

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-355-en.html



2- Department of Operative Dentistry, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran
3- Rheumatology Research Center, Razi Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
4- Department of Orthodontics, School of Dentistry, Tehran university of Medical Sciences, Tehran, Iran
5- Dental Sciences Research Center, Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran ,
|
Abstract |
Introduction
Sjogren’s syndrome is a chronic autoimmune disease, characterized by chronic infiltration of lymphocytes in exocrine glands particularly the lacrimal and salivary glands, and subsequent development of sicca syndrome.[1-4] The incidence of primary Sjogren’s syndrome is 6.92 per 100,000 population (95% CI:4.98-8.86). The prevalence of Sjogren’s syndrome is 60.82 per 100,000 population (95% CI: 43.69-77.94); this rate has been reported to be 43.03 per 100,000 population (25.74 to 60.31) in epidemiological studies.[2,3] The female to male ratio is 9.15 (95% CI: 3.35 to 13.18) for incidence and 10.72 (95% CI: 7.35 to 15.62) for prevalence of Sjogren’s syndrome. The mean age of patients with primary Sjogren’s yndrome is 56 years.[1,3,5,6]
Mouth dryness (xerostomia) and eye dryness are the main complaints of patients with Sjogren’s syndrome. Mouth dryness results in dental erosion, swelling of the salivary glands, and severe dental caries particularly cervical caries and caries at the cusp tips and incisal edges, which are hard to control.[7,8]
Initial diagnosis and screening of patients with Sjogren’s syndrome are challenging.[2,3,9] The diagnosis of Sjogren’s syndrome is mainly based on mouth dryness (determined by questioning the patient), measurement of salivary flow rate, and biopsy of minor salivary glands as well as counting of lymphocyte foci in the salivary glands. Circulatory antibodies (anti-Ro, anti-La, ANA, etc.) are valuable biomarkers as well.[10, 11]
At present, use of salivary diagnostic markers is preferred among the available diagnostic markers due to their easy accessibility, cost-effectiveness, and non-invasiveness; moreover, they often have optimal sensitivity and specificity. In general, salivary biomarkers are divided into three groups of (I) disease-specific biomarkers, (II) non-specific biomarkers, which show abnormal conditions and (III) biomarkers that show accidental differences between patients and controls.[12, 13] Changes in the quality and quantity of the saliva in patients with Sjogren’s syndrome evaluated by sialometry and sialo-chemistry have been among the main topics of research in the recent years.[4,13,14] Reduction of salivary flow rate to less than 0.1 mL/minute is considered pathological, and is among the most important changes that can be used for detection of patients with Sjogren’s syndrome. Changes in the composition of saliva in patients with Sjogren’s syndrome include increased levels of sodium, chloride, beta-2 microglobulin proteins, and matrix metalloproteinases. [12,15,16]
Calcium can be found in ionic form or bound to inorganic ions and proteins in the saliva, which enhances the mineralization of dental hard tissue. Changes in the calcium level of oral fluids surrounding enamel crystals affect enamel hydroxyapatite based on the degree of calcium saturation.[17-19] Saliva contains calcium and phosphate ions often in super-saturated state surrounding hydroxyapatite crystals. Since the pellicle is permeable, it allows the passage of ions; thus, remineralization of tooth structure can occur. An important characteristic of calcium is that its concentration is not different in stimulated and unstimulated saliva (in contrast to other elements), and always follows a gradient-free pattern. The concentration of calcium in the liquid phase is higher than in hydroxyapatite in dental enamel due to the lower pH of the liquid phase.[17,19] It has been hypothesized that calcium may serve as a simple and affordable biomarker for detection of Sjogren’s syndrome.[20] In case of presence of a significant association between the salivary level of calcium and Sjogren’s syndrome, salivary level of calcium may be used as a biomarker for detection of patients with Sjogren’s syndrome.
This study aimed to quantitatively assess the saliva and measure the salivary level of calcium in patients with Sjogren’s syndrome in comparison with healthy controls.
Materials and Methods
This case-control study was conducted on 30 patients with Sjogren’s syndrome and 30 age (±3 years) and sex-matched healthy controls. The study was conducted at the Rheumatology clinic and Research Center of Razi Hospital in Guilan University of Medical Sciences and School of Dentistry of Guilan University of Medical Sciences. All patients met the European-American Consensus Group criteria for classification of Sjogren’s syndrome.[10] The patients were selected from the hospital records and recalled for measurement of their salivary calcium level and salivary flow rate. The study protocol was approved by the committee of medical ethics of Guilan University of Medical Sciences (IR.GUMS.RES.1395.120). All procedures performed in the study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patients with a history of head and neck radiotherapy, hepatitis C, acquired immunodeficiency syndrome, sarcoidosis, graft versus host disease, or connective tissue diseases, those who took cholinergic drugs in the past 24 hours, cigarette smokers, professional athletes, those who took calcium tablets in the past week, or bromhexine or globin drop in the past 24 hours, patients using antidepressants, and those not consenting to participation in the study were all excluded.[21-23]
All patients signed written informed consent forms prior to participation in the study. Demographic information of patients was recorded through an interview and included age, sex, level of education, and frequency of tooth brushing. Underlying diseases, drugs taken, time of diagnosis, and duration of affliction were also recoded in a questionnaire.
Dental examination: Number of decayed (D), missed (M) and filled (F) tooth surfaces (DMFS) was recorded according to the World Health Organization criteria, and the total number of filled, decayed or lost tooth surfaces was calculated (D+M+F).[24] Saliva collection: The patients rinsed their mouth with deionized water, and saliva was collected using the spitting method.
Unstimulated saliva was collected in the morning (8-9 a.m.), and the patients were requested to brush their teeth prior to saliva collection. To prevent stimulation of saliva secretion, the patients were requested to refrain from eating and drinking for 90 minutes prior to saliva collection. Salivary flow rate was reported in milliliters per minute (mL/minute). The collected saliva was transferred to a laboratory in a cool box and was frozen in the laboratory. To prevent errors in measuring the salivary calcium level, all sampling instruments were acid-washed 3 hours prior to testing.[25] Laboratory procedures: Total salivary concentration of calcium was assessed by atomic absorption spectroscopy using Arsenazo III calcium-sensitive dye (BT3500 auto-analyzer, Bioteqniqua, Rome, Italy). The level of calcium was reported in milligrams per deciliter (mg/dL). The samples were frozen at -20°C in the laboratory. For the measurements, the samples were removed from the freezer and allowed to thaw to reach the room temperature. The samples were then centrifuged at 2000 g for 10 minutes. The supernatant was separated. The concentration of calcium was measured using a halogen lamp light source (340-740 nm). Calcium reacts with Arsenazo III calcium-sensitive dye in neutral environment and forms blue complexes. The concentration of calcium is determined by measuring the optical density of the solution.[26]
Data analysis: The collected data were entered into SPSS version 21. The Kolmogorov-Smirnov test, parametric independent t-test, and Mann Whitney U test were used to compare the variables between the two groups. The Pearson’s and the Spearman’s correlation coefficients were used to analyze the relationship between quantitative variables. The logistic regression model was used to compare the variables between the two groups while controlling for the effect of confounding variables. Considering the presence of significant differences in this regard between the two groups, the receiver operating characteristic (ROC) curve was drawn to determine a cutoff point for clinical application. The cutoff point was then analyzed based on measures of diagnostic accuracy including sensitivity, specificity, positive predictive value, and negative predictive value. Level of significance was set at P<0.05.
Results
This study was conducted on 60 individuals including 30 patients with Sjogren’s syndrome and 30 healthy controls. The mean age of patients and controls was 42±13.04 years and 43±10.65 years, respectively. Most patients (33%) were in the age range of 30-40 years.
The salivary level of calcium was 4.44±0.78 mg/dL in the case and 4.22±0.51 mg/dL in the control group (P=0.189, independent t-test). The salivary flow rate in the case group (0.12±0.07 mL/minute, range: 0.03 to 0.4 mL/minute) was significantly lower than that in the control group (0.4±0.14 mL/minute, range: 0.1 to 0.6 mL/minute) (P<0.000, Mann Whitney U test). The DMFS score in the case group (78.08±36.24) was significantly higher than that in the control group (38.35±23.02) (P<0.000, independent t-test).
The DMFS components were D=397, M=340 and F=413 surfaces in the control group and D=347, M=1015 and F=980 surfaces in the case group. The mean duration of disease was 6.8±5.5 years and the mean time to diagnosis was 2.4±1.9 years.
Figure 1 shows the coefficient of determination of salivary flow rate for development of caries based on the DMFS score according to which, R2 linear was found to be 0.340 (the Spearman’s correlation coefficient). Figure 2 shows the coefficient of determination of salivary calcium level for development of caries based on the DMFS score according to which, R2 linear was found to be 0.002 (the Pearson’s correlation coefficient). Figure 2 shows lack of a correlation between salivary calcium level and DMFS score. The association of the DMFS score and salivary flow rate was found to be significant (r= -0.583, P<0.000) such that 34% of the changes in DMFS score were correlated with the salivary flow rate (R2=0.34).
Figure 1. Coefficient of determination of salivary flow rate for development of caries based on DMFS score
.png){kind=link}
Figure 2. Correlations of salivary calcium level and DMFS score
.png){kind=link}
According to the linear regression model, for each 1 mL increase in the salivary flow rate, tooth decay decreased by 73.83% (118 scores).
In the control group, correlations existed between the salivary flow rate and DMFS score (r=-0.363, P=0.049), and DMFS score and age (r=0.514, P=0.004). Duration of disease in patients had an inverse borderline significant correlation with salivary flow rate (r=-0.353, P=0.055).
According to the Pearson’s correlation coefficient, no significant correlation was found between the salivary calcium level and DMFS score in patients with Sjogren’s syndrome (r=-0.236, P=0.210) while salivary flow rate had an inverse correlation with DMFS score (r=-0.289, P=0.122).
For further accuracy in calculating the coefficient of determination of salivary calcium level, the area under the ROC curve (AUC) was calculated to be 0.611±0.074, which was not statistically significant (P=0.139) and showed a low discriminating function (11.1%). Thus, the salivary calcium level cannot be a criterion for Sjogren’s syndrome.
However, the AUC for salivary flow rate in Sjogren’s syndrome was found to be 0.96±0.027, which was statistically significant (P<0.0001). With 95% CI=0.907-1, the discriminating function was found to be 46%. The best cut off point of salivary flow rate for Sjogren’s syndrome was 0.165 mL/minute (96.7% sensitivity and 90% specificity). Thus, reduction in salivary flow rate can be used as a criterion for Sjogren’s syndrome (Figure 3).
The ROC curve was used to calculate the AUC in order to analyze the effect of salivary flow rate on the mean DMFS score (Figure 4). The results showed this value to be 0.854±0.049, which was statistically significant (P<0.000). With 95% CI=0.907-1, the discriminating function was found to be 34%.
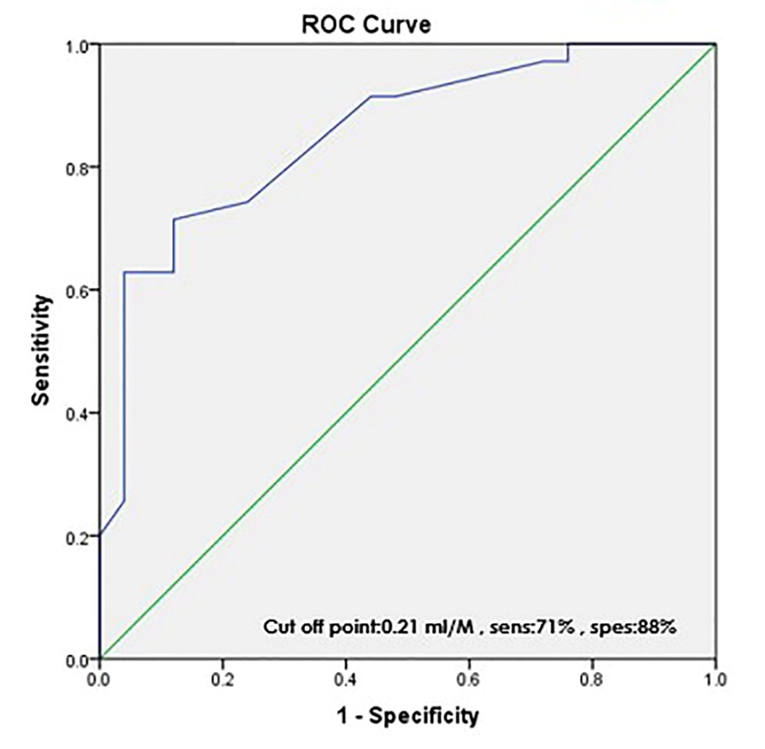
The ROC curve was also used to calculate the AUC in order to determine the effect of salivary calcium level on the mean DMFS (Figure 5).
Figure 3. Coefficient of determination of salivary flow rate (mL/minute) in Sjogren’s syndrome
{kind=link}
Figure 4. AUC for the effect of salivary flow rate (mL/minute) on DMFS score
{kind=link}
The results showed that the AUC was 0.666±0.075, which was not statistically significant (P=0.030).
According to the ROC curve, the qualitative effect of salivary flow rate on DMFS score was 85.0%; this value was 66.0% for the salivary calcium level. Thus, it can be concluded that the effect of salivary flow rate on DMFS score was1.5 times that of salivary calcium level.
Figure 5. AUC for the effect of salivary calcium level (mg/dL) on DMFS score
{kind=link}
ANCOVA was then performed to control for the effect of confounding variables and showed that the effect of salivary flow rate after controlling for the effect of salivary calcium level was significant in the two groups with an impact size of 0.706 (P=0.014) while no interaction was found for increased salivary calcium level when adjusting for the salivary flow rate in the two groups.
With regard to DMFS, ANCOVA showed that the effect of salivary flow rate and Sjogren’s syndrome on DMFS was significant while no interaction was noted between DMFS and salivary calcium level in the two groups.
Discussion
This study compared the salivary calcium level in patients with Sjogren’s syndrome and healthy controls. The results showed that although the salivary flow rate can be considered as a diagnostic criterion in Sjogren's syndrome (96.7% sensitivity and 90% specificity), salivary calcium level is not a suitable criterion for this purpose. Considering the ion exchange between oral fluids surrounding enamel hydroxyapatite crystals and the level of calcium on the basis of pH, the effect of salivary flow rate on DMFS was more prominent than that of salivary calcium level (71% sensitivity, 88% specificity). On the other hand, salivary calcium level may decrease in Sjögren patients as the salivary flow rate decreases.
At present, low salivary flow rate is an important criterion for primary and accurate classification of Sjogren’s syndrome. Previous studies have reported a certain limit of accuracy for xerostomia in Sjogren’s syndrome and stated that further precision can be achieved by tissue biopsy.[10-12] One valuable finding of the current study was that salivary flow rate less than 0.165 mL/minute (cutoff point) is an easily accessible criterion for Sjogren’s syndrome.
Reduction of salivary flow rate to 0.1 mL/minute (89.8% sensitivity and 74.3% specificity) is among the most important criteria for Sjogren’s syndrome, which is widely accepted by the American and European Associations of Rheumatologists. It has also shown the highest correlation with other tests such as anti-SSA and anti-SSB or FS≥1.[10-12] Another criterion is biopsy samples from minor salivary glands of the lips. Evidence suggests that biopsy is among the most accurate diagnostic criteria, and is widely accepted as the gold standard by oral medicine specialists. Systematic reviews have reported 63.9%-85.7% sensitivity and 89.7%-91.9% specificity for this method, yielding an optimal diagnostic accuracy.[11,27,28] It should be noted that presence of lymphocytic foci can also be part of the aging process not related to Sjogren’s syndrome.[14,29] In previous studies, surgeons and pathologists have questioned the feasibility of making a diagnosis based on histopathological findings. It has been argued that in presence of serological changes, the value of presence of lymphocytic foci is questionable. Also, there are disagreements on accurate diagnosis, scoring of foci, and histological changes in a tissue sample.
Moreover, inter- and intra-rater agreements may be low for pathologists, which is due to the use of different criteria for diagnosis and variable interpretations of scoring of foci. Thus, biopsy of the minor salivary glands of the lips can only serve as a gold standard of diagnosis for experienced and calibrated pathologists, who use the criteria with utmost precision.[14, 29-32] However, review of diagnostic criteria is among the most important challenges for pathologists. Surgical approaches, calibration of pathologist, requesting serological tests, and evidence of Sjogren’s syndrome make it difficult to reach a decision regarding easy use of this test as a diagnostic criterion. Therefore, measurement of salivary flow rate, which showed very high sensitivity in this study with a cutoff point of 0.165 mL/minute, is highly important as a main criterion for early patient detection. The cutoff point of salivary flow rate for detecting xerostomia has been reported to be 0.1 mL/minute. The cutoff point of salivary flow rate in Sjogren’s syndrome was found to be 0.165 mL/minute in the current study.
Although the above-mentioned two points almost match, it may be stated that measurement of salivary flow may have a higher diagnostic value than subjective questions regarding xerostomia; however, a diagnosis cannot be made until the patient reaches the cutoff point of xerostomia, which is > 0.1 mL/minute. This finding is completely in accordance with recent consensus on classification for primary Sjogren’s syndrome.[10,11] According to the results of current study, a patient with Sjogren’s syndrome may not feel mouth dryness at a cutoff point of 0.165 mL/minute.
It has been accepted that patients with Sjogren’s syndrome often complain of mouth or eye dryness and if Sjogren’s syndrome is suspected, laboratory tests are ordered (Figure 6). If the mouth dryness complaint matches the results of laboratory tests, salivary flow rate can be measured and then for final confirmation of diagnosis, biopsy of salivary glands may be required. In this process, the results of laboratory tests matching the reduction in salivary flow rate can indicate Sjogren’s syndrome even without histopathological confirmation of focal lymphocytic infiltration of salivary glands. It should be noted that antibody titers of patients with Sjogren’s syndrome are correlated with the degree of lymphocytic infiltration.[28,31-36]
Figure 6. Flowchart of patient complains and management
{kind=link}
Conclusion
The current study showed that the salivary calcium level was not a suitable biomarker for detection of Sjogren’s syndrome and its concentration played no significant role in predicting the occurrence of dental caries. However, the current results further highlighted the role of salivary flow rate in Sjogren’s syndrome with optimal sensitivity and specificity. Future studies are required on the use of salivary biomarkers as the classification criteria for Sjogren’s syndrome.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |