

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-238-en.html



2- Postgraduate Student, Department of Oral and Maxillofacial Radiology, School of Dentistry, Tehran University of Medical Science, Tehran, Iran. ,
Abstract
Background: Squamous odontogenic tumor-like proliferation (SOT-LP) is a rare benign lesion in the jaws with the same histological pattern to SOT but with different clinical and radiographic features. It originates from the epithelial cell rests of Malassez. The histological findings could be seen in the wall of some odontogenic cysts. Knowledge about the features of this lesion can help us in the diagnosis, treatment, and follow-up.
Case Presentation: Here, we present two cases of SOT-LP in the wall of a radicular cyst and a residual cyst.
Conclusion: SOT-LP shares several histologic characteristics with benign and malignant central jaw tumors. Making a definitive diagnosis is crucial to avoid incorrect treatment.
Keywords: Odontogenic Cysts, Radicular Cyst, Squamous Odontogenic Tumors, Cell Proliferation
Introduction
Squamous odontogenic tumor (SOT) is a rare benign neoplasm in the jaws, which originates from the epithelial cell rests of Malassez in the periodontal ligament (PDL) or remnant dental lamina; this was first described by Pullon et al. (1,2) The tumor may destroy the cortical bone with gradual growth and local infiltration. (2-4)
Usually, the lesion needs a conservative treatment but some lesions demonstrate an aggressive behavior and require block resection or hemimaxillectomy. (5,6)
The histological features consist of numerous islands of non-keratinized, well-differentiated squamous epithelium within a fibrous stroma without any sign of cellular atypia. (2-4) The bland-appearing feature differentiates SOT from squamous cell carcinoma (SCC). In addition, the peripheral cells of the epithelial islands do not show the characteristic reverse polar nuclei seen in ameloblastomas. (1,6)
SOT-like proliferation (SOT-LP) is an unusual histopathological finding in the fibrous walls of some odontogenic cysts; this was first reported by Wright. (5) Microscopically, SOT-LP demonstrates proliferating islands of squamous epithelium similar to SOT but with different clinical and radiographic features. (2,6-8)
SOT-LP with non-aggressive and non-neoplastic features has been reported in the cyst wall of keratocystic odontogenic tumors (KOTs), radicular cysts, residual cysts, and glandular odontogenic cysts; (3,6) it is considered as a hamartoid lesion. (2,7,9)
In this article, we present two cases of SOT-LP developing in the walls of a radicular cyst and a residual cyst.
Case Report 1
A 47-year-old man complaining of swelling of the right mandibular gingiva was referred to the Department of Oral and Maxillofacial Pathology, Tehran Dental School, Iran. The patient reported a slow-growing lesion that had been present for the last two years. The oral examination showed swelling in the right mandibular first premolar region with intact overlying mucosa that was normal in color. The patient had no history of previous trauma or other medical problems and only had poor oral hygiene.
The panoramic radiograph revealed a unilocular, well-defined radiolucency at the edentulous area of the mandibular first premolar (Figure 1). The lesion was approximately 2×3 cm in diameter. Aspiration of the lesion provided a viscous creamy substance.
Figure 1. Panoramic view showing a unilocular radiolucency with well-defined, corticated border in the right mandibular premolar region
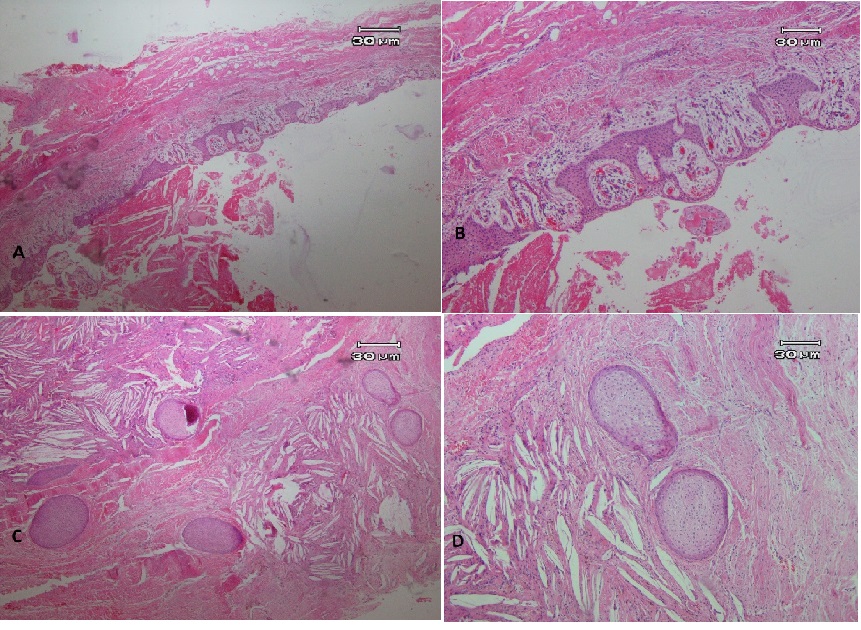
An excisional biopsy was performed using enucleation and curettage. Gross lesion revealed a cystic, creamy-brown elastic lesion with 0.2-cm maximum wall thickness. Microscopic examination showed a cystic lesion lined with odontogenic epithelium composed of non-keratinized stratified squamous epithelium with few mucin-producing cells (Figures 2a and 2b). The cyst wall revealed diffuse chronic inflammatory cell infiltration, cholesterol clefts, hemorrhage, and islands of bland-appearing odontogenic epithelium composed of squamous epithelium representing SOT-LP in the cyst wall (Figures 2c and 2d). The histological diagnosis of a residual cyst with SOT-LP was made. No recurrence occurred two years after surgery.
Figure 2. (A,B) Microscopic examinations showed a cyst lined with stratified squamous epithelium with exocytosis. (C,D) Islands of odontogenic epithelium are scattered through the connective tissue of the cyst wall, which demonstrates chronic inflammatory cell infiltration and aggregates of cholesterol clefts. Epithelial islands are composed of bland-appearing squamous cells.
Case Report 2
A 52-year-old man complaining of swelling of the left upper jaw was referred to the Department of Oral and Maxillofacial Pathology, Tehran Dental School, Iran. The patient reported a painless, slow-growing lesion present for one year at the site of the left upper incisor. Panoramic radiography revealed a round, well-defined radiolucent lesion that extended from the mesial aspect of the central incisor to the distal aspect of the canine. The left upper lateral incisor showed extensive caries. The lesion caused root divergence and displacement of the nasal cavity floor. No root resorption was seen (Figure 3).
Figure 3. Panoramic view showing a round, well-defined radiolucent lesion around the left maxillary lateral incisor.
Based on the clinical and radiographic findings, the differential diagnoses of radicular cyst, incisive canal cyst, and KOT were suggested. The aspiration provided a serosanguinous substance. The lesion was enucleated, and the lateral incisor was extracted.
Microscopic examinations showed a cystic lesion lined with stratified squamous epithelium with acanthosis, spongiosis, and arcade rete ridges (Figure 4a). Islands of bland-appearing squamous epithelium were seen (Figures 4b and 4c). Vacuolization and individual cell keratinization within the epithelium islands were noticeable. Extravasated red blood cells (RBCs) and severe, diffuse chronic inflammatory cell infiltration were also seen in the cyst wall (Figure 4).
The histopathological diagnosis of a radicular cyst with SOT-LP in the cyst wall was made. No recurrence occurred one year after surgery.
Figure 4. (A) Microscopic examination revealed a cystic lesion lined with stratified squamous epithelium with arcuate architecture, exocytosis, and spongiosis. (B) The cyst wall reveals islands of squamous epithelium with no evidence of columnar cells with reverse polar nuclei at the periphery of the islands. (C) Squamous cells have a bland appearance without nuclear atypia.
Discussion
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
SOT is a rare benign neoplasm originating from the rests of Malassez. (8) It has slow progressive growth and may invade the adjacent trabecular bone and perforate the cortical plates, eventually causing tooth mobility, pain, and swelling. (2)
SOT-LP in odontogenic cysts shares the same histopathologic features with SOT. SOT-LP is not a separate entity from odontogenic cysts but it has different clinical and radiographic features. Here, we reported two cases of SOT-LP within the wall of a radicular cyst and a residual cyst, which showed islands of bland-appearing stratified squamous epithelium in the fibrous wall of the cysts. The histological findings resemble those of true SOT. (8-10) A review of available published case reports of SOT-LP is shown in Table 1.
This entity was first described by Pullon et al. (1) The first case of SOT-LP within the wall of a radicular cyst was reported by Doyle et al. (4)
Brady et al reported the presence of these islands in the wall of a KOT associated with an unerupted tooth. (11)
The etiology of SOT-LP is unknown although some authors have suggested that SOT-LP originates from the epithelial cell rests of Malassez. (3,11-13)
Santos et al performed a study to assess the histopathological characteristics of radicular cysts in a Brazilian population. (14) Out of 73 cases, three cases showed epithelial islands resembling SOT. (14)
Goldblatt et al concluded that the absence of cellular atypia in SOT-LP indicates that it is not a true neoplastic process. (10) Unal et al proposed that the islands of SOT-LP seem to be a hamartoid lesion; (12) however, others are in controversy with this theory because of the origination of SOT-LP from the cystic surface. (12)
Philipsen et al suggested that SOT-LP develops as a result of inflammation and reactive hyperplasia of the cyst wall. (15)
Parmar et al and Oliveira et al suggested that the presence of SOT-LP in the wall of a radicular cyst is not the result of inflammation. (3,16)
The role of inflammation in the development of SOT-LP is unknown as this lesion has been reported not only in inflammatory cysts but also in developmental cysts such as dentigerous cyst and KOT. (3) Cysts with SOT-LP do not tend to change into SOT and do not show a recurrence rate higher than that of cysts without SOT-LP. (6,7,9)
The most frequent location for SOT-LP is the wall of odontogenic cysts such as radicular cysts, KOTs, follicular cysts or residual cysts. (2,5,9) In the present cases, SOT-LP has been seen to be located interradicularly (the permanent lateral incisor) in association with the radicular cyst and in an edentulous area in association with the residual cyst.
The histopathological features of SOT-LP in odontogenic cysts are similar to those of some neoplasms, including SOT, desmoplastic ameloblastoma, acanthomatous ameloblastoma, intra-osseous well-differentiated SCC, and KOT. Therefore, making a definitive diagnosis is crucial to avoid incorrect treatment. (3,16-18)
SOT-LP presents different clinical, radiological, and prognostic features than true SOT. SOTs are more aggressive than SOT-LP in cysts. (8) The clinical behavior of SOT includes mobility of the adjacent teeth, swelling of alveolar bone, and mild to moderate pain. The growth of SOT-LP is usually limited and it adds no symptoms to the cyst in which they occur. (2) Radiographically, SOT often exhibits a well-defined, unilocular radiolucency around the apex of teeth. It may cause apical divergence of adjacent teeth and root resorption. SOT-LP is a unilocular, well-circumscribed radiolucent lesion and may cause mild bony expansion. (3) SCC shows cellular atypia, including nuclear hyperchromatism, mitotic activity, abnormal mitosis, and altered nuclear/cytoplasm ratio, which are absent in islands of SOT-LP. (3)
SOT-LP may have the same origin as SOT; therefore, this lesion has been suggested by some authors to be the early expression of neoplastic transformation. (8)
Oliveira et al proposed that SOT-LP could be the initial expression of neoplastic transformation but not a carcinoma. (9)
None of the cases of SOT-LP has been reported to change into true SOT. Most of the reported cases show no more aggressive potential than an odontogenic cyst. (14)
SOT-LP management consists of enucleation, curettage or local excision of the lesion. It does not seem that SOT-LP could change the primary prognosis of the cystic process. (8)
To date, there is no report of malignant transformation or recurrences related to SOT-LP in odontogenic cysts. Therefore, SOT-LP has a good prognosis; however, it is important to diagnose it from other aggressive lesions.
Conclusion
SOT-LP has been reported in the wall of different odontogenic cysts and does not appear to have a significant impact on the behavior of these cysts; however, it shares several histologic characteristics with benign and malignant central jaw tumors. Therefore, making a definitive diagnosis is crucial to avoid incorrect treatment.
Table 1. Reported cases of squamous odontogenic tumor-like proliferation (SOT-LP) published in the literature
{kind=link}
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |