

Volume 4, Issue 2 (6-2019)
J Res Dent Maxillofac Sci 2019, 4(2): 12-18 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jalalian E, Banifatemeh A, Zarbakhsh A, Eskandari damaneh A, Hashemi E, Shariaty M. Comparison of the Effect of Two Different Abutment Diameters on Detorque Value Using Cyclic Loading and Thermocycling. J Res Dent Maxillofac Sci 2019; 4 (2) :12-18
URL: http://jrdms.dentaliau.ac.ir/article-1-251-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-251-en.html



1- Associate Professor, Prosthodontics Dept, Faculty of Dentistry, Tehran Medical Sciences
2- Postgraduate student, Prosthodontics Dept, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,a.banyfatemeh@gmail.com
3- Postgraduate student, Prosthodontics Dept, Faculty of Dentistry, Tehran Medical Sciences
2- Postgraduate student, Prosthodontics Dept, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,
3- Postgraduate student, Prosthodontics Dept, Faculty of Dentistry, Tehran Medical Sciences
Full-Text [PDF 331 kb]
(966 Downloads)
| Abstract (HTML) (3472 Views)
Abstract
Background and Aim: Screw loosening is a common problem with both screw-retained and cemented implant restorations. It is assumed that the abutment diameter affects detorque value and screw loosening. We aimed to determine the effect of two different abutment diameters on detorque value using cyclic loading and thermocycling.
Materials and Methods: This in-vitro experimental study was conducted on sixteen Morse-taper implants (4×10 mm) with two different diameters (3.9 and 5.2 mm) installed with a 25-Ncm torque (n=8). Eight screws from each group (3.9- and 5.2-mm abutments) were maintained for a month in a stable state while the rest of the screws underwent cyclic loading for 10,000 cycles with the frequency of 1 Hz and force of 75 N/cm. Then, thermocycling was done at 5-55°C. Detorque value was determined using the torque meter used for screw tightening. Removal torque values were recorded. Maximum deformation force and fracture resistance were documented. Data were analyzed according to Student's t-test using SPSS 21.0 software.
Results: Detorque values were 18.25±1.91 and 21.13±1.46 Ncm with 3.9- and 5.2-mm abutments, respectively. Detorque loss value was 15.50±5.83% with 5.2-mm abutment and 27±7.63% with 3.9-mm abutment. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm- compared to 5.2-mm-diameter abutments (P=0.004).
Conclusion: The results suggested that torque loss was lower with 5.2-mm abutment diameter.
Keywords: Dental Abutments, Diameter, Torque, Dental Implant loading, Fatigue
Introduction
Dental implants are used for tooth replacement in prosthodontic treatment; (1) however, some complications and failures have been reported. (2) The success of Implant treatment depends on biologic tissue response (soft tissues and bone) and the strength of the mechanical components (implant components and the superstructure). (2) There are numerous connection designs between the implant and abutment. The precise fit of the implant-abutment connection and the abutment screw preload are responsible for the success of implant rehabilitation. (3) The stress at the connection between the implant components could cause screw fracture as well as abutment and prosthesis damage, which require repair or replacement of the prosthesis and its components. (4)
Another essential aspect of prosthetic rehabilitation is the space available for a prosthetic crown. (5) Screw loosening is a common problem with both screw-retained and cemented implant restorations. (6) The stability of the retention screw is related to several factors including the geometrical shape, the format of the threads, fit of the prosthetic component, the frictional coefficient of the screw, and the speed and force of tightening. (7) Numerous complications may arise as a result of the loosening of abutment screws. Screw loosening may lead to fracture under load, causing long-term complications (8). The taper, height, and width of the abutment, the cement type, and abutment diameter influence treatment success. (7)
Researchers have expressed different views on the effect of different abutment diameters on screw loosening. (9) There is a correlation between abutment rotation and prosthetic screw loosening. (6) A wider abutment and the application of a torque driver to tighten the screws may help prevent this loosening. (8) Moris et al reported that a 3.8-mm-diameter abutment (reduced) has mechanical properties similar to that of 4.8-mm (conventional) abutments. (10) The implant diameter should be selected according to the depth and width of the residual alveolar bone, defect pattern, rehabilitation space, emergence profile, and occlusion. (11) Wide-diameter implants are mainly used with insufficient edentulous bone height or failure of osseointegration. (11) The misfit between the implant and abutment is one of the main factors for treatment failure. (12) Osseointegration and bone support maintenance are important for the success of dental implants. (13)
The presence of a microgap at the implant-abutment interface allows microorganisms to penetrate and colonize the inner part of the implant. (13) The presence of microorganisms in peri-implant tissues leads to inflammatory response, biofilm accumulation, and progressive bone loss. (14) The abutment diameter can influence the mechanical behavior and provide higher compressive resistance. (11) Despite numerous reports on the effect of the implant-abutment connection on screw loosing, the information on the effect of different abutment diameters on detorque value and screw loosing is limited. Therefore, the current study aimed to determine the effect of two different abutment diameters on detorque value using cyclic loading and thermocycling.
Materials and Methods
This in-vitro experimental study was conducted on sixteen Morse-taper implants (4×10 mm, Lazak, Prague, Czech Republic) with two different abutment diameters (3.9 and 5.2 mm) and with 3-mm gingival height (Figure 1).
Figure 1: Abutments with two different diameters (3.9 mm and 5.2 mm)
Each group included 8 fixtures and 8 straight abutments (n=8). The implants were wrapped in thin layers of radiographic film lead to prevent acrylic resin entrapment in implant threads and to allow effortless removal of the acryl from the implants after cyclic loading. Autopolymerized acrylic resin (Meliodent, Heraeus-Kulzer GmbH, Wehrheim, Germany) was poured inside the mold to 1 mm below the implant-abutment interface at a 90-degree angle using a surveyor (J.M. Ney Co., Bloomfield, CT, USA). When the load is applied at an angle of 30 degrees, it is subdivided into horizontal and vertical components such that the load is applied along both horizontal and vertical axes, similar to the load during mastication. (15)
Next, the abutments (3.9 and 5.2 mm) were installed into the implants with a 25-Ncm torque as recommended by the manufacturer. The torque was measured using a digital torque meter (Lutron Electronic Enterprise Co., Ltd., Taiwan; Figure 2).
Figure 2: Digital torque meter (Lutron Electronic Enterprise Co. Ltd., Taiwan)
The abutments were torqued to 25 Ncm and retorqued to 25 Ncm 10 minutes later for final prosthesis insertion appointment as recommended by the manufacturer. (12) Eight screws in each group were maintained for a month in a stable state while the rest of the screws underwent cyclic loading (Chewing simulator, SD Mechatronic, Feldkirchen, Westerham, Germany) for 10,000 cycles with the frequency of 1 Hz and force of 75 N/cm at a 30-degree angle, which is equal to occlusion loads exerted on a natural tooth for 20 months (Figures 3 and 4).
Figure 3: Applying a 75-N force on abutments with 1-Hz frequency at a 30-degree angle
Figure 4: Cyclic loading device
Thermocycling (model MSCT-3, Marcelo Nucci-Me, São Carlos, SP, Brazil) was done at 5-55°C. Next, the detorque value was determined using the torque meter that was used for tightening the screws. Finally, the removal torque values were recorded. (16) The values of maximum deformation force and fracture resistance were recorded as well. Data were analyzed by Student's t-test using SPSS software (version 21.0, SPSS Inc., Chicago, IL, USA).
Results
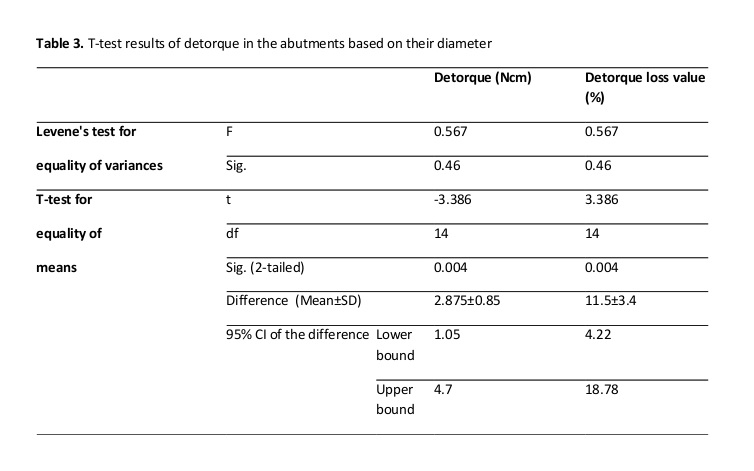
To analyze the statistical data according to the research objectives, Kolmogorov-Smirnov test was used to examine the normal distribution of data. According to Table 1, both 2.5- and 3.9-mm diameters are normally distributed. Parametric t-tests can be used to compare the mean of these two variables in the studied diameters. As seen in Table 2, the detorque values with 3.9- and 5.2-mm abutments were 18.25±1.91 Ncm and 21.13±1.46 Ncm, respectively. Also, detorque loss values with 3.9- and 5.2-mm abutments were 27.00±7.63% and 15.50±5.83%, respectively. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm-diameter abutments compared to the 5.2-mm-diameter abutments (P=0.004; Table 3).
Table 1. Kolmogorov-Smirnov test results
Table 2. Mean±standard deviation (SD) of detorque in the abutments based on their diameter
Table 3. T-test results of detorque in the abutments based on their diameter
Discussion
Abutment screw loosening is the main complication in implant-supported prostheses. Finding an approach to improve the retention and stability of the abutment screw was the main purpose of this study. To achieve this goal, we carried out this study to determine the effect of 3.9- and 5.2-mm abutment diameters on detorque value using cyclic loading and thermocycling. According to the findings of the current study, the detorque values with 3.9- and 5.2-mm-diameter abutments were 18.25±1.91 Ncm and 21.13±1.46 Ncm, respectively. Detorque loss value was 15.50±5.83% with 5.2-mm abutment and 27±7.63% with the 3.9-mm-diameter abutment. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm compared to the 5.2-mm-diameter abutments.
In a similar study, Moris et al reported that the 3.8-mm-diameter abutment had mechanical properties similar to that of 4.8-mm abutments, (10) which is different from our result. In another study that compared the fracture resistance of internal hexagon and Morse-taper connections, it was concluded that Morse-taper connection provides greater resistance to deformation and fracture compared to the internal hexagon. (17) Jalalian et al studied the effect of abutment connection type and cyclic loading on removal torque value and showed that the internal connection, irrespective of cyclic loading, was superior to the external connection, and cyclic loading decreased the torque value in all cases. (18) Also, de Sá et al studied the fracture strength of prosthetic abutments with different sizes and combinations, which supported a five-implant milled framework with distal extension. (19) Prosthetic abutments with different dimensions (4.8-mm-diameter mini-conical abutments and 3.5-mm-diameter micro-conical abutments) were used. They reported that the combination of standard- and small-diameter abutments leads to fractured prosthetic screws with lower fracture strength compared to standard-sized prosthetic abutments. (19)
There are two main regions of load concentration on screws, which could ultimately lead to fracture. The first region is between the screw head and screw stem, and the second region is located at the first screw thread. (20) The average maximum occlusal load recorded in the literature is 723 N on the second molar region; implants must resist this force. (19) Thermocycling may simulate the clinical situation more appropriately. (21) The effect of thermal cycling on marginal leakage depends on the thermal conductivity and coefficients of thermal expansion of the materials used. (22) On the influence of abutment size (1, 2, and 3 mm) and fixation screws on dental implant system, Mao et al reported that the diameter of the fixation screw should not be smaller than 1 mm, and unilateral wall thickness > 0.5 mm is optimal for abutments. (9) Lillo et al studied the compressive resistance of abutments with different diameters and transmucosal heights (4.5×2.5 mm, 4.5×3.5 mm, 3.3×2.5 mm, and 3.3×3.5 mm) in Morse-taper implants and reported stronger mechanical behavior and compressive resistance with 4.5-mm-diameter abutments; (11) our results were in agreement with this report. A higher stress concentration may be observed at the junction between the implant’s internal neck region and the abutment without damage of the implant threads in Morse-taper implants. (22)
Considering that the incisor region presents maximum bite force, ranging between 150 and 180 N, all the abutments used in this study could be used clinically without deformation. The aforementioned implant systems that are currently used in clinical practice have various connection types, fixture diameters, abutments, and abutment screws. Unfortunately, studies on the effect of such factors on the stability of the connection part associated with screw loosening are scarce. The implant diameter must be chosen by considering the teeth defect pattern, the depth and width of the residual alveolar bone, rehabilitation space, emergence profile, and occlusion. (11) The abutment’s diameter seems to influence the mechanical behavior related to permanent deformation, providing a higher compressive resistance in 5.2-mm-diameter abutments.
Gross et al reported that the microgap between the implant and abutment can provide a path for fluids and macromolecules generated from the saliva or the gingival crevicular fluid (GCF). (23) Microleakage can cause screw loosening followed by a decrease in detorque value. Cyclic loading of implant-supported prostheses may result in micromovements and fatigue of the metal in seemingly stable screwed prostheses. Also, screw joints on implants with low preload values exhibit significantly higher micromovements at the abutment-implant interface. (11)
Dixon et al reported the lack of influence of torque reduction after mechanical cycling on the implant-abutment connection. (24) In their study on thirty-six 4.1-mm-diameter implants with their matching RC platform Straumann abutments with constant-load amplitude fatigue lifetime testing at two frequencies (2 Hz and 15 Hz) with a stress ratio of 0.1 with lifetime ranging from 20,000 to 1,000,000 cycles, Duan and Griggs showed that there was no significant difference in lifetime and failure mode between 2 Hz and 15 Hz groups for this implant system. (25)
On the other hand, Arshad et al evaluated the effect of repeated screw joint closing and opening cycles and cyclic loading on abutment screw removal torque. (26) They concluded that using a new screw could not significantly increase the removal torque. They suggested that restricting the amount of screw tightening is more important than replacing the screw with a new one when an abutment is definitively placed. (26) Cibirka et al also observed preload reduction and screw joint stability after mechanical cycling. (27) Al-Turki et al evaluated implant-supported fixed prostheses under cyclic loading with a 298-N force at 1 Hz for 48 hours to simulate 144 days of function. (28) The results suggested that torque loss was lower with 5.2-mm abutment diameter. (28) The forces that led to permanent deformation of the abutment connections were dependent on the implant diameter. The differences between the implants used in this study were obvious, both macroscopically and microscopically.
Applying the correct amount of torque using a torque wrench is very important. In this study, 25 Ncm (manufacturer’s recommendation) was applied for a constant clamping torque (8). Ten minutes later, the same tightening torque was applied repeatedly to compensate for the loss of preload (8). To minimize the decrease in preload by surface settling, the tightening force should be reapplied 10 minutes after the first screw tightening. Al-Turki et al also stated that the tightening torque should be applied regularly and repetitively to compensate for the settling effect of the surface. (28)
Full-Text: (1393 Views)
Abstract
Background and Aim: Screw loosening is a common problem with both screw-retained and cemented implant restorations. It is assumed that the abutment diameter affects detorque value and screw loosening. We aimed to determine the effect of two different abutment diameters on detorque value using cyclic loading and thermocycling.
Materials and Methods: This in-vitro experimental study was conducted on sixteen Morse-taper implants (4×10 mm) with two different diameters (3.9 and 5.2 mm) installed with a 25-Ncm torque (n=8). Eight screws from each group (3.9- and 5.2-mm abutments) were maintained for a month in a stable state while the rest of the screws underwent cyclic loading for 10,000 cycles with the frequency of 1 Hz and force of 75 N/cm. Then, thermocycling was done at 5-55°C. Detorque value was determined using the torque meter used for screw tightening. Removal torque values were recorded. Maximum deformation force and fracture resistance were documented. Data were analyzed according to Student's t-test using SPSS 21.0 software.
Results: Detorque values were 18.25±1.91 and 21.13±1.46 Ncm with 3.9- and 5.2-mm abutments, respectively. Detorque loss value was 15.50±5.83% with 5.2-mm abutment and 27±7.63% with 3.9-mm abutment. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm- compared to 5.2-mm-diameter abutments (P=0.004).
Conclusion: The results suggested that torque loss was lower with 5.2-mm abutment diameter.
Keywords: Dental Abutments, Diameter, Torque, Dental Implant loading, Fatigue
Introduction
Dental implants are used for tooth replacement in prosthodontic treatment; (1) however, some complications and failures have been reported. (2) The success of Implant treatment depends on biologic tissue response (soft tissues and bone) and the strength of the mechanical components (implant components and the superstructure). (2) There are numerous connection designs between the implant and abutment. The precise fit of the implant-abutment connection and the abutment screw preload are responsible for the success of implant rehabilitation. (3) The stress at the connection between the implant components could cause screw fracture as well as abutment and prosthesis damage, which require repair or replacement of the prosthesis and its components. (4)
Another essential aspect of prosthetic rehabilitation is the space available for a prosthetic crown. (5) Screw loosening is a common problem with both screw-retained and cemented implant restorations. (6) The stability of the retention screw is related to several factors including the geometrical shape, the format of the threads, fit of the prosthetic component, the frictional coefficient of the screw, and the speed and force of tightening. (7) Numerous complications may arise as a result of the loosening of abutment screws. Screw loosening may lead to fracture under load, causing long-term complications (8). The taper, height, and width of the abutment, the cement type, and abutment diameter influence treatment success. (7)
Researchers have expressed different views on the effect of different abutment diameters on screw loosening. (9) There is a correlation between abutment rotation and prosthetic screw loosening. (6) A wider abutment and the application of a torque driver to tighten the screws may help prevent this loosening. (8) Moris et al reported that a 3.8-mm-diameter abutment (reduced) has mechanical properties similar to that of 4.8-mm (conventional) abutments. (10) The implant diameter should be selected according to the depth and width of the residual alveolar bone, defect pattern, rehabilitation space, emergence profile, and occlusion. (11) Wide-diameter implants are mainly used with insufficient edentulous bone height or failure of osseointegration. (11) The misfit between the implant and abutment is one of the main factors for treatment failure. (12) Osseointegration and bone support maintenance are important for the success of dental implants. (13)
The presence of a microgap at the implant-abutment interface allows microorganisms to penetrate and colonize the inner part of the implant. (13) The presence of microorganisms in peri-implant tissues leads to inflammatory response, biofilm accumulation, and progressive bone loss. (14) The abutment diameter can influence the mechanical behavior and provide higher compressive resistance. (11) Despite numerous reports on the effect of the implant-abutment connection on screw loosing, the information on the effect of different abutment diameters on detorque value and screw loosing is limited. Therefore, the current study aimed to determine the effect of two different abutment diameters on detorque value using cyclic loading and thermocycling.
Materials and Methods
This in-vitro experimental study was conducted on sixteen Morse-taper implants (4×10 mm, Lazak, Prague, Czech Republic) with two different abutment diameters (3.9 and 5.2 mm) and with 3-mm gingival height (Figure 1).
Figure 1: Abutments with two different diameters (3.9 mm and 5.2 mm)
.jpg){kind=link}
Each group included 8 fixtures and 8 straight abutments (n=8). The implants were wrapped in thin layers of radiographic film lead to prevent acrylic resin entrapment in implant threads and to allow effortless removal of the acryl from the implants after cyclic loading. Autopolymerized acrylic resin (Meliodent, Heraeus-Kulzer GmbH, Wehrheim, Germany) was poured inside the mold to 1 mm below the implant-abutment interface at a 90-degree angle using a surveyor (J.M. Ney Co., Bloomfield, CT, USA). When the load is applied at an angle of 30 degrees, it is subdivided into horizontal and vertical components such that the load is applied along both horizontal and vertical axes, similar to the load during mastication. (15)
Next, the abutments (3.9 and 5.2 mm) were installed into the implants with a 25-Ncm torque as recommended by the manufacturer. The torque was measured using a digital torque meter (Lutron Electronic Enterprise Co., Ltd., Taiwan; Figure 2).
Figure 2: Digital torque meter (Lutron Electronic Enterprise Co. Ltd., Taiwan)
{kind=link}
The abutments were torqued to 25 Ncm and retorqued to 25 Ncm 10 minutes later for final prosthesis insertion appointment as recommended by the manufacturer. (12) Eight screws in each group were maintained for a month in a stable state while the rest of the screws underwent cyclic loading (Chewing simulator, SD Mechatronic, Feldkirchen, Westerham, Germany) for 10,000 cycles with the frequency of 1 Hz and force of 75 N/cm at a 30-degree angle, which is equal to occlusion loads exerted on a natural tooth for 20 months (Figures 3 and 4).
Figure 3: Applying a 75-N force on abutments with 1-Hz frequency at a 30-degree angle
.jpg){kind=link}
Figure 4: Cyclic loading device
.jpg){kind=link}
Thermocycling (model MSCT-3, Marcelo Nucci-Me, São Carlos, SP, Brazil) was done at 5-55°C. Next, the detorque value was determined using the torque meter that was used for tightening the screws. Finally, the removal torque values were recorded. (16) The values of maximum deformation force and fracture resistance were recorded as well. Data were analyzed by Student's t-test using SPSS software (version 21.0, SPSS Inc., Chicago, IL, USA).
Results
To analyze the statistical data according to the research objectives, Kolmogorov-Smirnov test was used to examine the normal distribution of data. According to Table 1, both 2.5- and 3.9-mm diameters are normally distributed. Parametric t-tests can be used to compare the mean of these two variables in the studied diameters. As seen in Table 2, the detorque values with 3.9- and 5.2-mm abutments were 18.25±1.91 Ncm and 21.13±1.46 Ncm, respectively. Also, detorque loss values with 3.9- and 5.2-mm abutments were 27.00±7.63% and 15.50±5.83%, respectively. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm-diameter abutments compared to the 5.2-mm-diameter abutments (P=0.004; Table 3).
Table 1. Kolmogorov-Smirnov test results
{kind=link}
Table 2. Mean±standard deviation (SD) of detorque in the abutments based on their diameter
{kind=link}
Table 3. T-test results of detorque in the abutments based on their diameter
{kind=link}
Discussion
Abutment screw loosening is the main complication in implant-supported prostheses. Finding an approach to improve the retention and stability of the abutment screw was the main purpose of this study. To achieve this goal, we carried out this study to determine the effect of 3.9- and 5.2-mm abutment diameters on detorque value using cyclic loading and thermocycling. According to the findings of the current study, the detorque values with 3.9- and 5.2-mm-diameter abutments were 18.25±1.91 Ncm and 21.13±1.46 Ncm, respectively. Detorque loss value was 15.50±5.83% with 5.2-mm abutment and 27±7.63% with the 3.9-mm-diameter abutment. The mean difference between the two abutment diameters was 2.87±0.85 Ncm. Significant differences were observed on torque loss with 3.9-mm compared to the 5.2-mm-diameter abutments.
In a similar study, Moris et al reported that the 3.8-mm-diameter abutment had mechanical properties similar to that of 4.8-mm abutments, (10) which is different from our result. In another study that compared the fracture resistance of internal hexagon and Morse-taper connections, it was concluded that Morse-taper connection provides greater resistance to deformation and fracture compared to the internal hexagon. (17) Jalalian et al studied the effect of abutment connection type and cyclic loading on removal torque value and showed that the internal connection, irrespective of cyclic loading, was superior to the external connection, and cyclic loading decreased the torque value in all cases. (18) Also, de Sá et al studied the fracture strength of prosthetic abutments with different sizes and combinations, which supported a five-implant milled framework with distal extension. (19) Prosthetic abutments with different dimensions (4.8-mm-diameter mini-conical abutments and 3.5-mm-diameter micro-conical abutments) were used. They reported that the combination of standard- and small-diameter abutments leads to fractured prosthetic screws with lower fracture strength compared to standard-sized prosthetic abutments. (19)
There are two main regions of load concentration on screws, which could ultimately lead to fracture. The first region is between the screw head and screw stem, and the second region is located at the first screw thread. (20) The average maximum occlusal load recorded in the literature is 723 N on the second molar region; implants must resist this force. (19) Thermocycling may simulate the clinical situation more appropriately. (21) The effect of thermal cycling on marginal leakage depends on the thermal conductivity and coefficients of thermal expansion of the materials used. (22) On the influence of abutment size (1, 2, and 3 mm) and fixation screws on dental implant system, Mao et al reported that the diameter of the fixation screw should not be smaller than 1 mm, and unilateral wall thickness > 0.5 mm is optimal for abutments. (9) Lillo et al studied the compressive resistance of abutments with different diameters and transmucosal heights (4.5×2.5 mm, 4.5×3.5 mm, 3.3×2.5 mm, and 3.3×3.5 mm) in Morse-taper implants and reported stronger mechanical behavior and compressive resistance with 4.5-mm-diameter abutments; (11) our results were in agreement with this report. A higher stress concentration may be observed at the junction between the implant’s internal neck region and the abutment without damage of the implant threads in Morse-taper implants. (22)
Considering that the incisor region presents maximum bite force, ranging between 150 and 180 N, all the abutments used in this study could be used clinically without deformation. The aforementioned implant systems that are currently used in clinical practice have various connection types, fixture diameters, abutments, and abutment screws. Unfortunately, studies on the effect of such factors on the stability of the connection part associated with screw loosening are scarce. The implant diameter must be chosen by considering the teeth defect pattern, the depth and width of the residual alveolar bone, rehabilitation space, emergence profile, and occlusion. (11) The abutment’s diameter seems to influence the mechanical behavior related to permanent deformation, providing a higher compressive resistance in 5.2-mm-diameter abutments.
Gross et al reported that the microgap between the implant and abutment can provide a path for fluids and macromolecules generated from the saliva or the gingival crevicular fluid (GCF). (23) Microleakage can cause screw loosening followed by a decrease in detorque value. Cyclic loading of implant-supported prostheses may result in micromovements and fatigue of the metal in seemingly stable screwed prostheses. Also, screw joints on implants with low preload values exhibit significantly higher micromovements at the abutment-implant interface. (11)
Dixon et al reported the lack of influence of torque reduction after mechanical cycling on the implant-abutment connection. (24) In their study on thirty-six 4.1-mm-diameter implants with their matching RC platform Straumann abutments with constant-load amplitude fatigue lifetime testing at two frequencies (2 Hz and 15 Hz) with a stress ratio of 0.1 with lifetime ranging from 20,000 to 1,000,000 cycles, Duan and Griggs showed that there was no significant difference in lifetime and failure mode between 2 Hz and 15 Hz groups for this implant system. (25)
On the other hand, Arshad et al evaluated the effect of repeated screw joint closing and opening cycles and cyclic loading on abutment screw removal torque. (26) They concluded that using a new screw could not significantly increase the removal torque. They suggested that restricting the amount of screw tightening is more important than replacing the screw with a new one when an abutment is definitively placed. (26) Cibirka et al also observed preload reduction and screw joint stability after mechanical cycling. (27) Al-Turki et al evaluated implant-supported fixed prostheses under cyclic loading with a 298-N force at 1 Hz for 48 hours to simulate 144 days of function. (28) The results suggested that torque loss was lower with 5.2-mm abutment diameter. (28) The forces that led to permanent deformation of the abutment connections were dependent on the implant diameter. The differences between the implants used in this study were obvious, both macroscopically and microscopically.
Applying the correct amount of torque using a torque wrench is very important. In this study, 25 Ncm (manufacturer’s recommendation) was applied for a constant clamping torque (8). Ten minutes later, the same tightening torque was applied repeatedly to compensate for the loss of preload (8). To minimize the decrease in preload by surface settling, the tightening force should be reapplied 10 minutes after the first screw tightening. Al-Turki et al also stated that the tightening torque should be applied regularly and repetitively to compensate for the settling effect of the surface. (28)
Type of Study: Original article |
Subject:
Dental implant
References
1. Chaar MS, Att JR, Strub JR. Prosthetic outcome of cement-retained implant-supported fixed dental restorations: a systematic review. J Oral Rehabil. 2011;38:697-711. [DOI:10.1111/j.1365-2842.2011.02209.x] [PMID]
2. Rismanchian M, Hatami M, Badrian H, Khalighinejad N, Goroohi H. Evaluation of microgap size and microbial leakage in the connection area of 4 abutments with Straumann (ITI) implant. J Oral Implantol. 2012;38(6):677-85. [DOI:10.1563/AAID-JOI-D-11-00167] [PMID]
3. Assunção WG, Barão VA, Delben JA, Gomes ÉA, Garcia IR Jr. Effect of unilateral misfit on preload of retention screws of implant-supported prostheses submitted to mechanical cycling. J Prosthodont Res. 2011;55(1):12-8. [DOI:10.1016/j.jpor.2010.05.002] [PMID]
4. Lorenzoni FC, Coelho PG, Bonfante G, Carvalho RM, Silva NR, Suzuki M, et al. Sealing capability and SEM observation of the implant-abutment interface. Int J Dent. 2011;2011:864183. [DOI:10.1155/2011/864183] [PMID] [PMCID]
5. Shin HM, Huh JB, Yun MJ, Jeon YC, Chang B, Chang M. Influence of the implant-abutment connection design and diameter on the screw joint stability. Adv Prosthodont. 2014;6(2):126-32. [DOI:10.4047/jap.2014.6.2.126] [PMID] [PMCID]
6. Bhering CL, Takahashi JM, Luthi LF, Henriques GE, Consani RL, Mesquita MF. Influence of the casting technique and dynamic loading on screw detorque and misfit of single unit implant-supported prostheses. Acta Odontol Scand. 2013 May-Jul;71(3-4):404-9. [DOI:10.3109/00016357.2012.690528] [PMID]
7. Sahin C, Ayyildiz S. Correlation between microleakage and screw loosening at implant-abutment connection. J Adv Prosthodont. 2014;6(1):35-8. [DOI:10.4047/jap.2014.6.1.35] [PMID] [PMCID]
8. Kim ES, Shin SY. Influence of the implant abutment types and the dynamic loading on initial screw loosening. J Adv Prosthodont. 2013 Feb;5(1):21-8.. [DOI:10.4047/jap.2013.5.1.21] [PMID] [PMCID]
9. Mao Z, Yi D, Cao G. Influence of sizes of abutments and fixation screws on dental implant system: a non-linear finite element analysis. Biomed Tech (Berl). 2017 Aug 28;62(4):357-64. [DOI:10.1515/bmt-2015-0074] [PMID]
10. Moris IC, Faria AC, de Mattos Mda G, Ribeiro RF, Rodrigues RC. Mechanical analysis of conventional and small diameter conical implant abutments. J Adv Prosthodont. 2012 Aug;4(3):158-61. [DOI:10.4047/jap.2012.4.3.158] [PMID] [PMCID]
11. Lillo R, Parra C, Fuentes R, Borie E, Engelke W, Beltrán V. Compressive resistance of abutments with different diameters and transmucosal heights in Morse-taper implants. Braz Dent J. 2015 Mar-Apr;26(2):156-9. [DOI:10.1590/0103-6440201300221] [PMID]
12. Junqueira MC, Ribeiro RF, Faria ACL, Macedo AP, Almeida RP. Screw loosening of different UCLA-type abutments after mechanical cycling. Braz J Oral Sci. 2013;12(3):228-32. [DOI:10.1590/S1677-32252013000300014]
13. Torres JH, Mechali M, Romieu O, Tramini P, Callas S, Cuisinier FJ, et al. Development of a new quantitative gas permeability method for dental implant-abutment connection tightness assessment. Biomed Eng Online. 2011 Apr 14;10:28. [DOI:10.1186/1475-925X-10-28] [PMID] [PMCID]
14. Harder S, Dimaczek B, Açil Y, Terheyden H, Freitag-Wolf S, Kern M. Molecular leakage at implant-abutment connection--in vitro investigation of tightness of internal conical implant-abutment connections against endotoxin penetration. Clin Oral Investig. 2010;14(4):427-32. [DOI:10.1007/s00784-009-0317-x] [PMID]
15. Cho SC, Small PN, Elian N, Tarnow D. Screw loosening for standard and wide diameter implants in partially edentulous cases: 3- to 7-year longitudinal data. Implant Dent. 2004 Sep;13(3):245-50. [DOI:10.1097/01.id.0000140459.87333.f8] [PMID]
16. Arshad M, Shirani G, Refoua S, Rahimi Yeganeh M. Comparative study of abutment screw loosening with or without adhesive material. J Adv Prosthodont. 2017 Apr;9(2):99-103. [DOI:10.4047/jap.2017.9.2.99] [PMID] [PMCID]
17. Perriard J, Wiskott WA, Mellal A, Scherrer SS, Botsis J, Belser UC. Fatigue resistance of ITI implant-abutment connectors - a comparison of the standard cone with a novel internally keyed design. Clin Oral Implants Res. 2002 Oct;13(5):542-9. [DOI:10.1034/j.1600-0501.2002.130515.x] [PMID]
18. Jalalian E, Hashemi E, Naser Mostufi SH, Banifatemeh AR, Shariati M, Pirmoazen A, et al. Effect of Abutment Connection Type and Cyclic Loading on Removal Torque Value. J Res Dentomaxillofac Sci. 2019;4(1):36-40. [DOI:10.29252/jrdms.4.1.36]
19. de Sá BCM, Andrighetto AR, Bernardes SR, Tiossi R. Fracture Strength of Standard and Small Diameter Prosthetic Abutments for Full-Arch Implant-Supported Restorations. J Oral Implantol. 2017 Jun;43(3):175-9. [DOI:10.1563/aaid-joi-D-16-00108] [PMID]
20. Choi KS, Lozada JL, Kan JY, Lee SH, Kim CS, Kwon TG. Study of an experimental microthreaded scalloped implant design: proximal bone healing at different interimplant distances in a canine model. Int J Oral Maxillofac Implants. 2010;25:681-9.
21. Zeno HA, Buitrago RL, Sternberger SS, Patt ME, Tovar N, Coelho P, et al. The effect of tissue entrapment on screw loosening at the implant/abutment interface of external- and internal-connection implants: An in vitro study. J Prosthodont. 2016 Apr;25(3):216-23. [DOI:10.1111/jopr.12329] [PMID]
22. Cho WR, Huh YH, Park CJ, Cho LR. Effect of cyclic loading and retightening on reverse torque value in external and internal implants. J Adv Prosthodont. 2015 Aug;7(4):288-293. [DOI:10.4047/jap.2015.7.4.288] [PMID] [PMCID]
23. Gross M, Abramovich I, Weiss EI. Microleakage at the abutment- implant interface of osseointegrated implants: a comparative study. Int J Oral Maxillofac Implants. 1999 Jan-Feb;14(1):94-100.
24. Dixon DL, Breeding LC, Sadler JP, McKay ML. Comparison of screw loosening, rotation, and deflection among three implant designs. J Prosthet Dent. 1995 Sep;74(3):270-8. [DOI:10.1016/S0022-3913(05)80134-9]
25. Duan Y, Griggs JA. Effect of loading frequency on cyclic fatigue lifetime of a standard-diameter implant with an internal abutment connection. Dent Mater. 2018 Dec;34(12):1711-6. [DOI:10.1016/j.dental.2018.09.001] [PMID]
26. Arshad M, Mahgoli H, Payaminia L. Effect of Repeated Screw Joint Closing and Opening Cycles and Cyclic Loading on Abutment Screw Removal Torque and Screw Thread Morphology: Scanning Electron Microscopy Evaluation. Int J Oral Maxillofac Implants. 2018 Jan/Feb;33(1):31-40. [DOI:10.11607/jomi.5476] [PMID]
27. Cibirka RM, Nelson SK, Lang BR, Rueggeberg FA. Examination of the implant-abutment interface after fatigue testing. J Prosthet Dent. 2001 Mar;85(3):268-75. [DOI:10.1067/mpr.2001.114266] [PMID]
28. Al-Turki LE, Chai J, Lautenschlager EP, Hutten MC. Changes in prosthetic screw stability because of misfit of implant-supported prostheses. Int J Prosthodont. 2002 Jan-Feb;15(1):38-42.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
