Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 2 (6-2024)
J Res Dent Maxillofac Sci 2024, 9(2): 80-85 |
Back to browse issues page


Ethics code: IR.SBMU.DRC.REC.1398.162
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tabrizi R, Safavi M, MalekiGorji M, Torabzadeh M. Does Keratinized Mucosa Width Affect Marginal Bone Loss Around Dental Implants in Over Dentures? A Longitudinal Study. J Res Dent Maxillofac Sci 2024; 9 (2) :80-85
URL: http://jrdms.dentaliau.ac.ir/article-1-548-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-548-en.html



1- Oral and Maxillofacial Surgery Department, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Private Dentistry Practice, Tehran, Iran.
3- Oral and Maxillofacial Surgery Department, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,mohsen_malekigorji@yahoo.com
4- Department of Periodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Private Dentistry Practice, Tehran, Iran.
3- Oral and Maxillofacial Surgery Department, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
4- Department of Periodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 252 kb]
(867 Downloads)
| Abstract (HTML) (3271 Views)
Full-Text: (1123 Views)
Abstract
Background and Aim: Keratinized mucosa width (KMW) has an essential role in peri-implant health. This study aimed to evaluate the impact of KMW on marginal bone loss (MBL) around overdenture-supported dental implants.
Materials and Methods: In this cohort study, completely edentulous patients received an overdenture with implants in the maxilla and mandible. Two implants were placed in the maxilla and mandible. Ball attachments were used. KMW was measured, and gingival biotype was determined. MBL was evaluated on digital parallel radiographs taken at 12 and 24 months after loading. KMW was the predictive factor, and MBL was the outcome of the study. Data were analyzed using SPSS 21 via Pearson’s correlation test, independent t-test, and Chi-square test (alpha=0.05).
Results: Eighty implants in 20 patients were studied. The mean KMW was 2.05±0.88 mm. The mean MBL was 1.32±0.46 mm at 12 months after loading, and 1.71±0.49 mm at 24 months after loading. Analysis of the data demonstrated a correlation between MBL at 12 and 24 months after loading with KMW and dental implant diameter (P<0.001).
Conclusion: It appears that narrow KMW may be associated with an increase in MBL in two-implant-supported overdentures. Gingival biotype may play a role in the detrimental effect of narrow keratinized mucosa on MBL.
Keywords: Alveolar Bone Loss; Dental Implants; Gingiva; Mouth Mucosa
Introduction
Marginal bone loss (MBL) is an important criterion for assessment of the success of dental implants in the long-term [1]. The characteristics of the periodontium play an essential role in peri-implant soft tissue health [2]. Adequate keratinized mucosa including the free and attached gingiva may decrease the incidence of peri-implant inflammation. Dental biofilm may easily penetrate into the mobile mucosa around dental implants and induce the inflammatory mediators by activating neutrophils and lymphocytes [2]. It has been shown that insufficient keratinized mucosa width (KMW) leads to an increase in plaque accumulation and inflammation, which can cause subsequent gingival recession [3, 4].
Overdentures are generally used in edentulous patients with considerable bone resorption. Overdentures increase the satisfaction level and quality of life of edentulous patients [5]. Resorption of alveolar ridge following tooth loss causes keratinized mucosa loss due to a reduction in distance between the mucogingival line and the bone crest [6]. It appears that MBL is not different around dental implants supporting fixed or removable prostheses [7]. Many overdenture patients have insufficient KMW. Therefore, evaluating the possible effect of KMW on MBL may guide the clinicians to consider a technique to increase KMW for implant-supported overdentures. Several studies have assessed the impact of KMW on MBL in implant-supported fixed partial dentures [8-10]. However, studies focusing on KMW in overdentures are limited [11].
This study was designed to answer the following question: does KMW affect MBL around dental implants in edentulous patients with overdentures? The authors hypothesized that reduced KMW would be associated with an increase in MBL. Thus, this study aimed to assess the effect of KMW on MBL in overdenture patients.
Materials and Methods
Study design/sample:
The authors designed a longitudinal study. The participants were derived from the population of patients presenting to the Oral and Maxillofacial Surgery Department of Shahid Beheshti University of Medical Sciences and a private clinic between September 1, 2017 and October 31, 2020. The study protocol was approved by the medical ethics committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.DRC.REC.1398.162). Patients eligible for study inclusion were completely edentulous and received an overdenture with dental implants in the maxilla and mandible. The patients were excluded from the study enrollment if they were smokers, had fresh socket implant placement, had systemic diseases affecting bone metabolism, underwent soft and hard tissue augmentation, failed to show up for the follow-up, or refused study enrollment.
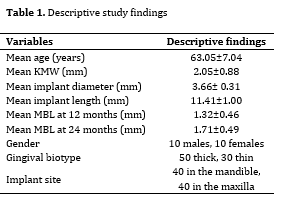
Age, gender, diameter and length of implant, implant site (maxilla or mandible), and gingival biotype (thick or thin) were the variables of the study. KMW was the predictive factor, and MBL was considered as the outcome of the study (Table 1).
Table 1. Descriptive study findings
Background and Aim: Keratinized mucosa width (KMW) has an essential role in peri-implant health. This study aimed to evaluate the impact of KMW on marginal bone loss (MBL) around overdenture-supported dental implants.
Materials and Methods: In this cohort study, completely edentulous patients received an overdenture with implants in the maxilla and mandible. Two implants were placed in the maxilla and mandible. Ball attachments were used. KMW was measured, and gingival biotype was determined. MBL was evaluated on digital parallel radiographs taken at 12 and 24 months after loading. KMW was the predictive factor, and MBL was the outcome of the study. Data were analyzed using SPSS 21 via Pearson’s correlation test, independent t-test, and Chi-square test (alpha=0.05).
Results: Eighty implants in 20 patients were studied. The mean KMW was 2.05±0.88 mm. The mean MBL was 1.32±0.46 mm at 12 months after loading, and 1.71±0.49 mm at 24 months after loading. Analysis of the data demonstrated a correlation between MBL at 12 and 24 months after loading with KMW and dental implant diameter (P<0.001).
Conclusion: It appears that narrow KMW may be associated with an increase in MBL in two-implant-supported overdentures. Gingival biotype may play a role in the detrimental effect of narrow keratinized mucosa on MBL.
Keywords: Alveolar Bone Loss; Dental Implants; Gingiva; Mouth Mucosa
Introduction
Marginal bone loss (MBL) is an important criterion for assessment of the success of dental implants in the long-term [1]. The characteristics of the periodontium play an essential role in peri-implant soft tissue health [2]. Adequate keratinized mucosa including the free and attached gingiva may decrease the incidence of peri-implant inflammation. Dental biofilm may easily penetrate into the mobile mucosa around dental implants and induce the inflammatory mediators by activating neutrophils and lymphocytes [2]. It has been shown that insufficient keratinized mucosa width (KMW) leads to an increase in plaque accumulation and inflammation, which can cause subsequent gingival recession [3, 4].
Overdentures are generally used in edentulous patients with considerable bone resorption. Overdentures increase the satisfaction level and quality of life of edentulous patients [5]. Resorption of alveolar ridge following tooth loss causes keratinized mucosa loss due to a reduction in distance between the mucogingival line and the bone crest [6]. It appears that MBL is not different around dental implants supporting fixed or removable prostheses [7]. Many overdenture patients have insufficient KMW. Therefore, evaluating the possible effect of KMW on MBL may guide the clinicians to consider a technique to increase KMW for implant-supported overdentures. Several studies have assessed the impact of KMW on MBL in implant-supported fixed partial dentures [8-10]. However, studies focusing on KMW in overdentures are limited [11].
This study was designed to answer the following question: does KMW affect MBL around dental implants in edentulous patients with overdentures? The authors hypothesized that reduced KMW would be associated with an increase in MBL. Thus, this study aimed to assess the effect of KMW on MBL in overdenture patients.
Materials and Methods
Study design/sample:
The authors designed a longitudinal study. The participants were derived from the population of patients presenting to the Oral and Maxillofacial Surgery Department of Shahid Beheshti University of Medical Sciences and a private clinic between September 1, 2017 and October 31, 2020. The study protocol was approved by the medical ethics committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.DRC.REC.1398.162). Patients eligible for study inclusion were completely edentulous and received an overdenture with dental implants in the maxilla and mandible. The patients were excluded from the study enrollment if they were smokers, had fresh socket implant placement, had systemic diseases affecting bone metabolism, underwent soft and hard tissue augmentation, failed to show up for the follow-up, or refused study enrollment.
Age, gender, diameter and length of implant, implant site (maxilla or mandible), and gingival biotype (thick or thin) were the variables of the study. KMW was the predictive factor, and MBL was considered as the outcome of the study (Table 1).
Table 1. Descriptive study findings
{kind=link}
Data collection methods:
Ball attachments were used in all patients. The patients had a mean age of 63.05±7.04 years. Dental implant (Megagen Anyone Line, South Korea) was placed for all patients. The fixture size was the same in all cases (4 mm diameter, and 10 mm length). The maxillary and mandibular overdentures were fabricated 3 months after implant placement. The one-stage surgical protocol was adopted for all cases.
KMW was measured by a periodontal probe (Williams PW, Hu-Friedy, Chicago, IL, USA) with 1, 2, 3, 5, 7, and 10-mm calibrations. The KMW was defined as the distance between the mucogingival junction and the peri-implant mucosal margin [3]. The border between the keratinized and alveolar mucosa was identified by examining the mucosal surface characteristics. For confirmation, a periodontal probe was used to retract the mucosa parallel to the border to identify the mucogingival junction.
Gingival biotype w:as char:acterized as thin or thick according to the transparency of a double-ended periodontal probe (Ø 0.5 and 0.75 mm; DBS12 prototype, Deppeler SA, Rolle, Switzerland). The periodontal probe has two unequal thick endings. Transparency was assessed through the gingival margin by probing the sulcus at the mid-buccal aspect of dental implants. If the thick ending of the probe was not seen through the tissue, the gingival biotype was considered to be thick [12].
Digital parallel radiographs (Dexcowin, iRay D3, South Korea) were obtained immediately after loading, and also after 12 and 24 months with 60 kV tube potential and 7 mA tube current in 0.20 s time. The MBL was measured at the mesial and distal aspects of dental implants by comparing the bone level on digital parallel radiographs taken immediately after loading and after 12 and 24 months. When the MBL was different at the mesial and distal aspects of dental implants, the mean MBL was calculated and reported. The bone level was measured from the alveolar crest to the implant collar [3].
Sample size calculation:
The sample size was calculated using the formula N = (Z α/2)2 s2 / d2; where Zα is considered to be 1.96 with 5% level of significance, assuming a mean difference in MBL equal to 0.3 mm (d) to be significant with a standard deviation of 1.3 mm according to a previous study [13]. Thus, the sample size was calculated to be 72 dental implants assuming a confidence interval of 95% and a study power of 90%.
To minimize the study bias, an independent dentist who did not participate in surgical or prosthodontic treatments measured the KMW. Furthermore, two examiners assessed the MBL on digital radiographs.
Statistical analysis:
The statistical analyses were performed using SPSS version 21 (SPSS Inc., IL, USA). The Pearson’s correlation test was used to find any correlation between KMW and MBL. Independent t-test was applied to compare KMW and MBL between males and females. The Chi-square test was used to compare the number of males and females and implant site (maxilla and mandible). A general linear model was used to predict possible MBL based on KMW. P values < 0.05 were considered statistically significant. The Kappa test was conducted to analyze the inter-examiner agreement.
Results
Eighty implants in 20 patients were studied. The mean age of the patients was 63.05±7.04 years. The mean KMW was 2.05±0.88 mm (range 0 mm to 4 mm). None of the implants failed during the follow-up time. The mean MBL was not significantly different between males and females at 12 and 24 months after loading (P=0.63 and P=0.49, respectively) (Table 2). The results did not demonstrate any difference in the mean MBL in the maxilla and mandible at 12 and 24 months following loading (P=0.25 and P=0.12, respectively) (Table 3).
The mean MBL was 1.07±0.33 mm in cases with thick gingival biotype and 1.72±0.36 mm in cases with thin gingival biotype at 12 months after loading. There was a significant difference in the mean MBL between the thick and thin gingival biotypes (P<0.001). At 24 months after implant loading, the mean MBL was 1.48±0.38 mm in the thick gingival biotype group, and 2.07±0.41 in the thin gingival biotype group. A significant difference was detected in the mean MBL between the thick and thin gingival biotypes at 24 months after loading (P<0.001, Table 4).
Analysis of the data demonstrated a correlation between MBL at 12 and 24 months after loading with KMW and implant diameter (P<0.001). Other variables did not have any correlation with MBL (Tables 5 and 6).
The general linear model demonstrated that MBL could be predicted based on KMW in 59.4% of implants with a thin gingival biotype 24 months after loading. Per each one-unit decrease in KMW, MBL is expected to increase by 0.48 mm. By a one-standard-deviation decrease in KMW, the MBL is expected to increase by 0.771 of standard deviation (P<0.001, R2=0.594, β=0.771).
Ball attachments were used in all patients. The patients had a mean age of 63.05±7.04 years. Dental implant (Megagen Anyone Line, South Korea) was placed for all patients. The fixture size was the same in all cases (4 mm diameter, and 10 mm length). The maxillary and mandibular overdentures were fabricated 3 months after implant placement. The one-stage surgical protocol was adopted for all cases.
KMW was measured by a periodontal probe (Williams PW, Hu-Friedy, Chicago, IL, USA) with 1, 2, 3, 5, 7, and 10-mm calibrations. The KMW was defined as the distance between the mucogingival junction and the peri-implant mucosal margin [3]. The border between the keratinized and alveolar mucosa was identified by examining the mucosal surface characteristics. For confirmation, a periodontal probe was used to retract the mucosa parallel to the border to identify the mucogingival junction.
Gingival biotype w:as char:acterized as thin or thick according to the transparency of a double-ended periodontal probe (Ø 0.5 and 0.75 mm; DBS12 prototype, Deppeler SA, Rolle, Switzerland). The periodontal probe has two unequal thick endings. Transparency was assessed through the gingival margin by probing the sulcus at the mid-buccal aspect of dental implants. If the thick ending of the probe was not seen through the tissue, the gingival biotype was considered to be thick [12].
Digital parallel radiographs (Dexcowin, iRay D3, South Korea) were obtained immediately after loading, and also after 12 and 24 months with 60 kV tube potential and 7 mA tube current in 0.20 s time. The MBL was measured at the mesial and distal aspects of dental implants by comparing the bone level on digital parallel radiographs taken immediately after loading and after 12 and 24 months. When the MBL was different at the mesial and distal aspects of dental implants, the mean MBL was calculated and reported. The bone level was measured from the alveolar crest to the implant collar [3].
Sample size calculation:
The sample size was calculated using the formula N = (Z α/2)2 s2 / d2; where Zα is considered to be 1.96 with 5% level of significance, assuming a mean difference in MBL equal to 0.3 mm (d) to be significant with a standard deviation of 1.3 mm according to a previous study [13]. Thus, the sample size was calculated to be 72 dental implants assuming a confidence interval of 95% and a study power of 90%.
To minimize the study bias, an independent dentist who did not participate in surgical or prosthodontic treatments measured the KMW. Furthermore, two examiners assessed the MBL on digital radiographs.
Statistical analysis:
The statistical analyses were performed using SPSS version 21 (SPSS Inc., IL, USA). The Pearson’s correlation test was used to find any correlation between KMW and MBL. Independent t-test was applied to compare KMW and MBL between males and females. The Chi-square test was used to compare the number of males and females and implant site (maxilla and mandible). A general linear model was used to predict possible MBL based on KMW. P values < 0.05 were considered statistically significant. The Kappa test was conducted to analyze the inter-examiner agreement.
Results
Eighty implants in 20 patients were studied. The mean age of the patients was 63.05±7.04 years. The mean KMW was 2.05±0.88 mm (range 0 mm to 4 mm). None of the implants failed during the follow-up time. The mean MBL was not significantly different between males and females at 12 and 24 months after loading (P=0.63 and P=0.49, respectively) (Table 2). The results did not demonstrate any difference in the mean MBL in the maxilla and mandible at 12 and 24 months following loading (P=0.25 and P=0.12, respectively) (Table 3).
The mean MBL was 1.07±0.33 mm in cases with thick gingival biotype and 1.72±0.36 mm in cases with thin gingival biotype at 12 months after loading. There was a significant difference in the mean MBL between the thick and thin gingival biotypes (P<0.001). At 24 months after implant loading, the mean MBL was 1.48±0.38 mm in the thick gingival biotype group, and 2.07±0.41 in the thin gingival biotype group. A significant difference was detected in the mean MBL between the thick and thin gingival biotypes at 24 months after loading (P<0.001, Table 4).
Analysis of the data demonstrated a correlation between MBL at 12 and 24 months after loading with KMW and implant diameter (P<0.001). Other variables did not have any correlation with MBL (Tables 5 and 6).
The general linear model demonstrated that MBL could be predicted based on KMW in 59.4% of implants with a thin gingival biotype 24 months after loading. Per each one-unit decrease in KMW, MBL is expected to increase by 0.48 mm. By a one-standard-deviation decrease in KMW, the MBL is expected to increase by 0.771 of standard deviation (P<0.001, R2=0.594, β=0.771).
Table 2. Comparison of MBL between males and females at 12 and 24 months after loading
Table 3. MBL in the maxilla and mandible at 12 and 24 months after loading
Table 4. Comparison of MBL between the thin and thick gingival biotypes
Table 5. Correlation between the variables and MBL at 12 months after loading
Table 6. Correlation between variables and MBL at 24 months after loading
In thick gingival biotype, MBL could be predicted based on KMW in 44.2% of implants with a thick gingival biotype 24 months after loading. For a one-unit decrease in KMW, MBL is expected to increase by 0.36 mm. Per one-standard-deviation decrease in KMW, MBL is expected to increase by 0.665 of standard deviation (P<0.001, R2=0.442, β=0.665).
The inter-examiner reliability was calculated to be Kappa=0.84 (P<0.001), which demonstrated substantial agreement between the examiners.
Discussion
Keratinized gingiva has been known to be important in preserving gingival health and preventing gingival recession. The keratinized tissue provides a biological protective barrier, which can increase the survival rate of dental implants [14]. In this study, the effect of KMW on MBL as an essential criterion for assessment of dental implant success was studied. It is believed that peri-implant MBL by more than 2 mm in the first year after loading is associated with poor clinical outcomes [1]. Therefore, one of the important roles of keratinized tissue around dental implants was investigated in the current study.
The present results showed a correlation between KMW and MBL at 12 and 24 months after loading. KMW and MBL had a stronger correlation in presence of thin gingival biotype compared with thick gingival biotype (R= 0.77 and R=0.66, respectively). Wennström and Derks [6] reported a significantly higher plaque score in cases with inadequate KMW (< 2 mm). Ravidà et al. [15] concluded that MBL influenced peri-implantitis at the time of treatment. KMW did not affect peri-implantitis. The impact of KMW on plaque index around dental implants has been well documented [16]. Subsequently, the risk of peri-implantitis in cases with insufficient KMW is higher than that in presence of sufficient KMW [17].
The present results revealed that in more than half of the patients with a thin gingival biotype, MBL could be predicted based on KMW. However, the etiology of MBL is multifactorial. It appears that local factors are more important than systemic factors in this regard [18]. Therefore, KMW is one of the main causative factors in the occurrence of MBL, particularly in cases with thin gingival biotype [19]. In the current study, MBL did not have any correlation with implant length. Implant type and attachment type were not found to be associated with any change in MBL in previous research [11, 20]. Adibrad et al. [21] demonstrated that the mean plaque index score, gingival index score, and bleeding on probing were significantly higher for cases with narrow (< 2 mm) KMW around dental implants supporting overdentures.
The different biomechanical loading of implants supporting fixed prostheses and overdentures suggests lower risk of MBL in use of overdentures. Saravi et al. [7] indicated that MBL and long-term outcomes were the same in patients with fixed implant-supported restorations and overdentures. Implant diameter was another adjunctive factor considered in the present study in addition to KMW. Telles et al., and Ma et al. assessed MBL in narrow single implants and reported comparable MBL in narrow and standard implants. Nonetheless, they believed that narrow implants might have a higher MBL than wide or standard implants [22, 23]. In contrast, MBL had an inverse correlation with implant diameter in the present study. One possible reason for the difference in the results may be the placement of wider implants in narrow atrophic ridges. Thus, thin buccal or lingual/palatal bone was responsible for the increase in MBL. The difference in biomechanics of fixed and removable implant-supported restorations may be another reason for the existing differences in the literature.
Several studies have demonstrated the important effect of KMW on MBL and gingival health around dental implants [24, 25]. Considering the multifactorial etiology of MBL, KMW could not be considered as a causative factor. However, KMW may be an adjunctive risk factor along with other risk factors. In the present study, the difference in MBL between the two gingival biotypes was small (0.59 mm) at 24 months, which may not be clinically important. However, an increase in MBL may occur in long-term follow-ups, which may have a clinical impact on the outcomes.
Conclusion
It appears that insufficient KMW may be associated with an increase in MBL in two-implant-supported overdentures. The gingival biotype may play a role in the detrimental effect of narrow keratinized gingiva on MBL.
{kind=link}
Table 3. MBL in the maxilla and mandible at 12 and 24 months after loading
{kind=link}
Table 4. Comparison of MBL between the thin and thick gingival biotypes
{kind=link}
Table 5. Correlation between the variables and MBL at 12 months after loading
{kind=link}
Table 6. Correlation between variables and MBL at 24 months after loading
{kind=link}
In thick gingival biotype, MBL could be predicted based on KMW in 44.2% of implants with a thick gingival biotype 24 months after loading. For a one-unit decrease in KMW, MBL is expected to increase by 0.36 mm. Per one-standard-deviation decrease in KMW, MBL is expected to increase by 0.665 of standard deviation (P<0.001, R2=0.442, β=0.665).
The inter-examiner reliability was calculated to be Kappa=0.84 (P<0.001), which demonstrated substantial agreement between the examiners.
Discussion
Keratinized gingiva has been known to be important in preserving gingival health and preventing gingival recession. The keratinized tissue provides a biological protective barrier, which can increase the survival rate of dental implants [14]. In this study, the effect of KMW on MBL as an essential criterion for assessment of dental implant success was studied. It is believed that peri-implant MBL by more than 2 mm in the first year after loading is associated with poor clinical outcomes [1]. Therefore, one of the important roles of keratinized tissue around dental implants was investigated in the current study.
The present results showed a correlation between KMW and MBL at 12 and 24 months after loading. KMW and MBL had a stronger correlation in presence of thin gingival biotype compared with thick gingival biotype (R= 0.77 and R=0.66, respectively). Wennström and Derks [6] reported a significantly higher plaque score in cases with inadequate KMW (< 2 mm). Ravidà et al. [15] concluded that MBL influenced peri-implantitis at the time of treatment. KMW did not affect peri-implantitis. The impact of KMW on plaque index around dental implants has been well documented [16]. Subsequently, the risk of peri-implantitis in cases with insufficient KMW is higher than that in presence of sufficient KMW [17].
The present results revealed that in more than half of the patients with a thin gingival biotype, MBL could be predicted based on KMW. However, the etiology of MBL is multifactorial. It appears that local factors are more important than systemic factors in this regard [18]. Therefore, KMW is one of the main causative factors in the occurrence of MBL, particularly in cases with thin gingival biotype [19]. In the current study, MBL did not have any correlation with implant length. Implant type and attachment type were not found to be associated with any change in MBL in previous research [11, 20]. Adibrad et al. [21] demonstrated that the mean plaque index score, gingival index score, and bleeding on probing were significantly higher for cases with narrow (< 2 mm) KMW around dental implants supporting overdentures.
The different biomechanical loading of implants supporting fixed prostheses and overdentures suggests lower risk of MBL in use of overdentures. Saravi et al. [7] indicated that MBL and long-term outcomes were the same in patients with fixed implant-supported restorations and overdentures. Implant diameter was another adjunctive factor considered in the present study in addition to KMW. Telles et al., and Ma et al. assessed MBL in narrow single implants and reported comparable MBL in narrow and standard implants. Nonetheless, they believed that narrow implants might have a higher MBL than wide or standard implants [22, 23]. In contrast, MBL had an inverse correlation with implant diameter in the present study. One possible reason for the difference in the results may be the placement of wider implants in narrow atrophic ridges. Thus, thin buccal or lingual/palatal bone was responsible for the increase in MBL. The difference in biomechanics of fixed and removable implant-supported restorations may be another reason for the existing differences in the literature.
Several studies have demonstrated the important effect of KMW on MBL and gingival health around dental implants [24, 25]. Considering the multifactorial etiology of MBL, KMW could not be considered as a causative factor. However, KMW may be an adjunctive risk factor along with other risk factors. In the present study, the difference in MBL between the two gingival biotypes was small (0.59 mm) at 24 months, which may not be clinically important. However, an increase in MBL may occur in long-term follow-ups, which may have a clinical impact on the outcomes.
Conclusion
It appears that insufficient KMW may be associated with an increase in MBL in two-implant-supported overdentures. The gingival biotype may play a role in the detrimental effect of narrow keratinized gingiva on MBL.
Type of Study: Original article |
Subject:
Dental implant
References
1. Galindo-Moreno P, Catena A, Pérez-Sayáns M, Fernández-Barbero JE, O'Valle F, Padial-Molina M. Early marginal bone loss around dental implants to define success in implant dentistry: A retrospective study. Clin Implant Dent Relat Res. 2022 Oct;24(5):630-42. [DOI:10.1111/cid.13122] [PMID] []
2. Monje A, Blasi G. Significance of keratinized mucosa/gingiva on peri-implant and adjacent periodontal conditions in erratic maintenance compliers. J Periodontol. 2019 May;90(5):445-53. [DOI:10.1002/JPER.18-0471] [PMID]
3. Grischke J, Karch A, Wenzlaff A, Foitzik MM, Stiesch M, Eberhard J. Keratinized mucosa width is associated with severity of peri-implant mucositis. A cross-sectional study. Clin Oral Implants Res. 2019 May;30(5):457-65. [DOI:10.1111/clr.13432] [PMID]
4. Stefanini M, Pispero A, Del Fabbro M, Gobbato L, Ghensi P, Lodi G, et al. The Effect of Keratinized Mucosa on Peri-Implant Health and Patient-Reported Outcome Measures: A Systematic Review and Meta-Analysis. Applied Sciences. 2023; 13(15):8631 [DOI:10.3390/app13158631]
5. Kutkut A, Bertoli E, Frazer R, Pinto-Sinai G, Fuentealba Hidalgo R, Studts J. A systematic review of studies comparing conventional complete denture and implant retained overdenture. J Prosthodont Res. 2018 Jan;62(1):1-9. [DOI:10.1016/j.jpor.2017.06.004] [PMID]
6. Wennström JL, Derks J. Is there a need for keratinized mucosa around implants to maintain health and tissue stability? Clin Oral Implants Res. 2012 Oct;23 Suppl 6:136-46. [DOI:10.1111/j.1600-0501.2012.02540.x] [PMID]
7. Saravi BE, Putz M, Patzelt S, Alkalak A, Uelkuemen S, Boeker M. Marginal bone loss around oral implants supporting fixed versus removable prostheses: a systematic review. Int J Implant Dent. 2020 Jun 3;6(1):20. [DOI:10.1186/s40729-020-00217-7] [PMID] []
8. Afrashtehfar KI, Oh KC, Jurado CA, Lee H. Lack of keratinized mucosa increases peri-implantitis risk. Evid Based Dent. 2023 Sep;24(3):118-20. [DOI:10.1038/s41432-023-00913-4] [PMID] []
9. Stefanini M, Barootchi S, Sangiorgi M, Pispero A, Grusovin MG, Mancini L, Zucchelli G, Tavelli L. Do soft tissue augmentation techniques provide stable and favorable peri-implant conditions in the medium and long term? A systematic review. Clin Oral Implants Res. 2023 Sep;34 Suppl 26:28-42. [DOI:10.1111/clr.14150] [PMID]
10. Moraschini V, Luz D, Velloso G, Barboza EDP. Quality assessment of systematic reviews of the significance of keratinized mucosa on implant health. Int J Oral Maxillofac Surg. 2017 Jun;46(6):774-81. [DOI:10.1016/j.ijom.2017.02.1274] [PMID]
11. Cehreli MC, Karasoy D, Kökat AM, Akça K, Eckert S. A systematic review of marginal bone loss around implants retaining or supporting overdentures. Int J Oral Maxillofac Implants. 2010 Mar-Apr;25(2):266-77.
12. Fischer KR, Künzlberger A, Donos N, Fickl S, Friedmann A. Gingival biotype revisited-novel classification and assessment tool. Clin Oral Investig. 2018 Jan;22(1):443-8. [DOI:10.1007/s00784-017-2131-1] [PMID]
13. Lombardi T, Berton F, Salgarello S, Barbalonga E, Rapani A, Piovesana F, Gregorio C, Barbati G, Di Lenarda R, Stacchi C. Factors Influencing Early Marginal Bone Loss around Dental Implants Positioned Subcrestally: A Multicenter Prospective Clinical Study. J Clin Med. 2019 Aug 4;8(8):1168. [DOI:10.3390/jcm8081168] [PMID] []
14. Kim BS, Kim YK, Yun PY, Yi YJ, Lee HJ, Kim SG, Son JS. Evaluation of peri-implant tissue response according to the presence of keratinized mucosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Mar;107(3):e24-8. [DOI:10.1016/j.tripleo.2008.12.010] [PMID]
15. Ravidà A, Saleh I, Siqueira R, Garaicoa-Pazmiño C, Saleh MHA, Monje A, Wang HL. Influence of keratinized mucosa on the surgical therapeutical outcomes of peri-implantitis. J Clin Periodontol. 2020 Apr;47(4):529-39. [DOI:10.1111/jcpe.13250] [PMID]
16. Boynueğri D, Nemli SK, Kasko YA. Significance of keratinized mucosa around dental implants: a prospective comparative study. Clin Oral Implants Res. 2013 Aug;24(8):928-33. [DOI:10.1111/j.1600-0501.2012.02475.x] [PMID]
17. Bouri A Jr, Bissada N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int J Oral Maxillofac Implants. 2008 Mar-Apr;23(2):323-6.
18. Güven SŞ, Cabbar F, Güler N. Local and systemic factors associated with marginal bone loss around dental implants: a retrospective clinical study. Quintessence Int. 2020;51(2):128-41.
19. Suárez-López Del Amo F, Lin GH, Monje A, Galindo-Moreno P, Wang HL. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J Periodontol. 2016 Jun;87(6):690-9. [DOI:10.1902/jop.2016.150571] [PMID]
20. Naser mostofy S, Jalalian E, Valaie N, Mohtashamrad Z, Haeri A, Bitaraf T. Study of the Effect of GapSeal on Microgap and Microleakage in Internal Hex Connection After Cyclic Loading. J Res Dent Maxillofac Sci 2019; 4 (3) :36-42. [DOI:10.29252/jrdms.4.3.36]
21. Adibrad M, Shahabuei M, Sahabi M. Significance of the width of keratinized mucosa on the health status of the supporting tissue around implants supporting overdentures. J Oral Implantol. 2009;35(5):232-7. [DOI:10.1563/AAID-JOI-D-09-00035.1] [PMID]
22. Telles LH, Portella FF, Rivaldo EG. Longevity and marginal bone loss of narrow-diameter implants supporting single crowns: A systematic review. PLoS One. 2019 Nov 11;14(11):e0225046. [DOI:10.1371/journal.pone.0225046] [PMID] []
23. Ma M, Qi M, Zhang D, Liu H. The Clinical Performance of Narrow Diameter Implants Versus Regular Diameter Implants: A Meta-Analysis. J Oral Implantol. 2019 Dec;45(6):503-8. [DOI:10.1563/aaid-joi-D-19-00025] [PMID]
24. Longoni S, Tinto M, Pacifico C, Sartori M, Andreano A. Effect of Peri-implant Keratinized Tissue Width on Tissue Health and Stability: Systematic Review and Meta-analysis. Int J Oral Maxillofac Implants. 2019 Nov/Dec;34(6):1307-17. [DOI:10.11607/jomi.7622] [PMID]
25. Perussolo J, Souza AB, Matarazzo F, Oliveira RP, Araújo MG. Influence of the keratinized mucosa on the stability of peri-implant tissues and brushing discomfort: A 4-year follow-up study. Clin Oral Implants Res. 2018 Dec;29(12):1177-85. [DOI:10.1111/clr.13381] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |