Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 3 (9-2025)
J Res Dent Maxillofac Sci 2025, 10(3): 238-247 |
Back to browse issues page

Ethics code: IR.IAU.DENTAL.REC.1401.139
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seraj F, Tavassoli-Hojjati S. In Vitro Effects of Various Agents on Discoloration of Demineralized Enamel Caused by Silver Diamine Fluoride. J Res Dent Maxillofac Sci 2025; 10 (3) :238-247
URL: http://jrdms.dentaliau.ac.ir/article-1-750-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-750-en.html



1- Dentist, Private Practice, Tehran, Iran.
2- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran. ,saratavasolihojati@gmail.com
2- Department of Pediatric Dentistry, TeMS.C., Islamic Azad University, Tehran, Iran. ,
Keywords: Dental Caries, Hydrogen Peroxide, Potassium Iodide, Silver Diamine Fluoride, Spectrophotometry
Full-Text [PDF 503 kb]
(605 Downloads)
| Abstract (HTML) (1944 Views)
Table 1. Mean ∆L, ∆a, ∆b, and ∆E values after the application of SDF compared to baseline in the three groups (n=11)
Table 2. Mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared to baseline in the three groups (n=11)
Table 3. Mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared with after the application of SDF in the three groups (n=11)
Discussion
Full-Text: (488 Views)
Abstract
Background and Aim: Silver diamine fluoride (SDF) is effective for arresting dental caries. However, its application results in dark tooth discoloration, raising concerns among pediatric patients and their parents. This study assessed the effects of potassium iodide (KI) plus hydrogen peroxide (H2O2), H2O2, and Tooth Stain Remover (TSR) on SDF-induced discoloration of artificially demineralized permanent enamel.
Materials and Methods: In this in vitro study, the buccal surface enamel of 33 sound premolars was artificially demineralized and exposed to 38% SDF. The specimens were then randomly assigned to 3 groups of (I) KI + H2O2 (application of water-soluble KI followed by 35% H2O2 on the discolored surface for 3 minutes), (II) H2O2 (application of 35% H2O2 for three 20-minute cycles), and (III) TSR (application of TSR for 3 minutes on the discolored surface). The color parameters were measured at baseline, 1 week after the application of SDF, and 1 week after the application of the abovementioned bleaching agents by a spectrophotometer. Data were analyzed by ANOVA and Tukey test (alpha=0.05).
Results: SDF caused significant color change (ΔE) of demineralized enamel in all groups (ΔE=36-40), with no significant difference among the study groups (P=0.361). Application of all bleaching agents significantly resolved the dark discoloration in all groups, but KI + H2O2 was significantly more effective than H2O2 and TSR (P<0.001). TSR was the least effective (P<0.001).
Conclusion: Within the study limitations, the results showed optimal efficacy of KI + H2O2 for correction of 38% SDF-induced discoloration in artificially demineralized permanent enamel.
Keywords: Dental Caries; Hydrogen Peroxide; Potassium Iodide; Silver Diamine Fluoride; Spectrophotometry
Introduction
Materials and Methods: In this in vitro study, the buccal surface enamel of 33 sound premolars was artificially demineralized and exposed to 38% SDF. The specimens were then randomly assigned to 3 groups of (I) KI + H2O2 (application of water-soluble KI followed by 35% H2O2 on the discolored surface for 3 minutes), (II) H2O2 (application of 35% H2O2 for three 20-minute cycles), and (III) TSR (application of TSR for 3 minutes on the discolored surface). The color parameters were measured at baseline, 1 week after the application of SDF, and 1 week after the application of the abovementioned bleaching agents by a spectrophotometer. Data were analyzed by ANOVA and Tukey test (alpha=0.05).
Results: SDF caused significant color change (ΔE) of demineralized enamel in all groups (ΔE=36-40), with no significant difference among the study groups (P=0.361). Application of all bleaching agents significantly resolved the dark discoloration in all groups, but KI + H2O2 was significantly more effective than H2O2 and TSR (P<0.001). TSR was the least effective (P<0.001).
Conclusion: Within the study limitations, the results showed optimal efficacy of KI + H2O2 for correction of 38% SDF-induced discoloration in artificially demineralized permanent enamel.
Keywords: Dental Caries; Hydrogen Peroxide; Potassium Iodide; Silver Diamine Fluoride; Spectrophotometry
Introduction
Correction of dark discoloration of teeth caused by the application of silver diamine fluoride (SDF) is a challenge in minimally invasive dentistry. Minimally invasive dental procedures are ideal for patients with special needs or those with poor cooperation, since they enable caries cessation without the conventional restorative procedures. Application of SDF gained increasing popularity in dentistry after its approval by the American Food and Drug Administration in August 2014 [1]. SDF can remineralize the demineralized tooth structure and stop caries progression by the formation of silver phosphate and calcium fluoride deposits, and impairing the mechanism of action of cariogenic microorganisms [2]. Also, SDF can be used for treatment of dentin hypersensitivity [3]. However, its application results in permanent black discoloration of porous tooth structure and particularly incipient enamel lesions, which limits its clinical application due to esthetic concerns [4].
Application of potassium iodide (KI) is a suggested strategy to resolve the dark discoloration caused by the application of SDF, which results in formation of silver iodide (AgI) white deposits [5]. However, simultaneous application of SDF and KI decreases the free silver ions, and may significantly compromise the advantages of SDF in the long term [6]. Bleaching agents containing hydrogen peroxide (H2O2) improve tooth appearance by intrinsic color change of teeth. The bleaching effect of H2O2 on discoloration caused by SDF has been scarcely evaluated [7]. Nonetheless, it has been demonstrated that H2O2 can successfully correct intrinsic and extrinsic discolorations [8]. Addition of H2O2 to KI results in release of significant amounts of oxygen [9]. For persistent discolorations, tooth surface micro-abrasion by using 18% hydrochloric acid and pumice paste is recommended. This technique causes erosion and abrasion of the surface [10]. Tooth Stain Remover (TSR) is a solution containing 3% hydrochloric acid, which does not have the corrosiveness of micro-abrasion. The manufacturer claims that it eliminates tooth stains and corrects discolorations quickly without requiring pumice paste.
The effects of KI, H2O2, and hydrochloric acid on dark discolorations of permanent teeth and the durability of treatment over time have not been previously investigated. Thus, this study aimed to assess the effects of KI plus H2O2, H2O2, and TSR on SDF-induced discoloration of artificially demineralized permanent enamel.
Materials and Methods
Application of potassium iodide (KI) is a suggested strategy to resolve the dark discoloration caused by the application of SDF, which results in formation of silver iodide (AgI) white deposits [5]. However, simultaneous application of SDF and KI decreases the free silver ions, and may significantly compromise the advantages of SDF in the long term [6]. Bleaching agents containing hydrogen peroxide (H2O2) improve tooth appearance by intrinsic color change of teeth. The bleaching effect of H2O2 on discoloration caused by SDF has been scarcely evaluated [7]. Nonetheless, it has been demonstrated that H2O2 can successfully correct intrinsic and extrinsic discolorations [8]. Addition of H2O2 to KI results in release of significant amounts of oxygen [9]. For persistent discolorations, tooth surface micro-abrasion by using 18% hydrochloric acid and pumice paste is recommended. This technique causes erosion and abrasion of the surface [10]. Tooth Stain Remover (TSR) is a solution containing 3% hydrochloric acid, which does not have the corrosiveness of micro-abrasion. The manufacturer claims that it eliminates tooth stains and corrects discolorations quickly without requiring pumice paste.
The effects of KI, H2O2, and hydrochloric acid on dark discolorations of permanent teeth and the durability of treatment over time have not been previously investigated. Thus, this study aimed to assess the effects of KI plus H2O2, H2O2, and TSR on SDF-induced discoloration of artificially demineralized permanent enamel.
Materials and Methods
This in vitro, experimental study was conducted on 33 permanent maxillary and mandibular premolar teeth extracted within the past 3 months for orthodontic purposes. The study protocol was approved by the ethics committee of the university (IR.IAU.DENTAL.REC.1401.139).
Premolars with no caries, cracks, hypoplasia, and discoloration [11-13] that had been extracted for orthodontic purposes within the past 3 months [14-16] were collected.
The sample size was calculated to be 11 in each of the 3 groups according to a study by Rafiee et al, [17] using one-way ANOVA analysis of PASS 11, assuming α=0.05, β=0.2, and standard deviation of color change (∆E)=0.2.
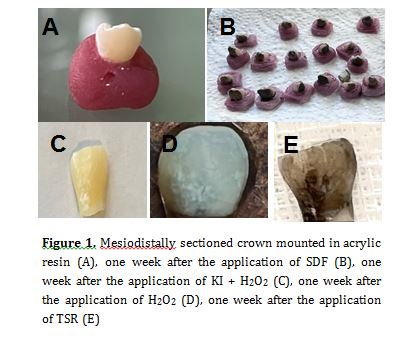
The collected teeth were inspected under a stereomicroscope (SZ240; Olympus, Tokyo, Japan) at x10 magnification to ensure their soundness and meet the eligibility criteria. The teeth were immersed in 0.5% chloramine T solution at room temperature for 7 days, and were then stored in distilled water at 4°C until the experiment [13-17]. The roots were then cut at 1 mm below the cementoenamel junction, and the crowns were split mesiodistally into buccal and lingual halves (Figure 1A). A window measuring 4 x 4 mm was created on the buccal surface of tooth crowns, and the entire buccal surface, except for the window, was coated with two layers of a colorless nail varnish (Nancy, Iran) [18]. The specimens were subsequently mounted in acrylic resin (Technovit 4000; Kulzer, Germany) such that their buccal surface remained exposed parallel to the mold surface [19].
The specimens were demineralized in a demineralizing solution composed of 2.2 mM KH2PO4, 2.2 mM CaCl2, and 50 mM acetate at a pH of 4.4 at 25°C for 4 days [11]. After demineralization, the specimens were rinsed with distilled water and dried. A microbrush was then used to apply 38% SDF (Advantage Arrest; Elevate Oral care, LLC, USA) on the created window on the buccal surface for 1 minute. The solution was reapplied several times within the first 30 seconds. Excess material was removed with a cotton pellet. The specimens were stored again in double-distilled water at room temperature for one week [20] (Figure 1B).
The teeth were first coded, and were then randomly assigned to 3 groups (n=11) of KI+ H2O2, H2O2, and TSR, using the Rand feature of Excel software.
KI + H2O2 group: 1.6 g of KI powder (Merck, Germany) was mixed with 0.5 mL of distilled water to obtain a paste-like consistency. The paste was applied on the discolored tooth, and 35% H2O2 (Whiteness HP; FGM, Joinville, SC, Brazil) with a pH of 6.0-8.5 was immediately added to it. After 5 minutes, it was rinsed with distilled water for 1 minute (according to the pilot study).
H2O2 group: 35% H2O2 was applied on the specimen surface with 0.5 to 1 mm thickness. After 20 minutes, the bleaching gel was gently removed by a cotton pellet. This process was repeated for 2 more times within the same session (a total of 60 minutes of treatment as instructed by the manufacturer). After the third round of bleaching, each specimen was rinsed with deionized water for 1 minute [7].
TSR: 3% HCl (Kemdent, UK) was applied on the specimen surface with a microbrush for 3 minutes, and was then rinsed with distilled water for 1 minute (according to the pilot study).
Prior to final color assessment, the specimens were immersed in double-distilled water at room temperature for one week [20, 21].
The color of the specimens was measured at baseline without any interventions, one week after the application of SDF, and one week after the application of bleaching agents at 26°C (Figure 1C, D, E). The examiner was blinded to the group allocation of the specimens. As instructed by the manufacturer, a piece of non-fluorescent Leneta paper was used in the background. The specimens were fixed on a jig, and a homogeneous light source (tungsten) illuminated the surface at a 45-degree angle relative to the longitudinal tooth axis. The spectrophotometer (CS-2000; Konica Minolta, Japan) was adjusted at zero-degree angle relative to the longitudinal axis at 70 cm distance with 0.1-degree viewing angle, creating a circle with 1.2 mm diameter at the center of the specimens. The spectrophotometer was calibrated prior to each measurement, and the color of each specimen was measured at the center of the middle third of the tooth surface at three points. The mean of the three values was calculated and reported.
The color parameters were measured under D65 viewing conditions of CS-S10W software according to the CIEL*a*b* color space. The L*, a*, and b* color parameters were recorded. L* indicates lightness and ranges from 0 (dark) to 100 (light); a* indicates redness-greenness, and b* indicates yellowness-blueness. ∆E of each specimen was calculated quantitatively using the following formula [22]:
∆E = [(L1-L2)2 + (a1-a2)2 + (b1-b2)2]1/2
Data were analyzed using SPSS version 26 (SPSS Inc., IL, USA). Normal distribution of data was confirmed by the Shapiro-Wilk test (P=0.187). Thus, comparisons were made by one-way ANOVA and Tukey HSD test at 0.05 level of significance.
Premolars with no caries, cracks, hypoplasia, and discoloration [11-13] that had been extracted for orthodontic purposes within the past 3 months [14-16] were collected.
The sample size was calculated to be 11 in each of the 3 groups according to a study by Rafiee et al, [17] using one-way ANOVA analysis of PASS 11, assuming α=0.05, β=0.2, and standard deviation of color change (∆E)=0.2.
The collected teeth were inspected under a stereomicroscope (SZ240; Olympus, Tokyo, Japan) at x10 magnification to ensure their soundness and meet the eligibility criteria. The teeth were immersed in 0.5% chloramine T solution at room temperature for 7 days, and were then stored in distilled water at 4°C until the experiment [13-17]. The roots were then cut at 1 mm below the cementoenamel junction, and the crowns were split mesiodistally into buccal and lingual halves (Figure 1A). A window measuring 4 x 4 mm was created on the buccal surface of tooth crowns, and the entire buccal surface, except for the window, was coated with two layers of a colorless nail varnish (Nancy, Iran) [18]. The specimens were subsequently mounted in acrylic resin (Technovit 4000; Kulzer, Germany) such that their buccal surface remained exposed parallel to the mold surface [19].
The specimens were demineralized in a demineralizing solution composed of 2.2 mM KH2PO4, 2.2 mM CaCl2, and 50 mM acetate at a pH of 4.4 at 25°C for 4 days [11]. After demineralization, the specimens were rinsed with distilled water and dried. A microbrush was then used to apply 38% SDF (Advantage Arrest; Elevate Oral care, LLC, USA) on the created window on the buccal surface for 1 minute. The solution was reapplied several times within the first 30 seconds. Excess material was removed with a cotton pellet. The specimens were stored again in double-distilled water at room temperature for one week [20] (Figure 1B).
The teeth were first coded, and were then randomly assigned to 3 groups (n=11) of KI+ H2O2, H2O2, and TSR, using the Rand feature of Excel software.
KI + H2O2 group: 1.6 g of KI powder (Merck, Germany) was mixed with 0.5 mL of distilled water to obtain a paste-like consistency. The paste was applied on the discolored tooth, and 35% H2O2 (Whiteness HP; FGM, Joinville, SC, Brazil) with a pH of 6.0-8.5 was immediately added to it. After 5 minutes, it was rinsed with distilled water for 1 minute (according to the pilot study).
H2O2 group: 35% H2O2 was applied on the specimen surface with 0.5 to 1 mm thickness. After 20 minutes, the bleaching gel was gently removed by a cotton pellet. This process was repeated for 2 more times within the same session (a total of 60 minutes of treatment as instructed by the manufacturer). After the third round of bleaching, each specimen was rinsed with deionized water for 1 minute [7].
TSR: 3% HCl (Kemdent, UK) was applied on the specimen surface with a microbrush for 3 minutes, and was then rinsed with distilled water for 1 minute (according to the pilot study).
Prior to final color assessment, the specimens were immersed in double-distilled water at room temperature for one week [20, 21].
The color of the specimens was measured at baseline without any interventions, one week after the application of SDF, and one week after the application of bleaching agents at 26°C (Figure 1C, D, E). The examiner was blinded to the group allocation of the specimens. As instructed by the manufacturer, a piece of non-fluorescent Leneta paper was used in the background. The specimens were fixed on a jig, and a homogeneous light source (tungsten) illuminated the surface at a 45-degree angle relative to the longitudinal tooth axis. The spectrophotometer (CS-2000; Konica Minolta, Japan) was adjusted at zero-degree angle relative to the longitudinal axis at 70 cm distance with 0.1-degree viewing angle, creating a circle with 1.2 mm diameter at the center of the specimens. The spectrophotometer was calibrated prior to each measurement, and the color of each specimen was measured at the center of the middle third of the tooth surface at three points. The mean of the three values was calculated and reported.
The color parameters were measured under D65 viewing conditions of CS-S10W software according to the CIEL*a*b* color space. The L*, a*, and b* color parameters were recorded. L* indicates lightness and ranges from 0 (dark) to 100 (light); a* indicates redness-greenness, and b* indicates yellowness-blueness. ∆E of each specimen was calculated quantitatively using the following formula [22]:
∆E = [(L1-L2)2 + (a1-a2)2 + (b1-b2)2]1/2
Data were analyzed using SPSS version 26 (SPSS Inc., IL, USA). Normal distribution of data was confirmed by the Shapiro-Wilk test (P=0.187). Thus, comparisons were made by one-way ANOVA and Tukey HSD test at 0.05 level of significance.
{kind=link}
∆E after the application of SDF compared with baseline:
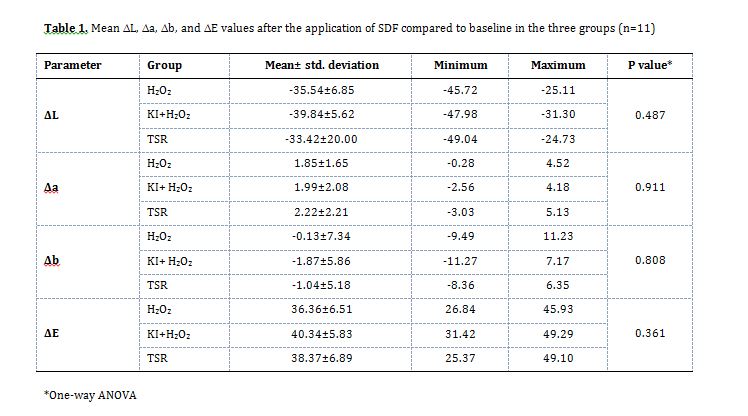
The mean ∆L, ∆a, ∆b, and ∆E values after the application of SDF compared with baseline in the three groups are presented in Table 1. One-way ANOVA revealed no significant difference in any parameter among the three groups [P>0.05].
∆E after the application of bleaching agents compared with baseline:
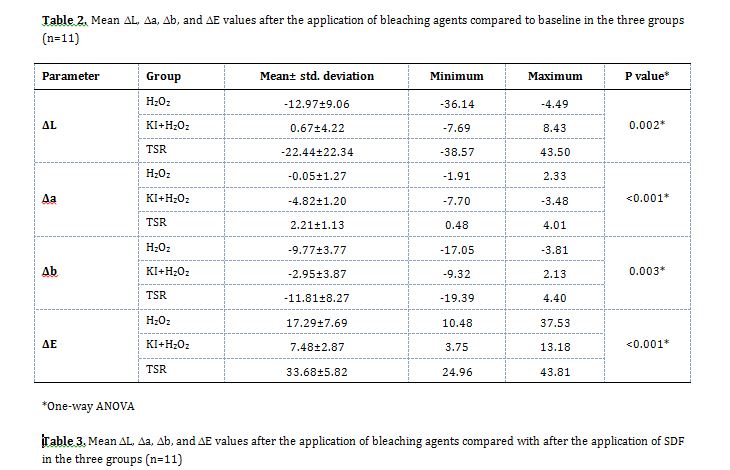
The mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared with baseline in the three groups are presented in Table 2. As shown, the lowest ∆L was recorded in the TSR group followed by the H2O2 group. The lowest ∆E belonged to the KI + H2O2 group, followed by the H2O2 group. One-way ANOVA revealed a significant difference in the mean ∆L (P=0.002), ∆a (P<0.001), ∆b (P=0.003), and ∆E (P<0.001) among the three groups. Pairwise comparisons by the Tukey HSD test indicated the following results:
∆L: The mean ∆L in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.002) but had no significant difference with ∆L in the H2O2 group (P=0.273). The difference in this parameter was not significant between KI + H2O2 and H2O2 groups (P=0.077).
∆a: The mean ∆a in the KI + H2O2 group was significantly lower than that in the H2O2 and TSR groups (P<0.001). The mean ∆a in the H2O2 group was lower than that in the TSR group (P<0.001).
∆b: The mean ∆b in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.003). The difference between the TSR and H2O2 groups was not significant (P=0.684). The mean ∆b in the H2O2 group was lower than that in the KI + H2O2 group (P=0.023).
∆E: The mean ∆E in the KI + H2O2 group was significantly lower than that in the H2O2 (P=0.001) and TSR (P<0.001) groups. The mean ∆E in the H2O2 group was significantly lower than that in the TSR group (P<0.001).
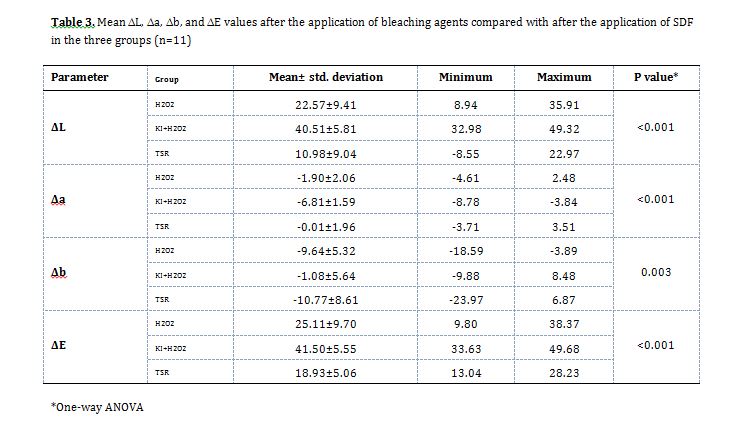
∆E after the application of bleaching agents compared with after the application of SDF:
As shown in Table 3, the lowest ∆L was recorded in the TSR group, followed by the H2O2 group. The lowest ∆E belonged to the TSR group, followed by the H2O2 group. The difference in ∆L (P<0.001), ∆a (P<0.001), ∆b (P=0.003), and ∆E (P<0.001) was significant among the three groups as shown by one-way ANOVA. Pairwise comparisons by the Tukey HSD test indicated the following results:
∆L: The mean ∆L in the TSR group was significantly lower than that in the KI + H2O2 (P<0.001) and H2O2 (P=0.007) groups. The mean ∆L in the H2O2 group was significantly lower than that in the KI + H2O2 group (P<0.001).
∆a: The mean ∆a in the KI + H2O2 group was significantly lower than that in the H2O2 and TSR groups (P<0.001). The mean ∆a in the H2O2 group had no significant difference with ∆a in the TSR group (P=0.062).
∆b: The mean ∆b in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.005). The difference between the TSR and H2O2 groups was not significant (P=0.918). The mean ∆b in the H2O2 group was significantly lower than that in the KI + H2O2 group (P=0.014).
∆E: The mean ∆E in the TSR group was significantly lower than that in the KI + H2O2 group (P<0.001). The difference between the TSR and H2O2 groups was not significant (P=0.119). The mean ∆E in the H2O2 group was significantly lower than that in the KI + H2O2 group (P<0.001).
The mean ∆L, ∆a, ∆b, and ∆E values after the application of SDF compared with baseline in the three groups are presented in Table 1. One-way ANOVA revealed no significant difference in any parameter among the three groups [P>0.05].
∆E after the application of bleaching agents compared with baseline:
The mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared with baseline in the three groups are presented in Table 2. As shown, the lowest ∆L was recorded in the TSR group followed by the H2O2 group. The lowest ∆E belonged to the KI + H2O2 group, followed by the H2O2 group. One-way ANOVA revealed a significant difference in the mean ∆L (P=0.002), ∆a (P<0.001), ∆b (P=0.003), and ∆E (P<0.001) among the three groups. Pairwise comparisons by the Tukey HSD test indicated the following results:
∆L: The mean ∆L in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.002) but had no significant difference with ∆L in the H2O2 group (P=0.273). The difference in this parameter was not significant between KI + H2O2 and H2O2 groups (P=0.077).
∆a: The mean ∆a in the KI + H2O2 group was significantly lower than that in the H2O2 and TSR groups (P<0.001). The mean ∆a in the H2O2 group was lower than that in the TSR group (P<0.001).
∆b: The mean ∆b in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.003). The difference between the TSR and H2O2 groups was not significant (P=0.684). The mean ∆b in the H2O2 group was lower than that in the KI + H2O2 group (P=0.023).
∆E: The mean ∆E in the KI + H2O2 group was significantly lower than that in the H2O2 (P=0.001) and TSR (P<0.001) groups. The mean ∆E in the H2O2 group was significantly lower than that in the TSR group (P<0.001).
∆E after the application of bleaching agents compared with after the application of SDF:
As shown in Table 3, the lowest ∆L was recorded in the TSR group, followed by the H2O2 group. The lowest ∆E belonged to the TSR group, followed by the H2O2 group. The difference in ∆L (P<0.001), ∆a (P<0.001), ∆b (P=0.003), and ∆E (P<0.001) was significant among the three groups as shown by one-way ANOVA. Pairwise comparisons by the Tukey HSD test indicated the following results:
∆L: The mean ∆L in the TSR group was significantly lower than that in the KI + H2O2 (P<0.001) and H2O2 (P=0.007) groups. The mean ∆L in the H2O2 group was significantly lower than that in the KI + H2O2 group (P<0.001).
∆a: The mean ∆a in the KI + H2O2 group was significantly lower than that in the H2O2 and TSR groups (P<0.001). The mean ∆a in the H2O2 group had no significant difference with ∆a in the TSR group (P=0.062).
∆b: The mean ∆b in the TSR group was significantly lower than that in the KI + H2O2 group (P=0.005). The difference between the TSR and H2O2 groups was not significant (P=0.918). The mean ∆b in the H2O2 group was significantly lower than that in the KI + H2O2 group (P=0.014).
∆E: The mean ∆E in the TSR group was significantly lower than that in the KI + H2O2 group (P<0.001). The difference between the TSR and H2O2 groups was not significant (P=0.119). The mean ∆E in the H2O2 group was significantly lower than that in the KI + H2O2 group (P<0.001).
Table 1. Mean ∆L, ∆a, ∆b, and ∆E values after the application of SDF compared to baseline in the three groups (n=11)
{kind=link}
Table 2. Mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared to baseline in the three groups (n=11)
{kind=link}
Table 3. Mean ∆L, ∆a, ∆b, and ∆E values after the application of bleaching agents compared with after the application of SDF in the three groups (n=11)
{kind=link}
Discussion
This study assessed the effects of KI plus H2O2, H2O2, and TSR on SDF-induced discoloration of artificially demineralized permanent enamel. A spectrophotometer, as an ISO-approved gold standard, was used for color assessment in the present study [23,24]. ∆E below 3.3 is not often detected by the untrained eye [25, 26], and ∆E values up to 6.8 are considered clinically acceptable [11]. In the present study, 38% SDF was used since evidence shows that it can effectively stop caries progression in primary and permanent teeth [27,28]. One drop of SDF contains 9.5 mg SDF, which is 50 times lower than the toxic dose of fluoride, and 400 times lower than the toxic dose of silver [29]. The present results indicated that application of SDF on demineralized enamel caused a significant dark discoloration in all groups, with no significant difference among the three groups. Zhao et al. [11] measured the depth of enamel demineralization to be 70-100 µm at 4 days after immersion in an artificial cariogenic solution at 25°C. The penetration depth of SDF in permanent teeth is 25 to 200 µm [17]. Evidence shows that 38% SDF with a pH of 10 contains silver (24.4%-28.8% w/v) and fluoride (5.0%-5.9%) ions, and penetrates into the porous tooth structure and forms silver phosphate (Ag3PO4), calcium fluoride (CaF2), and fluorapatite [Ca10(PO4)6F2] [17,30]. Discoloration by SDF occurs as a result of oxidation of silver ions to metal silver and silver oxide, and deposition of silver proteins and silver phosphate complexes on the tooth structure [31]. Ag3PO4 is light yellow in color, which becomes dark following exposure to sunlight and air [32].
The present results indicated significant resolution of discoloration in all groups with KI + H2O2 resulting in significantly superior color correction than H2O2 and TSR. Also, KI + H2O2 was significantly more effective than H2O2 and TSR in regaining the baseline color. Although the ΔE in the KI + H2O2 group was > 3.3, it was close to the clinically acceptable threshold [11]. KI includes 76% iodine and 23% potassium, and forms a white crystalline, and transparent salt. KI is sensitive to light, has hygroscopic properties, and is highly water-soluble. Application of KI along with SDF results in formation of silver iodide (AgI), which is yellow and insoluble, and prevents dark discoloration to some extent. The results regarding the efficacy of SDF along with KI for caries cessation are controversial. A previous study showed that KI decreased the cariostatic effect of SDF by reducing the number of silver ions [32]. Application of KI immediately after SDF acceptably decreased the formation of black stains, compared with the application of SDF alone in some previous studies [20, 33]. However, long-term assessments (12, 24 or 30 months) revealed that KI was not effective for color correction, and the tooth color became darker over time [34].
In the present study, water-soluble KI was used along with 35% H2O2 for only 5 minutes. Demineralized enamel becomes dark after exposure to SDF due to the formation of Ag2O and Ag3PO4. H2O2 in combination with KI solution generates oxygen gas, which forms bubbles. Also, this reaction leads to formation of I2, which causes a brownish discoloration. Ag2O and Ag3PO4 break down in presence of oxygen ions, and form white silver iodide following reaction with I2, creating a color shift in tooth structure from black to white. The reactions may be explained as follows:
At first, KI serves as a catalyst and does not participate in the reaction. 2H2O2+KI=>O2+2H2O+KI.
When KI is subjected to oxidizing conditions in presence of H2O2, the following reaction occurs:
2 KI+H2O2 → 2 KOH+I2
Next, at a pH<7, and following the breakdown of H2O2, the following reaction occurs:
Ag2O+2I- → 2 AgI+H2O, which is almost non-reversible [35].
The present results revealed that 35% H2O2 corrected the discoloration caused by penetration of silver ions into enamel porosities after demineralization; however, this effect was significantly lower than that of KI + H2O2. Studies on the bleaching effect of H2O2 on SDF-induced discolorations are limited [7, 17]. Al-Angari et al. [7] evaluated the effects of 40% H2O2 and 15% carbamide peroxide (CP) for color correction of discolorations due to metallic and non-metallic stains. They reported that metallic stains caused darker discolorations than non-metallic stains and were significantly more resistant to bleaching. They showed that home bleaching with 15% CP had superior bleaching effects on metallic stains than 40% H2O2. However, the teeth treated with CP had lower resistance to acid attacks due to long-term exposure to peroxide, and were at higher risk of demineralization. Peroxides have higher capacity for oxidation of organic chromogens present in non-metallic stains, while metallic compounds such as silver compounds are not easily degraded by oxidation [7, 36]. Rafiee et al. [17] demonstrated that application of 10% CP for 2 to 3 weeks on demineralized primary teeth discolored by SDF resolved their discoloration. However, they only assessed the ΔE between the bleaching stage and SDF, and did not assess the post-bleaching/baseline ΔE. Thus, it was not clarified that to what extent bleaching regained the baseline color.
The present results indicated that TSR had a significantly lower efficacy than H2O2 and KI + H2O2 for correction of discoloration caused by SDF. TSR contains 3% hydrochloric acid and is effective on dark and particularly black dental stains. Search of the literature by the authors yielded no study on the application of TSR. However, a pilot study was conducted before the main study, which showed that application of TSR for 5 minutes was effective for correction of SDF black stains. The present results showed that TSR application caused significant correlation of SDF discoloration. However, it could not regain the baseline color. Hydrochloric acid is a transparent, colorless solution with a strong odor that is prepared by addition of hydrogen chloride (HCl) to water. It is a strong corrosive acid with a pH of 0 to 2. It appears that the acidic and corrosive effect of hydrochloric acid eliminates the superficial layer, resulting in acid penetration by 60 µm, and subsequent color correction [37]. In summary, the current result indicated that KI + H2O2, with a significant improvement in color and the lowest ΔE, showed a significant difference in all three indices of Δa, Δb, and ΔL compared to H2O2 and TSR.
Previously, it was assumed that the discoloration caused by SDF is constant and permanent [5]. The present study was the first to report the application of KI in addition to H2O2 and showed its optimal efficacy for correction of SDF-induced discolorations and almost restoring the baseline color, which was a major strength of the present study. Future studies are required to assess the effect of this combination on mineral content of enamel and its resistance to demineralization.
This study had some limitations as well. The in vitro design limits the generalizability of the findings. Also, the possible effect of heat generated from the reaction of KI with H2O2 on dental pulp is still unknown. Furthermore, this reaction generates high amounts of oxygen, which may affect the pulp or cause hypersensitivity, and needs to be further investigated. Moreover, future studies should better simulate the clinical setting by thermocycling to obtain more reliable results.
Conclusion
The present results indicated significant resolution of discoloration in all groups with KI + H2O2 resulting in significantly superior color correction than H2O2 and TSR. Also, KI + H2O2 was significantly more effective than H2O2 and TSR in regaining the baseline color. Although the ΔE in the KI + H2O2 group was > 3.3, it was close to the clinically acceptable threshold [11]. KI includes 76% iodine and 23% potassium, and forms a white crystalline, and transparent salt. KI is sensitive to light, has hygroscopic properties, and is highly water-soluble. Application of KI along with SDF results in formation of silver iodide (AgI), which is yellow and insoluble, and prevents dark discoloration to some extent. The results regarding the efficacy of SDF along with KI for caries cessation are controversial. A previous study showed that KI decreased the cariostatic effect of SDF by reducing the number of silver ions [32]. Application of KI immediately after SDF acceptably decreased the formation of black stains, compared with the application of SDF alone in some previous studies [20, 33]. However, long-term assessments (12, 24 or 30 months) revealed that KI was not effective for color correction, and the tooth color became darker over time [34].
In the present study, water-soluble KI was used along with 35% H2O2 for only 5 minutes. Demineralized enamel becomes dark after exposure to SDF due to the formation of Ag2O and Ag3PO4. H2O2 in combination with KI solution generates oxygen gas, which forms bubbles. Also, this reaction leads to formation of I2, which causes a brownish discoloration. Ag2O and Ag3PO4 break down in presence of oxygen ions, and form white silver iodide following reaction with I2, creating a color shift in tooth structure from black to white. The reactions may be explained as follows:
At first, KI serves as a catalyst and does not participate in the reaction. 2H2O2+KI=>O2+2H2O+KI.
When KI is subjected to oxidizing conditions in presence of H2O2, the following reaction occurs:
2 KI+H2O2 → 2 KOH+I2
Next, at a pH<7, and following the breakdown of H2O2, the following reaction occurs:
Ag2O+2I- → 2 AgI+H2O, which is almost non-reversible [35].
The present results revealed that 35% H2O2 corrected the discoloration caused by penetration of silver ions into enamel porosities after demineralization; however, this effect was significantly lower than that of KI + H2O2. Studies on the bleaching effect of H2O2 on SDF-induced discolorations are limited [7, 17]. Al-Angari et al. [7] evaluated the effects of 40% H2O2 and 15% carbamide peroxide (CP) for color correction of discolorations due to metallic and non-metallic stains. They reported that metallic stains caused darker discolorations than non-metallic stains and were significantly more resistant to bleaching. They showed that home bleaching with 15% CP had superior bleaching effects on metallic stains than 40% H2O2. However, the teeth treated with CP had lower resistance to acid attacks due to long-term exposure to peroxide, and were at higher risk of demineralization. Peroxides have higher capacity for oxidation of organic chromogens present in non-metallic stains, while metallic compounds such as silver compounds are not easily degraded by oxidation [7, 36]. Rafiee et al. [17] demonstrated that application of 10% CP for 2 to 3 weeks on demineralized primary teeth discolored by SDF resolved their discoloration. However, they only assessed the ΔE between the bleaching stage and SDF, and did not assess the post-bleaching/baseline ΔE. Thus, it was not clarified that to what extent bleaching regained the baseline color.
The present results indicated that TSR had a significantly lower efficacy than H2O2 and KI + H2O2 for correction of discoloration caused by SDF. TSR contains 3% hydrochloric acid and is effective on dark and particularly black dental stains. Search of the literature by the authors yielded no study on the application of TSR. However, a pilot study was conducted before the main study, which showed that application of TSR for 5 minutes was effective for correction of SDF black stains. The present results showed that TSR application caused significant correlation of SDF discoloration. However, it could not regain the baseline color. Hydrochloric acid is a transparent, colorless solution with a strong odor that is prepared by addition of hydrogen chloride (HCl) to water. It is a strong corrosive acid with a pH of 0 to 2. It appears that the acidic and corrosive effect of hydrochloric acid eliminates the superficial layer, resulting in acid penetration by 60 µm, and subsequent color correction [37]. In summary, the current result indicated that KI + H2O2, with a significant improvement in color and the lowest ΔE, showed a significant difference in all three indices of Δa, Δb, and ΔL compared to H2O2 and TSR.
Previously, it was assumed that the discoloration caused by SDF is constant and permanent [5]. The present study was the first to report the application of KI in addition to H2O2 and showed its optimal efficacy for correction of SDF-induced discolorations and almost restoring the baseline color, which was a major strength of the present study. Future studies are required to assess the effect of this combination on mineral content of enamel and its resistance to demineralization.
This study had some limitations as well. The in vitro design limits the generalizability of the findings. Also, the possible effect of heat generated from the reaction of KI with H2O2 on dental pulp is still unknown. Furthermore, this reaction generates high amounts of oxygen, which may affect the pulp or cause hypersensitivity, and needs to be further investigated. Moreover, future studies should better simulate the clinical setting by thermocycling to obtain more reliable results.
Conclusion
Within the limitations of this in vitro study, the results showed optimal efficacy of KI + H2O2 for correction of discoloration caused by SDF in artificially demineralized permanent enamel. H2O2 was less effective than KI+H2O2, and more effective than TSR for this purpose.
Type of Study: Original article |
Subject:
pediatric
References
1. Varughese A, Janakiram C, Varma B, Mathew A, Venugopalan SR, Ramanarayanan V, et al. Effectiveness of 38% Silver Diamine Fluoride Application along with Atraumatic Restorative Treatment for Arresting Caries in Permanent Teeth When Compared to Atraumatic Restorative Treatment in Adults-Study Protocol for a Randomized Controlled Trial. Methods Protoc. 2022 Oct 26;5(6):87. [DOI:10.3390/mps5060087] [PMID] []
2. Chu CH, Mei L, Seneviratne CJ, Lo EC. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int J Paediatr Dent. 2012 Jan;22(1):2-10. [DOI:10.1111/j.1365-263X.2011.01149.x] [PMID]
3. Kim S, Nassar M, Tamura Y, Hiraishi N, Jamleh A, Nikaido T, Tagami J. The effect of reduced glutathione on the toxicity of silver diamine fluoride in rat pulpal cells. J Appl Oral Sci. 2021 Apr 19;29:e20200859. [DOI:10.1590/1678-7757-2020-0859] [PMID] []
4. Vennela E, Sharada J, Hasanuddin S, Suhasini K, Hemachandrika I, Singh PT. Comparison of staining potential of silver diamine fluoride versus silver diamine fluoride and potassium iodide under tooth-colored restorations: An in vitro study. J Indian Soc Pedod Prev Dent. 2021 Jan-Mar;39(1):47-52. [DOI:10.4103/jisppd.jisppd_533_20] [PMID]
5. Detsomboonrat P, Thongmak P, Lertpayab P, Aiemsri W, Sooampon S. Optimal concentration of potassium iodide to reduce the black staining of silver diamine fluoride. J Dent Sci. 2022 Jan;17(1):300-7. [DOI:10.1016/j.jds.2021.03.014] [PMID] []
6. Sayed M, Matsui N, Hiraishi N, Nikaido T, Burrow MF, Tagami J. Effect of Glutathione Bio-Molecule on Tooth Discoloration Associated with Silver Diammine Fluoride. Int J Mol Sci. 2018 Apr 29;19(5):1322. [DOI:10.3390/ijms19051322] [PMID] []
7. Al-Angari SS, Lippert F, Platt JA, Eckert GJ, González-Cabezas C, Li Y, Hara AT. Dental bleaching efficacy and impact on demineralization susceptibility of simulated stained-remineralized caries lesions. J Dent. 2019 Feb;81:59-63. [DOI:10.1016/j.jdent.2018.12.008] [PMID]
8. Irusa K, Abd Alrahaem I, Ngoc CN, Donovan T. Tooth whitening procedures: A narrative review. Dentistry Review. 2022 Sep 1;2(3):100055. [DOI:10.1016/j.dentre.2022.100055]
9. Dalmázio I, Moura FC, Araújo MH, Alves T, Lago RM, Lima GF, et al. The iodide-catalyzed decomposition of hydrogen peroxide: Mechanistic details of an old reaction as revealed by electrospray ionization mass spectrometry monitoring. Journal of the Brazilian Chemical Society. 2008;19:1105-10. [DOI:10.1590/S0103-50532008000600008]
10. Silva PL, Maciel PP, Martins LB, Carvalho FG, Santos RL, Medeiros ES, et al. Weight-loss and surface roughness of enamel after microabrasion procedure with different agents. Revista de Odontologia da UNESP. 2021 Oct 25;50:e20210020. [DOI:10.1590/1807-2577.02021]
11. Zhao IS, Yin IX, Mei ML, Lo ECM, Tang J, Li Q, So LY, et al. Remineralising Dentine Caries Using Sodium Fluoride with Silver Nanoparticles: An In Vitro Study. Int J Nanomedicine. 2020 Apr 23;15:2829-39. [DOI:10.2147/IJN.S247550] [PMID] []
12. Turton B, Horn R, Durward C. Caries arrest and lesion appearance using two different silver fluoride therapies on primary teeth with and without potassium iodide: 12-month results. Clin Exp Dent Res. 2021 Aug;7(4):609-19. [DOI:10.1002/cre2.367] [PMID] []
13. Ghadirian H, Geramy A, Shallal W, Heidari S, Noshiri N, Keshvad MA. The Effect of Remineralizing Agents With/Without CO2 Laser Irradiation on Structural and Mechanical Properties of Enamel and its Shear Bond Strength to Orthodontic Brackets. J Lasers Med Sci. 2020 Spring;11(2):144-52.. [DOI:10.34172/jlms.2020.25] [PMID] []
14. Firouzmandi M, Mohaghegh M, Jafarpisheh M. Effect of silver diamine fluoride on the bond durability of normal and carious dentin. J Clin Exp Dent. 2020 May 1;12(5):e468-e473. [DOI:10.4317/jced.56303] [PMID] []
15. Burns J, Hollands K. Nano Silver Fluoride for preventing caries. Evid Based Dent. 2015 Mar;16(1):8-9. [DOI:10.1038/sj.ebd.6401073] [PMID]
16. Duangthip D, Chu CH, Lo EC. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides--18 month results. J Dent. 2016 Jan;44:57-63. [DOI:10.1016/j.jdent.2015.05.006] [PMID]
17. Rafiee A, Memarpour M, Benam H. Evaluation of bleaching agent effects on color and microhardness change of silver diamine fluoride-treated demineralized primary tooth enamel: An in vitro study. BMC Oral Health. 2022 Aug 12;22(1):347. [DOI:10.1186/s12903-022-02371-3] [PMID] []
18. Pani SC, Alenazi FM, Alotain AM, Alanazi HD, Alasmari AS. Extrinsic tooth staining potential of high dose and sustained release iron syrups on primary teeth. BMC oral health. 2015 Dec;15:1-6. [DOI:10.1186/s12903-015-0072-0] [PMID] []
19. Mehran MA, Bassir MM, Jafari SE. Effect of two kinds of iron drops on the discoloration, atomic absorption and structural changes of primary teeth enamel. Journal of Dental Medicine. 2009 Mar 1;21(4).
20. Patel J, Anthonappa RP, King NM. Evaluation of the staining potential of silver diamine fluoride: in vitro. Int J Paediatr Dent. 2018 Jul 4. [DOI:10.1111/ipd.12401] [PMID]
21. Xavier SR, Pilownic KJ, Gastmann AH, Echeverria MS, Romano AR, Geraldo Pappen F. Bovine Tooth Discoloration Induced by Endodontic Filling Materials for Primary Teeth. Int J Dent. 2017;2017:7401962. [DOI:10.1155/2017/7401962] [PMID] []
22. Lertsukprasert N, Locharoenrat K. Efficiency of tooth bleaching agent on staining and discoloration characteristics of nicotine stained dental enamel model. BMC Oral Health. 2020 Aug 10;20(1):221. [DOI:10.1186/s12903-020-01207-2] [PMID] []
23. Madani Z, Alvandifar S, Bizhani A. Evaluation of tooth discoloration after treatment with mineral trioxide aggregate, calcium-enriched mixture, and Biodentine® in the presence and absence of blood. Dent Res J (Isfahan). 2019 Nov 12;16(6):377-83. [DOI:10.4103/1735-3327.270787] [PMID] []
24. Mutlu ŞN, Akbulut MB. Tooth Discoloration Effect of BIOfactor Mineral Trioxide Aggregate: A 6-Month In Vitro Study. Applied Sciences. 2023 Aug 2;13(15):8914.. [DOI:10.3390/app13158914]
25. Ellakany P, Madi M, Aly NM, Al-Aql ZS, AlGhamdi M, AlJeraisy A, Alagl AS. Effect of CAD/CAM Ceramic Thickness on Shade Masking Ability of Discolored Teeth: In Vitro Study. Int J Environ Res Public Health. 2021 Dec 18;18(24):13359. [DOI:10.3390/ijerph182413359] [PMID] []
26. Możyńska J, Metlerski M, Lipski M, Nowicka A. Tooth Discoloration Induced by Different Calcium Silicate-based Cements: A Systematic Review of In Vitro Studies. J Endod. 2017 Oct;43(10):1593-601. [DOI:10.1016/j.joen.2017.04.002] [PMID]
27. Zaffarano L, Salerno C, Campus G, Cirio S, Balian A, Karanxha L, Cagetti MG. Silver Diamine Fluoride (SDF) Efficacy in Arresting Cavitated Caries Lesions in Primary Molars: A Systematic Review and Metanalysis. Int J Environ Res Public Health. 2022 Oct 9;19(19):12917. [DOI:10.3390/ijerph191912917] [PMID] []
28. Muntean A, Mzoughi SM, Pacurar M, Candrea S, Inchingolo AD, Inchingolo AM, et al. Silver Diamine Fluoride in Pediatric Dentistry: Effectiveness in Preventing and Arresting Dental Caries-A Systematic Review. Children (Basel). 2024 Apr 22;11(4):499. [DOI:10.3390/children11040499] [PMID] []
29. Punyanirun K, Yospiboonwong T, Kunapinun T, Thanyasrisung P, Trairatvorakul C. Silver diamine fluoride remineralized artificial incipient caries in permanent teeth after bacterial pH-cycling in-vitro. J Dent. 2018 Feb;69:55-9. [DOI:10.1016/j.jdent.2017.09.005] [PMID]
30. Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment - a systematic review. BMC Oral Health. 2016 Feb 1;16:12. [DOI:10.1186/s12903-016-0171-6] [PMID] []
31. Lee KE, Erdenebulgan M, Kang CM, Jung HI, Song JS. Effect of Silver Diamine Fluoride and Potassium Iodide Solution on Enamel Remineralization and Discoloration in Artificial Caries. Materials (Basel). 2022 Jun 27;15(13):4523. [DOI:10.3390/ma15134523] [PMID] []
32. Mouafy NM, Ezz El Din S, Shash RY, Wassef N. Microhardness and Bacterial Inhibitory Effect of Riva Star versus Silver Diamine Fluoride on Carious Dentin of Primary Teeth (In-vitro study). Advanced Dental Journal. 2023 Apr 1;5(2):442-8. [DOI:10.21608/adjc.2023.196751.1271]
33. Nguyen V, Neill C, Felsenfeld J, Primus C. Potassium iodide. The solution to silver diamine fluoride discoloration. Health. 2017;5(1):555655. [DOI:10.19080/ADOH.2017.05.555655]
34. Li R, Lo EC, Liu BY, Wong MC, Chu CH. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J Dent. 2016 Aug;51:15-20. [DOI:10.1016/j.jdent.2016.05.005] [PMID]
35. Krausmann E, Drossinos Y. A model of silver-iodine reactions in a light water reactor containment sump under severe accident conditions. Journal of nuclear materials. 1999 Jan 1;264(1-2):113-21. [DOI:10.1016/S0022-3115(98)00471-1]
36. Alqahtani MQ. Tooth-bleaching procedures and their controversial effects: A literature review. Saudi Dent J. 2014 Apr;26(2):33-46. [DOI:10.1016/j.sdentj.2014.02.002] [PMID] []
37. Feiz A, Barekatain B, Khalesi S, Khalighinejad N, Badrian H, Swift EJ. Effect of several bleaching agents on teeth stained with a resin-based sealer. Int Endod J. 2014 Jan;47(1):3-9. [DOI:10.1111/iej.12116] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |