Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 4 (12-2024)
J Res Dent Maxillofac Sci 2024, 9(4): 222-232 |
Back to browse issues page

Ethics code: IR.SBMU.DRC.REC.1402.006
Clinical trials code: IRCT20190313043046N2
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esmaeilzadeh M, Mahdavi N S, Fallahinejad Ghajari M, soleymani A, Eghbali A, Faghihi T. Comparative Efficacy of Buccal Infiltration Anesthesia with Articaine and Inferior Alveolar Nerve Block with Lidocaine for Pulpotomy of Primary Mandibular Second Molars Under Sedation: A Clinical Trial. J Res Dent Maxillofac Sci 2024; 9 (4) :222-232
URL: http://jrdms.dentaliau.ac.ir/article-1-594-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-594-en.html
Mohammad Esmaeilzadeh1 

 , Nastaran Sadat Mahdavi2 , Masoud Fallahinejad Ghajari1 , Aliasghar Soleymani1 , Ahmad Eghbali3 , Taraneh Faghihi *4
, Nastaran Sadat Mahdavi2 , Masoud Fallahinejad Ghajari1 , Aliasghar Soleymani1 , Ahmad Eghbali3 , Taraneh Faghihi *4
, Nastaran Sadat Mahdavi2 , Masoud Fallahinejad Ghajari1 , Aliasghar Soleymani1 , Ahmad Eghbali3 , Taraneh Faghihi *4
1- Department of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- DDepartment of Anesthesiology, School of Medicine, Mofid Children’s Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Anesthesiology Research Center, Mofid Children Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,trnfaghihi@gmail.com
2- DDepartment of Anesthesiology, School of Medicine, Mofid Children’s Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Anesthesiology Research Center, Mofid Children Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 785 kb]
(1015 Downloads)
| Abstract (HTML) (3185 Views)
Full-Text: (832 Views)
Abstract
Background and Aim: This study compared the efficacy of buccal infiltration anesthesia (BIA) with articaine versus inferior alveolar nerve block (IANB) with lidocaine for pulpotomy of primary mandibular second molars under intravenous sedation.
Materials and Methods: This split-mouth randomized clinical trial was conducted on 29 uncooperative children (Frankl scores I & II) between 3-6 years with bilateral primary mandibular second molars requiring pulpotomy. After intravenous sedation, one random quadrant received IANB with 2% lidocaine and the respective tooth underwent pulpotomy with mineral trioxide aggregate and subsequent coronal restoration with a stainless-steel crown. The other quadrant received BIA with 4% articaine in the next session for pulpotomy of the respective tooth. The behavior of children was evaluated right after receiving the sedative (T0), during anesthetic injection (T1), during pulp exposure (T2), and in the recovery room (T3) using non-verbal pain scale-revised (NVPS-R). Data were analyzed by one-way and two-way repeated measures ANOVA (alpha=0.05).
Results: The odds of calmness of children during the entire procedure were 1.7 times higher in BIA than IANB but this difference was not significant (P=0.061). The mean heart rate (HR) of children was generally higher in IANB than BIA (P=0.04 at T1, P<0.001 at T2, and P=0.01 at T3). The effect of time on HR was also significant (P<0.001). Blood oxygen saturation rate (SPO2) was higher in BIA than IANB during the procedure (P<0.001).
Conclusion: BIA with articaine had optimal efficacy comparable to that of IANB with lidocaine for pulpotomy of primary second molars under sedation.
Keywords: Anesthesia, Local; articaine; Deep Sedation; Lidocaine; Mandibular Nerve; Pulpotomy
Introduction
Non-pharmaceutical behavioral control methods such as verbal communication, positive reinforcement, and proper pain control are among the proposed methods for reduction and management of dental fear and anxiety [1, 2]. Nonetheless, pharmaceutical behavioral control techniques such as sedation or general anesthesia may be necessarily required for some young and highly anxious children, those with systemic underlying conditions, or patients with mental retardation [3, 4].
Deep sedation is defined as suppression of the central nervous system while preserving the respiratory and cardiovascular function. It controls the anxiety and unwanted patient movements and aids the clinician in provision of optimal-quality treatment.
Pain control during the procedure directly affects the quality of sedation. Pain experience during the procedure can have different effects on the vital signs of patients [5]. Severe pain during the procedure can increase the heart rate (HR), blood pressure, respiratory rate, and contraction of the respiratory muscles, and decrease the blood oxygen saturation rate (SPO2) as such [6].
One adopted strategy to control unwanted patient movements caused by pain during dental procedures under sedation is to increase the dosage of the sedative; however, it can intensify the unwanted complications and side effects of the sedative, and complicate and prolong the recovery period [5]. A more practical and logical alternative is to induce deep local anesthesia prior to the onset of treatment to minimize pain experience by patient during the entire sedation period [7]. Type of local anesthetic agent and its injection technique are among the influential factors in achieving a successful anesthesia [8].
Lidocaine is currently the safest and most commonly used amide dental anesthetic agent [9]. However, articaine has also gained recent popularity as an amide anesthetic agent due to its unique pharmacological properties [10]. Replacement of the aromatic ring with a thiophene ring in its structure increases its lipid solubility and is responsible for its higher potency than lidocaine (1.5 times higher). Thus, a lower dosage of articaine, compared with lidocaine, is required for anesthesia induction in one quadrant [11]. This structural change is also responsible for the faster onset and longer effect of articaine. Thus, it has a more predictable diffusion in hard and soft tissues compared with other anesthetic agents [10]. The majority of studies comparing the efficacy of lidocaine and articaine have been conducted on conscious children with good cooperation, and their efficacy in non-cooperative sedated children has not been well compared. Also, care must be taken not to exceed the safe volume of anesthetic agent in uncooperative children with high number of carious teeth in all four quadrants; to do so, the most efficient technique should be adopted with the minimum volume of anesthetic agent possible.
The technique of injection is another influential factor in the quality of anesthesia. Inferior alveolar nerve block (IANB) is the most commonly adopted injection technique for anesthesia induction in the mandible. IANB anesthetizes the mandibular teeth, lower lip, and chin at the injection side. The success rate of IANB ranges from 80%-85% [12]. Hematoma, trismus, accidental intravenous injection in case of no aspiration and the resultant drug overdose (which is particularly important in children under sedation) are among the drawbacks of IANB [13].
Buccal infiltration anesthesia (BIA) is defined as direct injection of the anesthetic agent into the vestibule at the site of respective tooth. The volume of the anesthetic agent used in this technique is lower than that used in IANB. Also, shorter needles are used in BIA, and it is less invasive than the IANB [12]. In BIA, injection next to each tooth results in its anesthesia. In primary dentition, the adjacent mesial tooth is also usually anesthetized due to thinness of bone and better penetration of anesthetic agent. Therefore, there is no need for repeated injections for each tooth in sedated patients [12].
Considering the lower thickness of the mandible in children than adults, BIA may be a suitable alternative to IANB. Considering the limitations for the safe volume of local anesthetic agents in children under sedation, and high number of teeth in need of treatment in such patients, articaine may be a suitable alternative to lidocaine for them since it can be used in a smaller volume due to its higher lipid solubility, better tissue diffusion, and higher potency. Considering the shortcomings of IANB, this study aimed to compare the efficacy of BIA with articaine versus IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation. The null hypothesis of the study was that the efficacy of BIA with articaine would not be significantly different from that of IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation.
Materials and Methods
This study was conducted at the Pediatric Dentistry Department of School of Dentistry, Shahid Beheshti University of Medical Sciences from June 2023 to September 2023. The study protocol was approved by the ethics committee of the university (IR.SBMU.DRC.REC.1402.006) and registered in the Iranian Registry of Clinical Trials (IRCT20190313043046N2).
Trial design:
A randomized double-blind split-mouth clinical trial was designed in which the patients underwent pulpotomy of primary mandibular second molars following an IANB with lidocaine in one quadrant and following a BIA with articaine in the other quadrant in two different sessions. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were uncooperative children with negative or completely negative behavior according to the Frankl behavior rating scale (Frankl scores I & II) [14], age between 3-6 years, ASA Class I systemic health condition, having carious mandibular second molars bilaterally with no clinical or radiographic symptoms requiring pulpotomy after caries removal, requiring at least 2 similar treatment sessions with local anesthesia under sedation, no history of clinical signs/symptoms such as spontaneous pain, soft tissue swelling, fistula, mobility of primary mandibular second molars, and unusual bleeding during access cavity preparation, no radiographic findings such as internal or external pathological resorption, periapical or furcation radiolucencies, physiological resorption of more than one-third of the root length, and no history of common cold in the past 14 days, or drug allergy to anesthetic agents or sedatives.
The sample consisted of 30 uncooperative children between 3 to 6 years presenting to the Pediatric Dentistry Department of School of Dentistry of Shahid Beheshti University of Medical Sciences requiring pulpotomy of primary second molars bilaterally under sedation.
Interventions:
After obtaining written informed consent from the parents for dental treatment of their children and their study enrollment, the children underwent precise medical examination by a medical practitioner with a fellowship in pediatric anesthesia to ensure their general health status (ASA Class I) and meet the eligibility criteria. The parents received thorough oral and written instructions prior to treatment. Accordingly, the children had to refrain from eating solid foods and non-human milk for 8 hours prior to sedation, and clear liquids for 2 hours prior to sedation [8].
In the recovery room, 0.3 mg/kg oral midazolam (Tehran Chemie, Tehran, Iran) along with 2 cc of 50% dextrose solution (to improve its taste) were gently poured into the children’s mouth by a syringe as premedication to induce a mild sedation. After 30 minutes, the child was seated on the dental unit with the help of a parent. A venous catheter was then placed, and sedation was induced by ketamine (Rotexmedica, Germany) at a titrated dose of 1-2 mg/kg and propofol (Dongkook Pharma. Co., Ltd., South Korea) at a titrated dose of 1-2 mg/kg. Atropine (Alborz Daru) was also injected at a dosage of 0.02 mg/kg. Sedation was maintained with propofol continuous infusion at a rate of 25-100 µg/kg/minute. An additional dose of propofol and ketamine was administered if the patient regained consciousness or moved during the dental procedure. During the entire procedure (from baseline to discharge), a pulse oximeter probe (Alborz Medical Equipment, Iran) was placed on the children’s index finger to monitor their vital signs such as HR and SPO2. Moreover, oxygen was administered through a nasal cannula at a flow rate of 3-5 L/min to maintain optimal level of SPO2. In the first treatment session, one quadrant of the mandible was randomly selected for local anesthesia with either an IANB with one cartridge of 2% lidocaine (Darupakhsh, Iran) or BIA with half of a cartridge of 4% articaine (Darupakhsh) [15]. All injections were performed by a 30-gauge needle with no topical anesthesia. The second treatment session was scheduled after a one-week period, for treatment of the other quadrant of the mandible with the other anesthetic technique/agent. The dental procedure in both treatment sessions included pulpotomy of a primary mandibular second molar tooth. The two treatment sessions were the same in terms of type and duration of treatment, and each session took approximately 30 minutes. During the procedure, additional dosage of medications was administered if required.
For pulpotomy of the respective teeth, caries was first removed by a large round bur with a low-speed hand-piece (TizKaavan, Iran). After access cavity preparation by a round bur and high-speed hand-piece (TizKaavan, Iran) and removal of the coronal inflamed pulp, hemostasis was achieved by a moist cotton pellet. Next, mineral trioxide aggregate (Angelus, Londrina, PR, Brazil) was placed over the pulp tissue at the orifice. Zonalin (Zoliran, Golchai, Iran) was placed in the pulp chamber, and the tooth was restored with a stainless-steel crown (3M) and glass ionomer cement (GC, Japan).
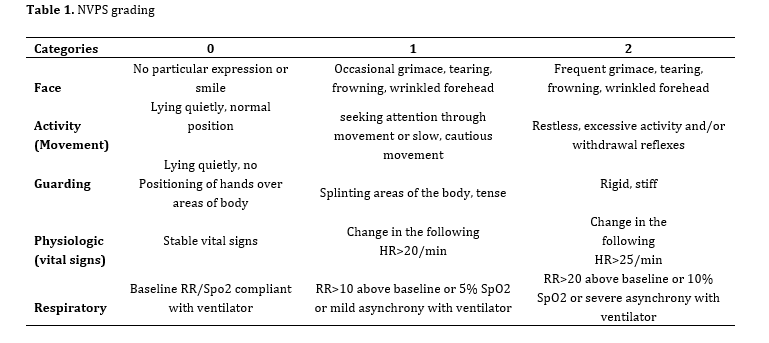
The behavior of children was evaluated by using the non-verbal pain scale-revised (NVPS-R), which included behavioral parameters (facial expression, activity, and resistance of the child) and physiological parameters including HR and SPO2 using a monitoring machine (Alborz Medical Equipment, Iran) (Table 1) [16]. The behavior of children was evaluated right after receiving the sedative (T0), during anesthetic injection (T1), during pulp exposure (T2), and in the recovery room (T3). Assessments were performed by a pediatric dentist blindly. Also, a pediatric anesthesiology fellow and an anesthesia technician evaluated and recorded the behavior of children. BP was monitored every 15 minutes with a child-size blood pressure cuff. Respiratory rate was also controlled during the entire time of deep sedation by a pediatric anesthesiologist. After stabilization of the vital signs and relative regaining of consciousness, the patient was transferred to the recovery room by a parent, and was under supervision of a pediatric anesthesiology fellow until meeting the discharge criteria, including full consciousness, cardiovascular and respiratory stability, and suitable reactions to stimuli.
Table 1. NVPS grading
Outcomes (primary and secondary):
HR, SPO2, and patient movements were the primary outcomes in this study. There was no secondary outcome.
Sample size calculation:
The sample size was calculated to be 28 according to a previous study [17] assuming alpha=0.05, beta=0.1, study power of 90%, mean difference of 1.2 units, and standard deviation of 0.2 for the dependent variable with the highest standard deviation and the lowest mean difference.
Interim analyses and stopping guidelines:
No interim analyses were performed, and no stopping guidelines were established.
Randomization:
Random allocation of the anesthesia techniques to the quadrants was performed by tossing a coin. For allocation concealment, sealed envelopes with a random sequence were used, which were randomly delivered to each patient in the first treatment session by the assistant.
Blinding:
This study had a single-blind design since the assessor who evaluated the outcomes was an anesthetic technician blinded to the group allocation of the quadrants.
Statistical analysis:
Normal distribution of data was evaluated by the Kolmogorov-Smirnov and Shapiro-Wilk tests. Paired samples t-test or Wilcoxon signed-rank test was used to compare the effects of anesthesia techniques on dependent variables. Repeated measures two-way ANOVA was applied to analyze the simultaneous effect of time and anesthesia technique on the variables. Generalized estimating equation (GEE) was used to analyze the results regarding patient movement since it was a qualitative ordinal variable and also due to cluster data. Pairwise comparisons were performed by the Bonferroni test. All statistical analyses were performed using SPSS version 25 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
Participant flow:
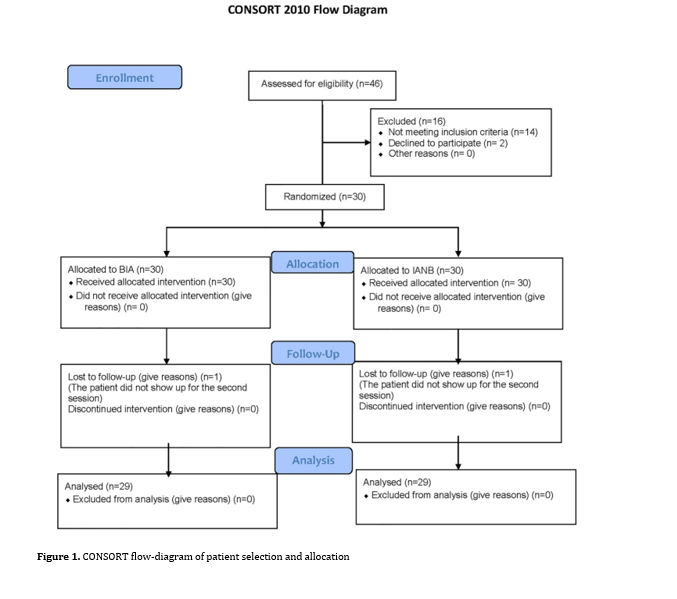
The sample consisted of 30 children including 12 girls (41.4%) and 17 boys (58.6%) with a mean age of 4.52±1.35 years (3 to 7 years), and a mean weight of 17.53±3.37 kg (12.5 to 26 kg). One child did not show up for the second treatment session and was excluded. Thus, the data of 29 children were statistically analyzed. Figure 1 shows the CONSORT flow diagram of patient selection and allocation.
Primary outcomes:
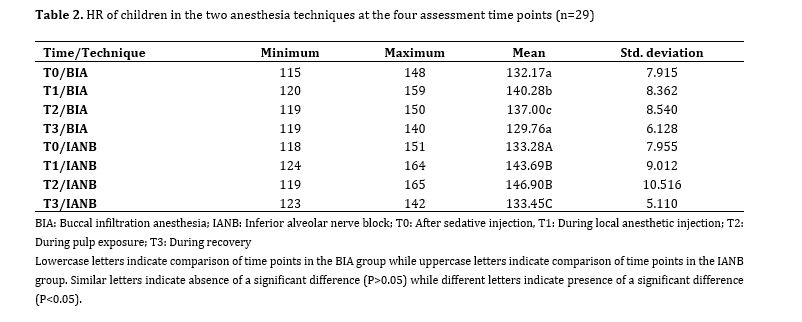
HR: Table 2 presents the HR of children in the two anesthesia techniques at the four assessment time points. Considering the normal distribution of HR data, two-way repeated measures ANOVA was applied to analyze the effects of time and anesthesia technique on the HR, which showed the significant effect of anesthesia technique on the HR (P=0.001), such that BIA caused a significantly smaller increase in HR than the IANB. The effect of time on the HR was also significant (P<0.001), such that the mean HR first increased and then decreased. The interaction effect of time and anesthesia technique on the HR was also significant (P<0.001), indicating that the mean HR was different between the two groups at different time points.
Comparison of the mean HR at different time points between the two techniques by paired t-test showed that the difference in HR was not significant between the two groups at T0 (P=0.419). However, the mean HR was significantly higher in the IANB group than the BIA group at T1 (P=0.04), T2 (P<0.001), and T3 (P=0.01).
Background and Aim: This study compared the efficacy of buccal infiltration anesthesia (BIA) with articaine versus inferior alveolar nerve block (IANB) with lidocaine for pulpotomy of primary mandibular second molars under intravenous sedation.
Materials and Methods: This split-mouth randomized clinical trial was conducted on 29 uncooperative children (Frankl scores I & II) between 3-6 years with bilateral primary mandibular second molars requiring pulpotomy. After intravenous sedation, one random quadrant received IANB with 2% lidocaine and the respective tooth underwent pulpotomy with mineral trioxide aggregate and subsequent coronal restoration with a stainless-steel crown. The other quadrant received BIA with 4% articaine in the next session for pulpotomy of the respective tooth. The behavior of children was evaluated right after receiving the sedative (T0), during anesthetic injection (T1), during pulp exposure (T2), and in the recovery room (T3) using non-verbal pain scale-revised (NVPS-R). Data were analyzed by one-way and two-way repeated measures ANOVA (alpha=0.05).
Results: The odds of calmness of children during the entire procedure were 1.7 times higher in BIA than IANB but this difference was not significant (P=0.061). The mean heart rate (HR) of children was generally higher in IANB than BIA (P=0.04 at T1, P<0.001 at T2, and P=0.01 at T3). The effect of time on HR was also significant (P<0.001). Blood oxygen saturation rate (SPO2) was higher in BIA than IANB during the procedure (P<0.001).
Conclusion: BIA with articaine had optimal efficacy comparable to that of IANB with lidocaine for pulpotomy of primary second molars under sedation.
Keywords: Anesthesia, Local; articaine; Deep Sedation; Lidocaine; Mandibular Nerve; Pulpotomy
Introduction
Non-pharmaceutical behavioral control methods such as verbal communication, positive reinforcement, and proper pain control are among the proposed methods for reduction and management of dental fear and anxiety [1, 2]. Nonetheless, pharmaceutical behavioral control techniques such as sedation or general anesthesia may be necessarily required for some young and highly anxious children, those with systemic underlying conditions, or patients with mental retardation [3, 4].
Deep sedation is defined as suppression of the central nervous system while preserving the respiratory and cardiovascular function. It controls the anxiety and unwanted patient movements and aids the clinician in provision of optimal-quality treatment.
Pain control during the procedure directly affects the quality of sedation. Pain experience during the procedure can have different effects on the vital signs of patients [5]. Severe pain during the procedure can increase the heart rate (HR), blood pressure, respiratory rate, and contraction of the respiratory muscles, and decrease the blood oxygen saturation rate (SPO2) as such [6].
One adopted strategy to control unwanted patient movements caused by pain during dental procedures under sedation is to increase the dosage of the sedative; however, it can intensify the unwanted complications and side effects of the sedative, and complicate and prolong the recovery period [5]. A more practical and logical alternative is to induce deep local anesthesia prior to the onset of treatment to minimize pain experience by patient during the entire sedation period [7]. Type of local anesthetic agent and its injection technique are among the influential factors in achieving a successful anesthesia [8].
Lidocaine is currently the safest and most commonly used amide dental anesthetic agent [9]. However, articaine has also gained recent popularity as an amide anesthetic agent due to its unique pharmacological properties [10]. Replacement of the aromatic ring with a thiophene ring in its structure increases its lipid solubility and is responsible for its higher potency than lidocaine (1.5 times higher). Thus, a lower dosage of articaine, compared with lidocaine, is required for anesthesia induction in one quadrant [11]. This structural change is also responsible for the faster onset and longer effect of articaine. Thus, it has a more predictable diffusion in hard and soft tissues compared with other anesthetic agents [10]. The majority of studies comparing the efficacy of lidocaine and articaine have been conducted on conscious children with good cooperation, and their efficacy in non-cooperative sedated children has not been well compared. Also, care must be taken not to exceed the safe volume of anesthetic agent in uncooperative children with high number of carious teeth in all four quadrants; to do so, the most efficient technique should be adopted with the minimum volume of anesthetic agent possible.
The technique of injection is another influential factor in the quality of anesthesia. Inferior alveolar nerve block (IANB) is the most commonly adopted injection technique for anesthesia induction in the mandible. IANB anesthetizes the mandibular teeth, lower lip, and chin at the injection side. The success rate of IANB ranges from 80%-85% [12]. Hematoma, trismus, accidental intravenous injection in case of no aspiration and the resultant drug overdose (which is particularly important in children under sedation) are among the drawbacks of IANB [13].
Buccal infiltration anesthesia (BIA) is defined as direct injection of the anesthetic agent into the vestibule at the site of respective tooth. The volume of the anesthetic agent used in this technique is lower than that used in IANB. Also, shorter needles are used in BIA, and it is less invasive than the IANB [12]. In BIA, injection next to each tooth results in its anesthesia. In primary dentition, the adjacent mesial tooth is also usually anesthetized due to thinness of bone and better penetration of anesthetic agent. Therefore, there is no need for repeated injections for each tooth in sedated patients [12].
Considering the lower thickness of the mandible in children than adults, BIA may be a suitable alternative to IANB. Considering the limitations for the safe volume of local anesthetic agents in children under sedation, and high number of teeth in need of treatment in such patients, articaine may be a suitable alternative to lidocaine for them since it can be used in a smaller volume due to its higher lipid solubility, better tissue diffusion, and higher potency. Considering the shortcomings of IANB, this study aimed to compare the efficacy of BIA with articaine versus IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation. The null hypothesis of the study was that the efficacy of BIA with articaine would not be significantly different from that of IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation.
Materials and Methods
This study was conducted at the Pediatric Dentistry Department of School of Dentistry, Shahid Beheshti University of Medical Sciences from June 2023 to September 2023. The study protocol was approved by the ethics committee of the university (IR.SBMU.DRC.REC.1402.006) and registered in the Iranian Registry of Clinical Trials (IRCT20190313043046N2).
Trial design:
A randomized double-blind split-mouth clinical trial was designed in which the patients underwent pulpotomy of primary mandibular second molars following an IANB with lidocaine in one quadrant and following a BIA with articaine in the other quadrant in two different sessions. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were uncooperative children with negative or completely negative behavior according to the Frankl behavior rating scale (Frankl scores I & II) [14], age between 3-6 years, ASA Class I systemic health condition, having carious mandibular second molars bilaterally with no clinical or radiographic symptoms requiring pulpotomy after caries removal, requiring at least 2 similar treatment sessions with local anesthesia under sedation, no history of clinical signs/symptoms such as spontaneous pain, soft tissue swelling, fistula, mobility of primary mandibular second molars, and unusual bleeding during access cavity preparation, no radiographic findings such as internal or external pathological resorption, periapical or furcation radiolucencies, physiological resorption of more than one-third of the root length, and no history of common cold in the past 14 days, or drug allergy to anesthetic agents or sedatives.
The sample consisted of 30 uncooperative children between 3 to 6 years presenting to the Pediatric Dentistry Department of School of Dentistry of Shahid Beheshti University of Medical Sciences requiring pulpotomy of primary second molars bilaterally under sedation.
Interventions:
After obtaining written informed consent from the parents for dental treatment of their children and their study enrollment, the children underwent precise medical examination by a medical practitioner with a fellowship in pediatric anesthesia to ensure their general health status (ASA Class I) and meet the eligibility criteria. The parents received thorough oral and written instructions prior to treatment. Accordingly, the children had to refrain from eating solid foods and non-human milk for 8 hours prior to sedation, and clear liquids for 2 hours prior to sedation [8].
In the recovery room, 0.3 mg/kg oral midazolam (Tehran Chemie, Tehran, Iran) along with 2 cc of 50% dextrose solution (to improve its taste) were gently poured into the children’s mouth by a syringe as premedication to induce a mild sedation. After 30 minutes, the child was seated on the dental unit with the help of a parent. A venous catheter was then placed, and sedation was induced by ketamine (Rotexmedica, Germany) at a titrated dose of 1-2 mg/kg and propofol (Dongkook Pharma. Co., Ltd., South Korea) at a titrated dose of 1-2 mg/kg. Atropine (Alborz Daru) was also injected at a dosage of 0.02 mg/kg. Sedation was maintained with propofol continuous infusion at a rate of 25-100 µg/kg/minute. An additional dose of propofol and ketamine was administered if the patient regained consciousness or moved during the dental procedure. During the entire procedure (from baseline to discharge), a pulse oximeter probe (Alborz Medical Equipment, Iran) was placed on the children’s index finger to monitor their vital signs such as HR and SPO2. Moreover, oxygen was administered through a nasal cannula at a flow rate of 3-5 L/min to maintain optimal level of SPO2. In the first treatment session, one quadrant of the mandible was randomly selected for local anesthesia with either an IANB with one cartridge of 2% lidocaine (Darupakhsh, Iran) or BIA with half of a cartridge of 4% articaine (Darupakhsh) [15]. All injections were performed by a 30-gauge needle with no topical anesthesia. The second treatment session was scheduled after a one-week period, for treatment of the other quadrant of the mandible with the other anesthetic technique/agent. The dental procedure in both treatment sessions included pulpotomy of a primary mandibular second molar tooth. The two treatment sessions were the same in terms of type and duration of treatment, and each session took approximately 30 minutes. During the procedure, additional dosage of medications was administered if required.
For pulpotomy of the respective teeth, caries was first removed by a large round bur with a low-speed hand-piece (TizKaavan, Iran). After access cavity preparation by a round bur and high-speed hand-piece (TizKaavan, Iran) and removal of the coronal inflamed pulp, hemostasis was achieved by a moist cotton pellet. Next, mineral trioxide aggregate (Angelus, Londrina, PR, Brazil) was placed over the pulp tissue at the orifice. Zonalin (Zoliran, Golchai, Iran) was placed in the pulp chamber, and the tooth was restored with a stainless-steel crown (3M) and glass ionomer cement (GC, Japan).
The behavior of children was evaluated by using the non-verbal pain scale-revised (NVPS-R), which included behavioral parameters (facial expression, activity, and resistance of the child) and physiological parameters including HR and SPO2 using a monitoring machine (Alborz Medical Equipment, Iran) (Table 1) [16]. The behavior of children was evaluated right after receiving the sedative (T0), during anesthetic injection (T1), during pulp exposure (T2), and in the recovery room (T3). Assessments were performed by a pediatric dentist blindly. Also, a pediatric anesthesiology fellow and an anesthesia technician evaluated and recorded the behavior of children. BP was monitored every 15 minutes with a child-size blood pressure cuff. Respiratory rate was also controlled during the entire time of deep sedation by a pediatric anesthesiologist. After stabilization of the vital signs and relative regaining of consciousness, the patient was transferred to the recovery room by a parent, and was under supervision of a pediatric anesthesiology fellow until meeting the discharge criteria, including full consciousness, cardiovascular and respiratory stability, and suitable reactions to stimuli.
Table 1. NVPS grading
{kind=link}
Outcomes (primary and secondary):
HR, SPO2, and patient movements were the primary outcomes in this study. There was no secondary outcome.
Sample size calculation:
The sample size was calculated to be 28 according to a previous study [17] assuming alpha=0.05, beta=0.1, study power of 90%, mean difference of 1.2 units, and standard deviation of 0.2 for the dependent variable with the highest standard deviation and the lowest mean difference.
Interim analyses and stopping guidelines:
No interim analyses were performed, and no stopping guidelines were established.
Randomization:
Random allocation of the anesthesia techniques to the quadrants was performed by tossing a coin. For allocation concealment, sealed envelopes with a random sequence were used, which were randomly delivered to each patient in the first treatment session by the assistant.
Blinding:
This study had a single-blind design since the assessor who evaluated the outcomes was an anesthetic technician blinded to the group allocation of the quadrants.
Statistical analysis:
Normal distribution of data was evaluated by the Kolmogorov-Smirnov and Shapiro-Wilk tests. Paired samples t-test or Wilcoxon signed-rank test was used to compare the effects of anesthesia techniques on dependent variables. Repeated measures two-way ANOVA was applied to analyze the simultaneous effect of time and anesthesia technique on the variables. Generalized estimating equation (GEE) was used to analyze the results regarding patient movement since it was a qualitative ordinal variable and also due to cluster data. Pairwise comparisons were performed by the Bonferroni test. All statistical analyses were performed using SPSS version 25 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
Participant flow:
The sample consisted of 30 children including 12 girls (41.4%) and 17 boys (58.6%) with a mean age of 4.52±1.35 years (3 to 7 years), and a mean weight of 17.53±3.37 kg (12.5 to 26 kg). One child did not show up for the second treatment session and was excluded. Thus, the data of 29 children were statistically analyzed. Figure 1 shows the CONSORT flow diagram of patient selection and allocation.
Primary outcomes:
HR: Table 2 presents the HR of children in the two anesthesia techniques at the four assessment time points. Considering the normal distribution of HR data, two-way repeated measures ANOVA was applied to analyze the effects of time and anesthesia technique on the HR, which showed the significant effect of anesthesia technique on the HR (P=0.001), such that BIA caused a significantly smaller increase in HR than the IANB. The effect of time on the HR was also significant (P<0.001), such that the mean HR first increased and then decreased. The interaction effect of time and anesthesia technique on the HR was also significant (P<0.001), indicating that the mean HR was different between the two groups at different time points.
Comparison of the mean HR at different time points between the two techniques by paired t-test showed that the difference in HR was not significant between the two groups at T0 (P=0.419). However, the mean HR was significantly higher in the IANB group than the BIA group at T1 (P=0.04), T2 (P<0.001), and T3 (P=0.01).
{kind=link}
Considering the significant interaction effect of time and technique of anesthesia on the HR, within-group comparisons were also performed for each anesthesia technique using one-way repeated measures ANOVA. The results showed a significant change in HR over time in the BIA group (P<0.05). Pairwise comparisons of the HR at different time points in the BIA group by the Bonferroni test showed that the mean HR at T0 was significantly lower than that at T1 and T2 (both P<0.001) and significantly higher than that at T3 (P=0.029). The difference in HR between T1 and T2 was not significant (P>0.05), but the mean HR at T1 and T2 was significantly higher than that at T3 (P<0.05).
Comparison of the mean HR at different time points in the IANB group showed a significant difference (P<0.001). The HR at T0 was significantly lower than that at T1 and T2 (P<0.05) but the difference between T0 and T3 was not significant (P>0.05). The HR at T1 was significantly lower than that at T2 (P<0.05). The HR at T1 was significantly higher than that at T3 (P<0.05). The difference in HR between T2 and T3 was also significant (P<0.05).
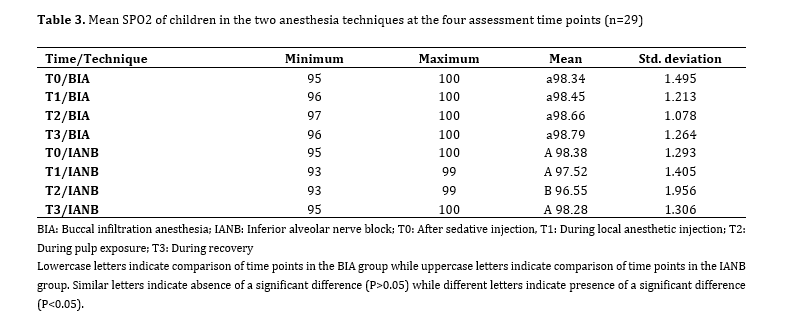
SPO2: Table 3 presents the mean SPO2 of children in the two anesthesia techniques at the four assessment time points. Two-way repeated measures ANOVA showed the significant effect of anesthesia technique on the SPO2 (P<0.001) such that the mean SPO2 was higher in the BIA technique compared with IANB (P<0.001). The effect of time on the SPO2 was also significant such that its trend of change was variable over time (P<0.001). The interaction effect of time and technique of anesthesia on the SPO2 was also significant (P=0.003). Thus, paired t-test was applied to compare the SPO2 between the two techniques at each time point, which showed that the difference between the two techniques was not significant at T0 (P=0.931) or T3 (P=0.117). However, the mean SPO2 was significantly lower in the IANB group than the BIA group at T1 (P=0.025) and T2 (P<0.001).
One-way repeated measures ANOVA showed that the change in SPO2 was not significant in BIA group over time (P=0.489). However, its trend of change was significant in the IANB group (P<0.001). Comparison of the SPO2 in the IANB group at different time points by the Bonferroni test showed no significant difference between T0 and T1 (P=0.089), or T0 and T3 (P=1.000). However, the mean SPO2 at T0 was significantly higher than that at T2 (P=0.001). The difference between T1 and T2 (P=0.267), or T1 and T3 (P=0.335) was not significant, but the mean SPO2 at T2 was significantly lower than that at T3 (P=0.008).
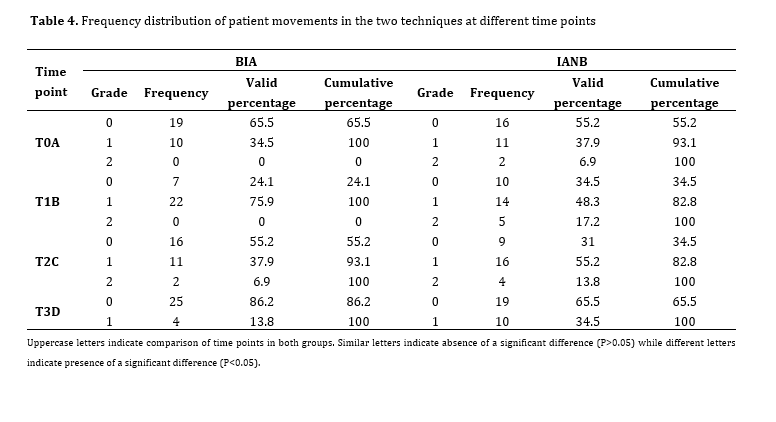
Patient movements: Table 4 shows the frequency distribution of patient movements in the two techniques at different time points. The results of GEE showed that the interaction effect of time and technique of anesthesia on patient movements was not significant (P=0.354). Thus, the results were analyzed irrespective of the interaction effect.
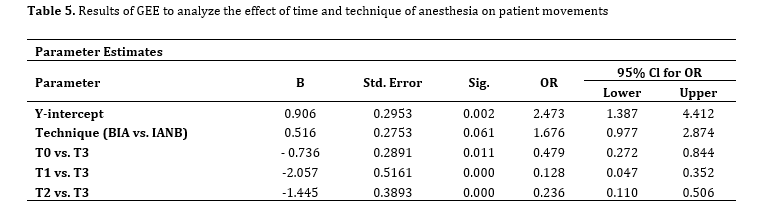
The results (Table 5) indicated that although the odds of calmness of children in the BIA group were 1.7 times higher than in the IANB group, this difference was not significant (P=0.061). Also, the odds of calmness of children at T0 were lower than those at T3 (OR=0.48, P=0.011), indicating that children were calmer at T3 compared with T0, and their odds of calmness at T3 were twice the rate at T0. Also, the odds of calmness of children at T1 were significantly lower than those at T3 (OR=0.13, P<0.001) indicating that children at T3 were calmer than T1, and their odds for calmness at T3 were 7.7 times the rate at T1. Calmness of children at T2 was significantly lower than that at T3 (OR=0.24, P<0.001), indicating that children at T3 were calmer than T2, and their odds for calmness at T3 were 4 times higher than those at T2.
Comparison of the mean HR at different time points in the IANB group showed a significant difference (P<0.001). The HR at T0 was significantly lower than that at T1 and T2 (P<0.05) but the difference between T0 and T3 was not significant (P>0.05). The HR at T1 was significantly lower than that at T2 (P<0.05). The HR at T1 was significantly higher than that at T3 (P<0.05). The difference in HR between T2 and T3 was also significant (P<0.05).
SPO2: Table 3 presents the mean SPO2 of children in the two anesthesia techniques at the four assessment time points. Two-way repeated measures ANOVA showed the significant effect of anesthesia technique on the SPO2 (P<0.001) such that the mean SPO2 was higher in the BIA technique compared with IANB (P<0.001). The effect of time on the SPO2 was also significant such that its trend of change was variable over time (P<0.001). The interaction effect of time and technique of anesthesia on the SPO2 was also significant (P=0.003). Thus, paired t-test was applied to compare the SPO2 between the two techniques at each time point, which showed that the difference between the two techniques was not significant at T0 (P=0.931) or T3 (P=0.117). However, the mean SPO2 was significantly lower in the IANB group than the BIA group at T1 (P=0.025) and T2 (P<0.001).
One-way repeated measures ANOVA showed that the change in SPO2 was not significant in BIA group over time (P=0.489). However, its trend of change was significant in the IANB group (P<0.001). Comparison of the SPO2 in the IANB group at different time points by the Bonferroni test showed no significant difference between T0 and T1 (P=0.089), or T0 and T3 (P=1.000). However, the mean SPO2 at T0 was significantly higher than that at T2 (P=0.001). The difference between T1 and T2 (P=0.267), or T1 and T3 (P=0.335) was not significant, but the mean SPO2 at T2 was significantly lower than that at T3 (P=0.008).
Patient movements: Table 4 shows the frequency distribution of patient movements in the two techniques at different time points. The results of GEE showed that the interaction effect of time and technique of anesthesia on patient movements was not significant (P=0.354). Thus, the results were analyzed irrespective of the interaction effect.
The results (Table 5) indicated that although the odds of calmness of children in the BIA group were 1.7 times higher than in the IANB group, this difference was not significant (P=0.061). Also, the odds of calmness of children at T0 were lower than those at T3 (OR=0.48, P=0.011), indicating that children were calmer at T3 compared with T0, and their odds of calmness at T3 were twice the rate at T0. Also, the odds of calmness of children at T1 were significantly lower than those at T3 (OR=0.13, P<0.001) indicating that children at T3 were calmer than T1, and their odds for calmness at T3 were 7.7 times the rate at T1. Calmness of children at T2 was significantly lower than that at T3 (OR=0.24, P<0.001), indicating that children at T3 were calmer than T2, and their odds for calmness at T3 were 4 times higher than those at T2.
Table 2. HR of children in the two anesthesia techniques at the four assessment time points (n=29)
Table 3. Mean SPO2 of children in the two anesthesia techniques at the four assessment time points (n=29)
Table 4. Frequency distribution of patient movements in the two techniques at different time points
Table 5. Results of GEE to analyze the effect of time and technique of anesthesia on patient movements
Discussion
This study compared the efficacy of BIA with articaine versus IANB with lidocaine for pulpotomy of primary mandibular second molars under IV sedation. The null hypothesis of the study was that the efficacy of BIA with articaine would not be significantly different from that of IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation.
Evidence shows that the HR of 3-6-year-old children is 80-120 pulses/minute, which can increase by 20% due to pain, stress, or physical activity. This increase in HR is normal and does not require any intervention [5]. The present results showed an increase in HR in both techniques; however, this increase was significantly greater in the IANB group at T1 (during anesthetic injection), T2 (during pulp exposure), and T3 (recovery). Thus, the null hypothesis of the study was rejected in this regard. The greater increase in HR in the IANB group at T1 can be due to the painful nature of the IANB [15]. Better diffusion, higher potency, and faster onset of effect of articaine might have been responsible for lower HR at T2 and T3 in the BIA group (due to lower pain). Lower HR at T2 and T3 in the BIA group can also be due to the fact that articaine has the shortest metabolic half-life (estimated to be 27 to 42 minutes); whereas, the elimination half-life of most amide local anesthetic agents, such as lidocaine, is 90 minutes [18]. Lip numbness in infiltration anesthesia in children is due to the deposition of local anesthetic agent in the buccal vestibule, since it is not very far from the mental foramen. Thus, diffusion of the anesthetic agent towards the mental foramen produces lip numbness. However, the soft tissue anesthesia in using articaine is shorter (2.25 hours) [19] in comparison with lidocaine (3-5 hours) [20]. Considering the short half-life of sedatives, it is imperative to start the treatment as soon as possible after the injection of sedative, which justifies the use of BIA with articaine.
In the present study, the SPO2 was significantly higher in the BIA group at T1 and T2 than the IANB group, which indicates lower pain during anesthetic injection and pulp exposure in the BIA group and higher pain of IANB injection (T1) and slower onset of effect of IANB (T2). Pain affects the physiological parameters. It not only increases the HR, but also causes respiratory depression, and resultantly lowers the blood oxygen saturation rate [21, 22]. Thus, this part of the null hypothesis was rejected as well. Similarly, Daneswari et al. [17], Almadhoon et al. [23], Ghaffari et al. [24], Elchaghaby et al. [25] and Bahrololoomi and Rezaei [26] reported higher analgesic efficacy of BIA with articaine than IANB with lidocaine. However, Daneshvar et al. [13] reported higher success rate of IANB with lidocaine than BIA with articaine, which was in contrast to the present findings. Also, time to onset was shorter in the present study since the children were sedated and the procedure had to be started and finished promptly. In contrast to the present results, Sharifi et al. [27] showed the superiority of IANB to BIA; however, they reported higher success rate of BIA in 4 to 6.5-year-olds due to the lower thickness of the cortical bone, which was similar to the present finding.
The results of behavioral assessment of children by NVPS-R in the present study showed that the odds of calmness of children during the entire procedure were 1.7 times higher in BIA than IANB but the difference was not significant. Thus, the null hypothesis was accepted in this regard. In general, maximum calmness was recorded during the recovery period at T3 since there is no painful stimulus such as anesthetic injection or pulpal exposure, or discomfort due to the placement of a mouth opener. Higher level of calmness at T3 compared to T0 may be explained by placement of the child on the dental unit and his agitation in this process at T0. The highest patient movements were recorded at T1 (during anesthetic injection) and the lowest at T3 (recovery) in both techniques.
This study had some limitations. Since two treatment sessions were required, one patient did not show-up for the second session and was excluded. Also, some parents did not adhere to the recommendations regarding NPO, which resulted in cancellation of some treatments and prolongation of the study course.
Conclusion
BIA with articaine had optimal efficacy comparable to that of IANB with lidocaine for pulpotomy of primary second molars under sedation, and caused smaller changes in hemodynamic parameters than IANB with lidocaine.
{kind=link}
Table 3. Mean SPO2 of children in the two anesthesia techniques at the four assessment time points (n=29)
{kind=link}
Table 4. Frequency distribution of patient movements in the two techniques at different time points
{kind=link}
Table 5. Results of GEE to analyze the effect of time and technique of anesthesia on patient movements
{kind=link}
Discussion
This study compared the efficacy of BIA with articaine versus IANB with lidocaine for pulpotomy of primary mandibular second molars under IV sedation. The null hypothesis of the study was that the efficacy of BIA with articaine would not be significantly different from that of IANB with lidocaine in pulpotomy of primary mandibular second molars under sedation.
Evidence shows that the HR of 3-6-year-old children is 80-120 pulses/minute, which can increase by 20% due to pain, stress, or physical activity. This increase in HR is normal and does not require any intervention [5]. The present results showed an increase in HR in both techniques; however, this increase was significantly greater in the IANB group at T1 (during anesthetic injection), T2 (during pulp exposure), and T3 (recovery). Thus, the null hypothesis of the study was rejected in this regard. The greater increase in HR in the IANB group at T1 can be due to the painful nature of the IANB [15]. Better diffusion, higher potency, and faster onset of effect of articaine might have been responsible for lower HR at T2 and T3 in the BIA group (due to lower pain). Lower HR at T2 and T3 in the BIA group can also be due to the fact that articaine has the shortest metabolic half-life (estimated to be 27 to 42 minutes); whereas, the elimination half-life of most amide local anesthetic agents, such as lidocaine, is 90 minutes [18]. Lip numbness in infiltration anesthesia in children is due to the deposition of local anesthetic agent in the buccal vestibule, since it is not very far from the mental foramen. Thus, diffusion of the anesthetic agent towards the mental foramen produces lip numbness. However, the soft tissue anesthesia in using articaine is shorter (2.25 hours) [19] in comparison with lidocaine (3-5 hours) [20]. Considering the short half-life of sedatives, it is imperative to start the treatment as soon as possible after the injection of sedative, which justifies the use of BIA with articaine.
In the present study, the SPO2 was significantly higher in the BIA group at T1 and T2 than the IANB group, which indicates lower pain during anesthetic injection and pulp exposure in the BIA group and higher pain of IANB injection (T1) and slower onset of effect of IANB (T2). Pain affects the physiological parameters. It not only increases the HR, but also causes respiratory depression, and resultantly lowers the blood oxygen saturation rate [21, 22]. Thus, this part of the null hypothesis was rejected as well. Similarly, Daneswari et al. [17], Almadhoon et al. [23], Ghaffari et al. [24], Elchaghaby et al. [25] and Bahrololoomi and Rezaei [26] reported higher analgesic efficacy of BIA with articaine than IANB with lidocaine. However, Daneshvar et al. [13] reported higher success rate of IANB with lidocaine than BIA with articaine, which was in contrast to the present findings. Also, time to onset was shorter in the present study since the children were sedated and the procedure had to be started and finished promptly. In contrast to the present results, Sharifi et al. [27] showed the superiority of IANB to BIA; however, they reported higher success rate of BIA in 4 to 6.5-year-olds due to the lower thickness of the cortical bone, which was similar to the present finding.
The results of behavioral assessment of children by NVPS-R in the present study showed that the odds of calmness of children during the entire procedure were 1.7 times higher in BIA than IANB but the difference was not significant. Thus, the null hypothesis was accepted in this regard. In general, maximum calmness was recorded during the recovery period at T3 since there is no painful stimulus such as anesthetic injection or pulpal exposure, or discomfort due to the placement of a mouth opener. Higher level of calmness at T3 compared to T0 may be explained by placement of the child on the dental unit and his agitation in this process at T0. The highest patient movements were recorded at T1 (during anesthetic injection) and the lowest at T3 (recovery) in both techniques.
This study had some limitations. Since two treatment sessions were required, one patient did not show-up for the second session and was excluded. Also, some parents did not adhere to the recommendations regarding NPO, which resulted in cancellation of some treatments and prolongation of the study course.
Conclusion
BIA with articaine had optimal efficacy comparable to that of IANB with lidocaine for pulpotomy of primary second molars under sedation, and caused smaller changes in hemodynamic parameters than IANB with lidocaine.
Type of Study: Randomized Clinical Trial |
Subject:
pediatric
References
1. Dahlander A, Soares F, Grindefjord M, Dahllöf G. Factors Associated with Dental Fear and Anxiety in Children Aged 7 to 9 Years. Dent J (Basel). 2019 Jul 1;7(3):68. [DOI:10.3390/dj7030068] [PMID] []
2. Pande P, Rana V, Srivastava N, Kaushik N. Effectiveness of different behavior guidance techniques in managing children with negative behavior in a dental setting: A randomized control study. J Indian Soc Pedod Prev Dent. 2020 Jul-Sep;38(3):259-65. [DOI:10.4103/JISPPD.JISPPD_342_20] [PMID]
3. Vasakova J, Duskova J, Lunackova J, Drapalova K, Zuzankova L, Starka L, Duskova M, Broukal Z. Midazolam and its effect on vital signs and behavior in children under conscious sedation in dentistry. Physiol Res. 2020 Sep 30;69(Suppl 2):S305-S314. [DOI:10.33549/physiolres.934511] [PMID] []
4. Ibrahim H, Nelson T, Thikkurissy S, Xu Z, Scott J. Comparison of Procedures, Time and Fees Associated with Procedural Sedation and General Anesthesia in a Pediatric Dentistry Residency Program. J Dent Child (Chic). 2022 May 15;89(2):104-9.
5. Gropper MA, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Cohen NH, Leslie K. Miller's Anesthesia. Elsevier Health Sciences; 2019.
6. Forte G, Troisi G, Pazzaglia M, Pascalis V, Casagrande M. Heart Rate Variability and Pain: A Systematic Review. Brain Sci. 2022 Jan 24;12(2):153. [DOI:10.3390/brainsci12020153] [PMID] []
7. SF M. Sedation-E-Book: A guide to patient management. Elsevier Health Sciences; 2017. p. Chapter 3:14-21.
8. Dean JA. McDonald and Avery's Dentistry for the Child and Adolescent: McDonald and Avery's Dentistry for the Child and Adolescent-E-Book, Elsevier Health Sciences 2021.
9. Bahar E, Yoon H. Lidocaine: A Local Anesthetic, Its Adverse Effects and Management. Medicina (Kaunas). 2021 Jul 30;57(8):782. [DOI:10.3390/medicina57080782] [PMID] []
10. Samdrup T, Kijsamanmith K, Vongsavan K, Rirattanapong P, Vongsavan N. The effect of inferior alveolar nerve block anesthesia of 4% articaine and epinephrine 1:100,000 on blood flow and anesthesia of human mandibular teeth. J Dent Sci. 2021 Jan;16(1):249-55. [DOI:10.1016/j.jds.2020.05.013] [PMID] []
11. Martin E, Nimmo A, Lee A, Jennings E. Articaine in dentistry: an overview of the evidence and meta-analysis of the latest randomised controlled trials on articaine safety and efficacy compared to lidocaine for routine dental treatment. BDJ Open. 2021 Jul 17;7(1):27. [DOI:10.1038/s41405-021-00085-2] [PMID] []
12. Malamed SF. Handbook of local anesthesia. 7th: South Asia Edition-E-Book ed, Elsevier India 2019.
13. Daneshvar SH, Dorani D, Daneshvar MM. Comparison of anaesthetic efficacy of 4% articaine buccal infiltration versus 2% lidocaine inferior alveolar nerve block for pulpotomy in mandibular primary second molars. J Indian Soc Pedod Prev Dent. 2021 Jul-Sep;39(3):299-302. [DOI:10.4103/jisppd.jisppd_21_21] [PMID]
14. Frankl S, Shiere F, Fogels H. Should the parent remain with the child in the dental operatory? J Dent Child. 1962;29:150-63.
15. Chopra R, Marwaha M, Bansal K, Mittal M. Evaluation of Buccal Infiltration with Articaine and Inferior Alveolar Nerve Block with Lignocaine for Pulp Therapy in Mandibular Primary Molars. J Clin Pediatr Dent. 2016;40(4):301-5. [DOI:10.17796/1053-4628-40.4.301] [PMID]
16. Pereira-Morales S, Arroyo-Novoa CM, Wysocki A, Sanzero Eller L. Acute Pain Assessment in Sedated Patients in the Postanesthesia Care Unit. Clin J Pain. 2018 Aug;34(8):700-6. [DOI:10.1097/AJP.0000000000000593] [PMID] []
17. Daneswari V, Venugopal Reddy N, Madhavi G, Pranathi P. Assessing the Pain Reaction of Children and Evaluation of Efficacy of Buccal Infiltration with Articaine and Inferior Alveolar Nerve Block with Lignocaine for Pulp Therapy in Primary Mandibular Second Molars. Int J Clin Pediatr Dent. 2021 May-Jun;14(3):335-9. [DOI:10.5005/jp-journals-10005-1976] [PMID] []
18. Zhang A, Tang H, Liu S, Ma C, Ma S, Zhao H. Anesthetic Efficiency of Articaine Versus Lidocaine in the Extraction of Lower Third Molars: A Meta-Analysis and Systematic Review. J Oral Maxillofac Surg. 2019 Jan;77(1):18-28. [DOI:10.1016/j.joms.2018.08.020] [PMID]
19. Kung J, McDonagh M, Sedgley CM. Does Articaine Provide an Advantage over Lidocaine in Patients with Symptomatic Irreversible Pulpitis? A Systematic Review and Meta-analysis. J Endod. 2015 Nov;41(11):1784-94. [DOI:10.1016/j.joen.2015.07.001] [PMID]
20. Nair M, Jeevanandan G, Mohan M. Comparing the efficiency of 2% lidocaine and 4% articaine as a local anesthetic agent in children. Asian J Pharm Clin Res. 2018;11(5):295-8. [DOI:10.22159/ajpcr.2018.v11i5.24440]
21. de Jesus JA, Tristao RM, Storm H, da Rocha AF, Campos D Jr. Heart rate, oxygen saturation, and skin conductance: a comparison study of acute pain in Brazilian newborns. Annu Int Conf IEEE Eng Med Biol Soc. 2011;2011:1875-9. [DOI:10.1109/IEMBS.2011.6090532] [PMID]
22. Cashman JN, Dolin SJ. Respiratory and haemodynamic effects of acute postoperative pain management: evidence from published data. Br J Anaesth. 2004 Aug;93(2):212-23. [DOI:10.1093/bja/aeh180] [PMID]
23. Almadhoon HW, Abuiriban RW, Almassri H, Al-Hamed FS. Efficacy of 4% articaine buccal infiltration versus inferior alveolar nerve block for mandibular molars with symptomatic irreversible pulpitis: a systematic review and meta-analysis. J Evid Based Dent Pract. 2022 Jun;22(2):101712. [DOI:10.1016/j.jebdp.2022.101712] [PMID]
24. Ghaffari E, Roozbahani NA, Ghasemi D, Baninajarian H. A comparison between articaine mandibular infiltration and lidocaine mandibular block anesthesia in second primary molar: A randomized clinical trial. Dent Res J (Isfahan). 2022 Dec 14;19:103. [DOI:10.4103/1735-3327.363533] [PMID] []
25. Elchaghaby MA, Aly MM, Yousry YM. Effectiveness of buccal infiltration anaesthesia compared to inferior alveolar nerve block anaesthesia in primary mandibular molar extractions: a randomised controlled study. Br Dent J. 2023 Jul 20. [DOI:10.1038/s41415-023-6063-7] [PMID]
26. Bahrololoomi Z, Rezaei M. Anesthetic efficacy of single buccal infiltration of 4% articaine compared to routine inferior alveolar nerve block with 2% lidocaine during bilateral extraction of mandibular primary molars: a randomized controlled trial. J Dent Anesth Pain Med. 2021 Feb;21(1):61-9. [DOI:10.17245/jdapm.2021.21.1.61] [PMID] []
27. Sharifi M, Karimaghaee A, Iranmanesh F, Sheikhfathalahi M. Comparison of the anesthetic efficacy of articaine infiltration versus lidocaine inferior alveolar nerve block in pulp therapy of lower primary molars. Journal of Mashhad Dental School, 2017; 41(4): 305-16.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |