

Volume 8, Issue 1 (1-2023)
J Res Dent Maxillofac Sci 2023, 8(1): 49-56 |
Back to browse issues page

Ethics code: IR.SBMU.RIDS.REC.1395.364
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Valian A, Tareh A, Zarei M, Gholami Mandali S. Effect of Pistacia lentiscus Extract on Dentin
Remineralization: An In Vitro Study. J Res Dent Maxillofac Sci 2023; 8 (1) :49-56
URL: http://jrdms.dentaliau.ac.ir/article-1-445-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-445-en.html



1- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Private Office, Tehran, Iran
3- Department of Pharmacology, Faculty of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran , sama.ghlm72@gmail.com
2- Private Office, Tehran, Iran
3- Department of Pharmacology, Faculty of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran , sama.ghlm72@gmail.com
Keywords: Dentin sensitivity, Dentin Desensitizing Agents, Pistacia lentiscus, Microscopy, Electron, Scanning
Full-Text [PDF 872 kb]
(467 Downloads)
| Abstract (HTML) (894 Views)
Introduction
Dentin hypersensitivity (DH) is a common clinical complaint, affecting 4% to 74% of the population [1-5]. It refers to the generation of short sharp pain in exposed dentin due to chemical, thermal, and osmotic stimuli [6]. This pain cannot be attributed to any other pathology [7, 8]. DH can lead to physical and psychological problems and affect the quality of life and the oral hygiene practice of patients [9]. Absence of enamel or cementum coverage on dentin and exposure of dentinal tubules into the oral cavity are the main reasons for DH [10]. Scanning electron microscopic (SEM) assessments have indicated that the number of exposed dentinal tubules in teeth with DH is 8 times higher than that in normal teeth [11-13]. Root surface denuding following gingival recession due to aging, chronic periodontitis, periodontal surgery, incorrect tooth brushing technique, occlusal trauma, scaling and rootplaning, and pocket removal surgery leads to cementum exposure [14].
According to the Brannstrom’s theory, the movement of dentinal fluid in dentinal tubules leads to stimulation of baroreceptors and pain generation [15]. In general, the mechanism of action of desensitizing agents is based on the reduction of dentinal fluid flow or decreasing the activity of nerve ends in dentin by interfering with their electrical conduction [16]. In the recent decades, several desensitizing agents have been proposed for treatment of DH such as fluoride, arginine, and citrate buffers [17].
The main mechanism of action of fluoride is through the prevention or reduction of fluid movement in dentinal tubules by the deposition of calcium and phosphorous compounds such as calcium fluoride and fluorapatite. Preliminary studies have demonstrated optimal desensitizing efficacy of fluoride products. The Canadian Advisory Board on Dentin Hypersensitivity in 2003 suggested the use of fluoridated toothpastes as the first-line non-invasive treatment for DH. Also, the efficacy of NaF as a fluoride compound for this purpose has been extensively studied [18].
The application of medicinal herbs for medical purposes has a long history. Use of Pistacia lentiscus (P. lentiscus) for treatment of gastrointestinal diseases in the Middle Eastern countries dates back to 3000 years ago [16]. P. lentiscus has selective antibacterial properties against Porphyromonas gingivalis and Prevotella melaninogenica. It also exerts anti-plaque effects by inhibiting the proliferation of salivary bacteria. In the Iranian traditional medicine, P. lentiscus is used for
enhancement of wound healing, treatment of gastrointestinal conditions, and for gingival health [15] Mastic gum is the resin released from the stem and leaves of P. lentiscus, which has therapeutic effects for treatment of gastrointestinal problems such as stomachache, indigestion, and gastrointestinal inflammation [19-21]. Evidence shows that chewing of mastic gum inhibits the proliferation of salivary bacteria and formation of microbial plaque on tooth surfaces [22]. Use of mastic gum for 3 weeks decreases the Streptococcus mutans count of the saliva and may help in caries prevention [23]. It has been demonstrated that mastic gum can enhance the remineralization of caries-like lesions; enhancement of remineralization appears to be related to increased saliva flow and pH due to mastication [1,24]. Different species of Pistacia have different chemical constituents such as phenol groups and gallic acid [25-27]. Gallic acid is a natural phenol compound found in many herbs and foods with anti-oxidant, anti-mutagenic, and anti-cariogenic properties. Gallic acid can also increase enamel remineralization and prevent demineralization [28]. A complex of metal ions and gallic acid can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. Calcium, potassium, and magnesium are the most abundant minerals in the leaves and fruits of P. lentiscus [30].
Considering the presence of phenol groups (gallic acid), minerals, and metal ions in P. lentiscus extract, this study aimed to assess the efficacy of P. lentiscus extract for dentin remineralization and sealing of dentinal tubules. The null hypothesis was that the effects of 10% P. lentiscus extract and 1000 PPM sodium fluoride (NaF) solution on the hardness of dentin would be the same.
Materials and Methods
Preparation of 10% alcoholic extract of P. lentiscus:
For this purpose, 10 g of dried solid mastic gum was weighed by a digital scale (Sartorius, type TE 124 S, Göttingen, Germany) and ground in a mortar and pestle. The obtained powder was dissolved in 10 cc of pure acetone and well stirred for 30 minutes for complete dissolution. Next, 95% alcohol was added to reach a total volume of 100 cc. The obtained solution was stirred for 30 minutes to obtain a homogenous solution; the pH was adjusted to 6-6.5 by a pH meter (Sartorius, PB 11, Göttingen, Germany).
Preparation of 1000 ppm NaF solution:
For this purpose, 1 g of NaF salt was weighed by a digital scale (Sartorius, type TE 124 S, Göttingen, Germany) and added to 1 L of deionized water and stirred for complete dissolution.
The demineralizing solution had a pH of 4 to 4.5 with the following formulation: NaCl (2.9 g), CaCl2 (0.12 g), NaH2PO4 (0.13 g), NaN3 (5 cc), and acetic acid (1.5 cc).
The remineralizing solution (artificial saliva) had a pH of 6.5 to 7 with the following formulation: NaCl (2.9 g), CaCl2 (0.12 g), NaH2PO4 (0.13 g), and NaN3 (5 cc) [31].
Sample preparation:
The sample size was found to be 15 per group using the multiple comparisons feature of PASS software considering alpha=0.05, beta=0.1, standard deviation of 6, and mean difference of 13 among the three groups.
A total of 45 sound premolars extracted for orthodontic treatment (ethical code: IR.SBMU.RIDS.REC.1395.364) were collected and randomly divided into three groups of NaF, P. lentiscus extract, and deionized water by simple randomization method. Cracked, restored, carious or worn teeth were excluded. The teeth were immersed in 10% formalin for 24 hours. Next, they were stored in deionized water until the experiment. The tooth crowns were first cut at 2 mm below the cementoenamel junction and then cut mesiodistally into the buccal and lingual halves by a high-speed handpiece and a cylindrical diamond bur (008, Teeskavan, Hashtgerd, Alborz Province, Iran) under the water coolant. To access cervical dentin, the enamel surface of the buccal and lingual halves was sectioned parallel to the direction of the first section. The obtained specimens were polished with 400 to 1000-grit abrasive papers (silicon carbide, Starcke, Matador, Wasserfest, Germany). The buccal surface of dentin specimens was coated with one layer of nail varnish (Inlay Red Velvet Nail varnish, code 012, Iran) except for a window measuring 4 x 4 mm. The dentin specimens were then randomly assigned to three groups of 15. Next, they underwent the microhardness test by a Vickers hardness tester (Zwick Roell, Ulm, Germany) at three points under 200 N load for 10 seconds. To induce dentin lesions, the specimens were placed in a demineralizing solution at 37°C for 96 hours and then underwent the microhardness test again.
Conduction of pH cycling:
The specimens in 1000 ppm NaF, 10% alcoholic extract, and deionized water (negative control) groups underwent pH cycling for a total duration of 14 days.
Accordingly, the specimens were placed in a demineralizing solution for 4 hours and were then transferred to artificial saliva (remineralizing solution) for 20 hours. In the process of transfer between the demineralizing and remineralizing solutions, the specimens were treated with 1000 ppm NaF in the first group, 10% P. lentiscus in the second group, and deionized water in the third group twice each time for 2 minutes and were then rinsed with deionized water for 15 seconds. After the pH cycling, the microhardness was measured for the second time. The specimens were incubated at 37°C during the process [32].
SEM analysis:
The specimens were dried and sputter-coated with gold/palladium. Two specimens from each group underwent SEM analysis (FE-SEM TESCAN MIRA3, Czech Republic) after demineralization and after 14 days of treatment with the solutions. SEM micrographs were obtained from the surface
of each specimen at x2000 magnification, and the diameter of dentinal tubules was measured.
Statistical analysis:
Data were analyzed by repeated-measures ANOVA.
Results
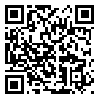
Table 1 indicates the mean microhardness values measured before and after demineralization and after 14 days of remineralization. Repeated-measures ANOVA showed no significant difference in microhardness of the groups before and after demineralization (P>0.05). However, after 14 days, the microhardness of the NaF group was significantly higher than that of the extract (P<0.001) and deionized water (P<0.001) groups, and the microhardness of the extract group was significantly higher than that of the deionized water group (P=0.004). Table 2 shows the mean difference and P values for the comparison of microhardness among the three groups at different time points. Repeated measures ANOVA showed the significant interaction effect of time of measurement and type of solution on microhardness (P<0.001).
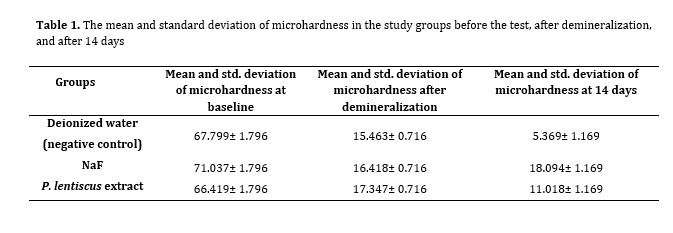
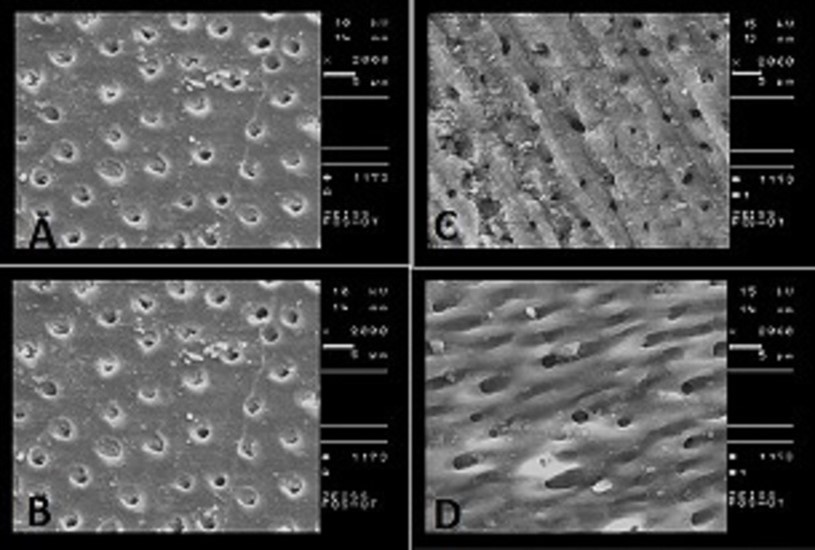
SEM assessment of dentin surface morphology of the two randomly selected specimens from each group indicated equal obstruction of dentinal tubules after demineralization in 10% extract and 1000 ppm NaF groups. After 14 days, the seal of dentinal tubules in 10% extract group was higher than that in 1000 ppm NaF group. Also, the smear layer formed on dentin was more homogenous in the extract group (Figures 1 and 2).
Table 1. The mean and standard deviation of microhardness in the study groups before the test, after demineralization, and after 14 days
Based on the results obtained in the present study, the effect of NaF (1000 ppm) was greater than P. lentiscus extract (10%) in the microhardness test after 14 days, but on the other hand, SEM analysis showed that the obstruction of dentinal tubules by the extract was more than that by the NaF.
Considering the economic conditions of Iran and attention to self-sufficiency in production of products with appropriate effectiveness, as well as attention to traditional and herbal medicine, the present study showed that P. lentiscus extract can be a suitable substance for treatment of DH.
Full-Text: (295 Views)
| Abstract
Background and Aim: This study aimed to assess the efficacy of Pistacia lentiscus (P. lentiscus) extract for dentin remineralization. Materials and Methods: This in vitro experimental study evaluated 45 extracted sound human premolars; pH cycling was performed to assess the effect of 10% P. lentiscus extract on dentin remineralization. The samples were randomly assigned to three groups of 1000 ppm sodium fluoride (NaF) solution, 10% P. lentiscus extract, and deionized water. To induce dentinal lesions, the teeth were immersed in a demineralizing solution at 37°C for 96 hours. The demineralized samples were then subjected to pH cycling for 14 days, and then underwent the Vickers microhardness test and scanning electron microscopic (SEM) assessment. Data were analyzed by repeated-measures ANOVA. Results: The mean microhardness in the NaF group was significantly higher than that in the extract and control groups after 14 days (P<0.05). SEM assessment after demineralization indicated tubular obstruction in the extract and NaF groups. However, after 14 days, the sealing of dentinal tubules in the extract group was greater than that in the NaF group. Conclusion: P. lentiscus extract can serve as a suitable organic compound for dentinal tubule occlusion as well as non-invasive and conservative treatment of dentin hypersensitivity (DH). Key Words: Dentin sensitivity; Dentin Desensitizing Agents; Pistacia lentiscus; Microscopy, Electron, Scanning |
Introduction
Dentin hypersensitivity (DH) is a common clinical complaint, affecting 4% to 74% of the population [1-5]. It refers to the generation of short sharp pain in exposed dentin due to chemical, thermal, and osmotic stimuli [6]. This pain cannot be attributed to any other pathology [7, 8]. DH can lead to physical and psychological problems and affect the quality of life and the oral hygiene practice of patients [9]. Absence of enamel or cementum coverage on dentin and exposure of dentinal tubules into the oral cavity are the main reasons for DH [10]. Scanning electron microscopic (SEM) assessments have indicated that the number of exposed dentinal tubules in teeth with DH is 8 times higher than that in normal teeth [11-13]. Root surface denuding following gingival recession due to aging, chronic periodontitis, periodontal surgery, incorrect tooth brushing technique, occlusal trauma, scaling and rootplaning, and pocket removal surgery leads to cementum exposure [14].
According to the Brannstrom’s theory, the movement of dentinal fluid in dentinal tubules leads to stimulation of baroreceptors and pain generation [15]. In general, the mechanism of action of desensitizing agents is based on the reduction of dentinal fluid flow or decreasing the activity of nerve ends in dentin by interfering with their electrical conduction [16]. In the recent decades, several desensitizing agents have been proposed for treatment of DH such as fluoride, arginine, and citrate buffers [17].
The main mechanism of action of fluoride is through the prevention or reduction of fluid movement in dentinal tubules by the deposition of calcium and phosphorous compounds such as calcium fluoride and fluorapatite. Preliminary studies have demonstrated optimal desensitizing efficacy of fluoride products. The Canadian Advisory Board on Dentin Hypersensitivity in 2003 suggested the use of fluoridated toothpastes as the first-line non-invasive treatment for DH. Also, the efficacy of NaF as a fluoride compound for this purpose has been extensively studied [18].
The application of medicinal herbs for medical purposes has a long history. Use of Pistacia lentiscus (P. lentiscus) for treatment of gastrointestinal diseases in the Middle Eastern countries dates back to 3000 years ago [16]. P. lentiscus has selective antibacterial properties against Porphyromonas gingivalis and Prevotella melaninogenica. It also exerts anti-plaque effects by inhibiting the proliferation of salivary bacteria. In the Iranian traditional medicine, P. lentiscus is used for
enhancement of wound healing, treatment of gastrointestinal conditions, and for gingival health [15] Mastic gum is the resin released from the stem and leaves of P. lentiscus, which has therapeutic effects for treatment of gastrointestinal problems such as stomachache, indigestion, and gastrointestinal inflammation [19-21]. Evidence shows that chewing of mastic gum inhibits the proliferation of salivary bacteria and formation of microbial plaque on tooth surfaces [22]. Use of mastic gum for 3 weeks decreases the Streptococcus mutans count of the saliva and may help in caries prevention [23]. It has been demonstrated that mastic gum can enhance the remineralization of caries-like lesions; enhancement of remineralization appears to be related to increased saliva flow and pH due to mastication [1,24]. Different species of Pistacia have different chemical constituents such as phenol groups and gallic acid [25-27]. Gallic acid is a natural phenol compound found in many herbs and foods with anti-oxidant, anti-mutagenic, and anti-cariogenic properties. Gallic acid can also increase enamel remineralization and prevent demineralization [28]. A complex of metal ions and gallic acid can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. Calcium, potassium, and magnesium are the most abundant minerals in the leaves and fruits of P. lentiscus [30].
Considering the presence of phenol groups (gallic acid), minerals, and metal ions in P. lentiscus extract, this study aimed to assess the efficacy of P. lentiscus extract for dentin remineralization and sealing of dentinal tubules. The null hypothesis was that the effects of 10% P. lentiscus extract and 1000 PPM sodium fluoride (NaF) solution on the hardness of dentin would be the same.
Materials and Methods
Preparation of 10% alcoholic extract of P. lentiscus:
For this purpose, 10 g of dried solid mastic gum was weighed by a digital scale (Sartorius, type TE 124 S, Göttingen, Germany) and ground in a mortar and pestle. The obtained powder was dissolved in 10 cc of pure acetone and well stirred for 30 minutes for complete dissolution. Next, 95% alcohol was added to reach a total volume of 100 cc. The obtained solution was stirred for 30 minutes to obtain a homogenous solution; the pH was adjusted to 6-6.5 by a pH meter (Sartorius, PB 11, Göttingen, Germany).
Preparation of 1000 ppm NaF solution:
For this purpose, 1 g of NaF salt was weighed by a digital scale (Sartorius, type TE 124 S, Göttingen, Germany) and added to 1 L of deionized water and stirred for complete dissolution.
The demineralizing solution had a pH of 4 to 4.5 with the following formulation: NaCl (2.9 g), CaCl2 (0.12 g), NaH2PO4 (0.13 g), NaN3 (5 cc), and acetic acid (1.5 cc).
The remineralizing solution (artificial saliva) had a pH of 6.5 to 7 with the following formulation: NaCl (2.9 g), CaCl2 (0.12 g), NaH2PO4 (0.13 g), and NaN3 (5 cc) [31].
Sample preparation:
The sample size was found to be 15 per group using the multiple comparisons feature of PASS software considering alpha=0.05, beta=0.1, standard deviation of 6, and mean difference of 13 among the three groups.
A total of 45 sound premolars extracted for orthodontic treatment (ethical code: IR.SBMU.RIDS.REC.1395.364) were collected and randomly divided into three groups of NaF, P. lentiscus extract, and deionized water by simple randomization method. Cracked, restored, carious or worn teeth were excluded. The teeth were immersed in 10% formalin for 24 hours. Next, they were stored in deionized water until the experiment. The tooth crowns were first cut at 2 mm below the cementoenamel junction and then cut mesiodistally into the buccal and lingual halves by a high-speed handpiece and a cylindrical diamond bur (008, Teeskavan, Hashtgerd, Alborz Province, Iran) under the water coolant. To access cervical dentin, the enamel surface of the buccal and lingual halves was sectioned parallel to the direction of the first section. The obtained specimens were polished with 400 to 1000-grit abrasive papers (silicon carbide, Starcke, Matador, Wasserfest, Germany). The buccal surface of dentin specimens was coated with one layer of nail varnish (Inlay Red Velvet Nail varnish, code 012, Iran) except for a window measuring 4 x 4 mm. The dentin specimens were then randomly assigned to three groups of 15. Next, they underwent the microhardness test by a Vickers hardness tester (Zwick Roell, Ulm, Germany) at three points under 200 N load for 10 seconds. To induce dentin lesions, the specimens were placed in a demineralizing solution at 37°C for 96 hours and then underwent the microhardness test again.
Conduction of pH cycling:
The specimens in 1000 ppm NaF, 10% alcoholic extract, and deionized water (negative control) groups underwent pH cycling for a total duration of 14 days.
Accordingly, the specimens were placed in a demineralizing solution for 4 hours and were then transferred to artificial saliva (remineralizing solution) for 20 hours. In the process of transfer between the demineralizing and remineralizing solutions, the specimens were treated with 1000 ppm NaF in the first group, 10% P. lentiscus in the second group, and deionized water in the third group twice each time for 2 minutes and were then rinsed with deionized water for 15 seconds. After the pH cycling, the microhardness was measured for the second time. The specimens were incubated at 37°C during the process [32].
SEM analysis:
The specimens were dried and sputter-coated with gold/palladium. Two specimens from each group underwent SEM analysis (FE-SEM TESCAN MIRA3, Czech Republic) after demineralization and after 14 days of treatment with the solutions. SEM micrographs were obtained from the surface
of each specimen at x2000 magnification, and the diameter of dentinal tubules was measured.
Statistical analysis:
Data were analyzed by repeated-measures ANOVA.
Results
Table 1 indicates the mean microhardness values measured before and after demineralization and after 14 days of remineralization. Repeated-measures ANOVA showed no significant difference in microhardness of the groups before and after demineralization (P>0.05). However, after 14 days, the microhardness of the NaF group was significantly higher than that of the extract (P<0.001) and deionized water (P<0.001) groups, and the microhardness of the extract group was significantly higher than that of the deionized water group (P=0.004). Table 2 shows the mean difference and P values for the comparison of microhardness among the three groups at different time points. Repeated measures ANOVA showed the significant interaction effect of time of measurement and type of solution on microhardness (P<0.001).
SEM assessment of dentin surface morphology of the two randomly selected specimens from each group indicated equal obstruction of dentinal tubules after demineralization in 10% extract and 1000 ppm NaF groups. After 14 days, the seal of dentinal tubules in 10% extract group was higher than that in 1000 ppm NaF group. Also, the smear layer formed on dentin was more homogenous in the extract group (Figures 1 and 2).
Table 1. The mean and standard deviation of microhardness in the study groups before the test, after demineralization, and after 14 days
{kind=link}
Table 2. Comparison of the microhardness of the three groups at different time points
Figure 1. SEM micrographs of the selected samples of 1000 ppm NaF group after demineralization (A, B) and after 14 days (C, D) at x2000 magnification
Figure 2. SEM micrographs of the selected samples of 10% P. lentiscus extract group after demineralization (A, B) and after 14 days (C, D) at x2000 magnification
Discussion
This study evaluated the microhardness and obstruction of dentinal tubules after the use of 10% P. lentiscus extract and 1000 ppm NaF. Calcium, potassium, and magnesium are the most abundant minerals in the leaves and fruits of P. lentiscus [33]. A complex of metal ions and gallic acid in P. lentiscus can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. In the present study, remineralization of demineralized dentin might have occurred through the continuous uptake of calcium, phosphate, and fluoride ions from the oral fluids by the demineralized tissue or by the provision of these ions by an external source such as the P. lentiscus extract [29,34].
According to the Vickers test results, after 14 days, the microhardness of the NaF group was significantly higher than that of the extract group, and the value in the extract group was significantly higher than that in the deionized water (control) group. Higher microhardness of the NaF group has been reported in other studies as well [35,36]. Xie et al. evaluated the effect of grape seed extract and 1000 ppm NaF on root dentin, and reported higher microhardness of the fluoride group than the control group at all depths of dentin, from 20 to 200 µm with no significant difference with the grape seed extract group. The effect of 1000 ppm NaF on dentin remineralization depends on the formation of calcium, phosphorous, and fluorapatite crystals in dentinal tubules [37]. Tang et al. evaluated the remineralization potential of grape seed extract enriched with proanthocyanidin for the demineralized dentin. After 14 days of remineralization, they found no significant difference in microhardness between 1000 ppm NaF and 15% grape seed extract groups. The Grape seed extract has high amounts of polyphenols such as hydroxyphenyl, which may react with the calcium ions present in the remineralizing solution, and lead to the growth of demineralized dentin crystals [36]. It appears that the effect of P. lentiscus extract on dentin remineralization agrees with the suggested theory regarding the effect of grape seed extract containing polyphenols. A complex of metal ions and gallic acid can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. Further studies are required to use different concentrations of P. lentiscus extract with different application times on dentin to more precisely assess the efficacy of this extract.
SEM assessment of dentin surface morphology by Ellingsen et al. in 1987 revealed the formation of a thick layer of globular NaF covering the dentinal tubules and uniform sealing of dentinal tubules by the NaF varnish [38]. In the present study, the extract obstructed the dentinal tubules more efficiently after 14 days compared with NaF. SEM assessment by Kunam et al. indicated that 2% NaF narrowed the lumen of dentinal tubules; however, it was unsuccessful in their complete obstruction. NaF reacts with the calcium in dentin and forms calcium fluoride crystals, which penetrate into dentinal tubules. Since these crystals have a small size, they cannot effectively obstruct the dentinal tubules [39]. Raafat et al. evaluated the efficacy of fluoride, ozone, and oxalate compounds for sealing of dentinal tubules. They reported that fluoride could not successfully seal the tubules; however, its efficacy improved when combined with ozone [40]. The main mechanism of action of NaF in the sealing of dentinal tubules has not yet been clearly understood. However, it appears that the calcium ions released from dentin due to the effect of acidic compounds are present in the dentinal fluid, and react with NaF and form calcium fluoride crystals, which deposit in dentinal tubules [41,42].
Moreover, it appears that calcium fluoride crystals do not adhere to dentinal tubules and due to their small size, they cannot tolerate environmental stress and degrade over time [41]. Thus, multiple applications of fluoride are recommended to enhance the seal of dentinal tubules [43]. Considering the significance of using medicinal herbs with fewer side effects than synthetic chemical agents, and supporting the national pharmaceutical products, it appears that P. lentiscus can serve as a suitable material for treatment of DH, and can overcome the problems related to
incomplete sealing of dentinal tubules by the action of fluoride.
Conclusion
{kind=link}
Figure 1. SEM micrographs of the selected samples of 1000 ppm NaF group after demineralization (A, B) and after 14 days (C, D) at x2000 magnification
{kind=link}
Figure 2. SEM micrographs of the selected samples of 10% P. lentiscus extract group after demineralization (A, B) and after 14 days (C, D) at x2000 magnification
{kind=link}
Discussion
This study evaluated the microhardness and obstruction of dentinal tubules after the use of 10% P. lentiscus extract and 1000 ppm NaF. Calcium, potassium, and magnesium are the most abundant minerals in the leaves and fruits of P. lentiscus [33]. A complex of metal ions and gallic acid in P. lentiscus can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. In the present study, remineralization of demineralized dentin might have occurred through the continuous uptake of calcium, phosphate, and fluoride ions from the oral fluids by the demineralized tissue or by the provision of these ions by an external source such as the P. lentiscus extract [29,34].
According to the Vickers test results, after 14 days, the microhardness of the NaF group was significantly higher than that of the extract group, and the value in the extract group was significantly higher than that in the deionized water (control) group. Higher microhardness of the NaF group has been reported in other studies as well [35,36]. Xie et al. evaluated the effect of grape seed extract and 1000 ppm NaF on root dentin, and reported higher microhardness of the fluoride group than the control group at all depths of dentin, from 20 to 200 µm with no significant difference with the grape seed extract group. The effect of 1000 ppm NaF on dentin remineralization depends on the formation of calcium, phosphorous, and fluorapatite crystals in dentinal tubules [37]. Tang et al. evaluated the remineralization potential of grape seed extract enriched with proanthocyanidin for the demineralized dentin. After 14 days of remineralization, they found no significant difference in microhardness between 1000 ppm NaF and 15% grape seed extract groups. The Grape seed extract has high amounts of polyphenols such as hydroxyphenyl, which may react with the calcium ions present in the remineralizing solution, and lead to the growth of demineralized dentin crystals [36]. It appears that the effect of P. lentiscus extract on dentin remineralization agrees with the suggested theory regarding the effect of grape seed extract containing polyphenols. A complex of metal ions and gallic acid can enhance the remineralization of hydroxyapatite, which is the main mechanism of cross-linking and formation of new hydroxyapatite cores on the surface of dentinal tubules [29]. Further studies are required to use different concentrations of P. lentiscus extract with different application times on dentin to more precisely assess the efficacy of this extract.
SEM assessment of dentin surface morphology by Ellingsen et al. in 1987 revealed the formation of a thick layer of globular NaF covering the dentinal tubules and uniform sealing of dentinal tubules by the NaF varnish [38]. In the present study, the extract obstructed the dentinal tubules more efficiently after 14 days compared with NaF. SEM assessment by Kunam et al. indicated that 2% NaF narrowed the lumen of dentinal tubules; however, it was unsuccessful in their complete obstruction. NaF reacts with the calcium in dentin and forms calcium fluoride crystals, which penetrate into dentinal tubules. Since these crystals have a small size, they cannot effectively obstruct the dentinal tubules [39]. Raafat et al. evaluated the efficacy of fluoride, ozone, and oxalate compounds for sealing of dentinal tubules. They reported that fluoride could not successfully seal the tubules; however, its efficacy improved when combined with ozone [40]. The main mechanism of action of NaF in the sealing of dentinal tubules has not yet been clearly understood. However, it appears that the calcium ions released from dentin due to the effect of acidic compounds are present in the dentinal fluid, and react with NaF and form calcium fluoride crystals, which deposit in dentinal tubules [41,42].
Moreover, it appears that calcium fluoride crystals do not adhere to dentinal tubules and due to their small size, they cannot tolerate environmental stress and degrade over time [41]. Thus, multiple applications of fluoride are recommended to enhance the seal of dentinal tubules [43]. Considering the significance of using medicinal herbs with fewer side effects than synthetic chemical agents, and supporting the national pharmaceutical products, it appears that P. lentiscus can serve as a suitable material for treatment of DH, and can overcome the problems related to
incomplete sealing of dentinal tubules by the action of fluoride.
Conclusion
Based on the results obtained in the present study, the effect of NaF (1000 ppm) was greater than P. lentiscus extract (10%) in the microhardness test after 14 days, but on the other hand, SEM analysis showed that the obstruction of dentinal tubules by the extract was more than that by the NaF.
Considering the economic conditions of Iran and attention to self-sufficiency in production of products with appropriate effectiveness, as well as attention to traditional and herbal medicine, the present study showed that P. lentiscus extract can be a suitable substance for treatment of DH.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Rees JS, Jin LJ, Lam S, Kudanowska I, Vowles R. The prevalence of dentine hypersensitivity in a hospital clinic popu-lation in Hong Kong. J Dent. 2003 Sep;31(7):453-61. [DOI:10.1016/S0300-5712(03)00092-7] [PMID]
2. Flynn J, Galloway R, Orchardson R. The incidence of ' hypersensitive' teeth in the West of Scotland. J Dent. 1985 Sep;13(3):230-6. [DOI:10.1016/0300-5712(85)90004-1] [PMID]
3. Fischer C, Fischer RG, Wennberg A. Prevalence and distribution of cervical dentine hypersensitivity in a population in Rio de Janeiro, Brazil. J Dent. 1992 Oct;20(5): 272-6. [DOI:10.1016/0300-5712(92)90043-C] [PMID]
4. Irwin CR, McCusker P. Prevalence of dentine hypersensitivity in a general dental population. J Ir Dent Assoc. 1997;43(1):7-9.
5. Taani DQ, Awartani F. Prevalence and distribution of dentin hypersensitivity and plaque in a dental hospital population. Quintessence Int. 2001 May;32(5):372-6.
6. Durmaz G, Gökmen V. Changes in oxidative stability, antioxidant capacity and phytochemical composition of Pistacia terebinthus oil with roasting. Food Chem. 2011 Sep 15;128(2):410-4. [DOI:10.1016/j.foodchem.2011.03.044] [PMID]
7. Asnaashari M, Moeini M. Effectiveness of lasers in the treat-ment of dentin hypersensitivity. J Lasers Med Sci. 2013 Win-ter;4(1):1-7.
8. Bartold PM. Dentinal hypersensitivity: a review. Aust Dent J. 2006 Sep;51(3):212-8; quiz 276. [DOI:10.1111/j.1834-7819.2006.tb00431.x] [PMID]
9. Mozaffarian V. Trees and Shrubs of Iran. Iran: Farhang Moaser Publishers;2005.1003 p.
10. Trushkowsky RD, Oquendo A. Treatment of dentin hypersensitivity. Dent Clin North Am. 2011 Jul;55(3):599-608, x. [DOI:10.1016/j.cden.2011.02.013] [PMID]
11. Mozaffarian V. A Dictionary of Iranian Plant Names: Latin - English - Persian. Tehran:Farhang Mo'aser;1966.
12. Tsokou A, Georgopoulou K, Melliou E, Magiatis P, Tsitsa E. Composition and enantiomeric analysis of the essential oil of the fruits and the leaves of Pistacia vera from Greece. Molecules. 2007 Jun 30;12(6):1233-9. [DOI:10.3390/12061233] [PMID] [PMCID]
13. Benamar H, Rached W, Derdour A, Marouf A. Screening of Algerian medicinal plants for acetylcholinesterase inhibitory activity. Journal of Biological Sciences. 2010;10(1):1-9. [DOI:10.3923/jbs.2010.1.9]
14. Drisko CH. Dentine hypersensitivity - dental hygiene and periodontal considerations. International Dental Journal. 2002;52(S5P2):385-93. [DOI:10.1002/j.1875-595X.2002.tb00938.x]
15. Bozorgi M, Memariani Z, Mobli M, Salehi Surmaghi MH, Shams-Ardekani MR, Rahimi R. Five Pistacia spe-cies (P. vera, P. atlantica, P. terebinthus, P. khinjuk, and P. len-tiscus): a review of their traditional uses, phytochemistry, and pharmacology. Scientific World Journal. 2013 Dec 15; 2013:219815. [DOI:10.1155/2013/219815] [PMID] [PMCID]
16. Dimas K, Hatziantoniou S, Wyche JH, Pantazis P. A mastic gum extract induces suppression of growth of human colorectal tumor xenografts in immunodeficient mice. In Vivo. 2009 Jan-Feb;23(1):63-8.
17. Arrais CA, Micheloni CD, Giannini M, Chan DC. Occluding effect of dentifrices on dentinal tubules. J Dent. 2003 Nov; 31 (8):577-84. [DOI:10.1016/S0300-5712(03)00115-5] [PMID]
18. Addy M. Etiology and clinical implications of dentine hyper-sensitivity. Dent Clin North Am. 1990 Jul;34(3):503-14. [DOI:10.1016/S0011-8532(22)01131-4] [PMID]
19. Derwich E, Manar A, Benziane Z, Boukir A. GC/MS analysis and in vitro antibacterial activity of the essential oil isolated from leaf of Pistacia lentiscus growing in Morocoo. World Appl Sci J. 2010;8:1267-76.
20. Giaginis C, Theocharis S. Current evidence on the anticancer potential of Chios mastic gum. Nutr Cancer. 2011 Nov;63(8):1174-84. [DOI:10.1080/01635581.2011.607546] [PMID]
21. Mahmoudi M, Ebrahimzadeh MA, Nabavi SF, Hafezi S, Nabavi SM, Eslami Sh. Antiinflammatory and antioxidant activities of gum mastic. Eur Rev Med Pharmacol Sci. 2010 Sep;14(9):765-9.
22. Takahashi K, Fukazawa M, Motohira H, Ochiai K, Nishikawa H, Miyata T. A pilot study on antiplaque effects of mastic chewing gum in the oral cavity. J Periodontol. 2003 Apr;74(4):501-5. [DOI:10.1902/jop.2003.74.4.501] [PMID]
23. Biria M, Eslami G, Taghipour E, Akbarzadeh Baghban A. Ef-fects of Three Mastic Gums on the Number of Mutans Strepto-cocci, Lactobacilli and PH of the Saliva. J Dent (Tehran). 2014 Nov;11(6):672-9.
24. Biria M, Malekafzali B, Kamel V. Comparison of the Effect of Xylitol Gum-and Masticchewing on the Remineralization Rate of Caries-like Lesions. Frontiers in Dentistry. 2009:6-10.
25. Romani A, Pinelli P, Galardi C, Mulinacci N, Tattini M. Identi-fication and quantification of galloyl derivatives, flavonoid glycosides and anthocyanins in leaves of Pistacia len-tiscus L. Phytochem Anal. 2002 Mar-Apr;13(2):79-86. [DOI:10.1002/pca.627] [PMID]
26. Bhouri W, Derbel S, Skandrani I, Boubaker J, Bouhlel I, Sghaier MB, Kilani S, Mariotte AM, Dijoux-Franca MG, Ghedira K, Chekir-Ghedira L. Study of genotoxic, antigenotoxic and antioxidant activities of the digallic acid iso-lated from Pistacia lentiscus fruits. Toxicol In Vitro. 2010 Mar;24(2):509-15. [DOI:10.1016/j.tiv.2009.06.024] [PMID]
27. Abdelwahed A, Bouhlel I, Skandrani I, Valenti K, Kadri M, Guiraud P, Steiman R, Mariotte AM, Ghedira K, Laporte F, Dijoux-Franca MG, Chekir-Ghedira L. Study of antimutagenic and anti-oxidant activities of gallic acid and 1,2,3,4,6-pentagalloylglucose from Pistacia lentiscus. Confirmation by microarray expression profiling. Chem Biol Interact. 2007 Jan 5;165(1):1-13. [DOI:10.1016/j.cbi.2006.10.003] [PMID]
28. Huang XL, Liu MD, Li JY, Zhou XD, ten Cate JM. Chemical com-position of Galla chinensis extract and the effect of its main com-ponent(s) on the prevention of enamel demineralization in vitro. Int J Oral Sci. 2012 Sep;4(3):146-51. [DOI:10.1038/ijos.2012.44] [PMID] [PMCID]
29. Prajatelistia E, Ju SW, Sanandiya ND, Jun SH, Ahn JS, Hwang DS. Tunicate-Inspired Gallic Acid/Metal Ion Complex for Instant and Efficient Treatment of Dentin Hypersensitivity.Adv Healthc Mater. 2016 Apr 20;5(8):919-27. [DOI:10.1002/adhm.201500878] [PMID]
30. Aouinti F, Zidane H, Tahri M, Wathelet JP, El Bachiri A. Chem-ical composition, mineral contents and antioxidant activity of fruits of Pistacia lentiscus L. from Eastern Morocco. J Mater Environ Sci. 2014;5(1):199-206.
31. Moslemi M, Mahmodabadi M, Bastani Z, Sadrabad ZK, Faghihi FS, Shadkar Z. Evaluation of Remineralization Effect of Various Toothpastes on White Spot Enamel Lesions: An in Vitro Study. American Journal of Pediatrics. 2022;8(2):91-7. [DOI:10.11648/j.ajp.20220802.17]
32. ten Cate JM, Duijsters PP. Alternating demineralization and remineralization of artificial enamel lesions. Caries Res. 1982;16(3):201-10. [DOI:10.1159/000260599] [PMID]
33. Aouinti F, Zidane H, Tahri M, Wathelet JP, El Bachiri A. Chem-ical composition, mineral contents and antioxidant activity of fruits of Pistacia lentiscus L. from Eastern Morocco. J. Mater. Environ. Sci. 5 (1) (2014) 199-206.
34. Arends J, ten Bosch JJ. Demineralization and remineraliza-tion evaluation techniques. J Dent Res. 1992 Apr;71 Spec No:924-8. [DOI:10.1177/002203459207100S27] [PMID]
35. Jose P, Sanjeev K, Sekar M. Effect of Green and White Tea Pretreatment on Remineralization of Demineralized Dentin by CPP-ACFP-An Invitro Microhardness Analysis. J Clin Diagn Res. 2016 Apr;10(4):ZC85-9. [DOI:10.7860/JCDR/2016/16038.7674] [PMID] [PMCID]
36. Tang CF, Fang M, Liu RR, Dou Q, Chai ZG, Xiao YH, Chen JH. The role of grape seed extract in the remineralization of demin-eralized dentine: micromorphological and physical analyses. Arch Oral Biol. 2013 Dec;58(12):1769-76. [DOI:10.1016/j.archoralbio.2013.09.007] [PMID]
37. Xie Q, Bedran-Russo AK, Wu CD. In vitro remineralization effects of grape seed extract on artificial root caries. J Dent. 2008 Nov;36(11):900-6. [DOI:10.1016/j.jdent.2008.07.011] [PMID] [PMCID]
38. Ellingsen JE, Rölla G. Treatment of dentin with stannous fluoride--SEM and electron microprobe study. Scand J Dent Res. 1987 Aug;95(4):281-6. [DOI:10.1111/j.1600-0722.1987.tb01843.x] [PMID]
39. Kunam D, Manimaran S, Sampath V, Sekar M. Evaluation of dentinal tubule occlusion and depth of penetration of nano-hydroxyapatite derived from chicken eggshell powder with and without addition of sodium fluoride: An in vitro study. J Con-serv Dent. 2016 May-Jun;19(3):239-44. [DOI:10.4103/0972-0707.181940] [PMID] [PMCID]
40. Raafat Abdelaziz R, Mosallam RS, Yousry MM. Tubular oc-clusion of simulated hypersensitive dentin by the combined use of ozone and desensitizing agents. Acta Odontol Scand. 2011 Nov;69(6):395-400. [DOI:10.3109/00016357.2011.572290] [PMID]
41. Ipci SD, Cakar G, Kuru B, Yilmaz S. Clinical evaluation of la-sers and sodium fluoride gel in the treatment of dentine hyper-sensitivity. Photomed Laser Surg. 2009 Feb;27(1):85-91. [DOI:10.1089/pho.2008.2263] [PMID]
42. Arrais CA, Chan DC, Giannini M. Effects of desensitizing agents on dentinal tubule occlusion. J Appl Oral Sci. 2004 Jun;12(2):144-8. [DOI:10.1590/S1678-77572004000200012] [PMID]
43. Corona SA, Nascimento TN, Catirse AB, Lizarelli RF, Dinelli W, Palma-Dibb RG. Clinical evaluation of low-level laser therapy and fluoride varnish for treating cervical dentinal hypersensitivity. J Oral Rehabil. 2003 Dec; 30(12): 1183-9. [DOI:10.1111/j.1365-2842.2003.01185.x] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
