Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 3 (9-2024)
J Res Dent Maxillofac Sci 2024, 9(3): 204-210 |
Back to browse issues page


Ethics code: IR.IAU.DENTAL.REC.1399.035
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadrimanesh R, Aref P, Tavasoli-Hojjati S, Haghighat S. Esthetic Reconstruction of Primary Molars with Direct Composite Crown: One-Year Report of Five Cases. J Res Dent Maxillofac Sci 2024; 9 (3) :204-210
URL: http://jrdms.dentaliau.ac.ir/article-1-438-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-438-en.html
Esthetic Reconstruction of Primary Molars with Direct Composite Crown: One-Year Report of Five Cases



1- Private Dental Practice, Tehran, Iran.
2- Department of Pediatric Dentistry, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran. ,parissa234@yahoo.com
3- Department of Pediatric Dentistry, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran.
2- Department of Pediatric Dentistry, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran. ,
3- Department of Pediatric Dentistry, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran.
Full-Text [PDF 408 kb]
(1339 Downloads)
| Abstract (HTML) (3114 Views)
Full-Text: (1186 Views)
Abstract
Background and Aim: Dissatisfaction of parents with the appearance of conventional stainless-steel crowns (SSCs) has led the pedodontists to choose alternative esthetic restorations such as zirconia crowns.
Case Presentation: In this report, a new approach for fabrication of direct composite crowns for primary molars was described using dual-cure core build-up composite material in five patients with one-year follow-up.
Conclusion: Direct composite crown appears to be a suitable esthetic restoration for pulpotomized primary molars in cooperative patients with acceptable oral hygiene.
Keywords: Child; Composite Resins; Crowns; Esthetics, Dental; Molar
Introduction
Case Presentation: In this report, a new approach for fabrication of direct composite crowns for primary molars was described using dual-cure core build-up composite material in five patients with one-year follow-up.
Conclusion: Direct composite crown appears to be a suitable esthetic restoration for pulpotomized primary molars in cooperative patients with acceptable oral hygiene.
Keywords: Child; Composite Resins; Crowns; Esthetics, Dental; Molar
Introduction
Dissatisfaction of parents with the unesthetic appearance of stainless-steel crowns (SSCs) is a challenge in pediatric dentistry [1-3]. SSCs are highly durable, and are the most commonly used type of crown for primary posterior teeth. However, unesthetic appearance is their main drawback [4]. Dissatisfaction of parents with the unesthetic appearance of SSCs led dental clinicians to search for alternative esthetically pleasant restorations [5]. Pre-veneered SSCs, resin-bonded strip crowns, and prefabricated zirconia crowns are among the alternative crowns introduced to the market to meet the esthetic demands of parents [6]. Zirconia crowns met the esthetic requirements to a great extent; however, they did not gain increasing popularity due to the need for extensive tooth preparation, inability to adjust the crown margins, and high cost [2,3,7]. Pre-veneered metal crowns had optimal esthetics; however, inability to adjust the crown margins, and chipping of the veneering over time were among their main drawbacks [3,8]. The long-term success of composite resin application along with a strip crown for full coverage of primary anterior teeth has been well documented [9,10]. However, this method was not widely accepted by dental clinicians for posterior teeth due to high technical sensitivity and difficult application [6,11]. Also, no clinical study is available regarding its true clinical efficacy. Composite resin restorations have long been successfully used for reconstruction of permanent posterior teeth. However, application of composite resin for multi-surface restoration of primary posterior teeth has not shown satisfactory results due to the occurrence of secondary caries [12,13]. Also, due to the risk of fracture of undermined tooth wall in multi-surface restorations, particularly after pulp therapy, such teeth should be preferably crowned [14]. A previous study reported successful results of indirect composite crown of primary molars with multi-surface caries after pulpotomy at the 1-year follow-up. They suggested this modality for cases requiring esthetic restorations. However, the need for laboratory fabrication of crowns is a limitation of this modality for esthetic reconstruction of primary teeth [15].
Dual-cure core build-up composite resins are used for core build-up after endodontic treatment in permanent teeth. Also, evidence shows that their application for direct restoration increases the fracture resistance of teeth [16]. This type of composite has increased percentage of fillers, which confers greater strength and decreases shrinkage. Also, such composites have increased fracture resistance due to improved flexural modulus [17,18]. These composite resins are available in flowable consistency, which enhances their application and results in their improved adaptation to surfaces [19]. Their dual-cure polymerization mode is another added advantage, which eliminates the need for incremental application of composite, and the composite resin can be applied as bulk in one step to save time [20]. Due to such favorable properties, such composite resins are optimal for use in pediatric dentistry. This study aimed to introduce a novel approach for complete crown coverage of primary posterior teeth by using a dual-cure core build-up composite resin. This restoration has optimal durability without the unesthetic appearance of SSCs.
Case Presentation
Dual-cure core build-up composite resins are used for core build-up after endodontic treatment in permanent teeth. Also, evidence shows that their application for direct restoration increases the fracture resistance of teeth [16]. This type of composite has increased percentage of fillers, which confers greater strength and decreases shrinkage. Also, such composites have increased fracture resistance due to improved flexural modulus [17,18]. These composite resins are available in flowable consistency, which enhances their application and results in their improved adaptation to surfaces [19]. Their dual-cure polymerization mode is another added advantage, which eliminates the need for incremental application of composite, and the composite resin can be applied as bulk in one step to save time [20]. Due to such favorable properties, such composite resins are optimal for use in pediatric dentistry. This study aimed to introduce a novel approach for complete crown coverage of primary posterior teeth by using a dual-cure core build-up composite resin. This restoration has optimal durability without the unesthetic appearance of SSCs.
Case Presentation
Five pediatric patients were selected among those presenting to the Pediatric Dentistry Department of School of Dentistry of Islamic Azad University, Tehran who required pulpotomy and complete coverage of their primary first molars. The patients had no systemic disease or bruxism. The selected teeth had to have sound buccal and lingual walls. Thus, pulpotomized teeth with mesio-occluso-distal, disto-occlusal, and mesio-occlusal cavities were selected. The gingival floor had to be located supra-gingivally, and the residual walls had to be free from caries, and supported by sound dentin. After caries removal, the walls had to have a minimum of 2 mm residual thickness. Also, the teeth had no caries in the buccal and lingual walls. The patients had to be cooperative (Frankl's behavior rating scale 3 or 4) and were between 4-8 years of age. They had good oral hygiene (oral hygiene index < 3) as well. The study was approved by the ethics committee of School of Dentistry of Islamic Azad University, Tehran (IR.IAU.DENTAL.REC.1399.035). The treatment was started after obtaining written informed consent from the parents.
Primary restoration:
After pulpotomy, Zonalin (Golchay, Iran) was applied in the pulp chamber with 2 mm thickness, and a 1-mm glass ionomer lining (Willmann & Pein, Germany) was applied over it to prevent the adverse effect of Zonalin on composite resin [21]. Next, the internal walls of the cavity were cleaned such that the sound dentin was visible. A matrix band was applied around the tooth with a matrix holder, and the internal cavity walls were etched with 37% phosphoric acid gel for 20 seconds. Care was taken not to over-etch the glass-ionomer. The tooth was then rinsed with water for 20 seconds and dried with gentle air spray [22]. Two layers of Single Bond (3M ESPE, USA) were then applied on the tooth, dried with gentle air spray for 10 seconds, and cured for 20 seconds. Auto-mix dual-cure core build-up composite (Rebilda DC, VOCO GmbH, Germany) was injected into the cavity to the level of the occlusal surface, and after chemical curing for 5 minutes, light curing was performed for 20 seconds [23] (Figure 1).
Figure 1. Schematic view of the tooth after primary restoration
Tooth preparation:
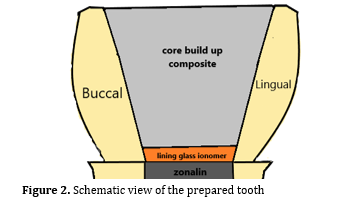
In the next step, the tooth received standard SSC preparation. The occlusal surface was prepared such that the respective tooth had 1.5 mm distance from the opposing tooth in occlusion. Also, adequate interproximal distance was ensured by passing the tip of an explorer through the interproximal space. After selecting the proper-size SSC, and its correct seating and adaptation with the tooth, a putty-wash impression was made from the tooth along with SSC. Next, the SSC was removed from the tooth. To achieve optimal composite thickness supra-gingivally, the sound walls were prepared with fissure bur (#847-010, Jota, Switzerland) by 0.5 mm according to the tooth contour to obtain a shoulder finish-line at the tooth periphery [24] (Figure 2).
In case of gingival bleeding, Access Edge (Centrix, USA) was injected into the gingival sulcus around the tooth for isolation of the area. For this purpose, it was first injected into the gingival sulcus by the respective gun, and the patient was asked to bite on the GingiCap (spongy cap placed on the tooth) for 2 minutes. Next, the GingiCap was removed, and the material was rinsed off with water spray. It is a kaolin clay-based material that retracts the gingiva. It also contains 15% aluminum chloride to induce hemostasis [25]. The area was isolated by placing cotton rolls in the buccal and lingual sulcus. Also, a subgingival retraction cord size 00 (Coltene/Whaledent AG, Switzerland) was packed in the gingival sulcus [26,27]. To protect the adjacent teeth during etching, they were protected with Teflon tape.
Figure 2. Schematic view of the prepared tooth
Final restoration:
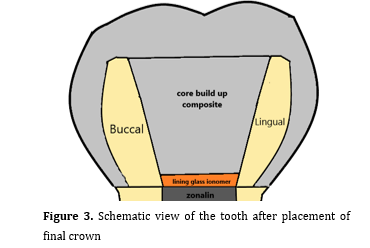
The tooth was etched with 37% phosphoric acid gel for 30 seconds. The etchant was rinsed with water for 20 seconds, and the tooth was dried with air spray. Two layers of adhesive (Single Bond Universal, 3M ESPE) were applied on the tooth, and dried with gentle air pressure for 10 seconds. Light curing was performed for 20 seconds using a curing unit (Woodpecker, China) with 1000 mW/cm2 light intensity. Automix dual-cure core build-up composite (Rebilda DC, VOCO GmbH) was applied into the tray at the site of the respective tooth, and the tray was placed in the oral cavity immediately after removing the cotton rolls, and held in place for 5 minutes with gentle pressure to allow completion of chemical curing. Next, the tray was removed and composite was cured from the buccal, lingual and occlusal surfaces, each for 20 seconds. The subgingival cord was removed, and the restoration margins were evaluated to ensure absence of excess composite. Next, the occlusion was checked by a copying paper. The contact area was checked by a dental floss, and the composite restoration was finished and polished (Figure 3). Finally, one layer of low-viscosity polishing liquid (Biscover LV, Bisco, Schaumburg, IL, USA) was applied on the crown. For this purpose, composite was etched for 15 seconds and rinsed. Next, a thin layer of liquid was applied on the composite, and after 15 seconds, it was light-cured for 30 seconds (Figure 4) [28,29]. To assess the final crown for integrity and absence of overhang, a bitewing radiograph was obtained from the tooth (Figure 5).
Figure 3. Schematic view of the tooth after placement of final crown
Figure 4. Clinical view of a maxillary first molar immediately after crowning
Figure 5. Bitewing radiograph showing a maxillary primary first molar with a composite crown
Follow-up:
The patients were followed-up for 3, 6, 9, and 12 months for evaluation of the crowns. In the recall sessions, the following parameters were evaluated according to the modified United States Public Health criteria [30]:
Primary restoration:
After pulpotomy, Zonalin (Golchay, Iran) was applied in the pulp chamber with 2 mm thickness, and a 1-mm glass ionomer lining (Willmann & Pein, Germany) was applied over it to prevent the adverse effect of Zonalin on composite resin [21]. Next, the internal walls of the cavity were cleaned such that the sound dentin was visible. A matrix band was applied around the tooth with a matrix holder, and the internal cavity walls were etched with 37% phosphoric acid gel for 20 seconds. Care was taken not to over-etch the glass-ionomer. The tooth was then rinsed with water for 20 seconds and dried with gentle air spray [22]. Two layers of Single Bond (3M ESPE, USA) were then applied on the tooth, dried with gentle air spray for 10 seconds, and cured for 20 seconds. Auto-mix dual-cure core build-up composite (Rebilda DC, VOCO GmbH, Germany) was injected into the cavity to the level of the occlusal surface, and after chemical curing for 5 minutes, light curing was performed for 20 seconds [23] (Figure 1).
Figure 1. Schematic view of the tooth after primary restoration
{kind=link}
Tooth preparation:
In the next step, the tooth received standard SSC preparation. The occlusal surface was prepared such that the respective tooth had 1.5 mm distance from the opposing tooth in occlusion. Also, adequate interproximal distance was ensured by passing the tip of an explorer through the interproximal space. After selecting the proper-size SSC, and its correct seating and adaptation with the tooth, a putty-wash impression was made from the tooth along with SSC. Next, the SSC was removed from the tooth. To achieve optimal composite thickness supra-gingivally, the sound walls were prepared with fissure bur (#847-010, Jota, Switzerland) by 0.5 mm according to the tooth contour to obtain a shoulder finish-line at the tooth periphery [24] (Figure 2).
In case of gingival bleeding, Access Edge (Centrix, USA) was injected into the gingival sulcus around the tooth for isolation of the area. For this purpose, it was first injected into the gingival sulcus by the respective gun, and the patient was asked to bite on the GingiCap (spongy cap placed on the tooth) for 2 minutes. Next, the GingiCap was removed, and the material was rinsed off with water spray. It is a kaolin clay-based material that retracts the gingiva. It also contains 15% aluminum chloride to induce hemostasis [25]. The area was isolated by placing cotton rolls in the buccal and lingual sulcus. Also, a subgingival retraction cord size 00 (Coltene/Whaledent AG, Switzerland) was packed in the gingival sulcus [26,27]. To protect the adjacent teeth during etching, they were protected with Teflon tape.
Figure 2. Schematic view of the prepared tooth
{kind=link}
Final restoration:
The tooth was etched with 37% phosphoric acid gel for 30 seconds. The etchant was rinsed with water for 20 seconds, and the tooth was dried with air spray. Two layers of adhesive (Single Bond Universal, 3M ESPE) were applied on the tooth, and dried with gentle air pressure for 10 seconds. Light curing was performed for 20 seconds using a curing unit (Woodpecker, China) with 1000 mW/cm2 light intensity. Automix dual-cure core build-up composite (Rebilda DC, VOCO GmbH) was applied into the tray at the site of the respective tooth, and the tray was placed in the oral cavity immediately after removing the cotton rolls, and held in place for 5 minutes with gentle pressure to allow completion of chemical curing. Next, the tray was removed and composite was cured from the buccal, lingual and occlusal surfaces, each for 20 seconds. The subgingival cord was removed, and the restoration margins were evaluated to ensure absence of excess composite. Next, the occlusion was checked by a copying paper. The contact area was checked by a dental floss, and the composite restoration was finished and polished (Figure 3). Finally, one layer of low-viscosity polishing liquid (Biscover LV, Bisco, Schaumburg, IL, USA) was applied on the crown. For this purpose, composite was etched for 15 seconds and rinsed. Next, a thin layer of liquid was applied on the composite, and after 15 seconds, it was light-cured for 30 seconds (Figure 4) [28,29]. To assess the final crown for integrity and absence of overhang, a bitewing radiograph was obtained from the tooth (Figure 5).
Figure 3. Schematic view of the tooth after placement of final crown
{kind=link}
Figure 4. Clinical view of a maxillary first molar immediately after crowning
{kind=link}
Figure 5. Bitewing radiograph showing a maxillary primary first molar with a composite crown
{kind=link}
Follow-up:
The patients were followed-up for 3, 6, 9, and 12 months for evaluation of the crowns. In the recall sessions, the following parameters were evaluated according to the modified United States Public Health criteria [30]:
- Assessment of gingival health by evaluation of bleeding on probing
- Assessment of secondary caries by bite-wing radiography
- Assessment of tooth fracture by clinical inspection and examination with a dental explorer
- Assessment of fracture, discoloration, integrity, and marginal adaptation of crown by visual inspection and clinical examination with a dental explorer [30].
Also, the patients received oral hygiene instructions, and underwent fluoride therapy at each recall session. Restoration loss, poor marginal adaptation, secondary caries, restoration discoloration, and periodontal problems did not occur in any patient during the follow-up period.
Discussion
Discussion
This study described a new approach for complete coronal reconstruction of primary teeth with a dual-cure core build-up composite resin. According to the guidelines of the American Association of Pediatric Dentistry, SSCs are recommended for restoration of primary teeth to increase their fracture resistance and success rate of pulp therapy [31]. Considering the high prevalence of early childhood caries in primary teeth [32], a high number of primary teeth require complete crown coverage after pulp therapy [33]. However, many parents are dissatisfied with the unesthetic appearance of SSCs [34], indicating the need for a more esthetic replacement for esthetically important zones. A dual-cure core build-up composite resin (Rebilda DC, VOCO GmbH) was used to fabricate direct composite crowns in the present study. This composite is suitable for the fabrication of composite crowns in children due to optimal properties. Dual-cure core build-up composite resins have higher filler content than conventional composites, which increases their fracture resistance [17]. They are dual-cure and are chemically cured in hard-to-reach areas for light curing [18]. Thus, when the tray containing composite resin is placed over the prepared tooth, primary setting occurs without requiring light. Such composite resins are flowable and auto-mix. Auto-mixing minimizes the risk of void formation while flowability ensures adequate adaptation of composite in the tray with the tooth [35].
Previous studies demonstrated that multi-surface restorations were not successful in primary teeth [36,37]. Pires et al, [38] in a systematic review and meta-analysis in 2018 compared the bond strength of primary and permanent teeth. They acknowledged the differences between the primary and permanent enamel and dentin, which are responsible for the different bond strength values of composite to primary and permanent teeth. The enamel in primary teeth is thin, and primary dentin has lower mineral content. Also, due to high density of dentinal tubules in primary teeth, the amount of available inter-tubular dentin for bonding is lower. All these factors are responsible for lower bond strength of composite to primary teeth, compared with permanent teeth [39]. However, the bond strength of composite to primary and permanent enamel has been reported to be comparable [40-42]. In the present study, direct composite crown had a larger bonding interface with enamel compared with multi-surface restorations, which can aid in clinical success and durability of restorations.
In the present study, the primary first molars of 5 patients were restored with direct composite crowns after pulpotomy. The teeth were evaluated according to the modified United States Public Health Service criteria at the 3, 6, 9, and 12-month follow-ups. All crowns were intact at the 1-year follow-up, and showed complete adaptation. None of the patients had secondary caries, and they all had acceptable gingival health. Also, none of the crowns showed discoloration. The present results were similar to those of Mohammadzadeh et al, [15] who restored teeth with indirect composite crowns by using fiber-reinforced composites for laboratory fabrication of tooth-colored crowns for primary molars, and reported optimal success rate at the 1-year follow-up.
The described approach has advantages such as designing a direct composite model by using the precise anatomy of SSCs, and using the available composite resins. Also, this approach does not require laboratory procedures, which saves time and cost. However, further studies on a higher number of patients with longer follow-ups are required to cast a final judgment regarding its widespread use.
Conclusion
Previous studies demonstrated that multi-surface restorations were not successful in primary teeth [36,37]. Pires et al, [38] in a systematic review and meta-analysis in 2018 compared the bond strength of primary and permanent teeth. They acknowledged the differences between the primary and permanent enamel and dentin, which are responsible for the different bond strength values of composite to primary and permanent teeth. The enamel in primary teeth is thin, and primary dentin has lower mineral content. Also, due to high density of dentinal tubules in primary teeth, the amount of available inter-tubular dentin for bonding is lower. All these factors are responsible for lower bond strength of composite to primary teeth, compared with permanent teeth [39]. However, the bond strength of composite to primary and permanent enamel has been reported to be comparable [40-42]. In the present study, direct composite crown had a larger bonding interface with enamel compared with multi-surface restorations, which can aid in clinical success and durability of restorations.
In the present study, the primary first molars of 5 patients were restored with direct composite crowns after pulpotomy. The teeth were evaluated according to the modified United States Public Health Service criteria at the 3, 6, 9, and 12-month follow-ups. All crowns were intact at the 1-year follow-up, and showed complete adaptation. None of the patients had secondary caries, and they all had acceptable gingival health. Also, none of the crowns showed discoloration. The present results were similar to those of Mohammadzadeh et al, [15] who restored teeth with indirect composite crowns by using fiber-reinforced composites for laboratory fabrication of tooth-colored crowns for primary molars, and reported optimal success rate at the 1-year follow-up.
The described approach has advantages such as designing a direct composite model by using the precise anatomy of SSCs, and using the available composite resins. Also, this approach does not require laboratory procedures, which saves time and cost. However, further studies on a higher number of patients with longer follow-ups are required to cast a final judgment regarding its widespread use.
Conclusion
It appears that direct composite crown can serve as a suitable esthetic restoration for pulpotomized primary molars in cooperative patients with acceptable oral hygiene.
Type of Study: Case report |
Subject:
pediatric
References
1. Akhlaghi N, Hajiahmadi M, Golbidi M. Attitudes of Parents and Children toward Primary Molars Restoration with Stainless Steel Crown. Contemp Clin Dent. 2017 Jul-Sep;8(3):421-6. [DOI:10.4103/ccd.ccd_379_17] [PMID] []
2. Lopez-Cazaux S, Aiem E, Velly AM, Muller-Bolla M. Preformed pediatric zirconia crown versus preformed pediatric metal crown: study protocol for a randomized clinical trial. Trials. 2019 Aug 24;20(1):530. [DOI:10.1186/s13063-019-3559-1] [PMID] []
3. Rezvi FB, Mathew MG, Gurunathan D. Crowns in Pediatric Dentistry-A Review. Annals of RSCB . 2021;25(3):30-9.
4. Abdulhadi BS, Abdullah MM, Alaki SM, Alamoudi NM, Attar MH. Clinical Evaluation Between Zirconia Crowns and Stainless Crowns in Primary Molars Teeth. Journal of Pediatric Dentistry 2017; 5(1): 21-7. [DOI:10.4103/jpd.jpd_21_17]
5. Möhn M, Frankenberger R, Krämer N. Wear and marginal quality of aesthetic crowns for primary molars. Int J Paediatr Dent. 2022 Mar;32(2):273-83. [DOI:10.1111/ipd.12852] [PMID]
6. Nowak AJ. Pediatric Dentistry: Infancy Through Adolescence. 6th ed. USA: ELSEVIER; 2019. 634 P.
7. Rocha MCM, Inácio GC, Taira TM, Delgado RZR, Maciel SM, Frítola MJPDJ. Zirconia crowns as an esthetic alternative for oral rehabilitation in pediatric dentistry: A review. Pediatric Dental Journal. 2021;31(3):224-34. [DOI:10.1016/j.pdj.2021.07.001]
8. Guelmann M, Shapira J, Silva DR, Fuks AB. Esthetic restorative options for pulpotomized primary molars: a review of literature. J Clin Pediatr Dent. 2011 Winter;36(2):123-6. [DOI:10.17796/jcpd.36.2.34h304265110137r] [PMID]
9. Chen X, Zhong J, Yan W, Zhang H, Jiang X, Huang Q, et al. Clinical performance of rensin-bonded composite strip crowns in primary incisors. Journal of Peking University Health Sciences 2020;52(5):907-12.
10. Grewal N, Jha S, Kaur N. Clinical and Radiographic Success of Resin-bonded Strip Crowns in Primary Incisors with Varying Extents of Sound Tooth Structure Available for Bonding. Int J Clin Pediatr Dent. 2021 Jul-Aug;14(4):454-61. [DOI:10.5005/jp-journals-10005-1984] [PMID] []
11. Garg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry: A review. J Adv Med Dent Scie Res 2016;4(2):41-6.
12. Chen K, Lei Q, Xiong H, Chen Y, Luo W, Liang Y. A 2-year clinical evaluation of stainless steel crowns and composite resin restorations in primary molars under general anaesthesia in China's Guangdong province. Br Dent J. 2018 Jul 13;225(1):49-52. [DOI:10.1038/sj.bdj.2018.519] [PMID]
13. Chisini LA, Collares K, Cademartori MG, de Oliveira LJC, Conde MCM, Demarco FF, Corrêa MB. Restorations in primary teeth: a systematic review on survival and reasons for failures. Int J Paediatr Dent. 2018 Mar;28(2):123-39. [DOI:10.1111/ipd.12346] [PMID]
14. Mathew MG, Roopa KB, Soni AJ, Khan MM, Kauser A. Evaluation of Clinical Success, Parental and Child Satisfaction of Stainless Steel Crowns and Zirconia Crowns in Primary Molars. J Family Med Prim Care. 2020 Mar 26;9(3):1418-23. [DOI:10.4103/jfmpc.jfmpc_1006_19] [PMID] []
15. Mohammadzadeh Z, Parisay I, Mehrabkhani M, Madani AS, Mazhari F. Clinical evaluation of fiber-reinforced composite crowns in pulp-treated primary molars: 12-month results. Eur J Dent. 2016 Oct-Dec;10(4):522-8. [DOI:10.4103/1305-7456.195177] [PMID] []
16. Rai D, Bondarde P, Patil S, Mujawar S, Vishwakarma A, Gakhare R. Comparative Evaluation Of Fracture Resistance Of Endodontically Treated Teeth Restored With Different Core Build-Up Materials: An Invitro Study. IOSR-JDMS. 2018;17(10):26-9.
17. Spinhayer L, Bui ATB, Leprince JG, Hardy CMF. Core build-up resin composites: an in-vitro comparative study. Biomater Investig Dent. 2020 Nov 3;7(1):159-66.. [DOI:10.1080/26415275.2020.1838283] [PMID] []
18. Zarow M, Dominiak M, Szczeklik K, Hardan L, Bourgi R, Cuevas-Suárez CE, et al. Effect of Composite Core Materials on Fracture Resistance of Endodontically Treated Teeth: A Systematic Review and Meta-Analysis of In Vitro Studies. Polymers (Basel). 2021 Jul 9;13(14):2251. [DOI:10.3390/polym13142251] [PMID] []
19. Bortolotto T, Melian K, Krejci I. Effect of dual-cure composite resin as restorative material on marginal adaptation of class 2 restorations. Quintessence Int. 2013 Oct;44(9):663-72.
20. Mathew MG, Roopa KB, Soni AJ, Khan MM, Kauser A. Evaluation of Clinical Success, Parental and Child Satisfaction of Stainless Steel Crowns and Zirconia Crowns in Primary Molars. J Family Med Prim Care. 2020 Mar 26;9(3):1418-23. [DOI:10.4103/jfmpc.jfmpc_1006_19] [PMID] []
21. Itskovich R, Lewinstein I, Zilberman U. The Influence of Zinc Oxide Eugenol (ZOE) and Glass Ionomer (GI) Base Materials on the Microhardness of Various Composite and GI Restorative Materials. Open Dent J. 2014 Feb 7;8:13-9. [DOI:10.2174/1874210601408010013] [PMID] []
22. Choi SM, Choi YC, Park JH, Choi SC. The effect of etching time on the pattern of acid etching on the enamel of primary teeth. J Korean Acad Pediatr Dent. 2008;35(3):437-45.
23. Tauböck TT, Bortolotto T, Buchalla W, Attin T, Krejci I. Influence of light-curing protocols on polymerization shrinkage and shrinkage force of a dual-cured core build-up resin composite. Eur J Oral Sci. 2010 Aug;118(4):423-9. [DOI:10.1111/j.1600-0722.2010.00746.x] [PMID]
24. Pan CY, Lan TH, Liu PH, Fu WR. Comparison of Different Cervical Finish Lines of All-Ceramic Crowns on Primary Molars in Finite Element Analysis. Materials (Basel). 2020 Mar 1;13(5):1094. [DOI:10.3390/ma13051094] [PMID] []
25. Dederichs M, Fahmy MD, Kuepper H, Guentsch A. Comparison of Gingival Retraction Materials Using a New Gingival Sulcus Model. J Prosthodont. 2019 Aug;28(7):784-9. [DOI:10.1111/jopr.13093] [PMID]
26. Loguercio AD, Luque-Martinez I, Lisboa AH, Higashi C, Queiroz VA, Rego RO, Reis A. Influence of Isolation Method of the Operative Field on Gingival Damage, Patients' Preference, and Restoration Retention in Noncarious Cervical Lesions. Oper Dent. 2015 Nov-Dec;40(6):581-93. [DOI:10.2341/14-089-C] [PMID]
27. Raskin A, Setcos JC, Vreven J, Wilson NH. Influence of the isolation method on the 10-year clinical behaviour of posterior resin composite restorations. Clin Oral Investig. 2000 Sep;4(3):148-52. [DOI:10.1007/s007840000069] [PMID]
28. Dede DÖ, Şahin O, Koroglu A, Yilmaz B. Effect of sealant agents on the color stability and surface roughness of nanohybrid composite resins. J Prosthet Dent. 2016 Jul;116(1):119-28. [DOI:10.1016/j.prosdent.2015.11.024] [PMID]
29. Yikilgan İ, Kamak H, Akgul S, Ozcan S, Bala O. Effects of three different bleaching agents on microhardness and roughness of composite sample surfaces finished with different polishing techniques. J Clin Exp Dent. 2017 Mar 1;9(3):e460-5. [DOI:10.4317/jced.53136] [PMID] []
30. Samer MS, Faraz Q, Al-Dubai SAR, Vohra F, Abdullah H, Taiyeb-Ali TB, Saub R. Clinical Outcomes and Predictors of Satisfaction in Patients with Improved Lithium Disilicate All-Ceramic Crowns. Med Princ Pract. 2017;26(5):470-9. [DOI:10.1159/000481864] [PMID] []
31. American Academy of Pediatric Dentistry. Pulp therapy for primary and immature ermanent teeth. The Reference Manual of Pediatric Dentistry. Chicago, Ill.: American Academy of Pediatric Dentistry; 2021:399-407.
32. Jullien S. Prophylaxis of caries with fluoride for children under five years. BMC Pediatr. 2021;21(1):1-11. [DOI:10.1186/s12887-021-02702-3] [PMID] []
33. Bargale S, Davangere Padmanabh SK, Kariya PB, Shah S, Dave B. Knowledge, attitude, and practice regarding standardized treatment protocol for pulp therapy in deciduous dentition among general dental practitioners of Vadodara, Gujarat, India. J Indian Soc Pedod Prev Dent. 2019 Oct-Dec;37(4):327-2. [DOI:10.4103/JISPPD.JISPPD_186_19] [PMID]
34. Karpagam N, Mathew MG. Knowledge awareness and practice among parents regarding the usage of crowns in pediatric dentistry. Drug Invention Today. 2020;13(5):695-8.
35. Almohareb T, Alayed AA, Alzahrani KM, Maawadh AM, Almutairi B, Alhamdan RS, Bahkali A, Abduljabbar T, Vohra F. Influence of curing duration and mixing techniques of bulk fill resin composites on bi-axial flexural strength and degree of conversion. J Appl Biomater Funct Mater. 2020 Jan-Dec;18:2280800020975721. [DOI:10.1177/2280800020975721] [PMID]
36. Liberman J, Franzon R, Guimarães LF, Casagrande L, Haas AN, Araujo FB. Survival of composite restorations after selective or total caries removal in primary teeth and predictors of failures: A 36-months randomized controlled trial. J Dent. 2020 Feb;93:103268. [DOI:10.1016/j.jdent.2019.103268] [PMID]
37. Pummer A, Cieplik F, Nikolić M, Buchalla W, Hiller KA, Schmalz G. Longevity of posterior composite and compomer restorations in children placed under different types of anesthesia: a retrospective 5-year study. Clin Oral Investig. 2020 Jan;24(1):141-50. [DOI:10.1007/s00784-019-02911-2] [PMID]
38. Pires CW, Soldera EB, Bonzanini LIL, Lenzi TL, Soares FZM, Montagner AF, Rocha RO. Is Adhesive Bond Strength Similar in Primary and Permanent Teeth? A Systematic Review and Meta-analysis. J Adhes Dent. 2018;20(2):87-97.
39. Martínez-Carrasco CA, Nevárez-Rascón A, Soto-Barreras U. Comparative Evaluation of Bond Strength of Self-Etching and Total Etch Dental Adhesive Systems to Dentin of Deciduous and Permanent Teeth. Int. J. Odontostomat. 2020;14(1):55-9. [DOI:10.4067/S0718-381X2020000100055]
40. Ilie N, Schöner C, Bücher K, Hickel R. An in-vitro assessment of the shear bond strength of bulk-fill resin composites to permanent and deciduous teeth. J Dent. 2014 Jul;42(7):850-5. [DOI:10.1016/j.jdent.2014.03.013] [PMID]
41. Nemati Anaraki S, Kazemi H, GHafari Z, Naser Z, Bitaraf T. In-Vitro Comparative Study of the Effect of Four Finishing and Polishing Tools on Surface Roughness of a Microhybrid Resin Composite. Journal of Research in Dental and Maxillofacial Sciences. 2019;4 (2):26-31. [DOI:10.29252/jrdms.4.2.26]
42. Tedesco TK, Soares FZ, Grande RH, Filho LE, Rocha Rde O. Effect of cariogenic challenge on bond strength of adhesive systems to sound and demineralized primary and permanent enamel. J Adhes Dent. 2014 Oct;16(5):421-8.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |