

Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 249-256 |
Back to browse issues page


Ethics code: None
Clinical trials code: None
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Madihi N, Hoorizad ganjkar M, Nasoohi N, Kaboudanian Ardestani A. Effect of Polywave and Monowave Light Curing Units on Color Change of Composites Containing Trime-thylbenzoyl-Diphenyl-Phosphine Before and After Aging. J Res Dent Maxillofac Sci 2023; 8 (4) :249-256
URL: http://jrdms.dentaliau.ac.ir/article-1-505-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-505-en.html



1- School of Dentistry, Tehran Medical Science Islamic Azad University, Tehran, Iran
2- Operative Dentistry Department, School of Dentistry, Tehran Medical Science Islamic Azad University, Tehran, Iran , Mahoorizad@yahoo.com
3- Operative Dentistry Department, School of Dentistry, Tehran Medical Science Islamic Azad University, Tehran, Iran
2- Operative Dentistry Department, School of Dentistry, Tehran Medical Science Islamic Azad University, Tehran, Iran , Mahoorizad@yahoo.com
3- Operative Dentistry Department, School of Dentistry, Tehran Medical Science Islamic Azad University, Tehran, Iran
Full-Text [PDF 740 kb]
(213 Downloads)
| Abstract (HTML) (841 Views)
Introduction
Color stability is an essential factor in success of esthetic dental restorations, and discoloration is a leading cause of restoration replacement, especially in anterior teeth.
Discoloration is multifactorial and can be either intrinsic or extrinsic [1]. Extrinsic factors affecting discoloration can result from dietary and smoking habits and bad oral hygiene, while filler particle structure, photo-initiator, resin matrix, filler-resin bond, composite color, and degree of polymerization are contributing factors to intrinsic discoloration [1-3]. Inadequate polymerization not only induces a reduction in composites' physicomechanical properties and biocompatibility but also increases the composite’s susceptibility to color change [4-8].
The growing demand for esthetic restorations in dentistry has spurred the rapid advancement of light-cure composite resins. Consequently, light-curing units were evolved to effectively polymerize light-activated composite resins [9]. Light-emitting diode (LED) curing units are the most commonly employed light-activation units in dentistry [10]. Their conventional types are mono-wave and have an emission spectrum of blue light to match the absorption spectrum of camphorquinone (CQ) [4, 7, 11-14]. CQ is the most widely used photo-initiator in composite resins which has a bright yellow shade that can affect the color of composites when lighter shades are desired. To address this, alternative initiators like Lucirin trimethylbenzoyl-diphenyl-phosphine oxide (TPO), with an emission spectrum peaking at shorter wavelengths in the violet light range (<420 nm), were incorporated in composite formulations to reduce the reliance on CQ [3, 4, 10, 13, 15]. Combined incorporation of multiple photo-initiators led to better esthetics and a higher degree of polymerization in composite resins [7, 11, 15-17]. As a result, poly-wave LED units that emit a broader spectrum ranging from blue light to ultraviolet light were introduced to facilitate curing with materials containing initiators other than or in addition to CQ [7, 15].
Presently, different composites and light-curing devices are used in dental clinics. In many cases, the dentist is unaware of the type of composite’s photo-initiator or light curing unit’s emission wavelength; thus, the question is whether problematic discoloration occurs over time when various light-curing units are employed in the clinical setting for curing of TPO-containing composites.
There is some evidence regarding the curing efficiency, degree of polymerization, and hardness of TPO-containing composites when using monowave and polywave light-curing units. Certain studies have indicated that polywave devices contribute to a higher degree of polymerization [4, 15]; while, no significant difference was observed between the two devices in another study [10]. The results regarding the hardness of TPO-containing composites have been controversial following the use of various curing units. Additionally, a study reported that TPO-containing composites demonstrated higher color stability compared to CQ-containing composites [18]. Several studies have been conducted on the effect of aging on color change (ΔE) of composites. However, limited evidence is available about the ΔE of TPO-containing composites cured by various curing units following aging.
The present study aimed to evaluate the ΔE of two TPO-containing composites cured with monowave and polywave light-curing units after accelerated artificial aging (AAA). The null hypothesis was that there would be no significant difference in discoloration of TPO-containing composites cured with either polywave or monowave light-curing units followed by AAA.
Materials and Methods
This in vitro experimental study used two TPO-containing composite resins namely Tetric N-Ceram (Ivoclar Vivadent, Liechtenstein) and Vit-l-escence (Ultradent, USA) in A1 shade [10]. The study was approved by the Research Council of Tehran Medical Science Islamic Azad University (IR.IAU.DENTAL.REC.1399.230).
Ten samples were fabricated from each composite type measuring 10 mm in diameter and 2 mm in thickness [15, 19, 20] by filling stainless steel molds on a Mylar strip (KerrHawe SA, Bioggio, Switzerland) and a glass slide. Another Mylar strip and a cover-slip covered each sample, and pressed by a 1-kg load to extrude excess material [15, 21]. The samples were light-cured for 20 seconds using Bluephase G2 (Ivoclar Vivadent, Liechtenstein) polywave curing unit in the low mode with 650 mW/cm2 intensity or Bluephase C5 (Ivoclar Vivadent, Liechtenstein) monowave curing unit with 600 mW/cm2 intensity through the cover-slip using the overlapping technique.
The output of the light-curing units was tested with a radiometer per specimen. The Mylar strips were discarded immediately after curing, and the samples were wet-polished with Sof-Lex aluminum oxide discs (coarse, medium, and fine, respectively) [4, 22]. All samples were stored in distilled water at 37°C for 24 hours prior to initial colorimetry [22]. A spectrophotometer (SP64 Xrite, USA) was used for initial colorimetry using the CIE L*a*b* color system [20]. Afterwards, the samples underwent AAA for 384 hours in a weathering tester (QUV, Q-panel, USA) according to the ASTMA standard protocol. The working program was set to 4 hours of exposure to UV-B at 50°C and 4 hours of water condensation at 50°C; the maximum aging time was 384 hours, corresponding to 1 year of clinical use [23].
Accordingly, in this study, 10 samples from each group (n=10) and a total of 40 composite samples were studied as follows [20, 23]: P1: Tetric N-Ceram cured with polywave curing unit P2: Vit-l-escence cured with polywave curing unit M1: Tetric N-Ceram cured with monowave curing unit M2: Vit-l-escence cured with monowave curing unit Then, final colorimetry was performed using a spectrophotometer (SP64 Xrite, USA), and ΔE was calculated using the following formula:

The data were analyzed by two-way ANOVA.
Results
The findings indicated that the interaction effect of composite type and light-curing unit type on ΔE was not significant (P=0.53).
Therefore, the effects of light-curing units and composites on ΔE were separately investigated. The two types of composites had a significant difference in ΔE (P=0.00). Tetric N-Ceram demonstrated significantly lower ΔE than Vit-l-escence.
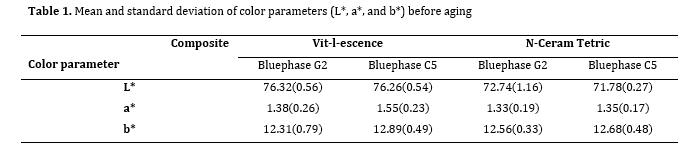
Before aging, the mean color parameters of Tetric N-Ceram (L, a, b) were as follows: L*= 72.74±1.16, a*=1.33±0.19, and b*=12.56±0.33 with the Bluephase G2 light-curing unit, and L*= 71.78±0.27, a*=1.35±0.17, and b*=12.68±0.48 with the Bluephase C5 light-curing unit (Table 1).
Before aging, the mean color parameters of Vit-l-escence were as follows: L*= 76.32±0.56, a*=1.38±0.26, and b*=12.31±0.79 with the Bluephase G2 light-curing unit, and L*= 76.26±0.54, a*=1.55±0.23, and b*=12.89±0.49 with the Bluephase C5 light-curing unit (Table 1).
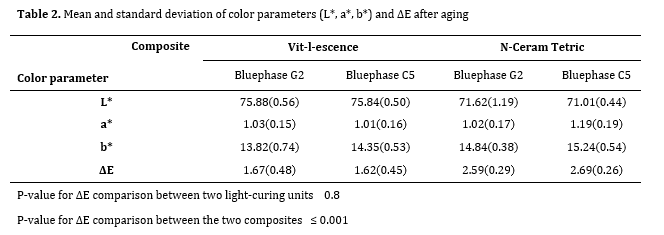
After aging, the mean color parameters of Tetric N-Ceram (L, a, b) were as follows: L*= 71.62±1.19, a*=1.02±0.17, and b*=14.84±0.38 with the Bluephase G2 light-curing unit, and L*= 71.01±0.44, a*=1.19±0.19, and b*=15.24±0.54 with the Bluephase C5 light-curing unit (Table 1).
After aging, the mean color parameters of Vit-l-escence (L, a, b) were as follows: L*= 75.88±0.56, a*=1.03±0.15, and b*=13.82±0.74 with the Bluephase G2 light-curing unit, and L*= 75.84±0.50, a*=1.01±0.16, and b*=14.35±0.53 with the BluephaseC5 light-curing unit (Table 1).
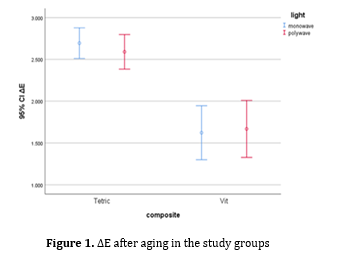
The mean ΔE in Vit-l-escence composite cured with Bluephase G2 and Bluephase C5 light-curing units was 1.67±0.48 and 1.62±0.45, respectively. These values were 2.59±0.29 and 2.69±0.26, respectively for Tetric N-Ceram composite cured with Bluephase G2 and Bluephase C5 light-curing units. The type of light-curing unit did not significantly affect the amount of ΔE of the two composites after aging (P=0.80). Table 1 shows the color parameters obtained in all groups before aging, and Table 2 indicates the color parameters and ΔE after aging. Figure 1summarizes the ΔE of the investigated groups.
Figure 1. ΔE after aging in the study groups
Table 1. Mean and standard deviation of color parameters (L*, a*, and b*) before aging
Table 2. Mean and standard deviation of color parameters (L*, a*, b*) and ΔE after aging
Discussion
The null hypothesis regarding no significant difference in discoloration between TPO-containing composites cured with polywave and monowave light-curing units after aging was accepted, as ΔE remained below 3.3 in all four groups. ΔE>1 indicates a perceptible difference between two colors, which can be perceived visually by at least 50% of the observers. The acceptable level of ΔE from the clinical point of view is controversial. Some studies considered ΔE>2.7 as clinically unacceptable, while others considered ΔE>3.3‒3.7 to be unacceptable from the clinical point of view [24]. However, most studies considered ΔE≤3.3 to be acceptable from the clinical point of view [1, 19, 25]. Thus, color change was acceptable in all specimens in the present study.
Composite resins as restorative materials have been widely employed due to their outstanding esthetic properties and bonding to enamel and dentin. However, their discoloration is a drawback and a primary reason for restoration replacement [5]. During clinical service, dental restorative materials must withstand widely variable conditions, including temperature shifts, continuous exposure to moisture, and mechanical stresses. Controlled clinical trials are necessary to affirm the reliability of treatments. Unfortunately, they are costly and time-consuming. Therefore, in vitro testing is an inexpensive technique that may precede clinical studies assessing the reliability of new restorative materials [26]. AAA simulates the environmental factors such as UV light and thermal and moisture fluxes. This technique was introduced in 1978 to evaluate the color stability of dental resin materials [24]. In this method, changes mainly occur in the organic matrix leading to color change and are related to composites' structural and chemical properties [21]. Studies have shown that the most significant color changes during 1440 hours of AAA occur during the first 300 hours [24].
According to a study, the results of 300 hours of AAA were the same as the results of 150 hours; therefore, aging of materials for more extended periods of time is believed to be unnecessary [22]. Some studies stated that 300 hours of AAA would correspond to 1 year of clinical performance [19, 26, 27]; while others corresponded 384 hours to 1 year of clinical service [21, 23], In the present study, specimens were submitted to 384 hours of AAA.
Discoloration of composite resins is multifactorial, and can be due to intrinsic or extrinsic factors. The intrinsic factors involve alterations in chemical stability of the resin matrix and the filler-matrix interface. In contrast, extrinsic factors are related to absorption of pigments and staining from exogenous sources, related to hygiene, dietary, and smoking habits [23, 28]. In the present study, the aim was to evaluate intrinsic factors.
A high degree of polymerization of composites is required to achieve optimal clinical and mechanical properties. CQ is the most widely used photo-initiator in composite resins. A high percentage of CQ helps improve the degree of polymerization, but it can be problematic in esthetic areas due to its yellow color. New optical initiators such as PPD, TPO, and DMBZ were added to composites to solve this problem. One of the problems of new composites is the incompatibility of light initiators with the wavelength range of conventional monowave light curing units. The absorbable spectrum of these photo-initiators is in the range of UV waves [29]. To solve this problem, polywave light curing units were released to the market, which have a wider wavelength range and can enable sufficient polymerization of these composites [10, 30, 31]. The clinicians need to know whether the composites containing TPO have acceptable polymerization if poly-wave units are not accessible and monowave units should be necessarily used [7].
The present study showed that in composites containing TPO, curing by polywave and monowave units did not show any difference in terms of color change after AAA. The results of Sim et al. [10], who examined the effect of single peak and dual peak devices on microhardness of composites containing TPO showed that microhardness mainly depended on the composite type and dual peak devices had an increasing effect on the microhardness of composites containing TPO. Lucy et al. [4] showed that the difference in the degree of polymerization of composites containing TPO after using single peak and dual peak devices was not significant. Conte et al. [7] and Santini et al. [15] reported that polywave devices produced a higher degree of polymerization and hardness in TPO-containing composites compared to monowave types. Sufficient optical polymerization is essential to improve composites' physical, mechanical and clinical properties. During the polymerization process, it would be ideal if all monomers participate in the reaction, but this never happens, and some monomers always remain unreacted [32]. Normally, the degree of polymerization of dimethacrylate polymers is between 43% and 75% [14]. The degree of polymerization may affect the degree of color change because as the degree of polymerization increases, the number of free monomers that cause color change of composites decreases. It should be noted that a correlation between the color stability of composite and degree of polymerization has never been proven [5]. A study on polywave and monowave light curing units showed that all light curing units led to a degree of polymerization above 50% in all types of composites, including those containing CQ and TPO, and an increase in degree of polymerization does not necessarily enhance the properties of composites [6]. Evidence shows that composites that have more than 35% free monomers are highly susceptible to color change [25]. In the present study, Vit-l-escence showed better chemical stability than Tetric N-Ceram. The color stability of composites depends on their properties, including matrix and filler combination (particle size, type of particles, percentage of particles), matrix and filler interface, composite color, degree of polymerization, and polishing technique of composites [22]. Tetric N-Ceram and Vit-l-escence composites are different in terms of chemical structure of dimethacrylate monomers. Presence of HEMA as a hydrophilic monomer can make Tetric N-Ceram more susceptible to color change due to water sorption [23]. Also, difference in type of fillers may play a role in this regard. Vit-l-escence is a micro-hybrid composite with an average particle size of 0.7 µm, while Tetric N-Ceram is a nanohybrid composite with a particle size of 40-3000 nm. The results showed that the degree of polymerization of composites containing nanofiller is much lower than that of micro-hybrid composites due to light refraction [32]. Santini et al, also showed that the degree of polymerization of Tetric N-Ceram composite was lower than that of Vit-l-escence [15]. In the present study, the samples were fabricated from A1 shade of composites with a thickness of 2 mm, equivalent to the thickness that can be cured in the clinical setting [4]. To simulate the clinical conditions, all the composite samples were wet-polished by polishing discs to remove the resin-rich layer [11]. Other factors influencing the polymerization of composites include the light intensity and duration of light curing [32]. In the present study, duration of light curing was standardized in all samples according to the manufacturers’ brochure, but it was impossible to standardize the light intensity, which depends on the commercial type of device. The light intensity of Bluephase C5 used in the present study was 600 mW/cm2, but Bluephase N2 has two modes of high (1200 mW/cm2) and low (650 mW/cm2); in the present study, the low mode of the curing unit was used to bring the light intensity of the two light curing units closer. The free monomersremaining in the composites can react with the pigments and lead to a change in the composites' color [24]. Therefore, future studies should focus on external color change of composites after immersing the samples in color solutions.
Conclusion
The results of the present study indicated that type of composite used had an impact on the extent of color change observed after clinical use. However, type of light-curing unit did not have a significant effect on the color change of composites. In other words, the material used for composite restoration affects its color change, but the device used to cure the composite does not have a noticeable impact on its color change
Conflict of interest
The authors declare no conflict of interests.
Acknowledgments
The authors would like to acknowledge colleagues who gave valuable comments.
Full-Text: (90 Views)
| Abstract
Background and Aim: The use of traditional camphorquinone (CQ) photo-initiators in dental composites may cause undesirable yellow discoloration. An alternative photo-initiator called lucirin trimethylbenzoyl-diphenyl-phosphine oxide (TPO) was recently introduced which exhibits minimal color change (ΔE). This study evaluated the color change of TPO-containing composites cured by different types of light-curing units, after accelerated artificial aging (AAA). Materials and Methods: In this in vitro experimental study, specimens were fabricated from Tetric N-Ceram and Vit-l-escence TPO-containing composites with 10 mm diameter and 2 mm thickness (n=10) and light-cured by Bluephase G2 polywave and Bluephase C5 monowave curing units. The samples were polished with Sof-Lex discs and underwent initial colorimetry by a spectrophotometer after 24 hours. Aging was performed for 384 hours in a weathering chamber and final colorimetry was then performed. The results were analyzed by two-way ANOVA. Results: The interaction effect of light curing unit and composite type on ΔE was not significant (P=0.53). The mean ΔE of Vit-l-escence and Tetric N-Ceram cured with Bluephase G2 and Bluephase C5 light-curing units was 1.67±0.48 and 1.62±0.45, and 2.59±0.29 and 2.69±0.26, respectively. Tetric N-Ceram demonstrated significantly greater ΔE than Vit-l-escence (P=0.001). Light curing units had no significant difference in ΔE (P=0.80). Conclusion: The ΔE of TPO-containing composites does not depend on the type of light curing unit but depends on the type of composite. Aging caused discoloration of the composites but this discoloration was clinically acceptable (ΔE<3. 3). Key Words: Aging; Composite Resins; Curing Lights, Dental; Photoinitiators, Dental |
Introduction
Color stability is an essential factor in success of esthetic dental restorations, and discoloration is a leading cause of restoration replacement, especially in anterior teeth.
Discoloration is multifactorial and can be either intrinsic or extrinsic [1]. Extrinsic factors affecting discoloration can result from dietary and smoking habits and bad oral hygiene, while filler particle structure, photo-initiator, resin matrix, filler-resin bond, composite color, and degree of polymerization are contributing factors to intrinsic discoloration [1-3]. Inadequate polymerization not only induces a reduction in composites' physicomechanical properties and biocompatibility but also increases the composite’s susceptibility to color change [4-8].
The growing demand for esthetic restorations in dentistry has spurred the rapid advancement of light-cure composite resins. Consequently, light-curing units were evolved to effectively polymerize light-activated composite resins [9]. Light-emitting diode (LED) curing units are the most commonly employed light-activation units in dentistry [10]. Their conventional types are mono-wave and have an emission spectrum of blue light to match the absorption spectrum of camphorquinone (CQ) [4, 7, 11-14]. CQ is the most widely used photo-initiator in composite resins which has a bright yellow shade that can affect the color of composites when lighter shades are desired. To address this, alternative initiators like Lucirin trimethylbenzoyl-diphenyl-phosphine oxide (TPO), with an emission spectrum peaking at shorter wavelengths in the violet light range (<420 nm), were incorporated in composite formulations to reduce the reliance on CQ [3, 4, 10, 13, 15]. Combined incorporation of multiple photo-initiators led to better esthetics and a higher degree of polymerization in composite resins [7, 11, 15-17]. As a result, poly-wave LED units that emit a broader spectrum ranging from blue light to ultraviolet light were introduced to facilitate curing with materials containing initiators other than or in addition to CQ [7, 15].
Presently, different composites and light-curing devices are used in dental clinics. In many cases, the dentist is unaware of the type of composite’s photo-initiator or light curing unit’s emission wavelength; thus, the question is whether problematic discoloration occurs over time when various light-curing units are employed in the clinical setting for curing of TPO-containing composites.
There is some evidence regarding the curing efficiency, degree of polymerization, and hardness of TPO-containing composites when using monowave and polywave light-curing units. Certain studies have indicated that polywave devices contribute to a higher degree of polymerization [4, 15]; while, no significant difference was observed between the two devices in another study [10]. The results regarding the hardness of TPO-containing composites have been controversial following the use of various curing units. Additionally, a study reported that TPO-containing composites demonstrated higher color stability compared to CQ-containing composites [18]. Several studies have been conducted on the effect of aging on color change (ΔE) of composites. However, limited evidence is available about the ΔE of TPO-containing composites cured by various curing units following aging.
The present study aimed to evaluate the ΔE of two TPO-containing composites cured with monowave and polywave light-curing units after accelerated artificial aging (AAA). The null hypothesis was that there would be no significant difference in discoloration of TPO-containing composites cured with either polywave or monowave light-curing units followed by AAA.
Materials and Methods
This in vitro experimental study used two TPO-containing composite resins namely Tetric N-Ceram (Ivoclar Vivadent, Liechtenstein) and Vit-l-escence (Ultradent, USA) in A1 shade [10]. The study was approved by the Research Council of Tehran Medical Science Islamic Azad University (IR.IAU.DENTAL.REC.1399.230).
Ten samples were fabricated from each composite type measuring 10 mm in diameter and 2 mm in thickness [15, 19, 20] by filling stainless steel molds on a Mylar strip (KerrHawe SA, Bioggio, Switzerland) and a glass slide. Another Mylar strip and a cover-slip covered each sample, and pressed by a 1-kg load to extrude excess material [15, 21]. The samples were light-cured for 20 seconds using Bluephase G2 (Ivoclar Vivadent, Liechtenstein) polywave curing unit in the low mode with 650 mW/cm2 intensity or Bluephase C5 (Ivoclar Vivadent, Liechtenstein) monowave curing unit with 600 mW/cm2 intensity through the cover-slip using the overlapping technique.
The output of the light-curing units was tested with a radiometer per specimen. The Mylar strips were discarded immediately after curing, and the samples were wet-polished with Sof-Lex aluminum oxide discs (coarse, medium, and fine, respectively) [4, 22]. All samples were stored in distilled water at 37°C for 24 hours prior to initial colorimetry [22]. A spectrophotometer (SP64 Xrite, USA) was used for initial colorimetry using the CIE L*a*b* color system [20]. Afterwards, the samples underwent AAA for 384 hours in a weathering tester (QUV, Q-panel, USA) according to the ASTMA standard protocol. The working program was set to 4 hours of exposure to UV-B at 50°C and 4 hours of water condensation at 50°C; the maximum aging time was 384 hours, corresponding to 1 year of clinical use [23].
Accordingly, in this study, 10 samples from each group (n=10) and a total of 40 composite samples were studied as follows [20, 23]: P1: Tetric N-Ceram cured with polywave curing unit P2: Vit-l-escence cured with polywave curing unit M1: Tetric N-Ceram cured with monowave curing unit M2: Vit-l-escence cured with monowave curing unit Then, final colorimetry was performed using a spectrophotometer (SP64 Xrite, USA), and ΔE was calculated using the following formula:
The data were analyzed by two-way ANOVA.
Results
The findings indicated that the interaction effect of composite type and light-curing unit type on ΔE was not significant (P=0.53).
Therefore, the effects of light-curing units and composites on ΔE were separately investigated. The two types of composites had a significant difference in ΔE (P=0.00). Tetric N-Ceram demonstrated significantly lower ΔE than Vit-l-escence.
Before aging, the mean color parameters of Tetric N-Ceram (L, a, b) were as follows: L*= 72.74±1.16, a*=1.33±0.19, and b*=12.56±0.33 with the Bluephase G2 light-curing unit, and L*= 71.78±0.27, a*=1.35±0.17, and b*=12.68±0.48 with the Bluephase C5 light-curing unit (Table 1).
Before aging, the mean color parameters of Vit-l-escence were as follows: L*= 76.32±0.56, a*=1.38±0.26, and b*=12.31±0.79 with the Bluephase G2 light-curing unit, and L*= 76.26±0.54, a*=1.55±0.23, and b*=12.89±0.49 with the Bluephase C5 light-curing unit (Table 1).
After aging, the mean color parameters of Tetric N-Ceram (L, a, b) were as follows: L*= 71.62±1.19, a*=1.02±0.17, and b*=14.84±0.38 with the Bluephase G2 light-curing unit, and L*= 71.01±0.44, a*=1.19±0.19, and b*=15.24±0.54 with the Bluephase C5 light-curing unit (Table 1).
After aging, the mean color parameters of Vit-l-escence (L, a, b) were as follows: L*= 75.88±0.56, a*=1.03±0.15, and b*=13.82±0.74 with the Bluephase G2 light-curing unit, and L*= 75.84±0.50, a*=1.01±0.16, and b*=14.35±0.53 with the BluephaseC5 light-curing unit (Table 1).
The mean ΔE in Vit-l-escence composite cured with Bluephase G2 and Bluephase C5 light-curing units was 1.67±0.48 and 1.62±0.45, respectively. These values were 2.59±0.29 and 2.69±0.26, respectively for Tetric N-Ceram composite cured with Bluephase G2 and Bluephase C5 light-curing units. The type of light-curing unit did not significantly affect the amount of ΔE of the two composites after aging (P=0.80). Table 1 shows the color parameters obtained in all groups before aging, and Table 2 indicates the color parameters and ΔE after aging. Figure 1summarizes the ΔE of the investigated groups.
Figure 1. ΔE after aging in the study groups
{kind=link}
Table 1. Mean and standard deviation of color parameters (L*, a*, and b*) before aging
{kind=link}
Table 2. Mean and standard deviation of color parameters (L*, a*, b*) and ΔE after aging
{kind=link}
Discussion
The null hypothesis regarding no significant difference in discoloration between TPO-containing composites cured with polywave and monowave light-curing units after aging was accepted, as ΔE remained below 3.3 in all four groups. ΔE>1 indicates a perceptible difference between two colors, which can be perceived visually by at least 50% of the observers. The acceptable level of ΔE from the clinical point of view is controversial. Some studies considered ΔE>2.7 as clinically unacceptable, while others considered ΔE>3.3‒3.7 to be unacceptable from the clinical point of view [24]. However, most studies considered ΔE≤3.3 to be acceptable from the clinical point of view [1, 19, 25]. Thus, color change was acceptable in all specimens in the present study.
Composite resins as restorative materials have been widely employed due to their outstanding esthetic properties and bonding to enamel and dentin. However, their discoloration is a drawback and a primary reason for restoration replacement [5]. During clinical service, dental restorative materials must withstand widely variable conditions, including temperature shifts, continuous exposure to moisture, and mechanical stresses. Controlled clinical trials are necessary to affirm the reliability of treatments. Unfortunately, they are costly and time-consuming. Therefore, in vitro testing is an inexpensive technique that may precede clinical studies assessing the reliability of new restorative materials [26]. AAA simulates the environmental factors such as UV light and thermal and moisture fluxes. This technique was introduced in 1978 to evaluate the color stability of dental resin materials [24]. In this method, changes mainly occur in the organic matrix leading to color change and are related to composites' structural and chemical properties [21]. Studies have shown that the most significant color changes during 1440 hours of AAA occur during the first 300 hours [24].
According to a study, the results of 300 hours of AAA were the same as the results of 150 hours; therefore, aging of materials for more extended periods of time is believed to be unnecessary [22]. Some studies stated that 300 hours of AAA would correspond to 1 year of clinical performance [19, 26, 27]; while others corresponded 384 hours to 1 year of clinical service [21, 23], In the present study, specimens were submitted to 384 hours of AAA.
Discoloration of composite resins is multifactorial, and can be due to intrinsic or extrinsic factors. The intrinsic factors involve alterations in chemical stability of the resin matrix and the filler-matrix interface. In contrast, extrinsic factors are related to absorption of pigments and staining from exogenous sources, related to hygiene, dietary, and smoking habits [23, 28]. In the present study, the aim was to evaluate intrinsic factors.
A high degree of polymerization of composites is required to achieve optimal clinical and mechanical properties. CQ is the most widely used photo-initiator in composite resins. A high percentage of CQ helps improve the degree of polymerization, but it can be problematic in esthetic areas due to its yellow color. New optical initiators such as PPD, TPO, and DMBZ were added to composites to solve this problem. One of the problems of new composites is the incompatibility of light initiators with the wavelength range of conventional monowave light curing units. The absorbable spectrum of these photo-initiators is in the range of UV waves [29]. To solve this problem, polywave light curing units were released to the market, which have a wider wavelength range and can enable sufficient polymerization of these composites [10, 30, 31]. The clinicians need to know whether the composites containing TPO have acceptable polymerization if poly-wave units are not accessible and monowave units should be necessarily used [7].
The present study showed that in composites containing TPO, curing by polywave and monowave units did not show any difference in terms of color change after AAA. The results of Sim et al. [10], who examined the effect of single peak and dual peak devices on microhardness of composites containing TPO showed that microhardness mainly depended on the composite type and dual peak devices had an increasing effect on the microhardness of composites containing TPO. Lucy et al. [4] showed that the difference in the degree of polymerization of composites containing TPO after using single peak and dual peak devices was not significant. Conte et al. [7] and Santini et al. [15] reported that polywave devices produced a higher degree of polymerization and hardness in TPO-containing composites compared to monowave types. Sufficient optical polymerization is essential to improve composites' physical, mechanical and clinical properties. During the polymerization process, it would be ideal if all monomers participate in the reaction, but this never happens, and some monomers always remain unreacted [32]. Normally, the degree of polymerization of dimethacrylate polymers is between 43% and 75% [14]. The degree of polymerization may affect the degree of color change because as the degree of polymerization increases, the number of free monomers that cause color change of composites decreases. It should be noted that a correlation between the color stability of composite and degree of polymerization has never been proven [5]. A study on polywave and monowave light curing units showed that all light curing units led to a degree of polymerization above 50% in all types of composites, including those containing CQ and TPO, and an increase in degree of polymerization does not necessarily enhance the properties of composites [6]. Evidence shows that composites that have more than 35% free monomers are highly susceptible to color change [25]. In the present study, Vit-l-escence showed better chemical stability than Tetric N-Ceram. The color stability of composites depends on their properties, including matrix and filler combination (particle size, type of particles, percentage of particles), matrix and filler interface, composite color, degree of polymerization, and polishing technique of composites [22]. Tetric N-Ceram and Vit-l-escence composites are different in terms of chemical structure of dimethacrylate monomers. Presence of HEMA as a hydrophilic monomer can make Tetric N-Ceram more susceptible to color change due to water sorption [23]. Also, difference in type of fillers may play a role in this regard. Vit-l-escence is a micro-hybrid composite with an average particle size of 0.7 µm, while Tetric N-Ceram is a nanohybrid composite with a particle size of 40-3000 nm. The results showed that the degree of polymerization of composites containing nanofiller is much lower than that of micro-hybrid composites due to light refraction [32]. Santini et al, also showed that the degree of polymerization of Tetric N-Ceram composite was lower than that of Vit-l-escence [15]. In the present study, the samples were fabricated from A1 shade of composites with a thickness of 2 mm, equivalent to the thickness that can be cured in the clinical setting [4]. To simulate the clinical conditions, all the composite samples were wet-polished by polishing discs to remove the resin-rich layer [11]. Other factors influencing the polymerization of composites include the light intensity and duration of light curing [32]. In the present study, duration of light curing was standardized in all samples according to the manufacturers’ brochure, but it was impossible to standardize the light intensity, which depends on the commercial type of device. The light intensity of Bluephase C5 used in the present study was 600 mW/cm2, but Bluephase N2 has two modes of high (1200 mW/cm2) and low (650 mW/cm2); in the present study, the low mode of the curing unit was used to bring the light intensity of the two light curing units closer. The free monomersremaining in the composites can react with the pigments and lead to a change in the composites' color [24]. Therefore, future studies should focus on external color change of composites after immersing the samples in color solutions.
Conclusion
The results of the present study indicated that type of composite used had an impact on the extent of color change observed after clinical use. However, type of light-curing unit did not have a significant effect on the color change of composites. In other words, the material used for composite restoration affects its color change, but the device used to cure the composite does not have a noticeable impact on its color change
Conflict of interest
The authors declare no conflict of interests.
Acknowledgments
The authors would like to acknowledge colleagues who gave valuable comments.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Farah RI, Elwi H. Spectrophotometric evaluation of color changes of bleach-shade resin-based composites after staining and bleaching. J Contemp Dent Pract. 2014 Sep 1;15 (5):587-94. [DOI:10.5005/jp-journals-10024-1584] [PMID]
2. AlSheikh R. Color stability of Lucirin-photo-activated resin composite after immersion in different staining solutions: a spectrophotometric study. Clin Cosmet Investig Dent. 2019 Sep 5;11:297-311. [DOI:10.2147/CCIDE.S216011] [PMID] []
3. Yazici AR, Celik C, Dayangaç B, Ozgünaltay G. The effect of curing units and staining solutions on the color stability of resin composites. Oper Dent. 2007 Nov-Dec;32(6):616-22. [DOI:10.2341/07-3] [PMID]
4. Lucey SM, Santini A, Roebuck EM. Degree of conversion of resin-based materials cured with dual-peak or single-peak LED light-curing units. Int J Paediatr Dent. 2015 Mar; 25(2): 93-102. [DOI:10.1111/ipd.12104] [PMID]
5. Domingos PA, Garcia PP, Oliveira AL, Palma-Dibb RG. Compo-site resin color stability: influence of light sources and immer-sion media. J Appl Oral Sci. 2011 May-Jun;19(3):204-11. [DOI:10.1590/S1678-77572011000300005] [PMID] []
6. Derchi G, Vano M, Ceseracciu L, Diaspro A, Salerno M. Stiffness effect of using polywave or monowave LED units for photo-curing different bulk fill composites. Dent Mater J. 2018 Sep 30;37(5):709-16. [DOI:10.4012/dmj.2017-278] [PMID]
7. Conte G, Panetta M, Mancini M, Fabianelli A, Brotzu A, Sorge R, Cianconi L. Curing effectiveness of single-peak and multi-peak led light curing units on tpo-containing resin composites with different chromatic characteristics. Oral Implantol (Rome). 2017 Sep 27;10(2):140-50. [DOI:10.11138/orl/2017.10.2.140] [PMID] []
8. Favarão J, Oliveira D, Zanini MM, Rocha MG, Correr-Sobrinho L, Sinhoreti M. Effect of curing-light attenuation on color stabil-ity and physical and chemical properties of resin cements con-taining different photoinitiators. J Mech Behav Biomed Mater. 2021 Jan;113:104110. [DOI:10.1016/j.jmbbm.2020.104110] [PMID]
9. Tanthanuch S, Kukiattrakoon B. The effect of curing time by conventional quartz tungsten halogens and new light-emitting diodes light curing units on degree of conversion and micro-hardness of a nanohybrid resin composite. J Conserv Dent. 2019 Mar-Apr;22(2):196-200. [DOI:10.4103/JCD.JCD_498_18] [PMID] []
10. Sim JS, Seol HJ, Park JK, Garcia-Godoy F, Kim HI, Kwon YH. Interaction of LED light with coinitiator-containing composite resins: effect of dual peaks. J Dent. 2012 Oct; 40 (10):836-42. [DOI:10.1016/j.jdent.2012.06.008] [PMID]
11. Cardoso KA, Zarpellon DC, Madruga CF, Rodrigues JA, Arrais CA. Effects of radiant exposure values using second and third generation light curing units on the degree of conversion of a lucirin-based resin composite. J Appl Oral Sci. 2017 Mar-Apr;25(2):140-6. [DOI:10.1590/1678-77572016-0388] [PMID] []
12. Pratap B, Gupta RK, Bhardwaj B, Nag M. Resin based restora-tive dental materials: characteristics and future perspectives. Jpn Dent Sci Rev. 2019 Nov;55(1):126-138. [DOI:10.1016/j.jdsr.2019.09.004] [PMID] []
13. Sahadi BO, Price RB, André CB, Sebold M, Bermejo GN, Pal-ma-Dibb RG, Faraoni JJ, Soares CJ, Giannini M. Multiple-peak and single-peak dental curing lights comparison on the wear re-sistance of bulk-fill composites. Braz Oral Res. 2018 Dec 17;32:e122. [DOI:10.1590/1807-3107bor-2018.vol32.0122] [PMID]
14. AlShaafi MM. Factors affecting polymerization of resin-based composites: A literature review. Saudi Dent J. 2017 Apr;29(2):48-58. [DOI:10.1016/j.sdentj.2017.01.002] [PMID] []
15. Santini A, Miletic V, Swift MD, Bradley M. Degree of conversion and microhardness of TPO-containing resin-based composites cured by polywave and monowave LED units. J Dent. 2012 Jul;40(7):577-84. [DOI:10.1016/j.jdent.2012.03.007] [PMID]
16. Leprince JG, Hadis M, Shortall AC, Ferracane JL, Devaux J, Leloup G, Palin WM. Photoinitiator type and applicability of exposure reciprocity law in filled and unfilled photoactive res-ins. Dent Mater. 2011 Feb;27(2):157-64. [DOI:10.1016/j.dental.2010.09.011] [PMID]
17. Miletic V, Santini A. Micro-Raman spectroscopic analysis of the degree of conversion of composite resins containing differ-ent initiators cured by polywave or monowave LED units. J Dent. 2012 Feb;40(2):106-13. [DOI:10.1016/j.jdent.2011.10.018] [PMID]
18. Arikawa H, Takahashi H, Kanie T, Ban S. Effect of various visible light photoinitiators on the polymerization and color of light-activated resins. Dent Mater J. 2009 Jul;28(4):454-60. [DOI:10.4012/dmj.28.454] [PMID]
19. Nikzad S, Azari A, Poursina M. Effects of beverage colorants and accelerated aging on the color stability of indirect resin composites. J Dent Sci. 2012;7(3):231-7. [DOI:10.1016/j.jds.2012.05.006]
20. Nasoohi N, Hoorizad Gangkar M, Hashemi S, Mansouri M. The effect of aging on color change of composite contaning si-loran-based methacrylate. Journal of Isfahan Dental School. 2016;11(6).
21. Shirinzad M, Rezaei-Soufi L, Mirtorabi MS, Vahdatinia F. Ef-fect of Accelerated Artificial Aging on Translucency of Methac-rylate and Silorane-Based Composite Resins. J Dent (Tehran). 2016 Mar;13(2):92-100.
22. Tuncdemir AR, Güven ME. Effects of Fibers on Color and Translucency Changes of Bulk-Fill and Anterior Composites after Accelerated Aging. Biomed Res Int. 2018 Jan 28; 2018: 2908696. [DOI:10.1155/2018/2908696] [PMID] []
23. Pires-de-Souza Fde C, Garcia Lda F, Roselino Lde M, Naves LZ. Color stability of silorane-based composites submitted to accelerated artificial ageing--an in situ study. J Dent. 2011 Jul;39 Suppl 1:e18-24. [DOI:10.1016/j.jdent.2011.03.003] [PMID]
24. Hamedi Rad F, Ghaffari T, Tamgaji R. Evaluation of the Color Stability of Methyl Methacrylate and Nylon Base Polymer. J Dent (Shiraz). 2017 Jun;18(2):136-42.
25. Sarafianou A, Iosifidou S, Papadopoulos T, Eliades G. Color stability and degree of cure of direct composite restoratives after accelerated aging. Oper Dent. 2007 Jul-Aug; 32(4):406-11. [DOI:10.2341/06-127] [PMID]
26. Korkmaz Ceyhan Y, Ontiveros JC, Powers JM, Paravina RD. Accelerated aging effects on color and translucency of flowable composites. J Esthet Restor Dent. 2014 Jul-Aug; 26 (4):272-8. [DOI:10.1111/jerd.12093] [PMID]
27. Hoorizad Ganjkar M, Heshmat H, Gholamisinaki M, Emami Arjomand M. Effect of Accelerated Aging on the Color Stability of Light-cured Res-in Cement and Flowable Composite Through Porcelain Laminate Veneer. Journal of Is-lamic Dental Association of IRAN. 2017;29(4):103-9. [DOI:10.30699/jidai.29.3.103]
28. Varshney I, Jha P, Nikhil V. Effect of monowave and poly-wave light curing on the degree of conversion and microhardness of composites with different photoinitiators: An in vitro study. J Conserv Dent. 2022 Nov-Dec;25(6):661-5. [DOI:10.4103/jcd.jcd_223_22] [PMID] []
29. Lima RBW, Melo AMDS, Dias JDN, Barbosa LMM, Santos JVDN, Souza GM, Andrade AKM, Assunção IV, Borges BCD. Are polywave light-emitting diodes more effective than monowave ones in the photoactivation of resin-based materials containing alternative photoinitiators? A systematic review. J Mech Behav Biomed Mater. 2023 Jul; 143:105905.
30. Lara L, Rocha MG, Menezes LR, Correr AB, Sinhoreti MAC, Oliveira D. Effect of combining photoinitiators on cure efficiency of dental resin-based composites. J Appl Oral Sci. 2021 Jul 23;29:e20200467. [DOI:10.1590/1678-7757-2020-0467] [PMID] []
31. Farzad A, Kasraei S, Haghi S, Masoumbeigi M, Torabzadeh H, Panahandeh N. Effects of 3 different light-curing units on the physico-mechanical properties of bleach-shade resin composites. Restor Dent Endod. 2022 Feb 7;47 (1):e9. [DOI:10.5395/rde.2022.47.e9] [PMID] []
32. Jafarzadeh TS, Erfan M, Behroozibakhsh M, Fatemi M, Ma-saeli R, Rezaei Y, Bagheri H, Erfan Y. Evaluation of Polymeriza-tion Efficacy in Composite Resins via FT-IR Spectroscopy and Vickers Microhardness Test. J Dent Res Dent Clin Dent Prospects. 2015 Fall;9(4):226-32. [DOI:10.15171/joddd.2015.041] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
