effectiveness of endodontic retreatment rotary files for removal of residual filling materials. This study aimed to compare the efficacy of ProTaper, M3, and Edge Endo rotary retreatment systems for removal of root canal filling materials using cone-beam computed tomography (CBCT).
Materials and Methods: This ex vivo experimental study involved mesiobuccal and mesiolingual canals of mandibular molars, and mesiobuccal canals of maxillary molars (n=60) with ≤20-degree curvature. Canals were instrumented with ProTaper files with the crown-down technique, and obturated with gutta-percha and AH26 sealer via cold lateral compaction technique. Specimens were randomly assigned to three groups (n=20) of ProTaper, M3, or Edge Endo. CBCT imaging and AutoCAD software were used to quantify residual filling material in the coronal, middle, and apical thirds, and along the full canal length. Procedural errors, including file fracture, were recorded. Data were analyzed using the Kruskal-Wallis, Mann-Whitney, and Chi-square tests, with a significance level of 0.05.
Results: A statistically significant difference was observed in the apical third (P=0.02), with ProTaper retaining the most (47.11%±24.59%), and M3 the least (28.47%±28.07%) filling material. No significant differences were found in the coronal (P=0.282) and middle thirds (P=0.824). File fracture occurred in 12% of the cases, with no significant difference among the groups (P=0.809).
Conclusion: Based on the results, while residual filling material remained in all canals, the M3 rotary retreatment files demonstrated superior efficiency in cleaning the apical third.
Keywords: Cone-Beam Computed Tomography; Gutta-Percha; Molar; Root Canal Obturation; Root Canal Therapy
Introduction
Although the overall success rate of root canal therapy is high, treatment failure and the need for retreatment remain potential outcomes [1]. In endodontic retreatment, complete removal of filling materials is crucial to ensure adequate contact of irrigants and intracanal medicaments with the canal walls. Several techniques are available for removal of filling materials from the root canal system, including the use of heat, solvents, manual files, ultrasonic instruments, lasers, and rotary files [2, 3]. However, none of the available methods can achieve complete removal of root canal filling materials [4]. The use of manual files, with or without solvents, can be particularly time-consuming and labor-intensive, especially when the filling material is highly compacted [3].
Rotary instruments typically require less time for canal cleaning compared to manual instruments, which helps reduce both patient discomfort and clinician fatigue [4]. The use of nickel-titanium (NiTi) rotary instruments for safe and efficient removal of root filling materials during endodontic retreatment has been well documented.
The ProTaper Universal retreatment kit includes three flexible instruments of varying lengths, specifically designed for removal of root canal filling materials from the coronal, middle, and apical thirds [5]. The M3 rotary files consist of three instruments with an inactive tip and a convex triangular cross-section, offering high flexibility and resistance to cyclic fatigue, which allows for continuous rotation [6]. The Edge-Endo rotary files feature four instruments made from an annealed NiTi alloy, treated with a heat process called Fire-Wire, which enhances their flexibility and resistance to cyclic fatigue [7].
Various methods, including stereomicroscopy, radiography, micro-computed tomography, and cone-beam computed tomography (CBCT), have been used to assess residual filling material in root canals after retreatment [8]. Stereomicroscopic assessment of longitudinally sectioned roots offers real-time visualization with reasonable accuracy; however, it may be prone to inaccuracies due to the loss of canal wall and displacement of gutta-percha debris during sectioning [9]. Radiography, providing a two-dimensional image of a three-dimensional structure, is less accurate for identifying gutta-percha and sealer [10]. In contrast, CBCT has demonstrated superior diagnostic performance in evaluating root canal systems, assessing resorptive lesions, and planning endodontic surgeries. Thus, CBCT is considered a highly accurate method for evaluation of residual filling materials following root canal retreatment [10].
Given the limited and conflicting findings in the literature regarding the efficacy of rotary files in endodontic retreatment, the present study aimed to evaluate the effectiveness of ProTaper, M3, and Edge Endo rotary retreatment files for removal of root canal filling materials using CBCT. The null hypothesis stated that there would be no statistically significant difference in the volume of remaining root filling material following retreatment using ProTaper, M2, and Edge Endo rotary file systems as evaluated by CBCT volumetric analysis.
Materials and Methods
This ex vivo experimental study was conducted on 60 maxillary and mandibular molars extracted for purposes not related to this study. The study protocol was approved by the Ethics Committee of Babol University of Medical Sciences (IR.MUBABOL.HRI.REC.1400.053).
The sample size for each group was determined based on the results of a similar study comparing the volume of residual filling materials after using ProTaper and H files [11], with a 95% confidence level (α=0.05) and a study power of 80% (β=0.2), yielding 20 samples per group.
Inclusion and exclusion criteria:
The mesiobuccal canals of maxillary and mandibular molars, and mesiolingual canals of mandibular molars, with a curvature of less than 20 degrees based on Schneider’s method [12] and no isthmus, classified as Vertucci's type 4 based on radiographic evaluation, were included [13]. Teeth with cracks, resorption defects, immature apices, or S-shaped curvature were excluded [11].
Specimen preparation:
Soft tissue and calculus were mechanically removed from the root surfaces, and the teeth were disinfected in 0.5% chloramine T solution (Merck KGaA, Darmstadt, Germany). To standardize the samples, all teeth were decoronated to ensure that the root length was consistently 18 mm. A size 10 stainless-steel K-file (Mani Inc., Tochigi, Japan) was then inserted into each root canal, with the file tip visible at the apical foramen. The working length was set to 1 mm shorter than the total root length. The roots were subsequently covered with two layers of paraffin wax (Kimia Gharb Co., Tehran, Iran), and mounted in dental gypsum (Pars Dandan, Tehran, Iran) blocks. All canals were instrumented with ProTaper NiTi rotary files (Sx, S1, S2, F1, and F2; Dentsply Maillefer, Switzerland) using a rotary endodontic motor (ENDO-MATE DT NE131; NSK, Nakanishi Inc., Tokyo, Japan) operating at 300 rpm with 3 N/cm torque, following the manufacturer's guidelines. The preparation of the apical region (apical 3 mm) was completed using a F2 file (size: 25, taper: 0.08). During each instrumentation step, the canals were irrigated with 1% NaOCl (Morvabon, Tehran, Iran), delivered via a syringe with a 30-gauge needle (NaviTip, Ultradent Products Inc., South Jordan, UT, USA). The root canals were subsequently filled with size 25 (or one size larger to match the F2 file size) gutta-percha (Dentsply Sirona, Ballaigues, Switzerland) and AH26 sealer (Dentsply Sirona, Ballaigues, Switzerland) using the lateral compaction technique, ensuring that the last gutta-percha point could not penetrate more than 5 mm into the canal. Any excess gutta-percha was removed using a heated plugger (Obtura Spartan, Algonquin, IL, USA). The obturation quality was assessed, and teeth with isthmuses were excluded from the study and replaced with new teeth. The access cavities were temporarily sealed with a cotton pellet and Cavisol temporary restorative material (Golchai Co., Tehran, Iran). To allow complete setting of the sealer, the samples were stored at 37°C and 100% humidity for 14 days. Afterwards, the temporary restoration was removed, and extra-pure chloroform (ED-430; Nik Darman, Iran) was used to soften the gutta-percha at the canal orifice [14].
Group allocation and procedure:
A total of 60 teeth were randomly assigned to three groups, each containing 20 teeth, ensuring uniform distribution in terms of canal types:
Background and Aim: Previous studies have reported inconsistent findings on the effectiveness of endodontic retreatment rotary files for removal of residual filling materials. This study aimed to compare the efficacy of ProTaper, M3, and Edge Endo rotary retreatment systems for removal of root canal filling materials using cone-beam computed tomography (CBCT).
Materials and Methods: This ex vivo experimental study involved mesiobuccal and mesiolingual canals of mandibular molars, and mesiobuccal canals of maxillary molars (n=60) with ≤20-degree curvature. Canals were instrumented with ProTaper files with the crown-down technique, and obturated with gutta-percha and AH26 sealer via cold lateral compaction technique. Specimens were randomly assigned to three groups (n=20) of ProTaper, M3, or Edge Endo. CBCT imaging and AutoCAD software were used to quantify residual filling material in the coronal, middle, and apical thirds, and along the full canal length. Procedural errors, including file fracture, were recorded. Data were analyzed using the Kruskal-Wallis, Mann-Whitney, and Chi-square tests, with a significance level of 0.05.
Results: A statistically significant difference was observed in the apical third (P=0.02), with ProTaper retaining the most (47.11%±24.59%), and M3 the least (28.47%±28.07%) filling material. No significant differences were found in the coronal (P=0.282) and middle thirds (P=0.824). File fracture occurred in 12% of the cases, with no significant difference among the groups (P=0.809).
Conclusion: Based on the results, while residual filling material remained in all canals, the M3 rotary retreatment files demonstrated superior efficiency in cleaning the apical third.
Keywords: Cone-Beam Computed Tomography; Gutta-Percha; Molar; Root Canal Obturation; Root Canal Therapy
Introduction
Although the overall success rate of root canal therapy is high, treatment failure and the need for retreatment remain potential outcomes [1]. In endodontic retreatment, complete removal of filling materials is crucial to ensure adequate contact of irrigants and intracanal medicaments with the canal walls. Several techniques are available for removal of filling materials from the root canal system, including the use of heat, solvents, manual files, ultrasonic instruments, lasers, and rotary files [2, 3]. However, none of the available methods can achieve complete removal of root canal filling materials [4]. The use of manual files, with or without solvents, can be particularly time-consuming and labor-intensive, especially when the filling material is highly compacted [3].
Rotary instruments typically require less time for canal cleaning compared to manual instruments, which helps reduce both patient discomfort and clinician fatigue [4]. The use of nickel-titanium (NiTi) rotary instruments for safe and efficient removal of root filling materials during endodontic retreatment has been well documented.
The ProTaper Universal retreatment kit includes three flexible instruments of varying lengths, specifically designed for removal of root canal filling materials from the coronal, middle, and apical thirds [5]. The M3 rotary files consist of three instruments with an inactive tip and a convex triangular cross-section, offering high flexibility and resistance to cyclic fatigue, which allows for continuous rotation [6]. The Edge-Endo rotary files feature four instruments made from an annealed NiTi alloy, treated with a heat process called Fire-Wire, which enhances their flexibility and resistance to cyclic fatigue [7].
Various methods, including stereomicroscopy, radiography, micro-computed tomography, and cone-beam computed tomography (CBCT), have been used to assess residual filling material in root canals after retreatment [8]. Stereomicroscopic assessment of longitudinally sectioned roots offers real-time visualization with reasonable accuracy; however, it may be prone to inaccuracies due to the loss of canal wall and displacement of gutta-percha debris during sectioning [9]. Radiography, providing a two-dimensional image of a three-dimensional structure, is less accurate for identifying gutta-percha and sealer [10]. In contrast, CBCT has demonstrated superior diagnostic performance in evaluating root canal systems, assessing resorptive lesions, and planning endodontic surgeries. Thus, CBCT is considered a highly accurate method for evaluation of residual filling materials following root canal retreatment [10].
Given the limited and conflicting findings in the literature regarding the efficacy of rotary files in endodontic retreatment, the present study aimed to evaluate the effectiveness of ProTaper, M3, and Edge Endo rotary retreatment files for removal of root canal filling materials using CBCT. The null hypothesis stated that there would be no statistically significant difference in the volume of remaining root filling material following retreatment using ProTaper, M2, and Edge Endo rotary file systems as evaluated by CBCT volumetric analysis.
Materials and Methods
This ex vivo experimental study was conducted on 60 maxillary and mandibular molars extracted for purposes not related to this study. The study protocol was approved by the Ethics Committee of Babol University of Medical Sciences (IR.MUBABOL.HRI.REC.1400.053).
The sample size for each group was determined based on the results of a similar study comparing the volume of residual filling materials after using ProTaper and H files [11], with a 95% confidence level (α=0.05) and a study power of 80% (β=0.2), yielding 20 samples per group.
Inclusion and exclusion criteria:
The mesiobuccal canals of maxillary and mandibular molars, and mesiolingual canals of mandibular molars, with a curvature of less than 20 degrees based on Schneider’s method [12] and no isthmus, classified as Vertucci's type 4 based on radiographic evaluation, were included [13]. Teeth with cracks, resorption defects, immature apices, or S-shaped curvature were excluded [11].
Specimen preparation:
Soft tissue and calculus were mechanically removed from the root surfaces, and the teeth were disinfected in 0.5% chloramine T solution (Merck KGaA, Darmstadt, Germany). To standardize the samples, all teeth were decoronated to ensure that the root length was consistently 18 mm. A size 10 stainless-steel K-file (Mani Inc., Tochigi, Japan) was then inserted into each root canal, with the file tip visible at the apical foramen. The working length was set to 1 mm shorter than the total root length. The roots were subsequently covered with two layers of paraffin wax (Kimia Gharb Co., Tehran, Iran), and mounted in dental gypsum (Pars Dandan, Tehran, Iran) blocks. All canals were instrumented with ProTaper NiTi rotary files (Sx, S1, S2, F1, and F2; Dentsply Maillefer, Switzerland) using a rotary endodontic motor (ENDO-MATE DT NE131; NSK, Nakanishi Inc., Tokyo, Japan) operating at 300 rpm with 3 N/cm torque, following the manufacturer's guidelines. The preparation of the apical region (apical 3 mm) was completed using a F2 file (size: 25, taper: 0.08). During each instrumentation step, the canals were irrigated with 1% NaOCl (Morvabon, Tehran, Iran), delivered via a syringe with a 30-gauge needle (NaviTip, Ultradent Products Inc., South Jordan, UT, USA). The root canals were subsequently filled with size 25 (or one size larger to match the F2 file size) gutta-percha (Dentsply Sirona, Ballaigues, Switzerland) and AH26 sealer (Dentsply Sirona, Ballaigues, Switzerland) using the lateral compaction technique, ensuring that the last gutta-percha point could not penetrate more than 5 mm into the canal. Any excess gutta-percha was removed using a heated plugger (Obtura Spartan, Algonquin, IL, USA). The obturation quality was assessed, and teeth with isthmuses were excluded from the study and replaced with new teeth. The access cavities were temporarily sealed with a cotton pellet and Cavisol temporary restorative material (Golchai Co., Tehran, Iran). To allow complete setting of the sealer, the samples were stored at 37°C and 100% humidity for 14 days. Afterwards, the temporary restoration was removed, and extra-pure chloroform (ED-430; Nik Darman, Iran) was used to soften the gutta-percha at the canal orifice [14].
Group allocation and procedure:
A total of 60 teeth were randomly assigned to three groups, each containing 20 teeth, ensuring uniform distribution in terms of canal types:
- Group 1 (retreatment with ProTaper Universal): ProTaper Retreatment files (Dentsply Maillefer, Ballaigues, Switzerland) were used at 300 rpm and 3 N/cm torque. The employed files included D1 (size: 30, length: 16 mm, taper: 9%), D2 (size: 25, length: 18 mm, taper: 8%), and D3 (size: 20, length: 22 mm, taper: 7%). The D2 file was used to the working length [5].
- Group 2 (M3 Retreatment System): M3 RT files (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland) were used at 350 rpm and 2 N/cm torque. The files included RT1 (size: 30, length: 16 mm, taper: 9%), RT2 (size: 25, length: 18 mm, taper: 8%), and RT3 (size: 20, length: 22 mm, taper: 7%). The RT2 file was used for the working length [6].
- Group 3 (Edge Endo XR Retreatment System): Edge Endo XR files (Edge Endo, Albuquerque, NM, USA) were used at speeds ranging from 300 to 500 rpm and 3 N/cm torque. The files included R1 (size: 25, length: 15 mm, taper: 12%), R2 (size: 25, length: 15 mm, taper: 8%), R3 (size: 25, length: 19 mm, taper: 6%), and R4 (size: 25, length: 23 mm, taper: 4%). The R2 file was used for the working length [7].
Each file was limited to a maximum of three uses to simulate clinical use and minimize the risk of instrument fatigue or fracture. Procedural errors, such as perforation, ledge formation, blockage, or instrument fracture, were recorded. If an instrument fractured, the tooth was excluded from the study, and the broken fragment was retrieved using a hand K file (Mani Inc., Japan). Final irrigation was performed with 5 mL of 17% EDTA (Aria Dent, Tehran, Iran) followed by 5 mL of 1% NaOCl (Morvabon, Tehran, Iran). Complete removal of the filling material was confirmed when no gutta-percha or sealer remained visible on the file flutes or during canal irrigation [5].
CBCT assessment after removal of root filling materials:
After removal of the filling material, the teeth were mounted in wax, and CBCT images were acquired using NewTom 5G CBCT scanner (QR srl, Verona, Italy) with the exposure settings of 90 kVp, 10 mA, and 8×8 cm field of view. To ensure blinding, the radiologist was unaware of the group assignments of the teeth. The CBCT images were analyzed in the axial, coronal, and sagittal sections with 1 mm slice thickness and 0.5 mm slice interval, covering the apical to coronal region of the canal, using NNT Viewer software version 6.2 (QR srl, Italy). The root length was divided into three regions of apical, middle, and coronal. The percentage of remaining filling material in each region was calculated using AutoCAD 2006 software (Autodesk Inc., San Rafael, CA, USA). This was done by measuring the canal surface area covered by residual filling material and expressing it as a percentage of the total canal surface area [15]. Additionally, radiographic images of the samples were assessed in the sagittal view with a slice thickness of 0.5 mm. The image that best displayed the entire canal length, from the orifice to the apex, at a thickness of 1 mm, was selected for analysis (Figure 1). The remaining filling material was scored using a qualitative scoring system suggested by Madani et al. [11]:
CBCT assessment after removal of root filling materials:
After removal of the filling material, the teeth were mounted in wax, and CBCT images were acquired using NewTom 5G CBCT scanner (QR srl, Verona, Italy) with the exposure settings of 90 kVp, 10 mA, and 8×8 cm field of view. To ensure blinding, the radiologist was unaware of the group assignments of the teeth. The CBCT images were analyzed in the axial, coronal, and sagittal sections with 1 mm slice thickness and 0.5 mm slice interval, covering the apical to coronal region of the canal, using NNT Viewer software version 6.2 (QR srl, Italy). The root length was divided into three regions of apical, middle, and coronal. The percentage of remaining filling material in each region was calculated using AutoCAD 2006 software (Autodesk Inc., San Rafael, CA, USA). This was done by measuring the canal surface area covered by residual filling material and expressing it as a percentage of the total canal surface area [15]. Additionally, radiographic images of the samples were assessed in the sagittal view with a slice thickness of 0.5 mm. The image that best displayed the entire canal length, from the orifice to the apex, at a thickness of 1 mm, was selected for analysis (Figure 1). The remaining filling material was scored using a qualitative scoring system suggested by Madani et al. [11]:
- Score 1: No remaining material or only a small amount on the dentinal surface (less than 25%).
- Score 2: Some debris on the dentinal surface (between 25%-50%).
- Score 3: Moderate debris on the dentinal surface (50%-75%).
- Score 4: A large amount of debris on the dentinal surface (more than 75%).
During all evaluations, no distinction was made between the filling material and the sealer.
Figure 1. CBCT cross-sections: (A) Calculation of the surface area, (B1, B2, and B3) sagittal views for qualitative scoring
{kind=link}
Statistical analysis:
Data were analyzed using SPSS version 26. Given that the data did not have a normal distribution based on the Shapiro-Wilk test result, the Kruskal-Wallis test followed by the Mann-Whitney test were used to compare the remaining filling material across the study groups. The Chi-square test was employed to assess the differences in the frequency of file fractures among the groups. A P value < 0.05 was considered statistically significant.
Results
The amount of remaining filling material in the apical, middle, and coronal thirds of the root in each group is presented in Table 1.
A statistically significant difference in the amount of remaining filling material was observed in the apical third among the groups (P=0.02). The ProTaper group exhibited the lowest, while the M3 group showed the highest. Pairwise comparisons revealed a significant difference between the ProTaper and M3 groups in the apical third (P=0.005). However, no significant differences were observed in the amount of remaining filling material among the groups in the middle (P=0.824) or coronal (P=0.282) thirds of the root canal.
File fracture frequency:
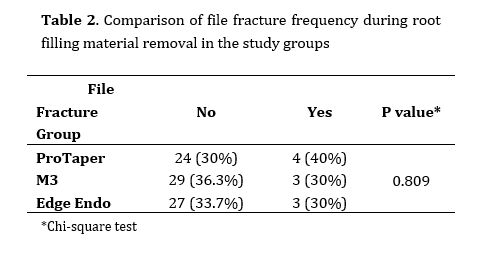
The frequency distribution of file fracture is shown in Table 2. File fracture occurred in 12% of the teeth (10 root canals), and no statistically significant difference was observed among the groups in this regard (P=0.809).
Table 1. Comparison of the percentage of remaining root filling material in the apical, middle, and coronal thirds of the roots among the study groups
Table 2. Comparison of file fracture frequency during root filling material removal in the study groups
Additionally, no apical transportation was observed in any of the samples.
Qualitative scoring of remaining filling material:
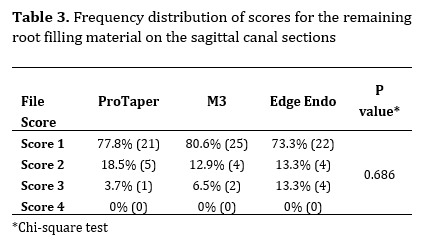
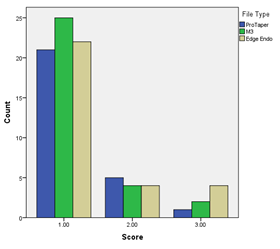
Table 3 presents the results of the qualitative scoring for the remaining root canal filling material, as assessed visually on sagittal sections. No significant differences were observed in the frequency of scoring categories among the three groups (P=0.686, Figure 2).
Table 3. Frequency distribution of scores for the remaining root filling material on the sagittal canal sections
Figure 2. Comparison of the frequency distribution of remaining root filling material scores by the file type used
Discussion
This study assessed the efficacy of three rotary retreatment systems—ProTaper, M3, and Edge Endo—in removal of root canal filling material using CBCT. The null hypothesis of the study was rejected since the results indicated a significant difference among the three file systems in the apical third, and the maximum amount of residual filling material was observed in the apical third of the root canal. Notably, the mean volume of remaining filling material in the apical third was significantly lower when the M3 system was used, as compared to ProTaper. These findings suggest that the M3 system was more effective in removing filling material from the apical third of the root canal. However, there was no statistically significant difference among the ProTaper, M3, and Edge Endo systems in terms of material removal from the middle and coronal thirds of the canal.
The superior performance of the M3 system in the apical third may be attributed to its specific design features, such as an inactive tip and a convex triangular cross-section, which enhance debris removal while reducing the tendency to transport or deviate from the canal curvature. Additionally, the M3 files are made of heat-treated NiTi alloy, offering improved flexibility and resistance to cyclic fatigue, which are essential for navigating and cleaning the curved apical areas without excessive force application [6].
Consistent with the results of the present study, Kong et al. [16] found no significant difference among the ProTaper Retreatment, Fengdu O-file, and M3-RT systems in terms of cleaning the root canal. However, the M3-RT system performed better overall. Similarly, Abdelnaby et al. [17] reached comparable conclusions in their study, comparing three file systems of Reciproc Blue, Hyflex EDM, and ProTaper, highlighting similar trends in effectiveness.
In the present study, the highest amount of remaining filling material was observed in the ProTaper group. This finding aligns with the results of Aly et al. [18], who assessed the removal of gutta-percha using ProTaper-D, R-ENDO, and MTwo-R files. The ProTaper Retreatment files have a progressively increasing taper and greater core diameter, which reduces flexibility. This reduced flexibility may hinder adaptation to the canal curvature, especially in the apical third, leading to incomplete removal of filling materials. The aggressive cutting action of the ProTaper files may also push softened gutta-percha apically rather than removing it effectively. Similar results regarding the higher volume of residual filling material with ProTaper Retreatment files have been reported by Madani et al. [11] and Ali et al. [19].
Edge Endo files, while also heat-treated, have a greater taper in their initial instruments (R1 and R2) and a relatively short working length. Such design features may contribute to variable performance in deeper canal regions. Although more flexible than ProTaper, their larger tip diameters in initial files might cause resistance in narrow apical areas.
Many researchers have reported that rotary instruments tend to push materials toward the apical region of the canal, regardless of the evaluation method used [20, 21]. This pushing effect is likely due to the rotary motion and helical design of the files, which can compact rather than remove gutta-percha and sealer when not accompanied by proper irrigation and solvent use. Additionally, the apical pressure applied to facilitate file penetration and solvent action may influence the amount of apically extruded debris. In a comparison of three file systems—TruNatomy, ProTaper, and RaCa—Akshay et al. [22] found that while TruNatomy exhibited the best performance in removing root canal filling material, it also caused the highest apical extrusion of debris.
In contrast to the present findings, Khedmat et al. [4] reported a statistically significant difference between the Mtwo R and ProTaper R systems in removing filling material using CBCT. In their study, the volume of residual filling material was lower with the ProTaper R system compared to Mtwo R. They attributed this result to the length and progressive taper of the ProTaper files. Anatomical differences and variations in the initial preparation technique could explain the discrepancies in the results. In the present study, the use of multi-rooted molars with up to 20-degree curvature introduced greater anatomical complexity, better reflecting clinical retreatment scenarios.
Some authors such as Atique et al. [23] found no significant difference in the efficacy of hand files and rotary files for gutta-percha removal. However, several other studies concluded that rotary file systems were generally more effective than hand files for this purpose [24-28]. Bramante et al. [29] attributed the advantage of rotary systems to the plasticizing effect of gutta-percha during file use, which facilitates easier removal of the filling material. However, this softened state may paradoxically increase the adhesion of gutta-percha and sealer to dentin, especially in curved canals or under-compacted obturations, which could account for the persistent presence of filling material despite rotary use [30].
In the present study, all the retreatment files left some filling material within the canal. This finding is consistent with previous studies that used various instruments, techniques, and solvents for retreatment [4, 15, 20, 21, 31, 32]. Instead of employing longitudinal sections, which could potentially displace material during sectioning and alter the tooth structure, sagittal CBCT sections were utilized in the present study. The results showed no statistically significant difference in the frequency of scores among the three file systems. This suggests that, while some systems may have quantitative advantages, they are not substantially superior when evaluated qualitatively. CBCT enables a more reliable and non-invasive assessment of residual filling material compared to destructive sectioning methods.
Chloroform is widely regarded as the most effective solvent for dissolving gutta-percha [20]. In the present study, 1-2 drops of chloroform were applied to the root canal orifice for one minute to soften the gutta-percha and facilitate the use of retreatment files. However, softened gutta-percha becomes more viscous, and may adhere more tenaciously to canal walls, particularly in oval or curved regions, making mechanical removal less predictable.
AH26 is a desirable choice for root canal sealing due to its antimicrobial properties, good adhesion to both gutta-percha and canal wall, long working time, easy mixing, and excellent sealing ability [33]. In a study by Kosti et al. [34], which assessed the removal of gutta-percha from endodontically treated teeth using four types of sealers (AH26, Roth 811, Endo-In, and RoeKaseal) with both manual and rotary techniques, residual sealer was found on the canal walls in all cases. The results showed no significant difference in the coronal third, but more residual filling material remained in the middle and apical thirds when AH26 sealer was used. The properties of the sealer, including adhesion to dentin and gutta-percha, the ability to penetrate dentinal tubules, layer thickness, dimensional changes, and solubility, may have made the removal process more difficult, particularly in the apical third.
Ni-Ti files are renowned for their exceptional elasticity, which allows for more precise canal preparation, and reduces the occurrence of aberrations. Despite their good flexibility, file fracture remains a significant concern [35]. In the present study, file fracture occurred in all three groups, although the frequency of fractures did not significantly differ among them. This outcome may be explained by similar usage limits (maximum of three uses) and similar torque/speed settings across groups, minimizing the influence of fatigue failure. The high taper of rotary files, coupled with the low radius of curvature in root canals, may contribute to instrument fracture. Another study also reported a higher risk of rotary instrument fracture compared to manual files [36].
The discrepancies in the results of various studies evaluating the effectiveness of different files in removing root canal filling material may stem from differences in sample sizes, tooth types, obturation techniques, retreatment methods, and limitations in evaluation protocols. The present study’s limitations may affect the generalizability of its findings. Being an ex-vivo investigation, it did not fully replicate clinical conditions, such as anatomical variability, patient-related factors, or operator differences. The use of one single sealer (AH26) and one obturation technique (cold lateral compaction) may also limit applicability to other clinical scenarios. While CBCT provided a non-destructive assessment, it may have limitations in distinguishing between sealer and gutta-percha or detecting very small residual volumes. Ultimately, understanding the interaction between file design, sealer type, canal anatomy, and retreatment strategy is essential for optimizing clinical outcomes. To address these limitations, future studies should include a wider range of root anatomies, obturation materials, and solvents, along with larger sample sizes and clinical trials. Evaluating canal transportation, dentin preservation, and long-term outcomes would also help optimize the safety and effectiveness of rotary retreatment systems in clinical practice.
Conclusion
The result of the present study showed that none of the rotary retreatment files used in this study were able to completely remove the root canal filling material, with some material always remaining after retreatment. However, the M3 retreatment files exhibited superior efficiency in cleaning the apical third of the root canal.
File fracture frequency:
The frequency distribution of file fracture is shown in Table 2. File fracture occurred in 12% of the teeth (10 root canals), and no statistically significant difference was observed among the groups in this regard (P=0.809).
Table 1. Comparison of the percentage of remaining root filling material in the apical, middle, and coronal thirds of the roots among the study groups
{kind=link}
Table 2. Comparison of file fracture frequency during root filling material removal in the study groups
{kind=link}
Additionally, no apical transportation was observed in any of the samples.
Qualitative scoring of remaining filling material:
Table 3 presents the results of the qualitative scoring for the remaining root canal filling material, as assessed visually on sagittal sections. No significant differences were observed in the frequency of scoring categories among the three groups (P=0.686, Figure 2).
Table 3. Frequency distribution of scores for the remaining root filling material on the sagittal canal sections
{kind=link}
Figure 2. Comparison of the frequency distribution of remaining root filling material scores by the file type used
{kind=link}
Discussion
This study assessed the efficacy of three rotary retreatment systems—ProTaper, M3, and Edge Endo—in removal of root canal filling material using CBCT. The null hypothesis of the study was rejected since the results indicated a significant difference among the three file systems in the apical third, and the maximum amount of residual filling material was observed in the apical third of the root canal. Notably, the mean volume of remaining filling material in the apical third was significantly lower when the M3 system was used, as compared to ProTaper. These findings suggest that the M3 system was more effective in removing filling material from the apical third of the root canal. However, there was no statistically significant difference among the ProTaper, M3, and Edge Endo systems in terms of material removal from the middle and coronal thirds of the canal.
The superior performance of the M3 system in the apical third may be attributed to its specific design features, such as an inactive tip and a convex triangular cross-section, which enhance debris removal while reducing the tendency to transport or deviate from the canal curvature. Additionally, the M3 files are made of heat-treated NiTi alloy, offering improved flexibility and resistance to cyclic fatigue, which are essential for navigating and cleaning the curved apical areas without excessive force application [6].
Consistent with the results of the present study, Kong et al. [16] found no significant difference among the ProTaper Retreatment, Fengdu O-file, and M3-RT systems in terms of cleaning the root canal. However, the M3-RT system performed better overall. Similarly, Abdelnaby et al. [17] reached comparable conclusions in their study, comparing three file systems of Reciproc Blue, Hyflex EDM, and ProTaper, highlighting similar trends in effectiveness.
In the present study, the highest amount of remaining filling material was observed in the ProTaper group. This finding aligns with the results of Aly et al. [18], who assessed the removal of gutta-percha using ProTaper-D, R-ENDO, and MTwo-R files. The ProTaper Retreatment files have a progressively increasing taper and greater core diameter, which reduces flexibility. This reduced flexibility may hinder adaptation to the canal curvature, especially in the apical third, leading to incomplete removal of filling materials. The aggressive cutting action of the ProTaper files may also push softened gutta-percha apically rather than removing it effectively. Similar results regarding the higher volume of residual filling material with ProTaper Retreatment files have been reported by Madani et al. [11] and Ali et al. [19].
Edge Endo files, while also heat-treated, have a greater taper in their initial instruments (R1 and R2) and a relatively short working length. Such design features may contribute to variable performance in deeper canal regions. Although more flexible than ProTaper, their larger tip diameters in initial files might cause resistance in narrow apical areas.
Many researchers have reported that rotary instruments tend to push materials toward the apical region of the canal, regardless of the evaluation method used [20, 21]. This pushing effect is likely due to the rotary motion and helical design of the files, which can compact rather than remove gutta-percha and sealer when not accompanied by proper irrigation and solvent use. Additionally, the apical pressure applied to facilitate file penetration and solvent action may influence the amount of apically extruded debris. In a comparison of three file systems—TruNatomy, ProTaper, and RaCa—Akshay et al. [22] found that while TruNatomy exhibited the best performance in removing root canal filling material, it also caused the highest apical extrusion of debris.
In contrast to the present findings, Khedmat et al. [4] reported a statistically significant difference between the Mtwo R and ProTaper R systems in removing filling material using CBCT. In their study, the volume of residual filling material was lower with the ProTaper R system compared to Mtwo R. They attributed this result to the length and progressive taper of the ProTaper files. Anatomical differences and variations in the initial preparation technique could explain the discrepancies in the results. In the present study, the use of multi-rooted molars with up to 20-degree curvature introduced greater anatomical complexity, better reflecting clinical retreatment scenarios.
Some authors such as Atique et al. [23] found no significant difference in the efficacy of hand files and rotary files for gutta-percha removal. However, several other studies concluded that rotary file systems were generally more effective than hand files for this purpose [24-28]. Bramante et al. [29] attributed the advantage of rotary systems to the plasticizing effect of gutta-percha during file use, which facilitates easier removal of the filling material. However, this softened state may paradoxically increase the adhesion of gutta-percha and sealer to dentin, especially in curved canals or under-compacted obturations, which could account for the persistent presence of filling material despite rotary use [30].
In the present study, all the retreatment files left some filling material within the canal. This finding is consistent with previous studies that used various instruments, techniques, and solvents for retreatment [4, 15, 20, 21, 31, 32]. Instead of employing longitudinal sections, which could potentially displace material during sectioning and alter the tooth structure, sagittal CBCT sections were utilized in the present study. The results showed no statistically significant difference in the frequency of scores among the three file systems. This suggests that, while some systems may have quantitative advantages, they are not substantially superior when evaluated qualitatively. CBCT enables a more reliable and non-invasive assessment of residual filling material compared to destructive sectioning methods.
Chloroform is widely regarded as the most effective solvent for dissolving gutta-percha [20]. In the present study, 1-2 drops of chloroform were applied to the root canal orifice for one minute to soften the gutta-percha and facilitate the use of retreatment files. However, softened gutta-percha becomes more viscous, and may adhere more tenaciously to canal walls, particularly in oval or curved regions, making mechanical removal less predictable.
AH26 is a desirable choice for root canal sealing due to its antimicrobial properties, good adhesion to both gutta-percha and canal wall, long working time, easy mixing, and excellent sealing ability [33]. In a study by Kosti et al. [34], which assessed the removal of gutta-percha from endodontically treated teeth using four types of sealers (AH26, Roth 811, Endo-In, and RoeKaseal) with both manual and rotary techniques, residual sealer was found on the canal walls in all cases. The results showed no significant difference in the coronal third, but more residual filling material remained in the middle and apical thirds when AH26 sealer was used. The properties of the sealer, including adhesion to dentin and gutta-percha, the ability to penetrate dentinal tubules, layer thickness, dimensional changes, and solubility, may have made the removal process more difficult, particularly in the apical third.
Ni-Ti files are renowned for their exceptional elasticity, which allows for more precise canal preparation, and reduces the occurrence of aberrations. Despite their good flexibility, file fracture remains a significant concern [35]. In the present study, file fracture occurred in all three groups, although the frequency of fractures did not significantly differ among them. This outcome may be explained by similar usage limits (maximum of three uses) and similar torque/speed settings across groups, minimizing the influence of fatigue failure. The high taper of rotary files, coupled with the low radius of curvature in root canals, may contribute to instrument fracture. Another study also reported a higher risk of rotary instrument fracture compared to manual files [36].
The discrepancies in the results of various studies evaluating the effectiveness of different files in removing root canal filling material may stem from differences in sample sizes, tooth types, obturation techniques, retreatment methods, and limitations in evaluation protocols. The present study’s limitations may affect the generalizability of its findings. Being an ex-vivo investigation, it did not fully replicate clinical conditions, such as anatomical variability, patient-related factors, or operator differences. The use of one single sealer (AH26) and one obturation technique (cold lateral compaction) may also limit applicability to other clinical scenarios. While CBCT provided a non-destructive assessment, it may have limitations in distinguishing between sealer and gutta-percha or detecting very small residual volumes. Ultimately, understanding the interaction between file design, sealer type, canal anatomy, and retreatment strategy is essential for optimizing clinical outcomes. To address these limitations, future studies should include a wider range of root anatomies, obturation materials, and solvents, along with larger sample sizes and clinical trials. Evaluating canal transportation, dentin preservation, and long-term outcomes would also help optimize the safety and effectiveness of rotary retreatment systems in clinical practice.
Conclusion
The result of the present study showed that none of the rotary retreatment files used in this study were able to completely remove the root canal filling material, with some material always remaining after retreatment. However, the M3 retreatment files exhibited superior efficiency in cleaning the apical third of the root canal.
Type of Study: Original article |
Subject:
Endodontics
References
1. de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study-phase 4: initial treatment. J Endod. 2008 Mar;34(3):258-63. [DOI:10.1016/j.joen.2007.10.017] [PMID]
2. Takahashi CM, Cunha RS, de Martin AS, Fontana CE, Silveira CF, da Silveira Bueno CE. In vitro evaluation of the effectiveness of ProTaper universal rotary retreatment system for gutta-percha removal with or without a solvent. J Endod. 2009 Nov;35(11):1580-3. [DOI:10.1016/j.joen.2009.07.015] [PMID]
3. Yadav P, Bharath MJ, Sahadev CK, Makonahalli Ramachandra PK, Rao Y, Ali A, et al. An in vitro CT comparison of gutta-percha removal with two rotary systems and hedstrom files. Iran Endod J. 2013 May;8(2):59-64.
4. Khedmat S, Azari A, Shamshiri AR, Fadae M, Fakhar HB. Efficacy of ProTaper and Mtwo retreatment files in removal of gutta-percha and GuttaFlow from root canals. Iran Endod J. 2016 May;11(3):184.
5. Bashar F, Bashar AK, Khan MM, Hasin A, Asaduszaman M, Hossain M. Evaluation of obturating material removal from root canal by hedstrom and rotary retreatment file. EJDENT. 2024 Mar;5(2):1-8. [DOI:10.24018/ejdent.2024.5.2.320]
6. Hawwash MM. Efficacy of retreatment in single-rooted mandibular premolars obturated with a novel Bioceramic sealer with two different filling techniques (A comparative in-vitro study).Protoc Exch. 2024 May ;44(4)238-48. [DOI:10.21203/rs.3.pex-2634/v1]
7. Srirama S, Chandrasekaran S, Arul B, Natanasabapathy V. Comparative evaluation of removal of gutta percha and bioceramic sealer using EdgeFile-XR and ProTaper Universal retreatment files: Micro-computed tomography study. Aust Endod J. 2025 May;51(2):358-68. [DOI:10.1111/aej.12949] [PMID]
8. Kfir A, Tsesis I, Yakirevich E, Matalon S, Abramovitz I. The efficacy of five techniques for removing root filling material: microscopic versus radiographic evaluation. Int Endod J. 2012 Jan;45(1):35-41. [DOI:10.1111/j.1365-2591.2011.01944.x] [PMID]
9. Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch Oral Biol. 2016 Jan;61:130-7. [DOI:10.1016/j.archoralbio.2015.10.020] [PMID]
10. Yilmaz F, Sonmez G, Kamburoglu K, Koc C, Ocak M, Celik HH. Accuracy of CBCT images in the volumetric assessment of residual root canal filling material: Effect of voxel size. Niger J Clin Pract. 2019 Aug;22(8):1091-8. [DOI:10.4103/njcp.njcp_678_18] [PMID]
11. Madani ZS, Simdar N, Moudi E, Bijani A. CBCT evaluation of the root canal filling removal using D-RaCe, ProTaper Retreatment Kit and hand files in curved canals. Iran Endod J. 2014 Dec;10(1):69-74.
12. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971 Aug;32(2):271-5. [DOI:10.1016/0030-4220(71)90230-1] [PMID]
13. Yanık D, Özel Ş. Shaping ability of three instrumentation system in moderately curved canals: A micro-CT study. Microsc Res Tech. 2024 Oct;87(10):2399-407. [DOI:10.1002/jemt.24613] [PMID]
14. Atmeh AR, Alshaiji D, Abdunabi F, Alamri M, Khamis AH. Comparing the softening effect of three gutta-percha solvents on different types of gutta-percha with different application durations. Saudi Dent J. 2024 Feb;36(2):281-5. [DOI:10.1016/j.sdentj.2023.10.025] [PMID] [PMCID]
15. Tejaswi S, Singh A, Manglekar S, Ambikathanaya UK, Shetty S. Evaluation of dentinal crack propagation, amount of gutta percha remaining and time required during removal of gutta percha using two different rotary instruments and hand instruments - An In vitro study. Niger J Clin Pract. 2022 Apr;25(4):524-30. [DOI:10.4103/njcp.njcp_1838_21] [PMID]
16. Kong J, Li C, Yin L, Dai X. Experimental study on central location ability and clearance rate of three nickel-titanium instruments for root canal retreatment. J Prev Treat Stomatol Dis. 2020:494-8.
17. Abdelnaby P, Ibrahim M, ElBackly R. In vitro evaluation of filling material removal and apical debris extrusion after retreatment using Reciproc blue, Hyflex EDM and ProTaper retreatment files. BMC Oral Health. 2023 Nov;23(1):902. [DOI:10.1186/s12903-023-03579-7] [PMID] [PMCID]
18. Aly AM, Abdallah AM, El Backly RM. Efficacy of three different retreatment file systems for gutta-percha removal using cone beam computed tomography. Alex Dent J. 2020 Dec;45(3):23-8.
19. Ali SM, Pradeep P, Paul S, Jhons DA, Ganesh Prasad B. Comparative evaluation of efficiency and time of gutta percha removal using hedstrom files, protaper retreatment and rendo files-an ex vivo study. J Evid Based Med Healthc. 2015;2(49):8484-87. [DOI:10.18410/jebmh/2015/1161] [PMID]
20. AbdelWahed A. Effect of different gutta-percha solvents on bond strength of AH Plus sealer to root canal dentin following retreatment. Egypt Dent J. 2022 Apr;68(2):1927-35. [DOI:10.21608/edj.2022.116091.1948]
21. Radeva E, Marinova-Takorova M, Kisjova I, Naseva E. Comparison of the time required for removal of bioceramic sealer and gutta-percha with different techniques. Int J Sci Res. 2018 Mar;7(3):1309-12.
22. Akshay VA, Srirekha A, Reddy J, Champa C, Shetty A, Srinivasan A. Evaluation of the efficacy of TruNatomy, ProTaper retreatment, and RaCe file systems in retreatment of moderately curved mandibular molars: An in vitro study. J Conserv Dent Endod. 2023 Jul;26(4):383-7.
23. Atique S, Ali K, Haroon S, Ahmed A, Javed MQ, Zafar MS, et al. Effectiveness of H-files and Pro-Taper universal systems in removing gutta-percha during endodontic retreatment: A comparative study. J Taibah Univ Med Sci. 2024 Jun;19(3):537-44. [DOI:10.1016/j.jtumed.2024.04.002] [PMID] [PMCID]
24. Giuliani V, Cocchetti R, Pagavino G. Efficacy of ProTaper universal retreatment files in removing filling materials during root canal retreatment. J Endod. 2008 Nov;34(11):1381-4. [DOI:10.1016/j.joen.2008.08.002] [PMID]
25. Joseph M, Ahlawat J, Malhotra A, Rao M, Sharma A, Talwar S. In vitro evaluation of efficacy of different rotary instrument systems for gutta percha removal during root canal retreatment. J Clin Exp Dent. 2016 Oct;8(4):e355-60. [DOI:10.4317/jced.52488] [PMID] [PMCID]
26. Mittal R, Singla MG, Garg A, Dhawan A. A comparison of apical bacterial extrusion in manual, ProTaper rotary, and One Shape rotary instrumentation techniques. J Endod. 2015 Dec;41(12):2040-4. [DOI:10.1016/j.joen.2015.09.002] [PMID]
27. Reddy NV, Done V. A clinical comparison of instrumentation time, obturation time and radiographic quality of obturation using the rotary and manual file system for pulpectomy in primary molars.Int J Pedo Rehab. 2024;9(1);70-80. [DOI:10.56501/intjpedorehab.v9i1.1089]
28. Somma F, Cammarota G, Plotino G, Grande NM, Pameijer CH. The effectiveness of manual and mechanical instrumentation for the retreatment of three different root canal filling materials. J Endod. 2008 Apr;34(4):466-9. [DOI:10.1016/j.joen.2008.02.008] [PMID]
29. Bramante CM, Fidelis NS, Assumpção TS, Bernardineli N, Garcia RB, Bramante AS, et al. Heat release, time required, and cleaning ability of MTwo R and ProTaper universal retreatment systems in the removal of filling material. J Endod. 2010 Nov;36(11):1870-3. [DOI:10.1016/j.joen.2010.08.013] [PMID]
30. Bhagavaldas MC, Diwan A, Kusumvalli S, Pasha S, Devale M, Chava DC. Efficacy of two rotary retreatment systems in removing gutta-percha and sealer during endodontic retreatment with or without solvent: A comparative in vitro study. J Conserv Dent. 2017 Jan;20(1):12-6. [DOI:10.4103/0972-0707.209075] [PMID] [PMCID]
31. Purba R, Sonarkar SS, Podar R, Singh S, Babel S, Kulkarni G. Comparative evaluation of retreatment techniques by using different file systems from oval-shaped canals. J Conserv Dent. 2020 Jan;23(1):91-6. [DOI:10.4103/JCD.JCD_167_20] [PMID] [PMCID]
32. Sameh R, Omaia M. The efficacy of two novel retreatment systems in the removal of root canal obturating materials (an in vitro study). Open Access Maced J Med Sci. 2022 Jan;10(D):76-82. [DOI:10.3889/oamjms.2022.8112]
33. Torabinejad M, Fouad AF, Shabahang S. Endodontics E-Book: Endodontics E-Book. Elsevier Health Sciences; 2020 Jun;14:303-5.
34. Kosti E, Lambrianidis T, Economides N, Neofitou C. Ex vivo study of the efficacy of H-files and rotary Ni-Ti instruments to remove gutta-percha and four types of sealer. Int Endod J. 2006 Jan;39(1):48-54. [DOI:10.1111/j.1365-2591.2005.01046.x] [PMID]
35. Bergmans L, Van Cleynenbreugel J, Wevers M, Lambrechts P. Mechanical root canal preparation with NiTi rotary instruments: rationale, performance and safety. Status report for the American Journal of Dentistry. Am J Dent. 2001 Oct;14(5):324-33.
36. Berman LH, Hargreaves KM. Cohen's pathways of the pulp expert consult. Elsevier Health Sciences; 2015 Oct;6;203-9.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |