

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-229-en.html



2- Postgraduate Student, Endodontics Dept, Faculty of Dentistry, Tehran Medical Sciences, ,
3- Assistant professor, Endodontics Dept, Faculty of Dentistry, Tehran Medical Sciences,
4- Assistant professor , Restorative Dept, Tehran Medical Science ,
5- Dentist
Abstract
Background and Aim: The main goal of root canal treatment is to prevent or treat apical periodontitis. The aim of the present study was to assess the coronal restoration status, root canal filling quality, periapical health condition, and related factors in endodontically treated teeth at the Dental Faculty of Islamic Azad University of Medical Sciences, Tehran, Iran, in 2011-12.
Materials and Methods: In this descriptive, historical cohort study, a total of 160 teeth submitted to endodontic treatment were clinically and radiographically reexamined one year (minimum) postoperatively. Each volunteer answered a questionnaire on demographic and socioeconomic factors. They were also questioned about the factors related to endodontic and restorative treatments. The restoration and root canal filling quality was classified according to the modified criteria introduced by Tronstad et al. The periapical status was evaluated according to the periapical index (PAI) scores.
Results: Periapical lesions (diseased/failure) were most prevalent in Inadequate Restoration/Inadequate Root Canal Filling group (70%) followed respectively by Inadequate Restoration/Adequate Root Canal Filling group (52.2%), Adequate Restoration/Inadequate Root Canal Filling group (30%), and Adequate Root Canal Filling/Adequate Restoration group (15.5%).
Conclusion: According to the results, an efficient appointment scheduling system has the greatest impact on the completion of coronal restoration after endodontic treatments. Provision of adequate root canal filling and perfect coronal restoration can reduce the prevalence of postoperative periapical lesions and increase the success rate of endodontic treatments.
Keywords: Root Canal Obturation, Periapical Diseases, Cohort Studies, Radiography
Introduction
The main goal of root canal treatment is to prevent or treat apical periodontitis for preserving the function of the tooth in the oral cavity. (1-4) Root canal treatment includes the removal of necrotic or damaged pulpal tissue followed by the preparation of well-condensed obturation to inhibit further microbial proliferation through the root canal system. (2,5)
For years, apical microleakage was considered as the key suspect of endodontic failure. (6) Today, it is generally accepted that the outcome of root canal treatment is positively associated with the technical quality of the root filling. (7) However, since Marshall and Massler (2) noted the effect of coronal leakage, more attention has been paid to coronal leakage as a potential cause of endodontic failure. (8-10)
In their in-vitro study, Torabinejad et al showed that bacterial products were found at the apex of root-filled teeth after 3 months when there was no coronal restoration. (11) Several experimental studies have indicated that a good coronal restoration is required for endodontically treated teeth to function and to prevent coronal leakage. (12,13) By studying 1010 endodontically treated teeth, Ray and Trope found that the quality of the coronal restoration had a greater impact on the periradicular state than the quality of the endodontic treatment. (14) Other cross-sectional studies have evaluated the influence of the quality of root canal fillings and coronal restorations on the periradicular status of root canal-treated teeth. (15-18) These studies have reported different results; some reports concluded that periradicular health depended equally on the quality of the root canal filling and the coronal restoration, (19,20) while some studies emphasized more on the quality of the root canal filling. (15,21,22)
The majority of studies evaluating the periapical status and the coronal restoration quality of root canal-treated teeth have been performed in Europe, North America, and East Asia. (8,23-28) For countries located in the Middle East, only limited information is available. (29,30) To the best of our knowledge, there are few studies evaluating the prevalence of apical periodontitis in root canal-treated teeth in the Iranian population; (31) therefore, the aim of the present descriptive, historical cohort study was to assess the coronal restoration status, root canal filling quality, periapical health condition, and related factors in endodontically treated teeth at the Dental Faculty of Islamic Azad University of Medical Sciences, Tehran, Iran, in 2011-12.
Materials and Methods
Study population:
This historical cohort study was performed at the Dental Faculty of Islamic Azad University of Medical Sciences, Tehran, Iran. Patients who had received primary root canal treatment in at least one permanent tooth at the Department of Endodontics, between April 2011 and April 2013, were contacted. Data on the affected tooth/teeth (pretreatment pulp status, pretreatment periapical health status, and pretreatment sinus tract presence) were obtained from the records. The unit ‘tooth’ was specified as the smallest study unit. In cases where more than one tooth had undergone endodontic treatment, each tooth was evaluated individually. All endodontic treatments had been conducted by senior dental students supervised by the teaching staff at the university clinic. The complete clinical procedure of endodontic treatment had been performed with rubber dam isolation. Following access cavity preparation and radiographic length determination, the root canals had been prepared with standardized hand instruments (reamers, K-files, and Hedstrom files) according to the step-back technique. All root canals had been obturated with gutta-percha points and AH-26 sealer (Dentsply, Tulsa Dental, Tulsa, OK, USA) using the lateral condensation technique. A control radiograph had been taken in each case upon the completion of the root canal filling. The patients were equally informed and invited for re-examination one year (minimum) postoperatively. Of all 1997 patients who were invited, 160 patients attended to the follow-up program.
Demographic and socioeconomic data collection:
Each volunteer answered a questionnaire on demographic factors (sex, age, nationality, and marital status) and socioeconomic factors (education, employment, and house ownership status).
Radiographic and clinical assessments:
All the follow-up assessments were performed by a single examiner under the supervision of an endodontist and an operative dentistry specialist. The teeth were grouped according to the quality of the root filling and the coronal restoration.
The quality of the root canal filling was assessed both clinically and radiographically. All periapical radiographs were obtained by the parallel technique and were evaluated using an x-ray viewer at ×3.5 magnification. The criteria used for radiographic evaluation were slightly modified from those described by Tronstad et al. (22) For the clinical evaluation, intraoral and extraoral examinations were performed to identify signs and symptoms related to root canal filling. The teeth were submitted to palpation and percussion. Thus, the clinical and radiographic classifications of the root canal filling quality were made according to the criteria listed below:
1. Adequate root canal filling: All canals obturated, no voids present, the root filling ends 0-2 mm short of the radiographic apex, no clinical symptoms or signs (elicited or spontaneous pain, sinus tract, edema, or exudation).
2. Inadequate root canal filling: The root filling ends more than 2 mm short of the radiographic apex or the canal grossly overfilled or unfilled, root filling with voids or inadequate density, the presence of clinical symptoms or signs.
The quality of the coronal restoration was assessed both clinically and radiographically. All periapical radiographs were obtained by the parallel technique and were evaluated using an x-ray viewer at ×3.5 magnification. The criteria used for radiographic evaluation were slightly modified from those described by Tronstad et al. (22) For the clinical evaluation, an intraoral examination was performed with the aid of a #5 dental mirror and a dental probe to identify the type and the quality of the coronal restoration. Thus, the clinical and radiographic classifications of the coronal restoration quality were made according to the criteria listed below:
1. Adequate coronal restoration: A permanent, intact restoration with a good marginal fit, no fractures, cracks, or recurrent caries.
2. Inadequate coronal restoration: Any permanent restoration showing detectable signs of overhangs, fractures, cracks, poor marginal fit, or recurrent caries or the presence of a temporary restoration. Teeth with no coronal restoration were also included in this group.
Periapical status evaluation:
The postoperative and follow-up periapical states were evaluated according to the periapical index (PAI) scores. (32) The teeth were classified according to healthy/success (PAI 1 and PAI 2, no clinical signs or symptoms) or diseased/failure (PAI 3, 4, and 5, the presence of clinical signs and/or symptoms). The unit of evaluation was the whole tooth; thus, the highest score of all roots (in multi-rooted teeth) was considered.
Results
The gender distribution was well balanced with 78 female (49%) and 80 male (51%) patients. At the time of root canal treatment, the patients ranged in age from 15 to 67 years, and 76 patients (47.5%) were aged 30-50 years. The unemployment rate was 36% among the patients, and the majority of them were literate (98.7%). A descriptive analysis of the demographic and socioeconomic characteristics of the studied samples is given in Table 1.
Table 1: Descriptive analysis of the demographic and socioeconomic characteristics of the samples (160 patients) using relative (%) and absolute (n) frequencies
Of the 160 teeth, 127 teeth survived and 33 were extracted due to fracture (31 teeth) and postoperative infection (2 teeth). The most frequent tooth group was that of premolars (37.5%), and the most frequent restoration type was composite resin (35.4%). Procedural mishaps were detectable in the postoperative radiograph of 6.9% of the cases. Radiolucent periapical lesions were notable in the postoperative radiograph of 23.1% of 160 cases and in the follow-up radiograph of 27.5% of 127 survived cases. The size of the periapical lesion reduced in 11 cases, increased in 9 cases, and remained unchanged in one case. A descriptive analysis of the studied samples is given in Table 2.
Table 2: Descriptive analysis of the studied samples (160 teeth) using relative (%) and absolute (n) frequencies
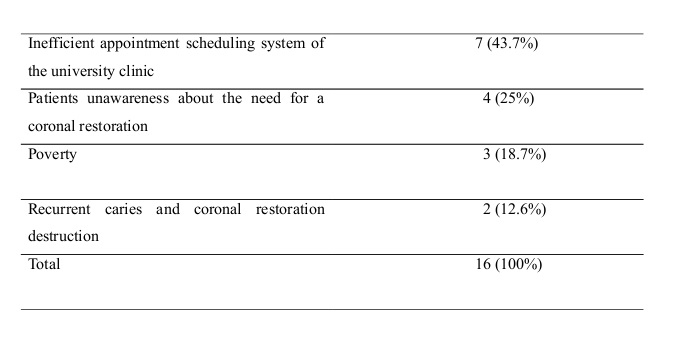
The most important reason for the lack of coronal restoration at the follow-up appointment was the inefficient appointment scheduling system of the university clinic (Table 3). The coronal restoration was completed in less than 30 days after root canal treatment in 42% of the cases, in 30-60 days after root canal treatment in 33% of the cases, and in more than 60 days after root canal treatment in 25% of the cases. The postoperative periapical status and the quality of the coronal restoration and the root canal filling for reexamined teeth are presented in (Table 4).
Table 3: Declared reasons for the lack of coronal restoration
Table 4: Postoperative periapical status and quality of coronal restoration and root canal filling of reexamined teeth
Discussion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In this historical cohort study, 160 out of 1997 patients who had received primary endodontic treatment during 2011-12 were reexamined for endodontic and restorative treatment outcome. The recall rate of the present study was 8% which is significantly lower compared to previous studies. (33,34) There are two main reasons for this result: first, recall examination is not a routine process at the center where this study was performed. Second, because the center is an educational one, many patients commute long distances to reach the place to get access to affordable treatments; therefore, they are not willing to come back just for a reexamination.
Cross-sectional studies have been used to evaluate the influence of the coronal restoration and the endodontic treatment quality on the periapical status, which have rendered different results from several geographic locations. (16,17) The main disadvantage of a cross-sectional design is that the data analysis is restricted to the available information and is therefore vulnerable to interpretation bias. For instance, the radiographs are examined only at one given time point, making it impossible to determine whether the observed periapical lesion is healing.
A recognized limitation of the present study was that periapical status assessment was based on a two-dimensional (2D) radiographic method. A three-dimensional (3D) evaluation using cone-beam computed tomography (CBCT) could improve the accuracy of the study. (35,36)
Other limitations include incomplete dental records of the patients, low-quality postoperative radiographs, and lack of access to the patients due to unresponsiveness to phone calls.
In this study, the original endodontic treatments were performed by different undergraduate students. The overall success rate was 57.5% in this study, confirming the results of similar studies performed for the most part by general clinicians or undergraduate students in a large number of countries, which reported high frequencies of periradicular lesions and poorly filled root canals (20,23) in contrast to studies in which endodontic treatments were performed by specialists. (34,37) It is well established that treatment carried out by graduate students and specialists has the highest weighted pooled estimate of success. (37,38)
Most studies have evaluated the coronal restoration quality based only on radiographic examinations; (14,16,39) however, this method is limited because radiographs have insufficient diagnostic value. Microleakage in occlusal margins, cracks, and perforations might not be observed in radiographs. Few studies have performed clinical and radiographic assessments of the coronal restoration quality and found any correlation between these different assessments. (8,19) In this study, we evaluated the coronal restoration quality both clinically and radiographically. 12.6% of the 127 survived teeth did not have any coronal restoration at the follow-up appointment. The most important reason remarked by the patients was the inefficient appointment scheduling system of the university clinic followed by patients’ unawareness about the need for a coronal restoration, poverty, recurrent caries, and coronal restoration destruction. It is obvious that a basic reform in the appointment scheduling system of the center is strongly needed; for example, coronal restoration of the teeth that receive endodontic treatment near New Year and summer vacation should be fully managed without any delay. In addition, patients’ knowledge about the necessity of a permanent coronal restoration after root canal treatment must be improved.
The effect of the root canal filling quality on treatment outcome is well established. In addition, the importance of bacteria and a tight coronal seal has been demonstrated in several studies. In-vitro studies have suggested that direct exposure of root canal filling to microorganisms and their products may lead to reinfection of the root canal system in a relatively short period of time. (10,12)
However, contradictory results have been reported by different studies that investigated the influence of endodontic treatment and the coronal restoration quality on the periapical status. Ray and Trope suggested that the quality of the restoration had a greater impact on periradicular health than the quality of the root canal filling. (14) Other studies have suggested that treatment success rates depend equally on the quality of the root canal filling and the coronal restoration. (19,20) Moreover, Ricucci et al reported that the exposure of root canal filling to the oral microbiota was not significantly correlated with the periradicular status. (40, 41)
The results of the present study indicate that periapical lesions (diseased/failure) are most prevalent in Inadequate Restoration/Inadequate Root Canal Filling group (70%) followed respectively by Inadequate Restoration/Adequate Root Canal Filling group (52.2%), Adequate Restoration/Inadequate Root Canal Filling group (30%), and Adequate Root Canal Filling/Adequate Restoration group (15.5%). The presence of periapical lesions in Adequate Root Canal Filling/Adequate Coronal Restoration group can be an indicator of insufficient root canal cleaning and disinfection or procedural mishaps.
Conclusion
Overall, the results of this study confirm that an efficient appointment scheduling system has the greatest impact on the completion of coronal restoration after endodontic treatments. Furthermore, the provision of adequate root canal filling and perfect coronal restoration can reduce the prevalence of postoperative periapical lesions and increase the success rate of endodontic treatments.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |