Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 3 (9-2025)
J Res Dent Maxillofac Sci 2025, 10(3): 184-191 |
Back to browse issues page

Ethics code: IR.IAU.DENTAL.REC.1401.022
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abbaspour G, Barzegar Reyhani N, Safarzadeh Khosroshahi S, Jalalian S. Fracture Resistance of Unsupported Enamel Reinforced by Glass Fiber Ribbon. J Res Dent Maxillofac Sci 2025; 10 (3) :184-191
URL: http://jrdms.dentaliau.ac.ir/article-1-783-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-783-en.html



1- Dentist, Private Practice, Tehran, Iran.
2- Department of Restorative Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran.
3- Department of Restorative Dentistry, Member of Dental Material Research Center, TeMS.C., Islamic Azad University, Tehran, Iran. ,shahriar.jalalian@yahoo.com
2- Department of Restorative Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran.
3- Department of Restorative Dentistry, Member of Dental Material Research Center, TeMS.C., Islamic Azad University, Tehran, Iran. ,
Full-Text [PDF 362 kb]
(664 Downloads)
| Abstract (HTML) (1872 Views)
Full-Text: (620 Views)
Abstract
Background and Aim: Fiber-reinforced composite (FRC) restoration is a relatively new method used to enhance the durability of composite restorations. This study measured the fracture resistance of unsupported enamel in composite restorations reinforced with fiber ribbon in comparison with conventional composite restorations.
Materials and Methods: In this in vitro study, 30 freshly extracted sound premolars were randomly divided into three groups (n=10): (I) control group: intact teeth, (II) mesio-occluso-distal (MOD) preparation followed by restoration with Filtek P60 composite, and (III) deep MOD preparation and cusp reduction, followed by reinforcement with Interlig fiber ribbon, and subsequent restoration and cusp coverage with Filtek P60 composite. The teeth were stored in saline for one week. Next, their fracture resistance was measured by a universal testing machine. The load at fracture was recorded in Newtons (N). One-way ANOVA followed by the Tamhane post-hoc test was used to compare the groups (alpha=0.05).
Results: Fracture resistance of enamel in both experimental groups was significantly reduced compared to intact teeth (P<0.05). Fracture resistance of enamel in FRC restorations was significantly higher compared to the conventional composite restorations (P<0.05).
Conclusion: FRC restorations significantly increased the fracture resistance of unsupported enamel compared to the conventional composite restorations under in vitro settings.
Keywords: Composite Resins; Dental Enamel; Dental Materials; Tooth Fractures
Introduction
Materials and Methods: In this in vitro study, 30 freshly extracted sound premolars were randomly divided into three groups (n=10): (I) control group: intact teeth, (II) mesio-occluso-distal (MOD) preparation followed by restoration with Filtek P60 composite, and (III) deep MOD preparation and cusp reduction, followed by reinforcement with Interlig fiber ribbon, and subsequent restoration and cusp coverage with Filtek P60 composite. The teeth were stored in saline for one week. Next, their fracture resistance was measured by a universal testing machine. The load at fracture was recorded in Newtons (N). One-way ANOVA followed by the Tamhane post-hoc test was used to compare the groups (alpha=0.05).
Results: Fracture resistance of enamel in both experimental groups was significantly reduced compared to intact teeth (P<0.05). Fracture resistance of enamel in FRC restorations was significantly higher compared to the conventional composite restorations (P<0.05).
Conclusion: FRC restorations significantly increased the fracture resistance of unsupported enamel compared to the conventional composite restorations under in vitro settings.
Keywords: Composite Resins; Dental Enamel; Dental Materials; Tooth Fractures
Introduction
Teeth affected by caries, previous restorations, or root canal treatments often lose a substantial portion of their structure. As the damage increases, the dentin-enamel complex becomes smaller, which significantly raises the risk of catastrophic fractures in the remaining tooth structure [1, 2]. The appropriate treatment plan for such teeth is selected based on the remaining tooth structure, cavity wall thickness, the tooth's position in dental arch, and the magnitude of force applied to the tooth [3]. Nowadays, reconstruction of posterior teeth with composite resins is the treatment of choice for most patients [4, 5]. Recent advances in adhesive technology and development of stronger composite materials have made it possible to create more conservative and esthetic restorations. However, polymerization shrinkage still remains a problem in large composite restorations [6, 7]. This issue can lead to secondary caries, pulpal sensitivity in vital teeth, and stress at the tooth-restoration interface [2, 8-10]. It should also be noted that composite resins are solid materials; hence, despite their high strength, they have low toughness [11], which reduces the material’s resistance to rapid crack propagation [1].
Reconstruction of teeth with fiber-reinforced composite (FRC) is a relatively new method, which was introduced to increase the durability of composite restorations, and enhance strength and distribution of forces along the fibers. The development of FRC has increased the use of composite resin materials in extensive cavities [12, 13].
In FRC restorations, various criteria such as toughness, durability, and force distribution have been evaluated [14-16], but research evaluating the fracture resistance of unsupported enamel in these treatments has been insufficient. This study compared the fracture resistance of intact teeth, unsupported enamel in composite restorations, and unsupported enamel in composite restorations reinforced with fiber.
Materials and Methods
Reconstruction of teeth with fiber-reinforced composite (FRC) is a relatively new method, which was introduced to increase the durability of composite restorations, and enhance strength and distribution of forces along the fibers. The development of FRC has increased the use of composite resin materials in extensive cavities [12, 13].
In FRC restorations, various criteria such as toughness, durability, and force distribution have been evaluated [14-16], but research evaluating the fracture resistance of unsupported enamel in these treatments has been insufficient. This study compared the fracture resistance of intact teeth, unsupported enamel in composite restorations, and unsupported enamel in composite restorations reinforced with fiber.
Materials and Methods
Specimen preparation:
In this in vitro study, 30 premolar teeth, extracted for periodontal or orthodontic reasons were selected (ethical approval code: IR.IAU.DENTAL.REC.1401.022). The inclusion criteria were absence of caries, root cracks, previous root canal treatments, posts, crowns, and resorption [17]. Immediately after extraction, the soft tissue covering the root was removed using a scaler, and the teeth were placed in 5.25% NaOCl solution (Morvabon, Tehran, Iran) for 5 minutes. They were then stored in 0.9% saline (Samen, Tehran, Iran) at room temperature until testing. Before testing, the tooth surfaces were polished with a rubber cup and pumice paste [18].
Cavity preparation and restorative procedures:
A total of 30 samples were randomly divided into three groups (n=10) by using a random generator with uniform probability distribution in Microsoft Excel to generate an array of random integers between 1 and 30 without duplicates. (I) Control group, (II) experimental group 1 with composite restoration, and (III) experimental group 2 with FRC restoration. For the control group, no intervention was performed (Figure 2a) [19]. For the two experimental groups, deep mesio-occluso-distal (MOD) cavities were prepared using a high-speed handpiece (BD-4, MME, China) with a cooling air and water system and a cylindrical diamond bur (841; Jota, Switzerland) with 1 mm diameter. The bur was replaced after every three tooth preparations. The cavity characteristics were as follows [20]: the buccolingual width of the cavity was prepared such that only 1 mm of enamel remained intact at the lingual and buccal walls. In order to ensure absence of dentin at the margins, both visual examination and measurement with a digital caliper (Guanglu, Guilin, China) were performed. Sliding jaws of the caliper were placed against marginal walls and opened slightly to match and fit the shape. Then, the value was measured. As the width in all marginal wall lengths was not more than 1 mm, there was no remaining dentin.
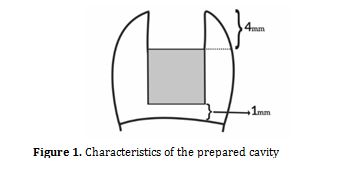
The pulpal depth of the cavity was 4 mm from the cavosurface. Gingival floor of the cavity was prepared such that only 1 mm of enamel remained intact in the buccal and lingual walls. The cavities extended to 1 mm above the cementoenamel junction in the occluso-cervical direction (Figure 1). All samples were rinsed for 10 seconds, and dried with air spray [18].
Figure 1. Characteristics of the prepared cavity
Experimental group 1 (composite): After applying a matrix band, the samples were etched with 37% phosphoric acid (Morvabon, Tehran, Iran) for 15 seconds, rinsed for 15 seconds, and dried. The cavities were then coated with Single Bond adhesive (3M, ESPE, USA) and air-dried for 3 seconds. Then, the second adhesive layer was applied. The intensity of the LED curing light (Guilin Woodpecker Medical Instrument Co., LTD, China) was measured with a radiometer (Guilin Woodpecker Medical Instrument Co., LTD, China). The samples were cured for 20 seconds with a light intensity of 600 mW/cm², placed 1 mm away from the samples [20]. A 0.5-mm-thick layer of flowable composite (ES Flow, Spident Co., Korea) was applied on the pulpal floor of the cavity and cured for 40 seconds [20]. The interproximal walls of the cavities were then reconstructed with Filtek P60 composite (3M, ESPE, USA) using the centripetal method to convert MOD cavities into Class I cavities [21]. The obtained Class I cavities were restored with Filtek P60 composite (3M, ESPE, USA) using the oblique incremental method, with a maximum thickness of 2 mm per layer and a curing time of 40 seconds per layer, while the LED curing unit was at a distance of 1 mm from the sample (Figures 2b and 3a).
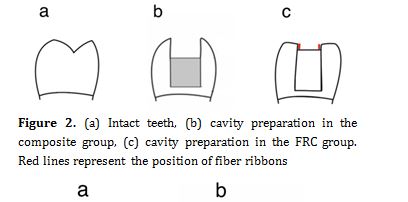
Experimental group 2 (FRC): The samples had their functional cusps reduced by 2 mm and non-functional cusps by 1.5 mm (Figure 2c) in order to increase the strength of the unsupported enamel walls. After applying a matrix band, the samples were etched with 37% phosphoric acid (Morvabon, Tehran, Iran) for 15 seconds, washed for 15 seconds, and dried. Before bonding, a piece of fiber ribbon (Interlig, Angelus, Brazil) was placed along the buccal wall and another piece along the lingual wall. The cavities were then coated with Single Bond adhesive (3M, ESPE, USA) and dried with air flow for 3 seconds. After applying the second adhesive layer, they were cured for 20 seconds with LED light (Guilin Woodpecker Medical Instrument Co., LTD, CHINA) with an intensity of 600 mW/cm², at 1 mm distance from the sample. A 0.5 mm-thick layer of flowable composite (ESFlow, SPIDENT CO., Korea) was applied on the pulpal floor of the cavity and cured for 40 seconds. The reduced cusps were then restored with Filtek P60 composite (3M, ESPE, USA). The interproximal walls of the cavities were reconstructed with Filtek P60 composite (3M, ESPE, USA) using the centripetal method to convert MOD cavities into Class I cavities. The obtained Class I cavities were restored with Filtek P60 composite (3M, ESPE, USA) using the oblique incremental method with a maximum thickness of 2 mm per layer and a curing time of 40 seconds per layer, while the tip had 1 mm distance from the sample [18, 22] (Figure 3b).
Figure 2. (a) Intact teeth, (b) cavity preparation in the composite group, (c) cavity preparation in the FRC group. Red lines represent the position of fiber ribbons
Figure 3. (a) Restoration in the composite group, (b) cusp coverage and restoration in the FRC group
After restoration, the samples were stored in saline for one week. All samples were then mounted in acrylic resin cylinders (Marlic Medical Industries Co., Alborz, Iran) up to 2 mm from the cementoenamel junction and tested with a universal testing machine (STM-20, Santam CO., Iran). Compression force was applied to the samples at a crosshead speed of 1 mm per minute parallel to the vertical axis of the tooth until its fracture. The value of the fracture force was recorded in Newtons (N) [18]. This value was divided by the cross-sectional area of the tooth to calculate the fracture resistance in megapascals (MPa).
Due to the normal distribution of data as checked by the Kolmogorov-Smirnov test, one-way ANOVA was applied for general comparison. Subsequent pairwise comparisons were performed by the Tamhane’s post-hoc test [23].
Results
In this in vitro study, 30 premolar teeth, extracted for periodontal or orthodontic reasons were selected (ethical approval code: IR.IAU.DENTAL.REC.1401.022). The inclusion criteria were absence of caries, root cracks, previous root canal treatments, posts, crowns, and resorption [17]. Immediately after extraction, the soft tissue covering the root was removed using a scaler, and the teeth were placed in 5.25% NaOCl solution (Morvabon, Tehran, Iran) for 5 minutes. They were then stored in 0.9% saline (Samen, Tehran, Iran) at room temperature until testing. Before testing, the tooth surfaces were polished with a rubber cup and pumice paste [18].
Cavity preparation and restorative procedures:
A total of 30 samples were randomly divided into three groups (n=10) by using a random generator with uniform probability distribution in Microsoft Excel to generate an array of random integers between 1 and 30 without duplicates. (I) Control group, (II) experimental group 1 with composite restoration, and (III) experimental group 2 with FRC restoration. For the control group, no intervention was performed (Figure 2a) [19]. For the two experimental groups, deep mesio-occluso-distal (MOD) cavities were prepared using a high-speed handpiece (BD-4, MME, China) with a cooling air and water system and a cylindrical diamond bur (841; Jota, Switzerland) with 1 mm diameter. The bur was replaced after every three tooth preparations. The cavity characteristics were as follows [20]: the buccolingual width of the cavity was prepared such that only 1 mm of enamel remained intact at the lingual and buccal walls. In order to ensure absence of dentin at the margins, both visual examination and measurement with a digital caliper (Guanglu, Guilin, China) were performed. Sliding jaws of the caliper were placed against marginal walls and opened slightly to match and fit the shape. Then, the value was measured. As the width in all marginal wall lengths was not more than 1 mm, there was no remaining dentin.
The pulpal depth of the cavity was 4 mm from the cavosurface. Gingival floor of the cavity was prepared such that only 1 mm of enamel remained intact in the buccal and lingual walls. The cavities extended to 1 mm above the cementoenamel junction in the occluso-cervical direction (Figure 1). All samples were rinsed for 10 seconds, and dried with air spray [18].
Figure 1. Characteristics of the prepared cavity
{kind=link}
Experimental group 1 (composite): After applying a matrix band, the samples were etched with 37% phosphoric acid (Morvabon, Tehran, Iran) for 15 seconds, rinsed for 15 seconds, and dried. The cavities were then coated with Single Bond adhesive (3M, ESPE, USA) and air-dried for 3 seconds. Then, the second adhesive layer was applied. The intensity of the LED curing light (Guilin Woodpecker Medical Instrument Co., LTD, China) was measured with a radiometer (Guilin Woodpecker Medical Instrument Co., LTD, China). The samples were cured for 20 seconds with a light intensity of 600 mW/cm², placed 1 mm away from the samples [20]. A 0.5-mm-thick layer of flowable composite (ES Flow, Spident Co., Korea) was applied on the pulpal floor of the cavity and cured for 40 seconds [20]. The interproximal walls of the cavities were then reconstructed with Filtek P60 composite (3M, ESPE, USA) using the centripetal method to convert MOD cavities into Class I cavities [21]. The obtained Class I cavities were restored with Filtek P60 composite (3M, ESPE, USA) using the oblique incremental method, with a maximum thickness of 2 mm per layer and a curing time of 40 seconds per layer, while the LED curing unit was at a distance of 1 mm from the sample (Figures 2b and 3a).
Experimental group 2 (FRC): The samples had their functional cusps reduced by 2 mm and non-functional cusps by 1.5 mm (Figure 2c) in order to increase the strength of the unsupported enamel walls. After applying a matrix band, the samples were etched with 37% phosphoric acid (Morvabon, Tehran, Iran) for 15 seconds, washed for 15 seconds, and dried. Before bonding, a piece of fiber ribbon (Interlig, Angelus, Brazil) was placed along the buccal wall and another piece along the lingual wall. The cavities were then coated with Single Bond adhesive (3M, ESPE, USA) and dried with air flow for 3 seconds. After applying the second adhesive layer, they were cured for 20 seconds with LED light (Guilin Woodpecker Medical Instrument Co., LTD, CHINA) with an intensity of 600 mW/cm², at 1 mm distance from the sample. A 0.5 mm-thick layer of flowable composite (ESFlow, SPIDENT CO., Korea) was applied on the pulpal floor of the cavity and cured for 40 seconds. The reduced cusps were then restored with Filtek P60 composite (3M, ESPE, USA). The interproximal walls of the cavities were reconstructed with Filtek P60 composite (3M, ESPE, USA) using the centripetal method to convert MOD cavities into Class I cavities. The obtained Class I cavities were restored with Filtek P60 composite (3M, ESPE, USA) using the oblique incremental method with a maximum thickness of 2 mm per layer and a curing time of 40 seconds per layer, while the tip had 1 mm distance from the sample [18, 22] (Figure 3b).
Figure 2. (a) Intact teeth, (b) cavity preparation in the composite group, (c) cavity preparation in the FRC group. Red lines represent the position of fiber ribbons
{kind=link}
Figure 3. (a) Restoration in the composite group, (b) cusp coverage and restoration in the FRC group
{kind=link}
After restoration, the samples were stored in saline for one week. All samples were then mounted in acrylic resin cylinders (Marlic Medical Industries Co., Alborz, Iran) up to 2 mm from the cementoenamel junction and tested with a universal testing machine (STM-20, Santam CO., Iran). Compression force was applied to the samples at a crosshead speed of 1 mm per minute parallel to the vertical axis of the tooth until its fracture. The value of the fracture force was recorded in Newtons (N) [18]. This value was divided by the cross-sectional area of the tooth to calculate the fracture resistance in megapascals (MPa).
Due to the normal distribution of data as checked by the Kolmogorov-Smirnov test, one-way ANOVA was applied for general comparison. Subsequent pairwise comparisons were performed by the Tamhane’s post-hoc test [23].
Results
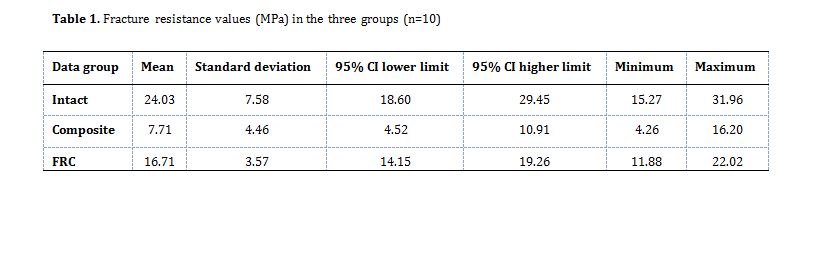
Figure 4 shows the cumulative failure in fracture resistance test in the three groups. Table 1 and Figure 5 show the fracture resistance values in the three groups. One-way ANOVA revealed a significant difference in fracture resistance among the groups (P=0.01). Due to the differences in standard deviations among the groups, pairwise comparisons were performed using the Tamhane’s post-hoc test (Table 2), which showed a significantly lower fracture resistance in the composite group compared to the intact group (P< 0.001). Similarly, the fracture resistance of the FRC group was significantly lower than that of intact teeth (P=0.048). The fracture resistance of the FRC group was significantly higher than that of composite group (P<0.001).
Figure 4. Cumulative failure in fracture resistance test in the three groups
Figure 5. Statistical distribution of fracture resistance in the three groups
Table 1. Fracture resistance values (MPa) in the three groups (n=10)
Table 2. Pairwise comparisons of the groups regarding fracture resistance (MPa) using the Tamhane’s post-hoc test
Discussion
Figure 4. Cumulative failure in fracture resistance test in the three groups
{kind=link}
Figure 5. Statistical distribution of fracture resistance in the three groups
{kind=link}
Table 1. Fracture resistance values (MPa) in the three groups (n=10)
{kind=link}
Table 2. Pairwise comparisons of the groups regarding fracture resistance (MPa) using the Tamhane’s post-hoc test
{kind=link}
Discussion
In this in vitro study, the fracture resistance of unsupported enamel in FRC restorations and the conventional composite restorations was compared with intact teeth. Fracture resistance was measured by a universal testing machine and applying compressive force to the samples. The results indicated that the fracture resistance of the FRC group was significantly higher compared to composite alone. However, FRC restorations still did not fully restore the properties of an intact tooth in deep MOD cavities.
According to various studies, a cavity design such as MOD, which results in loss of tooth's marginal ridge, can lead to 46% loss of tooth rigidity, and this preparation can also reduce cusp stiffness by up to 63% [24, 25]. With advancements in composite resins and the gradual phasing out of amalgam worldwide, composite resins are now routinely used for reconstruction of posterior teeth [17].
In the present study, the fracture resistance of the control group was the highest (24.21±7.58 MPa) while that of the composite group was the lowest (7.71±4.46 MPa). The fracture resistance in the fiber group was 16.71 ± 3.57 MPa, which was significantly higher than the second group, but still lower than the intact teeth. These results are consistent with previous studies [19,26]. The incorporated glass fiber ribbons have a reported flexural strength of 131 MPa [27] which is comparable with the flexural strength of Filtek P60 composite resin i.e., 155 MPa [28]; however, placement of fiber ribbons at the corners of MOD cavity significantly reduces the stress concentration. Additionally, the bond strength of fiber ribbons to dentin using Single Bond adhesive is 30 MPa [29] offering improved adhesion compared to Filtek P60 composite with a bond strength of 20 MPa [28]. Therefore, the enhancement in the mean fracture resistance of the restored teeth form 7.7 MPa to 16.7 MPa by using glass fiber ribbon may be attributed to the abovementioned two factors of reduced stress concentration and improved adhesion to dentin at the location of peak stress. Furthermore, the improved stress distribution and crack propagation resistance of glass fiber ribbon restorations are expected to improve the fatigue life and hence increase the lifespan of the restored teeth. The authors did not assess the fatigue life of the samples in the present study, and future studies are required in this respect.
The cost of FRC restorations in this study was 16.9% higher (due to materials and labor) compared to composite restorations. However, this increase in cost is justified, as the mean fracture resistance of the restored teeth increased from 7.7 MPa to 16.7 MPa. Additionally, the survival of the restored teeth is expected to increase significantly with fiber reinforcement.
Kirmah et al. [19] showed that using flowable composite with fiber under composite restorations significantly increased the fracture resistance of endodontically treated teeth with MOD cavities, and various fiber placement techniques can influence this increase in fracture resistance. In another study, Jafari Navimipour et al. [26] evaluated the effects of different fiber placement techniques on fracture resistance of maxillary premolars with MOD cavities. They reported that placing glass fibers from the buccal to the lingual wall increased the fracture resistance. Additionally, Patnana et al. [30] reported increased fracture resistance in reinforced restorations. In another study, Albar and khayat [31] found that placing polyethylene ribbons in axial walls significantly increased the fracture resistance of the samples, compared to other samples, including conventional composite restorations and fiber placement in the gingival and axial walls together with the gingival wall. Scotti et al. [32] also found that using fiber ribbons with different techniques in molars with MOD cavities significantly increased fracture resistance in fiber-reinforced samples, compared to conventional composite restorations. However, there was no significant difference among various techniques, including the use of fiber posts, mesiodistal glass fibers, and bucco-palatal glass fibers.
Nevertheless, there are still limitations in restoring large cavities such as MODs, which need to be considered. One of these limitations is the low fracture resistance of these restorations, which reduces the strength of the restoration against the forces of the masticatory system [33]. FRC restoration is one of the new methods to strengthen extensive restorations [34], as it reinforces the restoration from within [35]. The fibers commonly used for this purpose today are polyethylene ribbons and glass fibers. It has been shown that both types play a significant role in increasing the fracture resistance of restorations in both endodontically-treated and vital teeth [34].
Despite the significant difference between the composite restoration group and the FRC restoration group in this study, Daher et al. [36] reported no significant difference in fracture resistance among the groups in their study, although they reinforced the walls with glass fibers and used inlays and onlays in other groups. In their study, the fiber was used as a loop and in an X shape around the buccal and lingual walls. Increasing the number of layers and fibers, absence of cusp reduction, and use of molar teeth could be the reasons for lack of a significant difference between the test group and intact teeth and other groups in their study. In another study, Bahari et al. [37], concluded that despite reinforcing restorations with glass fibers on the occlusal surface or horizontally connecting the buccal and lingual walls, there was no significant difference in the study groups compared to the healthy teeth. The discrepancy between the results of their study and the present study could be due to the lack of identical preparation techniques and differences in fiber positioning.
Sengun et al. [38] also compared the fracture resistance of premolars restored with composite, with and without polyethylene fibers, and found no significant difference between the composite restoration group and the FRC group. In their study, the cavity preparation was more conservative and did not aim to achieve unsupported enamel. Additionally, the fiber was placed buccolingually on the occlusal surface, and the angle of placement in the universal testing machine was 45 degrees relative to the tooth's longitudinal axis. Cobankara et al. [39] conducted a study on endodontically-treated molars and found no significant difference in fracture resistance among the groups, which were restored with amalgam, inlay, composite alone, and composite reinforced with polyethylene fiber. The difference between the results of the two studies could be due to the lack of identical preparation and placing the samples against forces, which mimicked masticatory movements.
Conclusion
According to various studies, a cavity design such as MOD, which results in loss of tooth's marginal ridge, can lead to 46% loss of tooth rigidity, and this preparation can also reduce cusp stiffness by up to 63% [24, 25]. With advancements in composite resins and the gradual phasing out of amalgam worldwide, composite resins are now routinely used for reconstruction of posterior teeth [17].
In the present study, the fracture resistance of the control group was the highest (24.21±7.58 MPa) while that of the composite group was the lowest (7.71±4.46 MPa). The fracture resistance in the fiber group was 16.71 ± 3.57 MPa, which was significantly higher than the second group, but still lower than the intact teeth. These results are consistent with previous studies [19,26]. The incorporated glass fiber ribbons have a reported flexural strength of 131 MPa [27] which is comparable with the flexural strength of Filtek P60 composite resin i.e., 155 MPa [28]; however, placement of fiber ribbons at the corners of MOD cavity significantly reduces the stress concentration. Additionally, the bond strength of fiber ribbons to dentin using Single Bond adhesive is 30 MPa [29] offering improved adhesion compared to Filtek P60 composite with a bond strength of 20 MPa [28]. Therefore, the enhancement in the mean fracture resistance of the restored teeth form 7.7 MPa to 16.7 MPa by using glass fiber ribbon may be attributed to the abovementioned two factors of reduced stress concentration and improved adhesion to dentin at the location of peak stress. Furthermore, the improved stress distribution and crack propagation resistance of glass fiber ribbon restorations are expected to improve the fatigue life and hence increase the lifespan of the restored teeth. The authors did not assess the fatigue life of the samples in the present study, and future studies are required in this respect.
The cost of FRC restorations in this study was 16.9% higher (due to materials and labor) compared to composite restorations. However, this increase in cost is justified, as the mean fracture resistance of the restored teeth increased from 7.7 MPa to 16.7 MPa. Additionally, the survival of the restored teeth is expected to increase significantly with fiber reinforcement.
Kirmah et al. [19] showed that using flowable composite with fiber under composite restorations significantly increased the fracture resistance of endodontically treated teeth with MOD cavities, and various fiber placement techniques can influence this increase in fracture resistance. In another study, Jafari Navimipour et al. [26] evaluated the effects of different fiber placement techniques on fracture resistance of maxillary premolars with MOD cavities. They reported that placing glass fibers from the buccal to the lingual wall increased the fracture resistance. Additionally, Patnana et al. [30] reported increased fracture resistance in reinforced restorations. In another study, Albar and khayat [31] found that placing polyethylene ribbons in axial walls significantly increased the fracture resistance of the samples, compared to other samples, including conventional composite restorations and fiber placement in the gingival and axial walls together with the gingival wall. Scotti et al. [32] also found that using fiber ribbons with different techniques in molars with MOD cavities significantly increased fracture resistance in fiber-reinforced samples, compared to conventional composite restorations. However, there was no significant difference among various techniques, including the use of fiber posts, mesiodistal glass fibers, and bucco-palatal glass fibers.
Nevertheless, there are still limitations in restoring large cavities such as MODs, which need to be considered. One of these limitations is the low fracture resistance of these restorations, which reduces the strength of the restoration against the forces of the masticatory system [33]. FRC restoration is one of the new methods to strengthen extensive restorations [34], as it reinforces the restoration from within [35]. The fibers commonly used for this purpose today are polyethylene ribbons and glass fibers. It has been shown that both types play a significant role in increasing the fracture resistance of restorations in both endodontically-treated and vital teeth [34].
Despite the significant difference between the composite restoration group and the FRC restoration group in this study, Daher et al. [36] reported no significant difference in fracture resistance among the groups in their study, although they reinforced the walls with glass fibers and used inlays and onlays in other groups. In their study, the fiber was used as a loop and in an X shape around the buccal and lingual walls. Increasing the number of layers and fibers, absence of cusp reduction, and use of molar teeth could be the reasons for lack of a significant difference between the test group and intact teeth and other groups in their study. In another study, Bahari et al. [37], concluded that despite reinforcing restorations with glass fibers on the occlusal surface or horizontally connecting the buccal and lingual walls, there was no significant difference in the study groups compared to the healthy teeth. The discrepancy between the results of their study and the present study could be due to the lack of identical preparation techniques and differences in fiber positioning.
Sengun et al. [38] also compared the fracture resistance of premolars restored with composite, with and without polyethylene fibers, and found no significant difference between the composite restoration group and the FRC group. In their study, the cavity preparation was more conservative and did not aim to achieve unsupported enamel. Additionally, the fiber was placed buccolingually on the occlusal surface, and the angle of placement in the universal testing machine was 45 degrees relative to the tooth's longitudinal axis. Cobankara et al. [39] conducted a study on endodontically-treated molars and found no significant difference in fracture resistance among the groups, which were restored with amalgam, inlay, composite alone, and composite reinforced with polyethylene fiber. The difference between the results of the two studies could be due to the lack of identical preparation and placing the samples against forces, which mimicked masticatory movements.
Conclusion
The results of this in vitro study demonstrated that the fracture resistance of unsupported enamel in FRC restorations significantly increased compared to the conventional composite restorations. However, FRC in deep MOD cavities failed to restore the fracture resistance of an intact tooth.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Deliperi S, Alleman D, Rudo D. Stress-reduced Direct Composites for the Restoration of Structurally Compromised Teeth: Fiber Design According to the "Wallpapering" Technique. Oper Dent. 2017 May/Jun;42(3):233-43. [DOI:10.2341/15-289-T] [PMID]
2. Silva LR, de Lima KL, Santos AA, Leles CR, Estrela C, de Freitas Silva BS, Yamamoto-Silva FP. Dentin thickness as a risk factor for vertical root fracture in endodontically treated teeth: a case-control study. Clin Oral Investig. 2021 Mar;25(3):1099-5. [DOI:10.1007/s00784-020-03406-1] [PMID]
3. Deliperi S. Direct fiber-reinforced composite restoration in an endodontically-treated molar: a three-year case report. Oper Dent. 2008 Mar-Apr;33(2):209-14. [DOI:10.2341/07-99]
4. El-Mowafy O, El-Badrawy W, Eltanty A, Abbasi K, Habib N. Gingival microleakage of Class II resin composite restorations with fiber inserts. Oper Dent. 2007 May-Jun;32(3):298-305. [DOI:10.2341/06-86] [PMID]
5. Pizzolotto L, Moraes RR. Resin Composites in Posterior Teeth: Clinical Performance and Direct Restorative Techniques. Dent J (Basel). 2022 Nov 27;10(12):222. [DOI:10.3390/dj10120222] [PMID] []
6. de Gee AF, Feilzer AJ, Davidson CL. True linear polymerization shrinkage of unfilled resins and composites determined with a linometer. Dent Mater. 1993 Jan;9(1):11-4. [DOI:10.1016/0109-5641(93)90097-A] [PMID]
7. Yu P, Xu YX, Liu YS. Polymerization shrinkage and shrinkage stress of bulk-fill and non-bulk-fill resin-based composites. J Dent Sci. 2022 Jul;17(3):1212-1216. [DOI:10.1016/j.jds.2021.12.004] []
8. Belli S, Erdemir A, Ozcopur M, Eskitascioglu G. The effect of fibre insertion on fracture resistance of root filled molar teeth with MOD preparations restored with composite. Int Endod J. 2005 Feb;38(2):73-80. [DOI:10.1111/j.1365-2591.2004.00892.x] [PMID]
9. Brännström M. Communication between the oral cavity and the dental pulp associated with restorative treatment. Oper Dent. 1984 Spring;9(2):57-68.
10. Askar H, Krois J, Göstemeyer G, Schwendicke F. Secondary caries risk of different adhesive strategies and restorative materials in permanent teeth: Systematic review and network meta-analysis. J Dent. 2021 Jan;104:103541. [DOI:10.1016/j.jdent.2020.103541]
11. Rudo DN, Karbhari VM. Physical behaviors of fiber reinforcement as applied to tooth stabilization. Dent Clin North Am. 1999 Jan;43(1):7-35. [DOI:10.1016/S0011-8532(22)00504-3]
12. Deliperi S, Bardwell DN, Coiana C. Reconstruction of devital teeth using direct fiber-reinforced composite resins: a case report. J Adhes Dent. 2005 Summer;7(2):165-71.
13. Safwat EM, Khater AG, Abd-Elsatar AG, Khater GA. Glass fiber-reinforced composites in dentistry. Bulletin of the National Research Centre. 2021 Dec;45:1-9. [DOI:10.1186/s42269-021-00650-7]
14. Bae JM, Kim KN, Hattori M, Hasegawa K, Yoshinari M, Kawada E, et al. The flexural properties of fiber-reinforced composite with light-polymerized polymer matrix. Int J Prosthodont. 2001 Jan-Feb;14(1):33-9.
15. Halpin JC, Thomas RL. Ribbon reinforcement of composites. Journal of Composite Materials. 1968 Oct;2(4):488-97. [DOI:10.1177/002199836800200409]
16. Neri H, Aripin D, Muryani A, Dharsono HDA, Yolanda Y, Mahyuddin AI. Stress Analysis on Mesiolingual Cavity of Endodontically Treated Molar Restored Using Bidirectional Fiber-Reinforced Composite (Wallpapering Technique). Clin Cosmet Investig Dent. 2024 Apr 13;16:75-89. [DOI:10.2147/CCIDE.S450325] [PMID] []
17. Fráter M, Sáry T, Vincze-Bandi E, Volom A, Braunitzer G, Szabó P B, et al. Fracture Behavior of Short Fiber-Reinforced Direct Restorations in Large MOD Cavities. Polymers (Basel). 2021 Jun 23;13(13):2040. [DOI:10.3390/polym13132040] [PMID] []
18. Jalalian SH, Emami Arjomand M, Mahavi A. Comparative Evaluation of Fracture Strength of Cusp Coverage with Composite Versus Unsupported Enamel Reinforced with Composite in Posterior Dental Restorations. Journal of Research in Dental and Maxillofacial Sciences. 2018 Oct 10;3(4):26-32. [DOI:10.29252/jrdms.3.4.26]
19. Kirmah O, Sahin O, Aytac F, Sari F, Tugut F, Kustarci A. Comparison of fracture resistance of endodontically treated teeth with MOD cavity using different techniques of fibre insertion. J Res Dent. 2014;2(3):144-48. [DOI:10.4103/2321-4619.143598]
20. Mondelli RF, Ishikiriama SK, de Oliveira Filho O, Mondelli J. Fracture resistance of weakened teeth restored with condensable resin with and without cusp coverage. J Appl Oral Sci. 2009 May-Jun;17(3):161-5. [DOI:10.1590/S1678-77572009000300006] [PMID] []
21. Moosavi H, Abedini S. The effect of various placement techniques on the microhardness of Class II (slot) resin composite restorations. J Contemp Dent Pract. 2009 Sep 1;10(5):E009-16. [DOI:10.5005/jcdp-10-5-8]
22. Sáry T, Garoushi S, Braunitzer G, Alleman D, Volom A, Fráter M. Fracture behaviour of MOD restorations reinforced by various fibre-reinforced techniques - An in vitro study. J Mech Behav Biomed Mater. 2019 Oct;98:348-56. [DOI:10.1016/j.jmbbm.2019.07.006] [PMID]
23. Everitt, B.S. and A. Skrondal, The Cambridge dictionary of statistics. 2010. [DOI:10.1017/CBO9780511779633]
24. El-Helali R, Dowling AH, McGinley EL, Duncan HF, Fleming GJ. Influence of resin-based composite restoration technique and endodontic access on cuspal deflection and cervical microleakage scores. J Dent. 2013 Mar;41(3):216-22. [DOI:10.1016/j.jdent.2012.11.002] [PMID]
25. Plotino G, Buono L, Grande NM, Lamorgese V, Somma F. Fracture resistance of endodontically treated molars restored with extensive composite resin restorations. J Prosthet Dent. 2008 Mar;99(3):225-32. [DOI:10.1016/S0022-3913(08)60047-5] [PMID]
26. Jafari Navimipour E, Ebrahimi Chaharom ME, Alizadeh Oskoee P, Mohammadi N, Bahari M, Firouzmandi M. Fracture Resistance of Endodontically-treated Maxillary Premolars Restored with Composite Resin along with Glass Fiber Insertion in Different Positions. J Dent Res Dent Clin Dent Prospects. 2012 Fall;6(4):125-30.
27. Interlig fiber glass catalogue, 2016; 6 (Link: https://api.compodent.com/storage/files/PDF/INTERLIG_Low.pdf)
28. Filtek composite datasheet; 2019(Link: https://multimedia.3m.com/mws/media/1354715O/technical-product-profile.pdf
29. 3M ESPE. 3M™ Single Bond Universal Adhesive:3M Company; 2014 (Link: https://multimedia.3m.com/mws/ media/1279637O/3m-single-bond-universal-adhesive- technical-product-profile.pdf)
30. Patnana AK, Vanga NRV, Vabbalareddy R, Chandrabhatla SK. Evaluating the fracture resistance of fiber reinforced composite restorations - An in vitro analysis. Indian J Dent Res. 2020 Jan-Feb;31(1):138-44. [DOI:10.4103/ijdr.IJDR_465_18] [PMID]
31. Albar NHM, Khayat WF. Evaluation of Fracture Strength of Fiber-Reinforced Direct Composite Resin Restorations: An In Vitro Study. Polymers (Basel). 2022 Oct 15;14(20):4339. [DOI:10.3390/polym14204339] [PMID] []
32. Scotti N, Forniglia A, Tempesta RM, Comba A, Saratti CM, Pasqualini D, et al. Effects of fiber-glass-reinforced composite restorations on fracture resistance and failure mode of endodontically treated molars. J Dent. 2016 Oct;53:82-7. [DOI:10.1016/j.jdent.2016.08.001] [PMID]
33. Lassila L, Keulemans F, Säilynoja E, Vallittu PK, Garoushi S. Mechanical properties and fracture behavior of flowable fiber reinforced composite restorations. Dent Mater. 2018 Apr;34(4):598-606. [DOI:10.1016/j.dental.2018.01.002] [PMID]
34. Mangoush E, Garoushi S, Lassila L, Vallittu PK, Säilynoja E. Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies. Polymers (Basel). 2021 Oct 26;13(21):3682. [DOI:10.3390/polym13213682] [PMID] []
35. Dyer SR, Lassila LV, Jokinen M, Vallittu PK. Effect of cross-sectional design on the modulus of elasticity and toughness of fiber-reinforced composite materials. J Prosthet Dent. 2005 Sep;94(3):219-26. [DOI:10.1016/j.prosdent.2005.06.008] [PMID]
36. Daher R, Ardu S, Di Bella E, Rocca GT, Feilzer AJ, Krejci I. Fracture strength of non-invasively reinforced MOD cavities on endodontically treated teeth. Odontology. 2021 Apr;109(2):368-75. [DOI:10.1007/s10266-020-00552-6] [PMID] []
37. Bahari M, Mohammadi N, Kimyai S, Kahnamoui MA, Vahedpour H, Torkani MA, et al AS. Effect of different fiber reinforcement strategies on the fracture strength of composite resin restored endodontically treated premolars. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2019 Oct 31;19:e4465. [DOI:10.4034/PBOCI.2019.191.99]
38. Sengun A, Cobankara FK, Orucoglu H. Effect of a new restoration technique on fracture resistance of endodontically treated teeth. Dent Traumatol. 2008 Apr;24(2):214-9. [DOI:10.1111/j.1600-9657.2007.00538.x] [PMID]
39. Cobankara FK, Unlu N, Cetin AR, Ozkan HB. The effect of different restoration techniques on the fracture resistance of endodontically-treated molars. Oper Dent. 2008 Sep-Oct;33(5):526-33. [DOI:10.2341/07-132] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |