


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-249-en.html



2- Assistant professor, Prosthodontics Dept, Member of implant research center, Dental Faculty, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Faculty member of Thalasemia Research center, Mazandaran ,Iran
4- Dentist
5- Postgraduate student, Oral and maxillofacial surgery Dept, Dental Faculty, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
6- Assistant professor, Dental Implant Research Center, Dental Faculty, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran , taherehbitaraf@yahoo.com
Abstract
Background and Aim: Formation of microgaps between the fixture and abutment surfaces is still one of the major problems that may lead to mechanical and biological failure and inflammation around the implant. In this study, the effect of GapSeal on the prevention of liquid leakage and microgap in internal hex connection was investigated.
Materials and Methods: In this experimental study, sixteen internal hex implants (BioHorizons) were used in two groups. All implant-abutment assemblies were mounted in acrylic molds. GapSeal was inserted into the implants in the case group. All specimens were given a torque of 30 Ncm. Then, 1,200,000 cycles with a 100-N force and frequency of 1 Hz were applied to all samples. The samples were immersed in a methylene blue solution for microleakage evaluation. Microgap was randomly measured at six areas using scanning electron microscopy (SEM). Data were analyzed by SPSS 22 software using t-test.
Results: The size of microgap was 3.04±0.54 µm in the control group and 0.99±0.39 µm in the case group, which was three times larger in the control group; the t-test showed that this difference was significant (P<0.000). In the control group, all samples (100%) showed leakage in the internal hex connection while in the case group, none of the samples (0%) showed leakage; Fischer's exact test showed that the difference was statistically significant (P<0.0001).
Conclusion: According to the results of this study, it can be concluded that GapSeal reduces microgap and microleakage in the case group compared to the control group.
Keywords: Dental Implant-Abutment Design, Dental Leakage/Microbiology, Siloxanes, Dental Implants, Dental Leakage/Prevention and Control
Introduction
Formation of microgaps between the implant fixture and abutment surfaces is still one of the major problems that may lead to mechanical and biological failure and inflammation around the implant. (1,2) Implant failure rates in different studies have been reported to be less than 10%. (3,4)
For the first time, Donley and Gillette (1991) investigated the possibility of microorganism infiltration at the implant-abutment connection. (5) Some factors affecting microgap and microleakage between the implant and abutment include the implant system used, the geometry of the area of contact between the implant and abutment, and the amount of force used to tighten the abutment. (6) The consequences of such gaps are divided into two groups: 1) biological problems, including peri-implant mucositis, peri-implantitis, crestal bone resorption, and halitosis, and 2) mechanical problems, including abutment screw loosening and fracture, abutment fracture, and even fracture of the implant body. (7)
Microleakage occurs in both directions: from the internal parts of the implant to the outside and vice versa. Some methods have been reported to prevent or reduce leakage and bacterial contamination at the implant-abutment interface, such as the use of sealants, decontamination of the implant's internal cavity, the use of shape memory alloys and various connection geometries. Substances used for sealing the gap include silicone washer, chlorhexidine thymol varnish, and GapSeal. (8-10)
Various studies have shown fluid flow and bacterial accumulation around the implant-abutment junction regardless of the type of connection (external or internal); gaps of up to 49 µm have been reported. (11-17) Studies have shown a lower rate of microgap and leakage with internal implant-abutment connection compared to the external ones. (9) The effect of sealants on microgap and microleakage reduction between fixtures and abutments in internal connections under dynamic loading has been limitedly studied. In 2014, Nayak et al reported the lowest bacterial growth rate in the GapSeal group compared to O-ring. (8) They showed that the use of GapSeal at the inner surface of the fixture before torqueing reduces microleakage. In the cited study, the samples were evaluated statically. (8) In 2018, Ozdiler et al showed that sealants, contrary to different taper angles of conical implants, reduce bacterial leakage at the internal conical implant-abutment interface under a dynamic load of 50 N and 500,000 cycles. (11) In the present study, the specimens underwent cyclic loading with more force compared to previous studies in the physiological range (200,000 to 1,200,000 cycles, 15 to 160 N), evaluating the effect of GapSeal equivalent to 48 months of chewing force inside the mouth. (11)
In this study, the effect of GapSeal and its control group on preventing liquid leakage and microgaps in internal hexagon connection after dynamic loading with a 100-N force and 1,200,000 cycles was investigated.
Materials and Methods
In this in-vitro, experimental study, sixteen implant-abutment assemblies were divided into two groups of 8 samples each. According to the results of a study by Rismanchian et al, (18) using two-sample t-test power analysis option of PASS 11 software (NCSS, LLC. Kaysville, UT, USA), and considering α=0.05, β=0.02, a mean gap difference between the two groups equal to 19 μm, and standard deviations (SD) equal to 25 and 8 μm, the minimum number of samples in each group was calculated to be 8 samples. The implant system used was the BioHorizons system (Birmingham, AL 35244, Vereinigte Staaten) with internal hexagonal connection. Internal hexagon implants with a length of 10.5 mm and a diameter of 4 mm were used. Straight abutments with a length of 6 mm and a collar height of 1 mm were fixed on the fixtures (Figure 1).
Figure 1. BioHorizons internal hexagon fixture and abutment
Implants were mounted in transparent auto-polymerizing acrylic resin blocks (Moravia, Tokyo, Japan) with a circular cross-section and a diameter of 34 mm and a height of 19 mm using a parallelometer (Hahnenkratt, Berlin, Germany). (16) For the preparation of acrylic resin, an appropriate powder/liquid ratio was used according to the manufacturer’s instructions for all samples. A surveyor (J.M. Ney Co., Bloomfield, CT, USA) was used to mount the fixtures inside the acrylic mold in a completely perpendicular position (a 90-degree angle relative to the horizon). After the setting of the acrylic resin, all specimens were prepared for testing. (16)
In the case group, the internal parts of the implants were thoroughly cleaned with alcohol according to the manufacturer's instructions. GapSeal (Hager&Werken, Duisburg, Germany) was poured to the maximum capacity of the internal space of the abutments in the case group as instructed by the manufacturer to prevent air entrapment. Then, straight abutments were fixed on all samples; the abutment screws were torqued with a force of 30 Ncm using a digital torque meter (Lutron Electronic Enterprise Co. Ltd., Taipei, Taiwan) according to the implant manufacturer's instructions. In order to compensate for the settling effect, five minutes later, the abutment screw was re-tightened using the digital torque meter with a force of 30 Ncm (Figure 2). (16,17) The samples of the case group were numbered from 1 to 8, and the samples of the control group were numbered from 9 to 16. All specimens were placed inside the Chewing Stimulator CS-4 (SD Mechatronik, Munich, Germany) for cyclic loading, and 1,200,000 cycles with a 100-N force and frequency of 1 Hz were applied to all straight abutment-fixture assemblies mounted in acrylic resin blocks along the longitudinal axis (perpendicular to the abutment surface). (10) After 1,200,000 cycles, equivalent to 48 months of chewing inside the mouth, the samples were removed.
Figure 2. Case and control samples mounted in resin blocks
Microleakage measurement:
Methylene blue solution (Sigma-Aldrich, St. Louis, USA) was used to evaluate the microleakage. For this purpose, the upper contact surface of the case and control abutments was first sealed with a layer of rose wax and a layer of nail varnish to prevent methylene blue from penetrating the abutments from above. The methylene blue solution was prepared according to the manufacturer's instructions. All samples were then immersed in the solution and incubated for 24 hours at 37°C. (7)
To measure the microleakage, implant-abutment assemblies were cut (Mecatome T-201A, Presi, Paris, France) from the middle along the axial axis by a high-precision diamond wheel (Strauen Minitorm, Barcelona, Spain; Figure 3), and dye penetration at the implant-abutment interface was reported at two levels using scanning electron microscopy (SEM; Neon 40 with Gemini® column, Zeiss, Oberkochen, Germany) at x200 magnification.
Figure 3. Axial cross-section of one specimen under the scanning electron microscope (SEM; ×12)
Microgap measurement:
To measure the microgap, images were taken from the specimens sectioned at six areas, which were randomly selected (Figure 4; three points on the right and three points on the left) under the SEM at a voltage of 20 kV at ×2000 magnification, and measurements were made. (16)
The data collected from this study were entered into SPSS software (Version 22; SPSS Inc., Chicago, IL, USA) for analysis using t-test and Fischer’s exact test.
Results
.jpg){kind=link}
.jpg){kind=link}
.jpg){kind=link}
This study was performed on 16 samples including 8 samples with GapSeal (case group) and 8 samples without GapSeal (control group). The implants used were 10 mm in length and 4 mm in diameter. In this study, abutments with a length of 6 mm and a collar height of 1 mm were used.
The size of microgap was 3.04±0.54 µm in the control group and 0.99±0.39 µm in the case group, which was three times higher in the control group, and the t-test showed that this difference was statistically significant (P<0.000; Table 1; Figure 5).
Table 1. Comparison of microgaps in the control and case groups according to the use of GapSeal
Figure 4. Microgap in the group with GapSeal (left) and in the group without GapSeal (right) under the scanning electron microscope (SEM; x2000)
Figure 5. Seal of the implant-abutment interface by GapSeal (left) and penetration of methylene blue solution into the implant-abutment interface of one of the control samples (right)
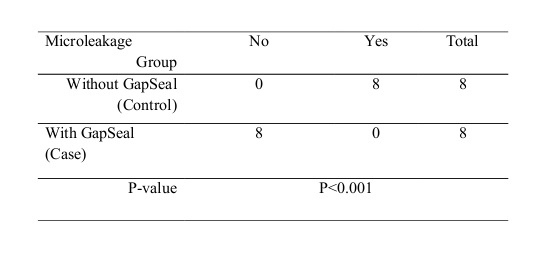
The amount of microleakage between the fixture and the abutment in internal hex connection according to the use of GapSeal is presented in Table 2 and shows that in the control group, all samples (100%) had leakage, whereas in the case group, none of the samples (0%) showed leakage. Fischer's exact test showed that this difference was statistically significant (P<0.001; Table 2).
Table 2. Distribution of samples according to microleakage divided by GapSeal
Discussion
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
This study was performed to investigate the effect of GapSeal on microleakage and microgap between the implant and abutment with internal hex connection in 8 case and 8 control samples. The results showed that the use of GapSeal decreased the microgap and microleakage in internal hex implant-abutment connection in the case group compared to the control group.
According to previous studies, leakage of liquids and bacteria at the implant-abutment interface depends on various factors, such as the implant-abutment :union:, the micromovement between the components, and the final abutment torque. The shape of the abutment-implant junction and dynamic loading can increase micromovement and create a pumping effect, affecting leakage of bacteria and liquids. (7,11,19) in some previous studies, the amount of leakage has been studied statically. In 2011, Lorenzoni et al showed that microleakage and gap at the implant-abutment interface were present in two types of hexagonal implants; however, the samples were not cyclically loaded. (16) In 2014, Smith and Turkyilmaz showed bacterial leakage at the implant-abutment interface of zirconia and titanium implants with two different torques under static conditions. (6) In 2012, Rismanchian et al evaluated microgap and microbial leakage in static conditions at the interface of four abutments of the Straumann system. (18) Their results showed that the use of different types of abutment affected the average size of microgaps and the mean number of leaked colonies (colony-forming unit [CFU]/ml) throughout the fixture and abutment junction within the first 5 hours, but it has no significant effect on the microleakage at 24 hours, 48 hours, and 14 days. (18) Failure to use cyclic loading makes the generalizability of the results difficult.
Numerous articles have pointed to the importance of leakage under loading conditions. According to various studies, cyclic loadings increase the microgap size at the implant-abutment interface, especially in implants with external hexagonal connections. (9,20-22) In the present study, the samples underwent cyclic loading to simulate clinical conditions, and the findings of the present study, indicating the presence of microleakage in the space present at the abutment-implant interface, are in line with previous studies. The results of studies that used bacteria to measure microleakage are more consistent with reality compared to the use of methylene blue. (6,11)
In the present study, the size of microgap was 0.99±0.39 µm in the GapSeal group and 3.04±0.54 µm in the control group. Bacteria ranged in size from 0.2 to 5 µm. Jansen et al suggest that the microgap between the implant and abutment can be as large as 49 µm, indicating that even the smallest microgaps are 0.4 to 10 times larger than bacteria. (16,23) In a study by Smith and Turkyilmaz, no relationship was found between the size of the microgap and bacterial leakage. (6) In 2015, Martin-Gili et al investigated fluid leakage in external and internal connections of screw abutments. (9) The size of microgap in the cited study was 2.34 µm in the internal hex connection after cyclic loading and 4.01 µm in the external hex connections. The size of microgap in the internal connection was significantly smaller compared to the external one. As the number of mechanical cycles increased, the size of microgaps increased due to titanium deformation. Methylene blue leakage was higher in the external connection. (9)
GapSeal is a silicone and bacteriostatic gel for implant cavity seal, which reduced microgap and microleakage in internal hex implant-abutment connections in the present study. The results of the previous studies that follow are in line with the present study. In 2018, Ozdiler et al showed that sealants (silicone sealant and chlorhexidine), unlike the taper angle, reduce bacterial leakage at the conical internal implant-abutment interface under dynamic loading with a 50-N force and 500,000 cycles. (11) In the present study, the specimens were loaded with more cycles and higher forces in the physiological range (200,000 to 1,200,000 cycles, 15 to 160 N); the results were consistent with the results of the study by Ozdiler et al. (11)
Nayak et al (2014) evaluated the sealing ability of O-ring polysilicon and GapSeal to prevent microleakage between the fixture and abutment in static conditions and showed that the use of GapSeal at the inner surface of the fixture before torqueing reduced the microleakage rate. (8) The c-clamp was used to fasten the abutment screw without mounting the fixture, whereas in the present study, the fixtures were mounted in molds containing acrylic resin, which were more similar to the fixture inserted in the patient's jaw. In an in-vivo study in 2014, Pimentel et al used silicone membranes to seal the microgap between the implant and abutment with external hexagonal connection. (21) Application of silicone membrane reduced bacterial strains that infiltrated the implant-abutment assembly after 30 and 90 days using DNA chain polymerization technique but did not completely prevent bacterial infiltration. Disadvantages of silicon membranes include film thickness and early decomposition in the mouth. GapSeal is also a silicone gel that disintegrates over time. Further studies are needed to evaluate the life span of GapSeal.
This double-blind study was performed with sufficient number of samples in each group. The positive aspect of this study is the evaluation of two important indices, namely microleakage and microgap. These two indices have important effects on biological and biomechanical factors that affect the success of implant treatment. One of the limitations of this study was the impossibility of placing the samples in the methylene blue solution in a cyclic loading device. Future studies can investigate the microleakage in different types of abutment-implant systems, even under different cyclic loading forces and lateral cyclic loading with different abutment lengths.
Conclusion
According to the results of this study, it can be concluded that GapSeal decreases microgap and microleakage in internal hex implant-abutment connection in the case group compared to the control group.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
