Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 3 (9-2025)
J Res Dent Maxillofac Sci 2025, 10(3): 168-175 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Guha P, Priscilla Antony D, Solete P, Arun N. Comparison of Remaining Dentin Thickness, Canal Transportation, and Canal Centering Ratio Using Three Different Rotary File Systems: A Cone-Beam Computed Tomography Analysis. J Res Dent Maxillofac Sci 2025; 10 (3) :168-175
URL: http://jrdms.dentaliau.ac.ir/article-1-821-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-821-en.html



1- Postgraduate Resident, Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science (SIMATS) Saveetha University, Chennai, India.
2- Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science (SIMATS) Saveetha University, Chennai, India. ,delphy.priscilla@gmail.com
3- Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science (SIMATS) Saveetha University, Chennai, India.
2- Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science (SIMATS) Saveetha University, Chennai, India. ,
3- Department of Conservative Dentistry and Endodontics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science (SIMATS) Saveetha University, Chennai, India.
Full-Text [PDF 693 kb]
(848 Downloads)
| Abstract (HTML) (2087 Views)
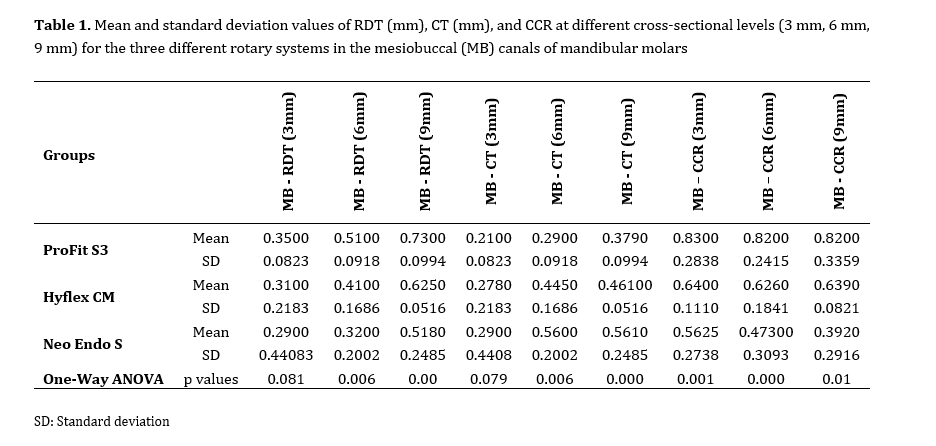
Table 1. Mean and standard deviation values of RDT (mm), CT (mm), and CCR at different cross-sectional levels (3 mm, 6 mm, 9 mm) for the three different rotary systems in the mesiobuccal (MB) canals of mandibular molars
Table 2. Mean and standard deviation values of RDT (mm), CT (mm), and CCR at 3, 6, and 9 mm from the apex for three different rotary systems in the mesiolingual (ML) canals of mandibular molars
Discussion
Full-Text: (401 Views)
Abstract
Background and Aim: This study evaluated the remaining dentin thickness (RDT), canal transportation (CT), and canal centering ratio (CCR) of three different rotary file systems using cone-beam computed tomography (CBCT).
Materials and Methods: In this in vitro study, 153 extracted mandibular molars were evaluated. The working length was determined using CBCT before starting the experiment. A skilled dentist then prepared the root canals using three types of rotary files: ProFit S3, HyFLEX CM, and NeoEndo S. Pre- and post-treatment CBCT scans were analyzed to compare the results. One-way ANOVA and Tukey test were used for statistical analysis.
Results: ProFit S3 demonstrated a superior performance in preserving dentin thickness and maintaining canal geometry compared to HyFlex CM and NeoEndo S. In both MB and ML canals, at 6 mm and 9 mm, ProFit S3 exhibited significantly higher RDT (P≤0.007), less CT (P≤0.006), and better CCR (P≤0.01) than other systems. Among the remaining systems, HyFlex CM performed better than NeoEndo S for RDT and CT at these levels. At 3 mm, no significant differences were found for RDT or CT; however, ProFit S3 showed significantly better CCR than NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
Conclusion: Among the tested systems, ProFit S3 resulted in the least change in canal volume, suggesting that it may be better at preserving the original shape of the root canal, as well as the surrounding dentin, compared to Hyflex CM and NeoEndo S.
Keywords: Cone-Beam Computed Tomography; Endodontics; In Vitro Techniques; Root Canal Preparation
Introduction
Materials and Methods: In this in vitro study, 153 extracted mandibular molars were evaluated. The working length was determined using CBCT before starting the experiment. A skilled dentist then prepared the root canals using three types of rotary files: ProFit S3, HyFLEX CM, and NeoEndo S. Pre- and post-treatment CBCT scans were analyzed to compare the results. One-way ANOVA and Tukey test were used for statistical analysis.
Results: ProFit S3 demonstrated a superior performance in preserving dentin thickness and maintaining canal geometry compared to HyFlex CM and NeoEndo S. In both MB and ML canals, at 6 mm and 9 mm, ProFit S3 exhibited significantly higher RDT (P≤0.007), less CT (P≤0.006), and better CCR (P≤0.01) than other systems. Among the remaining systems, HyFlex CM performed better than NeoEndo S for RDT and CT at these levels. At 3 mm, no significant differences were found for RDT or CT; however, ProFit S3 showed significantly better CCR than NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
Conclusion: Among the tested systems, ProFit S3 resulted in the least change in canal volume, suggesting that it may be better at preserving the original shape of the root canal, as well as the surrounding dentin, compared to Hyflex CM and NeoEndo S.
Keywords: Cone-Beam Computed Tomography; Endodontics; In Vitro Techniques; Root Canal Preparation
Introduction
The cleaning and shaping mechanisms in endodontic treatment are critical for eliminating microorganisms from the root canal while preserving its original size and shape to ensure effective treatment outcomes [1]. During biomechanical preparation, it is essential to maintain the root canal’s dimensions close to the original values to avoid excessive dentin removal or canal transportation; thereby, preserving the canal’s anatomy [2]. Root canals are typically complex, often featuring curvatures and angulations, especially in molars and premolars [3]. Both hand filing and rotary files can alter canal morphology, and significant changes may lead to issues such as ledge formation, zipping, or canal transportation [4].
Insufficient analysis of canal morphology may result in residual bacteria due to incomplete cleaning and shaping [5]. Instrumentation can induce changes in canal morphology, including wall alterations, apical enlargement, and canal transportation, which can compromise tooth structure integrity and treatment outcomes [6]. Proper biomechanical preparation depends on selecting a file system that preserves canal morphology and prevents excessive dentin removal or canal transportation [7]. Factors such as file tip design, taper, torque, and speed are essential for successful endodontic procedures [8]. Nickel-titanium (NiTi) rotary files, known for their flexibility, shape memory, and efficiency, have transformed endodontic practices, with brands like ProTaper Gold, Hyflex CM by Coltene, and TruAnatomy offering various options in the market [9].
Hyflex CM NiTi rotary files (Coltene, Switzerland) are made of Niti alloy with a controlled memory heat treatment [10]. These files were manufactured via a method that increases the flexibility and fracture resistance of the file systems by changing the NiTi alloy configuration at room temperature from austenite to martensite. They are available in 21 mm and 25 mm lengths. The file system consists of 6 files, starting with the orifice enlarger of 25/0.8 followed by 20/0.4, 25/0.4, 20/0.6, 30/0.4, and 40/0.4. NeoEndo S rotary files (Eighteenth Orikam, India) have an S-shaped cross-section and sharper flutes for greater cutting efficiency. They are available in a set of 6 files - a coronal flaring file of 8% in 19 mm length, followed by 17/4, 20/4, 25/4, 20/6, and 25/6 files in either 21 mm or 25 mm length. This system also uses the NiTi alloy system, which renders excellent flexibility. It also has a safety non-cutting tip, which minimizes the chances of ledge formation [11]. ProFit S3 (PS3) rotary file (ProFit Dental, India) is a patented file system that makes use of blue heat technology. This file system reduces the possibility of apical debris extrusion by having a variable taper design with a rectangular cross-section and two-point contact. There is one orifice opener and three finishing files in this file system. The files are PF1 (yellow), PF2 (red), PF3 (blue), and P0, which is the orifice opener. The taper levels in each of these files range from 4% to 8% with variable taper [12].
Remaining dentin thickness (RDT) is the amount of dentin that is preserved after biomechanical preparation. If the RDT is very low, the chances of fracture are high [14]. Canal centering ability (CCR) is a ratio that indicates how well the canal maintains its original path. The higher the ratio, the better the canal centering ability [15]. Canal transportation (CT) refers to the unintentional transportation of the apical foramen from its original location [16]. CT leads to increased chances of iatrogenic apical periodontitis [17].
Cone-beam computed tomography (CBCT) has been advocated as a gold standard for analysis of root canal morphology before and after treatment, as it provides a three-dimensional observation and is non-destructive in nature [13].
Thus, this study aimed to analyze three different rotary file systems namely Hyflex CM, NeoEndo S, and ProFit S3 rotary files in terms of RDT, CT, and CCR.
Materials and Methods
Insufficient analysis of canal morphology may result in residual bacteria due to incomplete cleaning and shaping [5]. Instrumentation can induce changes in canal morphology, including wall alterations, apical enlargement, and canal transportation, which can compromise tooth structure integrity and treatment outcomes [6]. Proper biomechanical preparation depends on selecting a file system that preserves canal morphology and prevents excessive dentin removal or canal transportation [7]. Factors such as file tip design, taper, torque, and speed are essential for successful endodontic procedures [8]. Nickel-titanium (NiTi) rotary files, known for their flexibility, shape memory, and efficiency, have transformed endodontic practices, with brands like ProTaper Gold, Hyflex CM by Coltene, and TruAnatomy offering various options in the market [9].
Hyflex CM NiTi rotary files (Coltene, Switzerland) are made of Niti alloy with a controlled memory heat treatment [10]. These files were manufactured via a method that increases the flexibility and fracture resistance of the file systems by changing the NiTi alloy configuration at room temperature from austenite to martensite. They are available in 21 mm and 25 mm lengths. The file system consists of 6 files, starting with the orifice enlarger of 25/0.8 followed by 20/0.4, 25/0.4, 20/0.6, 30/0.4, and 40/0.4. NeoEndo S rotary files (Eighteenth Orikam, India) have an S-shaped cross-section and sharper flutes for greater cutting efficiency. They are available in a set of 6 files - a coronal flaring file of 8% in 19 mm length, followed by 17/4, 20/4, 25/4, 20/6, and 25/6 files in either 21 mm or 25 mm length. This system also uses the NiTi alloy system, which renders excellent flexibility. It also has a safety non-cutting tip, which minimizes the chances of ledge formation [11]. ProFit S3 (PS3) rotary file (ProFit Dental, India) is a patented file system that makes use of blue heat technology. This file system reduces the possibility of apical debris extrusion by having a variable taper design with a rectangular cross-section and two-point contact. There is one orifice opener and three finishing files in this file system. The files are PF1 (yellow), PF2 (red), PF3 (blue), and P0, which is the orifice opener. The taper levels in each of these files range from 4% to 8% with variable taper [12].
Remaining dentin thickness (RDT) is the amount of dentin that is preserved after biomechanical preparation. If the RDT is very low, the chances of fracture are high [14]. Canal centering ability (CCR) is a ratio that indicates how well the canal maintains its original path. The higher the ratio, the better the canal centering ability [15]. Canal transportation (CT) refers to the unintentional transportation of the apical foramen from its original location [16]. CT leads to increased chances of iatrogenic apical periodontitis [17].
Cone-beam computed tomography (CBCT) has been advocated as a gold standard for analysis of root canal morphology before and after treatment, as it provides a three-dimensional observation and is non-destructive in nature [13].
Thus, this study aimed to analyze three different rotary file systems namely Hyflex CM, NeoEndo S, and ProFit S3 rotary files in terms of RDT, CT, and CCR.
Materials and Methods
Sample size calculation:
In this in vitro study, the sample size was determined using the G Power 3.1.9.7 algorithm, taking into account a previous study [18]. A total sample size of 153 was determined, achieving a power of 95% (1- β=95%, α=0.05).
The specimens were randomly distributed into three groups for experimentation. Ethical clearance for the current study was granted from the Institutional Human Ethical Committee for Dental Research with the approval number SRB/SDC/ENDO-2303/24/266. Specimen preparation:
This study included cleaning and shaping of the mesiolingual and mesiobuccal canals of 153 extracted mandibular first molars. The teeth had been extracted for purposes not related to this study. The assessment was carried out using CBCT. CareStream 3D Imaging version V3.10.21 software was used to obtain preoperative and postoperative CBCT scans of the specimens, which were obtained with 120 KV voltage and 5 mA power for 12 seconds with a dose of 642 mGy.cm2 and 300 μm voxel size. Preoperative CBCT scans were used to assess any defects present in the extracted teeth. Teeth with defects such as calcification, internal or external root resorption, and signs of previously attempted root canal treatment were excluded, and only teeth with intact root canal morphology were included in the study. In order to standardize the methodology, the extracted teeth were decoronated using a diamond disc (3M, India Diamond Cloth Disc 674W, India) with roots up to 16 mm in length (Figure 1). The extracted teeth were stored in saline (Baxter India Pvt Ltd) before use. The access cavity was created with an Endo Access bur size 2 (Dentsply Maillefer, Switzerland), and the canal patency was verified up to the working length using a #10 K-file (Mani, Utsunomiya, Tochigi, Japan). Also, 5.25% sodium hypochlorite (Acquafarma Farmácia, Niteroi, RJ, Brazil) was used for irrigating the prepared root canal space [9,19]. Teeth were randomly divided with the help of computer-generated numbers into three groups of 51 teeth each. The teeth in all three groups were mounted in a U-shaped rim made of modeling wax that mimicked the mandibular arch.
Group 1: ProFit S3 (ProFit Dental, India)
Group 2: HyFlex CM (Coltene, Switzerland)
Group 3: NeoEndo S (Eighteenth Orikam, India)
In this in vitro study, the sample size was determined using the G Power 3.1.9.7 algorithm, taking into account a previous study [18]. A total sample size of 153 was determined, achieving a power of 95% (1- β=95%, α=0.05).
The specimens were randomly distributed into three groups for experimentation. Ethical clearance for the current study was granted from the Institutional Human Ethical Committee for Dental Research with the approval number SRB/SDC/ENDO-2303/24/266. Specimen preparation:
This study included cleaning and shaping of the mesiolingual and mesiobuccal canals of 153 extracted mandibular first molars. The teeth had been extracted for purposes not related to this study. The assessment was carried out using CBCT. CareStream 3D Imaging version V3.10.21 software was used to obtain preoperative and postoperative CBCT scans of the specimens, which were obtained with 120 KV voltage and 5 mA power for 12 seconds with a dose of 642 mGy.cm2 and 300 μm voxel size. Preoperative CBCT scans were used to assess any defects present in the extracted teeth. Teeth with defects such as calcification, internal or external root resorption, and signs of previously attempted root canal treatment were excluded, and only teeth with intact root canal morphology were included in the study. In order to standardize the methodology, the extracted teeth were decoronated using a diamond disc (3M, India Diamond Cloth Disc 674W, India) with roots up to 16 mm in length (Figure 1). The extracted teeth were stored in saline (Baxter India Pvt Ltd) before use. The access cavity was created with an Endo Access bur size 2 (Dentsply Maillefer, Switzerland), and the canal patency was verified up to the working length using a #10 K-file (Mani, Utsunomiya, Tochigi, Japan). Also, 5.25% sodium hypochlorite (Acquafarma Farmácia, Niteroi, RJ, Brazil) was used for irrigating the prepared root canal space [9,19]. Teeth were randomly divided with the help of computer-generated numbers into three groups of 51 teeth each. The teeth in all three groups were mounted in a U-shaped rim made of modeling wax that mimicked the mandibular arch.
Group 1: ProFit S3 (ProFit Dental, India)
Group 2: HyFlex CM (Coltene, Switzerland)
Group 3: NeoEndo S (Eighteenth Orikam, India)
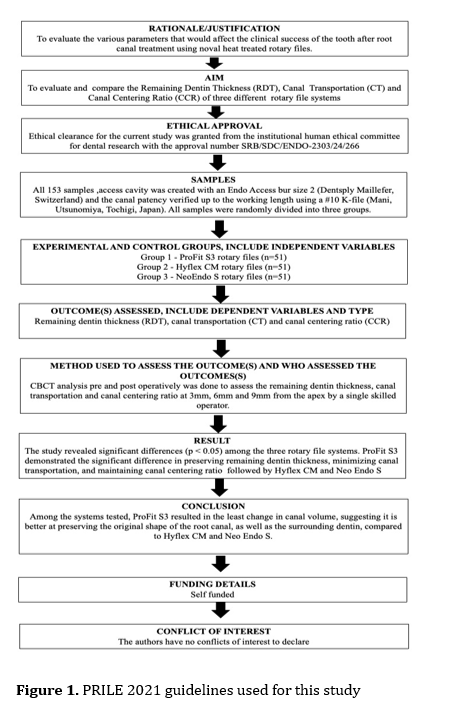
Figure 1. PRILE 2021 guidelines used for this study
The three groups of teeth were prepared to a rotary file size 25/6% in the corresponding file system. In the mesiobuccal and mesiolingual canals of the extracted teeth, measurements were made at 3 mm, 6 mm, and 9 mm from the apex to determine the RDT, CCR, and CT. The three file systems’ pre- and post-instrumentation states were examined on CBCT axial views [18].
The degree of CT was ascertained using the formula developed by Gambill et al, [20] [(x1-x2)-(y1-y2)] where y1 is the shortest distance between the instrumented canal's distal edge and the distal edge of the root, y2 is the shortest distance between the instrumented canal's distal edge and the distal edge of the root, and x1 is the shortest distance between the instrumented canal's mesial edge and the mesial edge of the root. Any value other than 0 shows that CT has taken place; whereas, a value of 0 implies no CT [20]. Similarly, the CCR was calculated using the same formula by Gambill et al. [20], i.e., (x1-x2)/(y1-y2)[20]. A result of ‘1’ indicates perfect CCR. The RDT was calculated by subtracting the un-instrumented canal width from the instrumented canal width [21]. The study adhered to the PRILE guidelines [22], with all the relevant details outlined in Figure 1. The RDT, CCR, and CT were compared among the three file systems using SPSS version 24. One-way ANOVA was used for intragroup and intergroup comparisons. The statistical significance was set at P=0.05.
Results
{kind=link}
The three groups of teeth were prepared to a rotary file size 25/6% in the corresponding file system. In the mesiobuccal and mesiolingual canals of the extracted teeth, measurements were made at 3 mm, 6 mm, and 9 mm from the apex to determine the RDT, CCR, and CT. The three file systems’ pre- and post-instrumentation states were examined on CBCT axial views [18].
The degree of CT was ascertained using the formula developed by Gambill et al, [20] [(x1-x2)-(y1-y2)] where y1 is the shortest distance between the instrumented canal's distal edge and the distal edge of the root, y2 is the shortest distance between the instrumented canal's distal edge and the distal edge of the root, and x1 is the shortest distance between the instrumented canal's mesial edge and the mesial edge of the root. Any value other than 0 shows that CT has taken place; whereas, a value of 0 implies no CT [20]. Similarly, the CCR was calculated using the same formula by Gambill et al. [20], i.e., (x1-x2)/(y1-y2)[20]. A result of ‘1’ indicates perfect CCR. The RDT was calculated by subtracting the un-instrumented canal width from the instrumented canal width [21]. The study adhered to the PRILE guidelines [22], with all the relevant details outlined in Figure 1. The RDT, CCR, and CT were compared among the three file systems using SPSS version 24. One-way ANOVA was used for intragroup and intergroup comparisons. The statistical significance was set at P=0.05.
Results
Tables 1 and 2 show the mean and standard deviation values of RDT (mm), CT (mm), and CCR at 3, 6 and 9 mm from the apex for three different rotary systems in the mesiobuccal and mesiolingual canals of mandibular molars. One-way ANOVA revealed that among the three rotary file systems—ProFit S3, HyFlex CM, and NeoEndo S—significant differences existed for most evaluated parameters at 6 mm and 9 mm levels in both mesiobuccal and mesiolingual canals (P<0.05). At the 3 mm level, no significant differences were found for RDT and CT (P>0.05); however, CCR showed a significant difference (P<0.05). Detailed findings are as follows:
At 3 mm from the apex:
Mesiobuccal canal: No significant differences were found among the three groups in RDT (P=0.081) or CT (P=0.079). However, a significant difference was found among the three groups in CCR (P=0.001). Pairwise comparisons showed that ProFit S3 maintained a more centered preparation compared to NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
Mesiolingual canal: No significant differences were found among the three groups in RDT (P=0.472) or CT (P=0.511). However, a significant difference was found among the three groups in CCR (P=0.001). Pairwise comparisons showed that ProFit S3 exhibited better centering than NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
At 6 mm from the apex:
Mesiobuccal canal: A significant difference existed in RDT among the three groups (P=0.006). Pairwise comparisons showed that ProFit S3 preserved more dentin than NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CT among the three groups (P=0.006). ProFit S3 exhibited the least transportation compared to NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CCR among the three groups (P=0.000). ProFit S3 had a higher centering ratio than both systems (P<0.01).
Mesiolingual canal: A significant difference existed in RDT among the three groups (P=0.007). ProFit S3 outperformed NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CT among the three groups (P=0.005). ProFit S3 demonstrated less CT than NeoEndo S (P<0.01). A significant difference existed in CCR among the three groups (P=0.000). ProFit S3 had superior CCR compared to the others (P<0.01).
At 9 mm from the apex:
Mesiobuccal canal: A significant difference existed in RDT among the three groups (P=0.000), such that ProFit S3>HyFlex CM>NeoEndo S (all P<0.01). A significant difference existed in CT among the three groups (P=0.000). ProFit S3 showed the least CT compared to other groups (P<0.01). A significant difference existed in CCR among the three groups (P=0.01). ProFit S3 demonstrated better CCR than the others (P<0.05).
Mesiolingual canal: A significant difference existed in RDT among the three groups (P=0.000). ProFit S3 preserved more dentin compared to HyFlex CM and NeoEndo S (P<0.01). A significant difference existed in CT among the three groups (P=0.000). ProFit S3 exhibited the least CT (P < 0.01) compared with the other two groups. A significant difference existed in CCR among the three groups (P=0.01). ProFit S3 achieved higher CCR than the other two groups (P<0.05).
ProFit S3 consistently demonstrated superior performance for all parameters at 6 mm and 9 mm, followed by HyFlex CM; while NeoEndo S performed least favorably. At 3 mm, differences for RDT and CT were not significant, although CCR was significantly better for ProFit S3.
At 3 mm from the apex:
Mesiobuccal canal: No significant differences were found among the three groups in RDT (P=0.081) or CT (P=0.079). However, a significant difference was found among the three groups in CCR (P=0.001). Pairwise comparisons showed that ProFit S3 maintained a more centered preparation compared to NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
Mesiolingual canal: No significant differences were found among the three groups in RDT (P=0.472) or CT (P=0.511). However, a significant difference was found among the three groups in CCR (P=0.001). Pairwise comparisons showed that ProFit S3 exhibited better centering than NeoEndo S (P<0.01) and HyFlex CM (P<0.05).
At 6 mm from the apex:
Mesiobuccal canal: A significant difference existed in RDT among the three groups (P=0.006). Pairwise comparisons showed that ProFit S3 preserved more dentin than NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CT among the three groups (P=0.006). ProFit S3 exhibited the least transportation compared to NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CCR among the three groups (P=0.000). ProFit S3 had a higher centering ratio than both systems (P<0.01).
Mesiolingual canal: A significant difference existed in RDT among the three groups (P=0.007). ProFit S3 outperformed NeoEndo S (P<0.01) and HyFlex CM (P<0.05). A significant difference existed in CT among the three groups (P=0.005). ProFit S3 demonstrated less CT than NeoEndo S (P<0.01). A significant difference existed in CCR among the three groups (P=0.000). ProFit S3 had superior CCR compared to the others (P<0.01).
At 9 mm from the apex:
Mesiobuccal canal: A significant difference existed in RDT among the three groups (P=0.000), such that ProFit S3>HyFlex CM>NeoEndo S (all P<0.01). A significant difference existed in CT among the three groups (P=0.000). ProFit S3 showed the least CT compared to other groups (P<0.01). A significant difference existed in CCR among the three groups (P=0.01). ProFit S3 demonstrated better CCR than the others (P<0.05).
Mesiolingual canal: A significant difference existed in RDT among the three groups (P=0.000). ProFit S3 preserved more dentin compared to HyFlex CM and NeoEndo S (P<0.01). A significant difference existed in CT among the three groups (P=0.000). ProFit S3 exhibited the least CT (P < 0.01) compared with the other two groups. A significant difference existed in CCR among the three groups (P=0.01). ProFit S3 achieved higher CCR than the other two groups (P<0.05).
ProFit S3 consistently demonstrated superior performance for all parameters at 6 mm and 9 mm, followed by HyFlex CM; while NeoEndo S performed least favorably. At 3 mm, differences for RDT and CT were not significant, although CCR was significantly better for ProFit S3.
Table 1. Mean and standard deviation values of RDT (mm), CT (mm), and CCR at different cross-sectional levels (3 mm, 6 mm, 9 mm) for the three different rotary systems in the mesiobuccal (MB) canals of mandibular molars
{kind=link}
Table 2. Mean and standard deviation values of RDT (mm), CT (mm), and CCR at 3, 6, and 9 mm from the apex for three different rotary systems in the mesiolingual (ML) canals of mandibular molars
{kind=link}
Discussion
The main goal of endodontic treatment is effective canal cleaning and shaping while maintaining the original canal anatomy, as this promotes optimal healing and minimizes complications during root canal therapy [23]. Preserving the original dimensions and shape of the canal is paramount, as CT can be detrimental, making it extremely challenging to restore canal integrity and negatively impacts the overall success of treatment [24]. This risk is especially prominent in canals that have a natural curvature or calcification, as they are more susceptible to shaping errors [25]. Evaluating the CCR and CT of various rotary file systems is critical, as it helps dental clinicians to choose instruments that optimize both cleaning efficiency and anatomical preservation. In this study, CCR and CT were analyzed specifically in the mesial canals of extracted mandibular first molars, where these risks are greater due to the narrower and more curved anatomy compared to the wider distal canal [26]. The use of CBCT imaging was instrumental in this study, as CBCT’s high resolution and 3D imaging capacity provide a precise, non-superimposed view of the canal morphology before and after instrumentation. CBCT was used to analyze the pre-instrumentation and post-instrumentation differences as it provides high-resolution images with 33D viewing facility, which enables the researchers to analyze the differences effectively. Another major advantage of CBCT is the ability to store the images, which are measurable and reproducible. CBCT offers superior resolution with minimal distortion, allowing for more accurate visualization of root canal anatomy compared to other imaging modalities. It enables precise measurement of canal dimensions and reduces the superimposition of the surrounding anatomical structures. This enhanced clarity facilitates a more detailed assessment of periapical tissue morphology and bone structure, providing a significant advantage over conventional radiographic techniques. Among the instruments evaluated, ProFit S3 performed best in maintaining canal centering, showing results closest to the ideal (a value of zero, indicating minimal deviation from the original canal center). This was in contrast to the Hyflex CM and NeoEndo S, which demonstrated higher CCR, suggesting that they are more prone to deviating from the canal’s original shape. ProFit S3’s superior performance in CCR can be attributed to its innovative design and material composition. The file system is manufactured with blue heat-treated NiTi, enhancing its flexibility and allowing it to better adapt to the natural curvatures of the canal. This flexibility prevents excessive force against canal walls, maintaining a more centered pathway. The ProFit S3’s controlled taper and unique cross-sectional design also contribute to this outcome by distributing dentin removal along the canal length more evenly, reducing the risk of unintentional overcutting in certain regions. In terms of CT, or the unintended displacement of the apical foramen, ProFit S3 also exhibited clear advantages. CT can lead to iatrogenic errors, including inadequate debris removal, which compromises the seal and increases the risk of reinfection, often requiring retreatment [27]. In this study, canal transportation was evaluated at three points: 3, 6, and 9 mm from the apex, capturing any shift in the canal pathway that could jeopardize the procedure’s outcome [28]. ProFit S3 showed minimal canal deviation, closely preserving the original apical position compared to Hyflex CM and NeoEndo S, which demonstrated greater CT. This can be explained by ProFit S3’s combination of design and alloy properties. The blue heat-treated NiTi provides exceptional flexibility, which allows the instrument to navigate curved canals with less risk of displacing the apical foramen. Furthermore, ProFit S3’s controlled engagement with the canal walls is facilitated by its design, reducing the lateral forces that often lead to CT.
The RDT is another crucial factor in endodontic success, as it directly impacts the structural integrity and resistance of the tooth during obturation. Excessive dentin removal can undermine the tooth’s stability, increase fracture risk, and lead to procedural errors such as perforations [29]. In summary, the ProFit S3 rotary file system demonstrated superior CCR, minimized CT, and better preserved dentin thickness compared to Hyflex CM and NeoEndo S. The combination of heat-treated NiTi flexibility, controlled taper, precise cross-sectional design, and efficient cutting action enabled ProFit S3 to provide more predictable and safe canal preparations, reducing the risks of procedural errors and enhancing the likelihood of successful outcomes. These attributes underscore ProFit S3 as an effective choice in complex cases, particularly where maintaining original canal morphology and minimizing structural compromise are the main priorities.
Conclusion
The RDT is another crucial factor in endodontic success, as it directly impacts the structural integrity and resistance of the tooth during obturation. Excessive dentin removal can undermine the tooth’s stability, increase fracture risk, and lead to procedural errors such as perforations [29]. In summary, the ProFit S3 rotary file system demonstrated superior CCR, minimized CT, and better preserved dentin thickness compared to Hyflex CM and NeoEndo S. The combination of heat-treated NiTi flexibility, controlled taper, precise cross-sectional design, and efficient cutting action enabled ProFit S3 to provide more predictable and safe canal preparations, reducing the risks of procedural errors and enhancing the likelihood of successful outcomes. These attributes underscore ProFit S3 as an effective choice in complex cases, particularly where maintaining original canal morphology and minimizing structural compromise are the main priorities.
Conclusion
Under the limitations of this study, it can be concluded that ProFit S3 showed the highest value of RDT and CCR, and minimal CT, followed by Hyflex CM and NeoEndo S.
Acknowledgment
Acknowledgment
The authors would like to acknowledge the Department of Conservative Dentistry and Endodontics, Saveetha Dental College, India.
Type of Study: Original article |
Subject:
Endodontics
References
1. Gomes BPFA, Aveiro E, Kishen A. Irrigants and irrigation activation systems in Endodontics. Braz Dent J. 2023 Jul-Aug;34(4):1-33. [DOI:10.1590/0103-6440202305577]
2. Abdelkafy H, Eldehna AM, Salem NA. Canal Transportation and Centring Ratio of Paediatric vs Regular Files in Primary Teeth. Int Dent J. 2023 Jun;73(3):423-9. [DOI:10.1016/j.identj.2022.09.003] [PMID] []
3. Chourasia HR, Meshram GK, Warhadpande M, Dakshindas D. Root canal morphology of mandibular first permanent molars in an Indian population. Int J Dent. 2012;2012:745152. [DOI:10.1155/2012/745152] [PMID] []
4. Antony SDP, Subramanian AK, Nivedhitha MS, Solete P. Comparative evaluation of canal transportation, centering ability, and dentin removal between ProTaper Gold, One Curve, and Profit S3: An in vitro study. J Conserv Dent. 2020 Nov-Dec;23(6):632-6. [DOI:10.4103/JCD.JCD_619_20] [PMID] []
5. Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016 Jan-Mar;10(1):144-7. [DOI:10.4103/1305-7456.175682] [PMID] []
6. Ali A, Saraf P, Kamatagi L, Khasnis S. Comparative Assessment of Canal Transportation, Dentin Loss, and Remaining Root Filling Material by Different Retreatment Files An In vitro Cross-Sectional Study. Contemp Clin Dent. 2021 Jan-Mar;12(1):14-20. [DOI:10.4103/ccd.ccd_31_20] [PMID] []
7. Chaudhary NR, Singh DJ, Somani R, Jaidka S. Comparative Evaluation of Efficiency of Different File Systems in Terms of Remaining Dentin Thickness Using Cone-Beam Computed Tomography: An In vitro Study. Contemp Clin Dent. 2018 Jul-Sep;9(3):367-71. [DOI:10.4103/ccd.ccd_72_18] [PMID] []
8. Kwak SW, Shen Y, Liu H, Kim HC, Haapasalo M. Torque Generation of the Endodontic Instruments: A Narrative Review. Materials (Basel). 2022 Jan 17;15(2):664. [DOI:10.3390/ma15020664] [PMID] []
9. Asha K, Ghivari S, Pujar M, Sait S. NiTi rotary system in endodontics-An overview. IP Indian J Conserv Endod. 2023;8:128-33. [DOI:10.18231/j.ijce.2023.025]
10. Al-Sudani D. Topographic Analysis of HyFlex(®) Controlled Memory Nickel-Titanium Files. J Int Oral Health. 2014 Nov-Dec;6(6):1-4.
11. Chhabra A, Ramya KP, Prathap BS, Yadav P. Life span of Neoendo Flex and ProTaper Next rotary files with reciprocating motion in single-rooted teeth. J Conserv Dent Endod. 2023 Jul-Aug;26(4):420-3.
12. Swathi S, Antony DP, Solete P, Jeevanandan G, Vishwanathaiah S, Maganur PC. Comparative evaluation of remaining dentin thickness, canal centering ability and apical deformity between ProFit S3 and Protaper gold - A nano CT study. Saudi Dent J. 2024 Apr;36(4):650-5. [DOI:10.1016/j.sdentj.2024.01.002] [PMID] []
13. Scarfe WC, Levin MD, Gane D, Farman AG. Use of cone beam computed tomography in endodontics. Int J Dent. 2009;2009:634567. [DOI:10.1155/2009/634567] [PMID] []
14. Makati D, Shah NC, Brave D, Singh Rathore VP, Bhadra D, Dedania MS. Evaluation of remaining dentin thickness and fracture resistance of conventional and conservative access and biomechanical preparation in molars using cone-beam computed tomography: An in vitro study. J Conserv Dent. 2018 May-Jun;21(3):324-7. [DOI:10.4103/JCD.JCD_311_17] [PMID] []
15. Jain A, Gupta AS, Agrawal R. Comparative analysis of canal-centering ratio, apical transportation, and remaining dentin thickness between single-file systems, i.e., OneShape and WaveOne reciprocation: An in vitro study. J Conserv Dent. 2018 Nov-Dec;21(6):637-641. [DOI:10.4103/JCD.JCD_101_18] [PMID] []
16. Puleio F, Bellezza U, Torre A, Giordano F, Lo Giudice G. Apical transportation of apical foramen by different NiTi alloy systems: a systematic review. Appl. Sci. 2023 Sep 22;13(19):10555. [DOI:10.3390/app131910555]
17. Karamifar K, Tondari A, Saghiri MA. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur Endod J. 2020 Jul 14;5(2):54-67. [DOI:10.14744/eej.2020.42714] [PMID] []
18. Kishore A, Gurtu A, Bansal R, Singhal A, Mohan S, Mehrotra A. Comparison of canal transportation and centering ability of Twisted Files, HyFlex controlled memory, and Wave One using computed tomography scan: An in vitro study. J Conserv Dent. 2017 May-Jun;20(3):161-5. [DOI:10.4103/JCD.JCD_110_16] [PMID] []
19. S DPA, Solete P, Jeevanandan G, Syed AA, Almahdi S, Alzhrani M, Maganur PC, Vishwanathaiah S. Effect of Various Irrigant Activation Methods and Its Penetration in the Apical Third of Root Canal-In Vitro Study. Eur J Dent. 2023 Feb;17(1):57-61. [DOI:10.1055/s-0041-1742122] [PMID] []
20. Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996 Jul;22(7):369-75. [DOI:10.1016/S0099-2399(96)80221-4] [PMID]
21. Jain A, Gupta AS, Agrawal R. Comparative analysis of canal-centering ratio, apical transportation, and remaining dentin thickness between single-file systems, i.e., OneShape and WaveOne reciprocation: An in vitro study. J Conserv Dent. 2018 Nov-Dec;21(6):637-41. [DOI:10.4103/JCD.JCD_101_18] [PMID] []
22. Nagendrababu V, Murray PE, Ordinola-Zapata R, Peters OA, Rôças IN, Siqueira JF Jr, Priya E, Jayaraman J, J Pulikkotil S, Camilleri J, Boutsioukis C, Rossi-Fedele G, Dummer PMH. PRILE 2021 guidelines for reporting laboratory studies in Endodontology: A consensus-based development. Int Endod J. 2021 Sep;54(9):1482-90. [DOI:10.1111/iej.13542] [PMID]
23. Marvaniya J, Agarwal K, Mehta DN, Parmar N, Shyamal R, Patel J. Minimal Invasive Endodontics: A Comprehensive Narrative Review. Cureus. 2022 Jun 16;14(6):e25984. [DOI:10.7759/cureus.25984] [PMID] []
24. Silva RV, Alcalde MP, Horta MC, Rodrigues CT, Silveira FF, Duarte MA, Nunes E. Root canal shaping of curved canals by Reciproc Blue system and Pro Taper Gold: A micro-computed tomographic study. J Clin Exp Dent. 2021 Feb 1;13(2):e112-8. [DOI:10.4317/jced.57180] [PMID] []
25. Hemalatha P, Sanjana V, Padmanabhan P, Muthalagu M, Shahul Hameed M. A comparative evaluation of the efficacy of intraoral periapical radiography, panoramic radiography and CBCT in the assessment of impacted mandibular third molars and their relation to the inferior alveolar nerve canal. IP Int J Maxillofac Imaging. 2021;7(4):156-62. [DOI:10.18231/j.ijmi.2021.028]
26. Pinheiro SR, Alcalde MP, Vivacqua-Gomes N, Bramante CM, Vivan RR, Duarte MAH, Vasconcelos BC. Evaluation of apical transportation and centring ability of five thermally treated NiTi rotary systems. Int Endod J. 2018 Jun;51(6):705-13. [DOI:10.1111/iej.12881] [PMID]
27. Mehta SD, Malhan S, Bansal C. Iatrogenic Complications Arising From Cleaning and Shaping: A Review. Int. J. of Health Sci. 2021:56-62. [DOI:10.53730/ijhs.v5nS1.5342]
28. Hasheminia SM, Soltani S, Mohamadian F, Saatchi M, Sadeghi SM. Evaluation of apical transportation and centering ability of three single-file systems in severely curved canals using micro-computed tomography. Dent Res J (Isfahan). 2024 Feb 22;21:12. [DOI:10.4103/drj.drj_270_23]
29. Haralur SB, Al-Qahtani AS, Al-Qarni MM, Al-Homrany RM, Aboalkhair AE. Influence of remaining dentin wall thickness on the fracture strength of endodontically treated tooth. J Conserv Dent. 2016 Jan-Feb;19(1):63-7. [DOI:10.4103/0972-0707.173201] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |