Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 110-118 |
Back to browse issues page


Ethics code: ZUMS.REC.1395.313
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nazemi Salman B, Eftekhar L, Arsang Jang S, Taheri S S, Jafari F. Knowledge and Practice of General Dentists
Regarding the COVID-19 in Zanjan, Iran. J Res Dent Maxillofac Sci 2023; 8 (2) :110-118
URL: http://jrdms.dentaliau.ac.ir/article-1-433-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-433-en.html
Bahareh Nazemi Salman1 
 , Leila Eftekhar2 , Shahram Arsang Jang3 , Seyede Solmaz Taheri4 , Fatemeh Jafari *5
, Leila Eftekhar2 , Shahram Arsang Jang3 , Seyede Solmaz Taheri4 , Fatemeh Jafari *5 
, Leila Eftekhar2 , Shahram Arsang Jang3 , Seyede Solmaz Taheri4 , Fatemeh Jafari *5
1- Department of Pediatrics, School of Dentistry, Zanjan University of Medical Sciences, Zanjan, Iran
2- Department of Pediatrics, Alborz Uni-versity of Medical Sciences, Karaj, Iran
3- Department of Biostatistics, Zanjan University of Medical Sciences, Zan-jan, Iran
4- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- School of Dentistry, Zanjan University of Medical Sciences, Zan-jan, Iran ,fatemeh.jafari.941820013@gmail.com
2- Department of Pediatrics, Alborz Uni-versity of Medical Sciences, Karaj, Iran
3- Department of Biostatistics, Zanjan University of Medical Sciences, Zan-jan, Iran
4- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- School of Dentistry, Zanjan University of Medical Sciences, Zan-jan, Iran ,
Full-Text [PDF 769 kb]
(1042 Downloads)
| Abstract (HTML) (3229 Views)
Introduction
Coronaviruses are the largest group of positively charged RNA viruses with different hosts in nature. Seven major coronaviruses were identified by 2020, three of which namely the severe acute respiratory syndrome coronavirus (SARS‑CoV), the Middle East respiratory syndrome coronavirus (MERS-CoV) and SARS-CoV-2 lead to severe respiratory syndromes with significant mortality [1–3]. SARS-CoV 2 causes coronavirus disease-2019 (COVID-19) which is a serious acute respiratory disease often associated with pneumonia and bronchitis with about 2.3% mortality [4,5]. Most patients infected with COVID-19 experience mild to moderate respiratory symptoms and recover without the need for a special treatment, but the elderly and people with underlying medical conditions such as cardiovascular disease, diabetes mellitus, chronic respiratory disease, and cancer are more likely to develop a more severe form of disease [6]. The most common symptoms are fever, dry cough, and fatigue, and other less common symptoms include sore throat, diarrhea, conjunctivitis, headache, loss of sense of smell and taste, skin rash, or discoloration of the fingers and toes. More severe symptoms include shortness of breath, chest pain, and difficulty speaking or moving [6]. SARS-CoV-2 is thought to be transmitted primarily through close contact between people (6 feet apart) via respiratory droplets when an infected person sneezes, coughs, or talks [7]. In fact, transmission of the virus occurs mainly through inhalation, ingestion, and direct mucosal contact with the saliva droplets inoculated with the virus [8]. Dental centers are at risk of infection with SARS-CoV-2 due to airborne virus particles (aerosols) generated by dental procedures, hand contact with dental equipment, and close proximity to the dentist's mouth and throat [2,9]. A patient suffering from COVID-19 may transmit the disease not only to the dentist and dental assistant through aerosols, but also to other patients through aerosols remaining in the environment and on surfaces for a long time. A previous study showed that SARS-COV-2 can survive in different environmental situations from hours to days [10]. Dental procedures involve the use of rotating instruments such as handpieces, ultrasonic scalers, and air-water syringes. These devices generate aerosols, which include small particles of water, saliva, blood and other debris [7]. The Center for Disease Control and Prevention, the World Health Organization, and the American Dental Association (ADA) responded to the epidemic by providing guidelines to better control the spread of the virus. These recommendations include the use of personal protective equipment such as FFP2 and FFP3 face protection masks for aerosol producing procedures, disposable protective clothing, goggles, regular and precise surface disinfection, office room ventilation, and hand washing with alcoholic solutions. Rinsing the mouth with chlorhexidine or hydrogen peroxide solution at the beginning of treatment can significantly reduce bacteria and viruses in the oral cavity. However, the use of rubber dam is especially recommended in restorative and endodontic procedures [11,12].
To ensure compliance with the new protocols, it is necessary to ensure the office safety by patient screening, categorizing and prioritizing patients through phone or online, observing social distancing, avoiding placing extra magazines and furniture in the waiting room and reducing the presence of companions, relatives, and parents [12]. In cases with coronary heart disease, dental procedures should be limited to emergency procedures [8]. Obviously, by observing the relevant instructions in this regard, we can take steps to control and prevent this disease and maintain the health of the staff and patients. Therefore, it is necessary to be aware of these principles and regulations and adopt appropriate practices during the COVID-19 epidemic. This study assessed the level of knowledge and practice of Zanjan general dentists regarding COVID-19.
Materials and Methods
This descriptive-analytical study was performed on 107 general dentists in Zanjan city between September 9 to 17, 2021 (ethical approval code: ZUMS.REC.13400.155) who were selected by census sampling. The inclusion criteria were general dentists working in clinics and offices in Zanjan. The exclusion criterion was unwillingness to participate in the study. The questionnaire used for this study was designed according to the questionnaires that had been used in similar previous studies [13–16]. The questionnaire consisted of three sections: demographic information, 4-choice questions for knowledge assessment, and multiple-choice questions for practice assessment. After initial designing of the questionnaire, in order to assess its content validity, the questionnaire was given to 15 experts including faculty members and general dentists, radiologists, oral medicine specialists, operative dentists, periodontists, and prosthodontists, and they were asked to express their opinion regarding each question. Finally, after a few spelling corrections and omission of two questions, the desired validity of 0.82 was achieved. The Cronbach's alpha test was used to evaluate its reliability. The internal correlation coefficient and open test were used to assess its reliability. For this purpose, the questionnaire was given to 8 general dentists and after 2 days (due to fast change in knowledge level of participants about COVID-19, such a short time period was considered), they were asked to fill out the questionnaire again. Finally, a Cronbach's alpha of 0.79 was achieved. The questionnaire was created by the researcher online in Porsline.ir and sent to the general dentists of Zanjan city through WhatsApp. The objectives of the study were also explained to them so that they could participate in the project if they wished to do so. Out of 107 dentists practicing in Zanjan city, 95 dentists participated in this study, of which 89 completed and returned the questionnaires (6 others were excluded from the study). To better describe the results and compare it with other studies, the scores were changed to 100. Then, according to the quadruple index, the dentists were classified into four groups according to their score: scores zero to 25: very low knowledge level, scores 26 to 50: low knowledge level, scores 51 to 75: medium to high knowledge level, and scores 76 to 100: high knowledge level. In terms of practice, scores zero to 25 indicated very poor practice, scores 26 to 50 indicated poor practice, scores 51 to 75 indicated medium to optimal practice, and scores 76 to 100 indicated optimal practice level. One-way ANOVA, independent sample t-test, and Pearson’s correlation test were used in SPSS 26 at 95% confidence level for data analysis.
Results
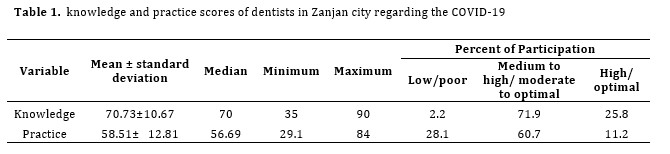
The mean knowledge score of dentists was found to be 70.73 ± 10.67. The knowledge level of most (71.9%) dentists was moderate to high and 25.8% had a high level of knowledge. Only 2.2% of them had a low level of knowledge and none of them acquired a knowledge score below 25. The mean practice score of dentists was 58.51± 10.03. Considering the classification of practice score, 60.7% had moderate to optimal practice and 11.2% had optimal practice. Also, 28.1% acquired a poor practice score and none of them subjects had a score below 25 (Table 1).
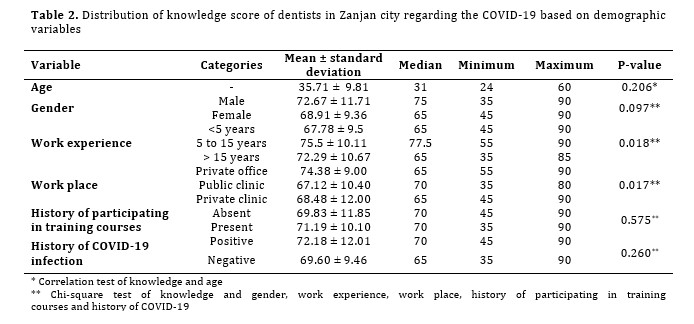
The level of knowledge of dentists with 5 to 15 years of work experience was significantly higher than others (P=0.018). Dentists working in private offices had significantly higher knowledge level (p=0.017) than the other two groups (public clinic and private clinic) (Table 2). There was a moderate correlation between age and practice (P=0.003). Dentists with more than 15 years of work experience had a higher practice score (P<0.001).
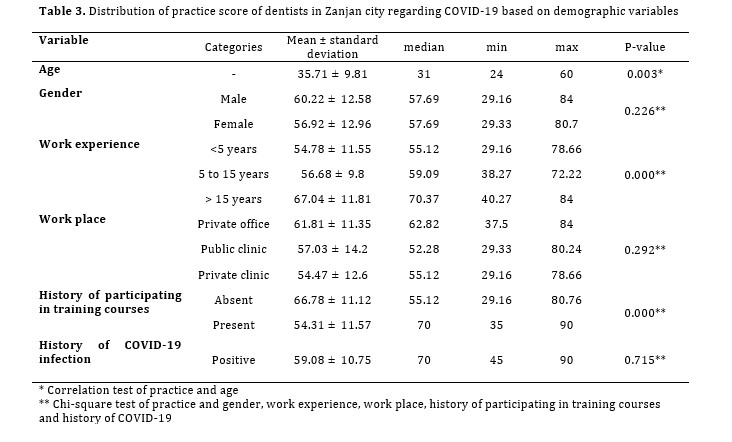
Participating in training courses improved the practice of dentists such that they acquired a higher practice score (P<0.001, Table 3)
Table 1. knowledge and practice scores of dentists in Zanjan city regarding the COVID-19
Table 2. Distribution of knowledge score of dentists in Zanjan city regarding the COVID-19 based on demographic variables
Discussion
According to the American Dental Association, people working in the field of dentistry are more exposed to the SARS-CoV2 than any other member of the medical staff, including general practitioners and nurses. Also, patients presenting to dental clinics and offices are at higher risk of contracting COVID-19 than those presenting to other medical centers [17]. Bazzazpour et al. examined the presence of COVID-19 virus in the air of dental clinics and announced that 36% of the samples obtained from the air of dental clinics in Tehran had SARS-CoV2 [18]. Therefore, it is necessary to adopt preventive strategies to prevent the spread of the virus and disease transmission. Khader et al. [19] stated that most Jordanian dentists were aware of the symptoms of COVID-19, methods of identifying suspected patients, routes of disease transmission, and prevention in dental clinics. De Stefani et al. [12], also stated that dentists' knowledge about the routes of disease transmission and disease symptoms was very good. Kamate et al. [13], also reported good knowledge level of dentists regarding COVID-19. Sarkarat et al. [20], in Iran, assessed the dentists' knowledge level about COVID-19, and reported that 70% of them correctly answered most of the knowledge questions. In a study by Widyarman et al. [21] conducted in Indonesia, the mean knowledge score of the study group was estimated at 78.8%, which was slightly higher than the score obtained in the current study. This difference could be due to smaller sample size in their study or using a simpler questionnaire, suggesting that the present questionnaire was probably more accurate. In contrast, in Pakistan, the knowledge of medical professionals was low and the first-line treatment providers in Pakistan were not prepared to deal with COVID-19 [22]. A similar study was conducted in India by Naveed et al. [23] who reported the students' knowledge about the clinical aspects of the disease to be good, but recommended more emphasis on knowledge related to the diagnosis and treatment of patients with COVID-19. Hleyhel et al. [24] reported that Lebanese dentists' knowledge and preventive practice against COVID-19 were low, and only 15% of dentists had high knowledge level. Such variations in the results can be due to differences in the questionnaire used or due to differences in the statistical population studied. Due to the novelty of the disease, it should be noted that all these studies were conducted in the past few months or year, and a time difference of one month can even affect the knowledge of researchers and clinicians. Studies about the dentists' knowledge to deal with airborne infections like SARS-CoV and MERS-CoV [25,26] showed poor knowledge and practice of dentists in relation to such diseases, which could be due to the fact that such diseases did not turn into a pandemic. Of course, development of the media and social networks and speed of information transfer compared to the past also play a significant role in knowledge enhancement of dentists. In the present study, no significant relationship was found between gender and age with the knowledge level, while in the study by Baseer et al. [26] regarding MERS, women had a higher knowledge level and in the study by Hleyhel et al. [24], young dentists were more knowledgeable. Perhaps because women care more about health and have higher knowledge of using international media. About 69% of the dentists in the present study acquired their knowledge from the social networks, which has been confirmed in several other studies such as the ones by Naveed et al, [23] Askarian et al, [25] Kamate et al, [13] and Pourfarrokh et al [27]. However, Putrino et al. [28] in Italy found the Ministry of Health to be the main source of information for 535 dentists, highlighting the Ministry of Health's key role in informing and raising awareness among healthcare providers. Overall, the present study and other studies on COVID-19, compared to studies on other airborne diseases, show an improvement in dentists' knowledge and preparedness, which may be due to the rapid spread of information and the fact that COVID-19 led to a global pandemic with high mortality rate. According to the results, 71.9% of dentists had moderate to optimal and optimal practice, which was close to the findings of Kamate et al. [13] reporting that 79.5% of the participants had good and optimal practice scores. In the study by Hleyhel et al. [24] dentists had a practice score of 71.25, and only 35% of them had optimal practice. In the present study, 62.9% of dentists asked patients to rinse 0.12-0.2% chlorhexidine before the procedure. Chlorhexidine was also the most widely used mouthwash in previous studies [29,30]. Considering the availability and low cost of chlorhexidine mouthwash compared with hydrogen peroxide, it seems to be a reasonable precaution in Zanjan city. According to the results of the present study, 44.9% of dentists screened patients for COVID-19 symptoms by asking them to fill out a self-report form, and 40.4% of dentists measured patients' body temperature before admission. In the study by Kamate et al. [13] 32% of dentists asked patients about the signs and symptoms of COVID-19. However, Yu et al. [31] reported pre-treatment screening by 98.5% of clinicians (92.8% took the patients’ temperature and 74.4% asked for a negative test). Also, 95% of dentists stated that they used face shields, 76.4% used protective glasses, 78.7% used N95 facial masks, and 85.4% use disposable gauze during treatment. The frequency of use of personal protective equipment in similar previous studies was lower, which may be due to enhancement of the dentists’ knowledge about COVID-19 over time [13,31]. In the present study, 16.9% used rubber dam and 62.9% used strong high volume suction during procedures, which indicates their correct practice due to definitely optimal efficacy of these measures to reduce aerosols [32]. In the present study, the practice of dentists improved with age, which appears to be due to the greater concern of older people about COVID-19 and higher rate of related complications at older ages. Also, people with more than 15 years of work experience performed better, which could be due to longer experience with airborne diseases. According to the results, 34% of dentists had participated in COVID-19 courses or workshops (virtually or in person); 44% of the dentists participating in the present study had contracted COVID-19, which is a significant number compared to the studies by Sarkarat et al. [33], (2.2%) and Ahmadi et al. [34] (7%). This increase in prevalence can be due to the peak of the disease, its high prevalence in the society, mutation of the virus, and its increased transmissibility.
Educating patients to prevent the spread of the virus (78.7%), performing purely emergency treatments only (61.8%) and adherence to preventive measures were among the most important tasks of dentists during the COVID-19 pandemic.
The present study was performed in September 2021, concomitant with the fifth wave of the COVID-19. General vaccination for the target population was underway, and vaccination of medical staff, including dentists, was almost complete. It can be said that even though the vaccine was available, dentists were bound by the protocols and principles of protection and prevention. However, vaccination is incomplete and information on its effectiveness is definitely not available, and adoption of these principles by dentists appears to be reasonable.
One advantage of the present study was using a comprehensive questionnaire that included questions about measures before, during, and after treatment. In addition, questions related to the COVID-19 vaccine, its types, and its symptoms and complications were included, which made the present questionnaire unique. Moreover, in this questionnaire, questions were asked to evaluate how dentists perform in challenging situations; including management of suspected patients with COVID-19 symptoms, management of suspected or infected staff, how to manage conditions after treatment of a person with COVID-19, and management of patients immediately after vaccination. This study had some limitations as well. Not all general dentists in Zanjan city participated in this study. Random answers to the questions, constantly changing information regarding the COVID-19, and emergence of new findings were among other limitations. Future evaluation of the knowledge and practice of specialists in Zanjan city regarding the COVID-19 pandemic in terms of general considerations and treatment measures is required for the purpose of comparison with the present findings.
Conclusion
Knowledge and practice of dentists in Zanjan city regarding COVID-19 was moderate to high (optimal). However, the knowledge and practice of dentists were still far from ideal.
Acknowledgment
Full-Text: (1556 Views)
| Abstract
Background and Aim: Severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) that caused the coronavirus disease-2019 (COVID-19) pandemic is ransmitted through close contact via respiratory droplets when an infected patient sneezes, coughs, or talks. Due to close contact with patients, dentists are at higher risk of COVID-19. The aim of this study was to evaluate the knowledge and practice of general dentists in Zanjan regarding the COVID-19. Materials and Methods: This cross-sectional study was conducted on 107 general dentists working in Zanjan city in September 2021, simultaneous with the fifth wave of the COVID-19, who were selected by census sampling. A researcher-designed questionnaire was used to assess the knowledge and practice after assessing its reliability and validity. The effect of age, gender, work experience, and place of work on knowledge and practice of dentists was analyzed by one-way ANOVA, independent sample t-test, and Pearson’s correlation test (alpha=0.05). Results: Of all, 89 questionnaires were returned. The mean age of the participants was 35.9 years, and 77.5% of dentists acquired their knowledge about COVID-19 pandemic through the social networks. The mean knowledge and practice scores of dentists were 70.73±10.67 and 58.51±12.81, respectively (out of 100). Dentists with 5 to 15 years of work experience had the highest level of knowledge (P=0.018). The practice score significantly increased with age (P=0.003). Also, dentists with more than 15 years of work experience acquired higher practice scores (P=0.000) Conclusion: Dentists' knowledge and practice regarding COVID-19 and its treatment was moderate to high (optimal). However, their knowledge and practice were still far from the ideal level, indicating the need for educational planning to enhance their knowledge and improve their practice to deal with COVID-19. Key Words: COVID-19; Infection Control; Knowledge; Pandemics; Practice Guideline |
Introduction
Coronaviruses are the largest group of positively charged RNA viruses with different hosts in nature. Seven major coronaviruses were identified by 2020, three of which namely the severe acute respiratory syndrome coronavirus (SARS‑CoV), the Middle East respiratory syndrome coronavirus (MERS-CoV) and SARS-CoV-2 lead to severe respiratory syndromes with significant mortality [1–3]. SARS-CoV 2 causes coronavirus disease-2019 (COVID-19) which is a serious acute respiratory disease often associated with pneumonia and bronchitis with about 2.3% mortality [4,5]. Most patients infected with COVID-19 experience mild to moderate respiratory symptoms and recover without the need for a special treatment, but the elderly and people with underlying medical conditions such as cardiovascular disease, diabetes mellitus, chronic respiratory disease, and cancer are more likely to develop a more severe form of disease [6]. The most common symptoms are fever, dry cough, and fatigue, and other less common symptoms include sore throat, diarrhea, conjunctivitis, headache, loss of sense of smell and taste, skin rash, or discoloration of the fingers and toes. More severe symptoms include shortness of breath, chest pain, and difficulty speaking or moving [6]. SARS-CoV-2 is thought to be transmitted primarily through close contact between people (6 feet apart) via respiratory droplets when an infected person sneezes, coughs, or talks [7]. In fact, transmission of the virus occurs mainly through inhalation, ingestion, and direct mucosal contact with the saliva droplets inoculated with the virus [8]. Dental centers are at risk of infection with SARS-CoV-2 due to airborne virus particles (aerosols) generated by dental procedures, hand contact with dental equipment, and close proximity to the dentist's mouth and throat [2,9]. A patient suffering from COVID-19 may transmit the disease not only to the dentist and dental assistant through aerosols, but also to other patients through aerosols remaining in the environment and on surfaces for a long time. A previous study showed that SARS-COV-2 can survive in different environmental situations from hours to days [10]. Dental procedures involve the use of rotating instruments such as handpieces, ultrasonic scalers, and air-water syringes. These devices generate aerosols, which include small particles of water, saliva, blood and other debris [7]. The Center for Disease Control and Prevention, the World Health Organization, and the American Dental Association (ADA) responded to the epidemic by providing guidelines to better control the spread of the virus. These recommendations include the use of personal protective equipment such as FFP2 and FFP3 face protection masks for aerosol producing procedures, disposable protective clothing, goggles, regular and precise surface disinfection, office room ventilation, and hand washing with alcoholic solutions. Rinsing the mouth with chlorhexidine or hydrogen peroxide solution at the beginning of treatment can significantly reduce bacteria and viruses in the oral cavity. However, the use of rubber dam is especially recommended in restorative and endodontic procedures [11,12].
To ensure compliance with the new protocols, it is necessary to ensure the office safety by patient screening, categorizing and prioritizing patients through phone or online, observing social distancing, avoiding placing extra magazines and furniture in the waiting room and reducing the presence of companions, relatives, and parents [12]. In cases with coronary heart disease, dental procedures should be limited to emergency procedures [8]. Obviously, by observing the relevant instructions in this regard, we can take steps to control and prevent this disease and maintain the health of the staff and patients. Therefore, it is necessary to be aware of these principles and regulations and adopt appropriate practices during the COVID-19 epidemic. This study assessed the level of knowledge and practice of Zanjan general dentists regarding COVID-19.
Materials and Methods
This descriptive-analytical study was performed on 107 general dentists in Zanjan city between September 9 to 17, 2021 (ethical approval code: ZUMS.REC.13400.155) who were selected by census sampling. The inclusion criteria were general dentists working in clinics and offices in Zanjan. The exclusion criterion was unwillingness to participate in the study. The questionnaire used for this study was designed according to the questionnaires that had been used in similar previous studies [13–16]. The questionnaire consisted of three sections: demographic information, 4-choice questions for knowledge assessment, and multiple-choice questions for practice assessment. After initial designing of the questionnaire, in order to assess its content validity, the questionnaire was given to 15 experts including faculty members and general dentists, radiologists, oral medicine specialists, operative dentists, periodontists, and prosthodontists, and they were asked to express their opinion regarding each question. Finally, after a few spelling corrections and omission of two questions, the desired validity of 0.82 was achieved. The Cronbach's alpha test was used to evaluate its reliability. The internal correlation coefficient and open test were used to assess its reliability. For this purpose, the questionnaire was given to 8 general dentists and after 2 days (due to fast change in knowledge level of participants about COVID-19, such a short time period was considered), they were asked to fill out the questionnaire again. Finally, a Cronbach's alpha of 0.79 was achieved. The questionnaire was created by the researcher online in Porsline.ir and sent to the general dentists of Zanjan city through WhatsApp. The objectives of the study were also explained to them so that they could participate in the project if they wished to do so. Out of 107 dentists practicing in Zanjan city, 95 dentists participated in this study, of which 89 completed and returned the questionnaires (6 others were excluded from the study). To better describe the results and compare it with other studies, the scores were changed to 100. Then, according to the quadruple index, the dentists were classified into four groups according to their score: scores zero to 25: very low knowledge level, scores 26 to 50: low knowledge level, scores 51 to 75: medium to high knowledge level, and scores 76 to 100: high knowledge level. In terms of practice, scores zero to 25 indicated very poor practice, scores 26 to 50 indicated poor practice, scores 51 to 75 indicated medium to optimal practice, and scores 76 to 100 indicated optimal practice level. One-way ANOVA, independent sample t-test, and Pearson’s correlation test were used in SPSS 26 at 95% confidence level for data analysis.
Results
The mean knowledge score of dentists was found to be 70.73 ± 10.67. The knowledge level of most (71.9%) dentists was moderate to high and 25.8% had a high level of knowledge. Only 2.2% of them had a low level of knowledge and none of them acquired a knowledge score below 25. The mean practice score of dentists was 58.51± 10.03. Considering the classification of practice score, 60.7% had moderate to optimal practice and 11.2% had optimal practice. Also, 28.1% acquired a poor practice score and none of them subjects had a score below 25 (Table 1).
The level of knowledge of dentists with 5 to 15 years of work experience was significantly higher than others (P=0.018). Dentists working in private offices had significantly higher knowledge level (p=0.017) than the other two groups (public clinic and private clinic) (Table 2). There was a moderate correlation between age and practice (P=0.003). Dentists with more than 15 years of work experience had a higher practice score (P<0.001).
Participating in training courses improved the practice of dentists such that they acquired a higher practice score (P<0.001, Table 3)
Table 1. knowledge and practice scores of dentists in Zanjan city regarding the COVID-19
{kind=link}
Table 2. Distribution of knowledge score of dentists in Zanjan city regarding the COVID-19 based on demographic variables
{kind=link}
{kind=link}
Discussion
According to the American Dental Association, people working in the field of dentistry are more exposed to the SARS-CoV2 than any other member of the medical staff, including general practitioners and nurses. Also, patients presenting to dental clinics and offices are at higher risk of contracting COVID-19 than those presenting to other medical centers [17]. Bazzazpour et al. examined the presence of COVID-19 virus in the air of dental clinics and announced that 36% of the samples obtained from the air of dental clinics in Tehran had SARS-CoV2 [18]. Therefore, it is necessary to adopt preventive strategies to prevent the spread of the virus and disease transmission. Khader et al. [19] stated that most Jordanian dentists were aware of the symptoms of COVID-19, methods of identifying suspected patients, routes of disease transmission, and prevention in dental clinics. De Stefani et al. [12], also stated that dentists' knowledge about the routes of disease transmission and disease symptoms was very good. Kamate et al. [13], also reported good knowledge level of dentists regarding COVID-19. Sarkarat et al. [20], in Iran, assessed the dentists' knowledge level about COVID-19, and reported that 70% of them correctly answered most of the knowledge questions. In a study by Widyarman et al. [21] conducted in Indonesia, the mean knowledge score of the study group was estimated at 78.8%, which was slightly higher than the score obtained in the current study. This difference could be due to smaller sample size in their study or using a simpler questionnaire, suggesting that the present questionnaire was probably more accurate. In contrast, in Pakistan, the knowledge of medical professionals was low and the first-line treatment providers in Pakistan were not prepared to deal with COVID-19 [22]. A similar study was conducted in India by Naveed et al. [23] who reported the students' knowledge about the clinical aspects of the disease to be good, but recommended more emphasis on knowledge related to the diagnosis and treatment of patients with COVID-19. Hleyhel et al. [24] reported that Lebanese dentists' knowledge and preventive practice against COVID-19 were low, and only 15% of dentists had high knowledge level. Such variations in the results can be due to differences in the questionnaire used or due to differences in the statistical population studied. Due to the novelty of the disease, it should be noted that all these studies were conducted in the past few months or year, and a time difference of one month can even affect the knowledge of researchers and clinicians. Studies about the dentists' knowledge to deal with airborne infections like SARS-CoV and MERS-CoV [25,26] showed poor knowledge and practice of dentists in relation to such diseases, which could be due to the fact that such diseases did not turn into a pandemic. Of course, development of the media and social networks and speed of information transfer compared to the past also play a significant role in knowledge enhancement of dentists. In the present study, no significant relationship was found between gender and age with the knowledge level, while in the study by Baseer et al. [26] regarding MERS, women had a higher knowledge level and in the study by Hleyhel et al. [24], young dentists were more knowledgeable. Perhaps because women care more about health and have higher knowledge of using international media. About 69% of the dentists in the present study acquired their knowledge from the social networks, which has been confirmed in several other studies such as the ones by Naveed et al, [23] Askarian et al, [25] Kamate et al, [13] and Pourfarrokh et al [27]. However, Putrino et al. [28] in Italy found the Ministry of Health to be the main source of information for 535 dentists, highlighting the Ministry of Health's key role in informing and raising awareness among healthcare providers. Overall, the present study and other studies on COVID-19, compared to studies on other airborne diseases, show an improvement in dentists' knowledge and preparedness, which may be due to the rapid spread of information and the fact that COVID-19 led to a global pandemic with high mortality rate. According to the results, 71.9% of dentists had moderate to optimal and optimal practice, which was close to the findings of Kamate et al. [13] reporting that 79.5% of the participants had good and optimal practice scores. In the study by Hleyhel et al. [24] dentists had a practice score of 71.25, and only 35% of them had optimal practice. In the present study, 62.9% of dentists asked patients to rinse 0.12-0.2% chlorhexidine before the procedure. Chlorhexidine was also the most widely used mouthwash in previous studies [29,30]. Considering the availability and low cost of chlorhexidine mouthwash compared with hydrogen peroxide, it seems to be a reasonable precaution in Zanjan city. According to the results of the present study, 44.9% of dentists screened patients for COVID-19 symptoms by asking them to fill out a self-report form, and 40.4% of dentists measured patients' body temperature before admission. In the study by Kamate et al. [13] 32% of dentists asked patients about the signs and symptoms of COVID-19. However, Yu et al. [31] reported pre-treatment screening by 98.5% of clinicians (92.8% took the patients’ temperature and 74.4% asked for a negative test). Also, 95% of dentists stated that they used face shields, 76.4% used protective glasses, 78.7% used N95 facial masks, and 85.4% use disposable gauze during treatment. The frequency of use of personal protective equipment in similar previous studies was lower, which may be due to enhancement of the dentists’ knowledge about COVID-19 over time [13,31]. In the present study, 16.9% used rubber dam and 62.9% used strong high volume suction during procedures, which indicates their correct practice due to definitely optimal efficacy of these measures to reduce aerosols [32]. In the present study, the practice of dentists improved with age, which appears to be due to the greater concern of older people about COVID-19 and higher rate of related complications at older ages. Also, people with more than 15 years of work experience performed better, which could be due to longer experience with airborne diseases. According to the results, 34% of dentists had participated in COVID-19 courses or workshops (virtually or in person); 44% of the dentists participating in the present study had contracted COVID-19, which is a significant number compared to the studies by Sarkarat et al. [33], (2.2%) and Ahmadi et al. [34] (7%). This increase in prevalence can be due to the peak of the disease, its high prevalence in the society, mutation of the virus, and its increased transmissibility.
Educating patients to prevent the spread of the virus (78.7%), performing purely emergency treatments only (61.8%) and adherence to preventive measures were among the most important tasks of dentists during the COVID-19 pandemic.
The present study was performed in September 2021, concomitant with the fifth wave of the COVID-19. General vaccination for the target population was underway, and vaccination of medical staff, including dentists, was almost complete. It can be said that even though the vaccine was available, dentists were bound by the protocols and principles of protection and prevention. However, vaccination is incomplete and information on its effectiveness is definitely not available, and adoption of these principles by dentists appears to be reasonable.
One advantage of the present study was using a comprehensive questionnaire that included questions about measures before, during, and after treatment. In addition, questions related to the COVID-19 vaccine, its types, and its symptoms and complications were included, which made the present questionnaire unique. Moreover, in this questionnaire, questions were asked to evaluate how dentists perform in challenging situations; including management of suspected patients with COVID-19 symptoms, management of suspected or infected staff, how to manage conditions after treatment of a person with COVID-19, and management of patients immediately after vaccination. This study had some limitations as well. Not all general dentists in Zanjan city participated in this study. Random answers to the questions, constantly changing information regarding the COVID-19, and emergence of new findings were among other limitations. Future evaluation of the knowledge and practice of specialists in Zanjan city regarding the COVID-19 pandemic in terms of general considerations and treatment measures is required for the purpose of comparison with the present findings.
Conclusion
Knowledge and practice of dentists in Zanjan city regarding COVID-19 was moderate to high (optimal). However, the knowledge and practice of dentists were still far from ideal.
Acknowledgment
The authors would like to thank Zanjan University of Medical Sciences, Department of Dentistry and the Research Vice-Chancellor of the University for facilitating the conduction of this research project.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Berry M, Gamieldien J, Fielding BC. Identification of new res-piratory viruses in the new millennium. Viruses. 2015 Mar 6;7(3):996-1019. [DOI:10.3390/v7030996] [PMID] [PMCID]
2. Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020 Mar 3;12(1):9. [DOI:10.1038/s41368-020-0075-9] [PMID] [PMCID]
3. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012 Nov 8;367(19):1814-20. [DOI:10.1056/NEJMoa1211721] [PMID]
4. Zhao WM, Song SH, Chen ML, Zou D, Ma LN, Ma YK, Li RJ, et al. The 2019 novel coronavirus resource. Yi Chuan. 2020 Feb 20;42(2):212-21.
5. Eurosurveillance editorial team. Note from the editors: novel coronavirus (2019-nCoV). Euro Surveill. 2020 Jan; 25 (3):2001231. [DOI:10.2807/1560-7917.ES.2020.25.3.2001231] [PMID]
6. WHO. World Health Organization. World Health Organization [Internet]. Vol. 2019, WHO. 2021 [cited 2022 Mar 30]. p. 5. Available from:https://apps.who.int/gb/bd/PDF/bd47/ EN/constitutionen.pdf?fbclid=IwAR3bSPmEMO5GR9oP9tFp5lD0BZFJM-fAtc12ogjAp8kFTD2t_fahFbfFeNY.
7. Lewis NM, Salmanson AP, Price A, Risk I, Guymon C, Wisner M, Gardner K, Fukunaga R, Schwitters A, Lambert L, Baggett HC, Ewetola R, Dunn AC. Community-Associated Out-break of COVID-19 in a Correctional Facility - Utah, September 2020-January 2021. MMWR Morb Mortal Wkly Rep. 2021 Apr 2;70(13):467-72. [DOI:10.15585/mmwr.mm7013a2] [PMID] [PMCID]
8. Shirzaiy M. The effect of corona disease(COVID-19) on dentis-try. J Res Dent Sci. 2020; 17 (2) :80-83. [DOI:10.29252/jrds.17.2.80]
9. Kashid R, Shidhore A, Kazi M, Patil S. Awareness of COVID-19 amongst undergraduate dental students in India-A questionnaire based cross-sectional study. IJDSIR. 2020; 3 (3):90-7. [DOI:10.21203/rs.3.rs-27183/v1]
10. Marquès M, Domingo JL. Contamination of inert surfaces by SARS-CoV-2: Persistence, stability and infectivity. A review. Environ Res. 2021 Feb;193:110559. [DOI:10.1016/j.envres.2020.110559] [PMID] [PMCID]
11. Derruau S, Bouchet J, Nassif A, Baudet A, Yasukawa K, Lorim-ier S, Prêcheur I, Bloch-Zupan A, Pellat B, Chardin H, Jung S, On Behalf Of Task Force Covid-Collège National des EnseignantS En Biologie Orale Cnesbo-France. COVID-19 and Dentistry in 72 Questions: An Overview of the Literature. J Clin Med. 2021 Feb 16;10(4):779.. [DOI:10.3390/jcm10040779] [PMID] [PMCID]
12. De Stefani A, Bruno G, Mutinelli S, Gracco A. COVID-19 Out-break Perception in Italian Dentists. Int J Environ Res Public Health. 2020 May 29;17(11):3867. [DOI:10.3390/ijerph17113867] [PMID] [PMCID]
13. Kamate SK, Sharma S, Thakar S, Srivastava D, Sengupta K, Hadi AJ, Chaudhary A, Joshi R, Dhanker K. Assessing Knowledge, Attitudes and Practices of dental practitioners regarding the COVID-19 pandemic: A multinational study. Dent Med Probl. 2020 Jan-Mar;57(1):11-7. [DOI:10.17219/dmp/119743] [PMID]
14. Bontà G, Campus G, Cagetti MG. COVID-19 pandemic and dental hygienists in Italy: a questionnaire survey. BMC Health Serv Res. 2020 Oct 31;20(1):994. [DOI:10.1186/s12913-020-05842-x] [PMID] [PMCID]
15. Quadri MFA, Jafer MA, Alqahtani AS, Al mutahar SAB, Odabi NI, Daghriri AA, et al. Novel corona virus disease (COVID-19) awareness among the dental interns, dental auxiliaries and den-tal specialists in Saudi Arabia: A nationwide study. J Infect Public Health. 2020;13(6):856-64. [DOI:10.1016/j.jiph.2020.05.010] [PMID] [PMCID]
16. Duruk G, Gümüşboğa ZŞ, Çolak C. Investigation of Turkish dentists' clinical attitudes and behaviors towards the COVID-19 pandemic: a survey study. Braz Oral Res. 2020;34:e054. [DOI:10.1590/1807-3107bor-2020.vol34.0054] [PMID]
17. Prati C, Pelliccioni GA, Sambri V, Chersoni S, Gandolfi MG. COVID-19: its impact on dental schools in Italy, clinical problems in endodontic therapy and general considerations. Int Endod J. 2020 May;53(5):723-5. [DOI:10.1111/iej.13291] [PMID] [PMCID]
18. Bazzazpour S, Rahmatinia M, Mohebbi SR, Hadei M, Shah-savani A, Hopke PK, Houshmand B, Raeisi A, Jafari AJ, Yarahmadi M, Farhadi M, Hasanzadeh V, Kermani M, Vaziri MH, Tanhaei M, Zali MR, Alipour MR. The detection of SARS-CoV-2 RNA in indoor air of dental clinics during the COVID-19 pandemic. Environ Sci Pollut Res Int. 2021 Aug 3:1-9. [DOI:10.1007/s11356-021-15607-6] [PMID] [PMCID]
19. Khader Y, Al Nsour M, Al-Batayneh OB, Saadeh R, Bashier H, Alfaqih M, Al-Azzam S, AlShurman BA. Dentists' Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study Among Jordanian Dentists. JMIR Public Health Surveill. 2020 Apr 9;6(2):e18798. [DOI:10.2196/18798] [PMID] [PMCID]
20. Sarkarat F, Tootoonchian A, Hosseinpour M , Moghadasi M , Rakhshan V. Knowledge of Iranian Dentists, Dental Specialists, and Dental Students Towards COVID-19: A Preliminary Survey of 778 Subjects. Shiraz E-Med J. 2020; 21 (12):e106515. [DOI:10.5812/semj.106515]
21. Widyarman AS, Bachtiar EW, Theodorea CF, Rizal MI, Roeslan MO, Djamil MS, Santosa DN, Bachtiar BM. COVID-19 Awareness Among Dental Professionals in Indonesia. Front Med (Lausanne). 2020 Nov 4;7:589759. [DOI:10.3389/fmed.2020.589759] [PMID] [PMCID]
22. Khan S, Khan M, Maqsood K, Hussain T, Noor-Ul-Huda, Zee-shan M. Is Pakistan prepared for the COVID-19 epidemic? A questionnaire-based survey. J Med Virol. 2020 Jul; 92(7): 824-32. [DOI:10.1002/jmv.25814] [PMID] [PMCID]
23. Naveed N, Thailavathy, Sabapathy K. Awareness of COVID-19 among dental students in Chennai, India- A questionnaire based study. Eur J Mol Clin Med. 2020;7(4): 1620-5.
24. Hleyhel M, Haddad C, Haidar N, Charbachy M, Saleh N. De-terminants of knowledge and prevention measures towards COVID-19 pandemic among Lebanese dentists: a cross sectional survey. BMC Oral Health. 2021 May 6;21(1): 241. [DOI:10.1186/s12903-021-01599-9] [PMID] [PMCID]
25. Askarian M, Mirzaei K, Honarvar B, Etminan M, Araujo MW. Knowledge, attitude and practice towards droplet and airborne isolation precautions among dental health care professionals in Shiraz, Iran. J Public Health Dent. 2005 Winter;65(1):43-7. [DOI:10.1111/j.1752-7325.2005.tb02785.x] [PMID]
26. Baseer MA, Ansari SH, AlShamrani SS, Alakras AR, Mahrous R, Alenazi AM. Awareness of droplet and airborne isolation precautions among dental health professionals during the out-break of corona virus infection in Riyadh city, Saudi Arabia. J Clin Exp Dent. 2016 Oct 1;8(4):e379-87. [DOI:10.4317/jced.52811] [PMID] [PMCID]
27. Pourfarrokh P, Kkermani M, Jamali J. Assessment of the level of Perception stress of students of Mashhad University of Medi-cal Sciences about COVID19 in 2020. Horizons Med Educ Dev. 2020;11(2):66-76.
28. Putrino A, Raso M, Magazzino C, Galluccio G. Coronavirus (COVID-19) in Italy: knowledge, management of patients and clinical experience of Italian dentists during the spread of conta-gion. BMC Oral Health. 2020 Jul 10;20(1):200. [DOI:10.1186/s12903-020-01187-3] [PMID] [PMCID]
29. Marui VC, Souto MLS, Rovai ES, Romito GA, Chambrone L, Pannuti CM. Efficacy of preprocedural mouthrinses in the reduc-tion of microorganisms in aerosol: A systematic review. J Am Dent Assoc. 2019 Dec;150(12):1015-26.e1. [DOI:10.1016/j.adaj.2019.06.024] [PMID]
30. Kohn WG, Collins AS, Cleveland JL, Harte JA, Eklund KJ, Mal-vitz DM; Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings--2003. MMWR Recomm Rep. 2003 Dec 19;52(RR-17):1-61. [DOI:10.14219/jada.archive.2004.0019] [PMID]
31. Yu J, Hua F, Shen Y, Haapasalo M, Qin D, Zhao D, Peng B, Fouad AF. Resumption of Endodontic Practices in COVID-19 Hardest-Hit Area of China: A Web-based Survey. J Endod. 2020 Nov;46(11):1577-83.e2. [DOI:10.1016/j.joen.2020.08.001] [PMID] [PMCID]
32. Samaranayake LP, Reid J, Evans D. The efficacy of rubber dam isolation in reducing atmospheric bacterial contamination. ASDC J Dent Child. 1989 Nov-Dec;56(6):442-4.
33. Sarkarat F, Tootoonchian A, Haraji A, Rastegarmoghaddam Shaldoozi H, Mostafavi M, Naghibi Sistani SMM. Evaluation of dentistry staff involvement with COVID-19 in the first 3 month of epidemiologic spreading in Iran. J Res Dent Sci. 2020;17(2):137-45. [DOI:10.29252/jrds.17.2.137]
34. Ahmadi H, Ebrahimi A, Ghorbani F. The impact of COVID-19 pandemic on dental practice in Iran: a questionnaire-based re-port. BMC Oral Health. 2020 Dec 3;20(1):354. [DOI:10.1186/s12903-020-01341-x] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |