Journal of Research in Dental
and Maxillofacial Sciences
Volume 2, Issue 4 (10-2017)
J Res Dent Maxillofac Sci 2017, 2(4): 44-49 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mehralizadeh S, Nemati Anaraki S, Orshesh M. Comparison of CMOS and PSP intraoral digital sensors in the diagnosis of secondary caries adjacent to amalgam restorations. J Res Dent Maxillofac Sci 2017; 2 (4) :44-49
URL: http://jrdms.dentaliau.ac.ir/article-1-180-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-180-en.html


1- Assistant professor, Department of Oral and Maxillofacial Radiology, , sandramehr@yahoo.com
2- Assistant professor, Department of Restorative Dentistry,
3- Dentist
2- Assistant professor, Department of Restorative Dentistry,
3- Dentist
Full-Text [PDF 270 kb]
(3593 Downloads)
| Abstract (HTML) (6954 Views)
Abstract
Background and Aim: Considering the consequences of false positive (FP) and false negative (FN) diagnoses as well as the lack of information on the diagnostic ability of photostimulable phosphor plate (PSP) and complementary metal oxide semiconductor (CMOS) sensors in the detection of secondary caries, this study aimed to compare the diagnostic ability of these two sensors in the detection of secondary caries adjacent to amalgam restorations.
Materials and Methods: This diagnostic study was performed on 40 intact permanent premolars. Class II cavities were prepared and restored with amalgam. Periapical radiography was performed by using PSP and CMOS sensors via parallel technique. A 0.5-mm round bur was used to create another cavity under amalgam restorations. To simulate secondary gingival caries at the cementoenamel junction (CEJ), the samples were placed inside 0.1M lactic acid solution and were incubated at 37°C for three weeks. The teeth were placed in gypsum blocks and were radiographed again by CMOS and PSP sensors. The presence of decay was determined by an oral and maxillofacial radiologist, and the results were recorded in datasheets and were statistically analyzed by the ratio test.
Results: The sensitivity and specificity of PSP in caries detection were 52.5% and 77.5%, respectively. The sensitivity and specificity of CMOS in caries detection were 57.5% and 82.5%, respectively. Incorrect diagnoses (FP+FN) were equal to 35% for PSP and 30% for CMOS (P=0.89).
Conclusion: The results indicated that PSP and CMOS sensors have similar abilities in the detection of secondary caries under amalgam restorations, while none of the two sensors has the adequate ability for a precise and thorough diagnosis of secondary caries.
Keywords: Dental digital radiography, Dental caries, Diagnosis, Amalgam
Introduction
The diagnosis of secondary caries is one of the concerns that dentists constantly face. According to Black, secondary caries is the recurrence of caries at the margins of a restoration. (1) Secondary carious lesions occur adjacent to restorations following microleakage, an inadequate extension of the restoration, or inadequate removal of primary caries. (2) Approximately 75% of dental procedures include the replacement of a restoration due to various reasons, the main of which has been announced by dentists to be secondary caries. (3)
Currently, the diagnostic methods for secondary caries include clinical examination in a clean and dry environment under adequate light, visual inspection, tactile sense by using a dental explorer, caries detectors, dental floss, radiographic techniques, and knowledge of probabilities to determine that whether the assumed situation is healthy or it imposes a risk for caries. (3) Radiographic techniques are applicable and noninvasive methods for the diagnosis of caries that are clinically invisible and may cause a delay in the replacement of suspicious restorations until the appearance of radiographic signs. (4) Albeit, there are some controversies over the accuracy and validity of detection of decay by the use of radiographic methods. (5,6)
Radiation detectors are used in digital radiography. The electrical efficiency of the detectors is relatively proportional to the intensity of radiation. Ultimately, the produced signal is converted from the analog state to digital format. This image is displayed on a monitor after computerized processing. (7) Photostimulable phosphor plates (PSP) absorb and store the x-ray energy and release this energy as light (phosphorescence). A number is assigned to this phosphorescence light, which is indicative of the amount of x-ray energy that the material has absorbed. The complementary metal oxide semiconductor (CMOS) technology is the basis of customary video cameras; these are semiconductor detectors with a silicon base. Each pixel is separate from the adjacent pixel and is directly connected to a transistor. The electron-hole pairs inside the pixel produce a charge proportional to the amount of the absorbed x-ray energy. This charge is transferred to the transistor as a small voltage. The voltage in each transistor can be read separately and be stored and consequently appear as a grey value. (8)
Syriopoulos et al found no significant difference between the diagnostic accuracy of two types of radiographic films and digital intraoral PSP systems (Digora and DenOptix). (9) Castro et al showed that there is no significant difference between conventional radiography (Ekta Speed and Ekta Speed Plus) and direct digital imaging (CMOS and PSP) in terms of the diagnosis of caries. (10)
Ilguy et al concluded that D-speed and Digora images on liquid-crystal display (LCD) monitors have a greater diagnostic ability compared to E-speed and F-speed films. (11)
In a study by Murat et al, it was observed that cone-beam computerized tomography (CBCT) images have a significantly higher diagnostic ability compared to the images obtained by the use of PSP or conventional radiography. (12)
Nair et al showed that higher levels of contrast and brightness in digital images provide an opportunity for a better diagnosis of secondary caries compared to conventional films. (13)
The results of similar studies have indicated that there is no significant difference between original digital images and radiographic films, while enhanced digital images have a significantly lower accuracy in the detection of caries, and numerous factors influence the diagnostic ability of an observer, including the imaging system (digital or conventional). (14,15)
Considering the known complications of false positive (FP) and false negative (FN) diagnoses and the information gap with regard to the diagnostic ability of digital intraoral sensors (CMOS and PSP) in the diagnosis of secondary caries, the purpose of the present study was to compare the diagnostic ability of CMOS and PSP sensors in the detection of secondary caries adjacent to amalgam restorations.
Materials and Methods
In this in-vitro diagnostic study, 40 human permanent premolars without caries, cracks, cavities, previous restorations, or fractures were selected. A class II cavity was prepared in each tooth by using a #08 bur (D&Z, Germany) and a high-speed handpiece. To equalize the final depth of the cavities, the bur was placed on the occlusal surface of each tooth such that the shank of the bur prevented extra preparations after reaching the surface of the tooth (the long axis of the bur was perpendicular to the long axis of the tooth). The prepared cavities (DO or MO) were filled with amalgam (Tytin FC, Kerr, USA) prepared by a Degussa Dentomat 3 amalgamator with the speed of 3500 rpm (revolutions per minute). After regulating the density and contrast, periapical radiography was performed by using PSP (Digora Optime, DXR-50 001, Soredex, Orion Corp., Helsinki, Finland) and CMOS (Rayence Co., Ltd., South Korea) sensors. Afterwards, another small cavity was created underneath the amalgam restorations by using a 0.5-mm round bur (D&Z, Germany). The bur was exchanged after five preparations. (16) Next, to simulate secondary gingival caries at the cementoenamel junction (CEJ), the samples were placed inside 0.1M lactic acid solution and were incubated at 37°C for three weeks (dental surfaces, except for the area prepared by the round bur, were covered with a layer of nail polish to protect them from acid). (9) The teeth were placed in gypsum blocks and were radiographed by using the CMOS sensor with the resolution of 14.2 lp/mm and active pixel array: size 1.5:686×944 pixels (24.01×33.04 mm), and then, they were radiographed once again by using Digora Optime sensor with bit depth of 14 bits, pixel size of 35 µm, resolution of 14.3 lp/mm, plate size of 41×31 mm, and matrix dimensions of 886×1171 pixels. The CMOS sensor was exposed by the use of AET-Orix 70 x-ray unit (ARDET Dental, Buccinasco, Italy) with the exposure parameters of 70 kilovoltage peak (kVp) and 9 milliamperes (mA), while the PSP sensor was exposed by the use of Minray x-ray machine (Soredex, Orion Corp., Helsinki, Finland) with the same exposure parameters. The duration of exposure was 0.2 seconds. The periapical radiographs were taken via parallel technique. Next, the images were shown on a 17" LCD monitor (LG Flatron W1752S, South Korea). An oral and maxillofacial radiologist with at least five years of experience in radiographic interpretation of carious lesions assessed the presence or absence of secondary caries. The observer-monitor distance was 50 cm. To prevent eye fatigue, the observer assessed the images at different time intervals. The observer was blind to the presence and absence of caries. The presence and absence of caries were registered in special datasheets according to a three-point scale (carious, without caries, indiscernible). To compare the data with the gold standard, an agreement table was used, and the level of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of these techniques were calculated according to the related formulae. To determine the level of each of the abovementioned indices, the ratio test was used. Statistical analyses were performed by using SPSS version 13 software program (IBM Co., Chicago, IL, USA).
Results
This study was performed on 80 samples, including 40 teeth with secondary caries and 40 teeth without secondary caries. CMOS and PSP sensors were used for radiography.
The distribution of the samples according to caries detection by using the PSP sensor shows that the level of sensitivity of this sensor in the detection of caries is 52.5%, and the specificity is 77.5%. Correct diagnoses (TP+TN) were equal to 65%, while incorrect diagnoses (FP+FN) were equal to 35%.
The distribution of the samples according to caries diagnosis by using the CMOS sensor shows that the level of sensitivity of this sensor in the detection of caries is 57.5%, and the specificity is 82.5%. Correct diagnoses (TP+TN) were equal to 70%, while incorrect diagnoses (FP+FN) were equal to 30%. The sensitivity and specificity of these two sensors were not significantly different (P=0.625).
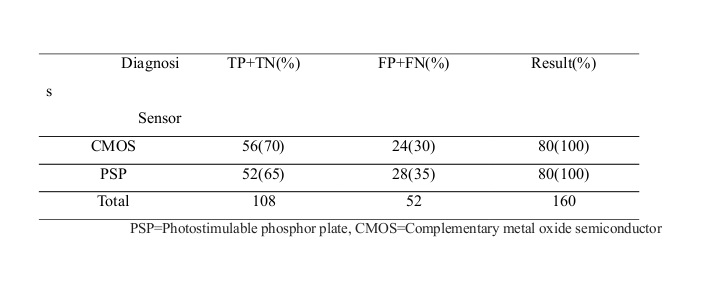
The distribution of the samples according to correct diagnoses (TP+TN) and incorrect diagnoses (FP+FN) and categorized by the type of sensor is shown in Table 1, which shows that the value is 35% for PSP and 30% for CMOS, and the ratio test showed that the difference in incorrect diagnoses between the two sensors was not significant (P=0.89).
Table 1: Distribution of the samples according to correct diagnoses (TP+TN) and incorrect diagnoses (FP+FN) and categorized by the type of sensor
Discussion
This research showed that PSP and CMOS sensors have similar diagnostic abilities in the detection of secondary caries. Syriopoulos et al compared dental radiographic films (Dentus Comfort E and E plus), charge-coupled device (CCD) digital intraoral systems (Sidexis and Visualix), and digital intraoral PSP systems (Digora and DenOptix) in the detection of proximal caries. The results showed no significant difference in the diagnostic accuracy of radiographic films, Digora system, and Sidexis system, (9) which is in line with our results.
Castro et al compared conventional radiography (Ekta Speed and Ekta Speed Plus) and direct digital imaging (CMOS and PSP) in the diagnosis of proximal caries and concluded that the three modalities had no significant difference in this regard, (10) which is in agreement with our findings.
Ilguy et al evaluated the diagnosis of artificial occlusal caries with PSP system on two types of LCD monitors in comparison with three types of radiographic films and concluded that the images obtained by the use of D-speed films and Digora sensor on both types of LCD monitors rendered a higher diagnostic ability compared to E-speed and F-speed films. (11)
Murat et al assessed the diagnosis of artificial secondary buccal caries under restorations with the use of different radiographic modalities and observed that CBCT images have a significantly higher diagnostic ability compared to PSP and conventional radiography. (12)
Nair et al evaluated the diagnostic accuracy of intraoral films (Ekta Speed) and different digital images including enhanced PSP and CCD for the detection of secondary caries; this study on 24 extracted posterior teeth showed that higher levels of contrast and brightness in digital images improved the diagnosis of secondary caries compared to conventional films. They also declared that the performance of CCD and PSP is not significantly different in the detection of secondary caries, (13) which is similar to the results of the current study.
De Araujo et al evaluated the presence of caries in 52 premolars (104 proximal surfaces) by using original and enhanced digital methods and E-speed and F-speed films. The results indicated that there is no significant difference between original digital images and radiographic films, while enhanced digital images had a significantly lower diagnostic accuracy in the detection of caries. (14)
One of the limitations of the present study was its small sample size. It seems that with increasing the number of samples, there might be a possibility of extracting significant statistical results. Since in-vitro conditions are different from oral conditions and it is impossible to precisely simulate the oral cavity in in-vitro studies, it seems that these conditions create some limitations in the extraction of significant statistical results, and only the results of in-vivo studies can be generalized to clinical situations.
One of the advantages of the present study was the use of a single software to eliminate interferences caused by different software programs. Our goal in using advanced technologies is to reach a better caries diagnosis. Therefore, in the present study, we used two sensors that are extremely new and popular among radiologists and dentists.
Considering the extensive research on the diagnosis of secondary caries and the importance of this topic, finding a more reliable method in line with the advancement of technology is a necessity. Overall, numerous factors influence the diagnostic ability of the observer, including the type of imaging modality (digital or conventional), the type of monitor or radiographic film, image enhancements, viewing conditions, and the experience of the observer. (15,16) Therefore, in addition to visual conditions, it seems that implementing the latest technology of monitor and sensor and best software programs with suitable designs is effective in making an accurate diagnosis of different lesions including carious lesions.
Since both PSP and CMOS systems are digital and two-dimensional (2D), they have similar advantages and disadvantages (similar sensitivity and specificity). We aimed to show that whether CMOS, as a superior technology, has some advantages over PSP; however, we did not find such advantages. An important issue in digital imaging is the experience of the observer, which can greatly influence the diagnosis of different lesions. It seems that an observer who has a greater experience in assessing digital images and is familiar with the related software programs has a higher diagnostic ability compared to an observer who has more experience in working with radiographic films. To reach more accurate and reliable diagnoses, the combined use of different radiographic systems and diagnostic tools such as DIAGNOdent is recommended. (17)
Conclusions
The results of the present study indicated that PSP and CMOS sensors are similar in the diagnosis of secondary caries under amalgam restorations. In addition, none of these sensors has the necessary diagnostic ability for the accurate and thorough diagnosis of secondary caries. It seems that further studies are necessary to reach a definitive conclusion.
Full-Text: (2358 Views)
Abstract
Background and Aim: Considering the consequences of false positive (FP) and false negative (FN) diagnoses as well as the lack of information on the diagnostic ability of photostimulable phosphor plate (PSP) and complementary metal oxide semiconductor (CMOS) sensors in the detection of secondary caries, this study aimed to compare the diagnostic ability of these two sensors in the detection of secondary caries adjacent to amalgam restorations.
Materials and Methods: This diagnostic study was performed on 40 intact permanent premolars. Class II cavities were prepared and restored with amalgam. Periapical radiography was performed by using PSP and CMOS sensors via parallel technique. A 0.5-mm round bur was used to create another cavity under amalgam restorations. To simulate secondary gingival caries at the cementoenamel junction (CEJ), the samples were placed inside 0.1M lactic acid solution and were incubated at 37°C for three weeks. The teeth were placed in gypsum blocks and were radiographed again by CMOS and PSP sensors. The presence of decay was determined by an oral and maxillofacial radiologist, and the results were recorded in datasheets and were statistically analyzed by the ratio test.
Results: The sensitivity and specificity of PSP in caries detection were 52.5% and 77.5%, respectively. The sensitivity and specificity of CMOS in caries detection were 57.5% and 82.5%, respectively. Incorrect diagnoses (FP+FN) were equal to 35% for PSP and 30% for CMOS (P=0.89).
Conclusion: The results indicated that PSP and CMOS sensors have similar abilities in the detection of secondary caries under amalgam restorations, while none of the two sensors has the adequate ability for a precise and thorough diagnosis of secondary caries.
Keywords: Dental digital radiography, Dental caries, Diagnosis, Amalgam
Introduction
The diagnosis of secondary caries is one of the concerns that dentists constantly face. According to Black, secondary caries is the recurrence of caries at the margins of a restoration. (1) Secondary carious lesions occur adjacent to restorations following microleakage, an inadequate extension of the restoration, or inadequate removal of primary caries. (2) Approximately 75% of dental procedures include the replacement of a restoration due to various reasons, the main of which has been announced by dentists to be secondary caries. (3)
Currently, the diagnostic methods for secondary caries include clinical examination in a clean and dry environment under adequate light, visual inspection, tactile sense by using a dental explorer, caries detectors, dental floss, radiographic techniques, and knowledge of probabilities to determine that whether the assumed situation is healthy or it imposes a risk for caries. (3) Radiographic techniques are applicable and noninvasive methods for the diagnosis of caries that are clinically invisible and may cause a delay in the replacement of suspicious restorations until the appearance of radiographic signs. (4) Albeit, there are some controversies over the accuracy and validity of detection of decay by the use of radiographic methods. (5,6)
Radiation detectors are used in digital radiography. The electrical efficiency of the detectors is relatively proportional to the intensity of radiation. Ultimately, the produced signal is converted from the analog state to digital format. This image is displayed on a monitor after computerized processing. (7) Photostimulable phosphor plates (PSP) absorb and store the x-ray energy and release this energy as light (phosphorescence). A number is assigned to this phosphorescence light, which is indicative of the amount of x-ray energy that the material has absorbed. The complementary metal oxide semiconductor (CMOS) technology is the basis of customary video cameras; these are semiconductor detectors with a silicon base. Each pixel is separate from the adjacent pixel and is directly connected to a transistor. The electron-hole pairs inside the pixel produce a charge proportional to the amount of the absorbed x-ray energy. This charge is transferred to the transistor as a small voltage. The voltage in each transistor can be read separately and be stored and consequently appear as a grey value. (8)
Syriopoulos et al found no significant difference between the diagnostic accuracy of two types of radiographic films and digital intraoral PSP systems (Digora and DenOptix). (9) Castro et al showed that there is no significant difference between conventional radiography (Ekta Speed and Ekta Speed Plus) and direct digital imaging (CMOS and PSP) in terms of the diagnosis of caries. (10)
Ilguy et al concluded that D-speed and Digora images on liquid-crystal display (LCD) monitors have a greater diagnostic ability compared to E-speed and F-speed films. (11)
In a study by Murat et al, it was observed that cone-beam computerized tomography (CBCT) images have a significantly higher diagnostic ability compared to the images obtained by the use of PSP or conventional radiography. (12)
Nair et al showed that higher levels of contrast and brightness in digital images provide an opportunity for a better diagnosis of secondary caries compared to conventional films. (13)
The results of similar studies have indicated that there is no significant difference between original digital images and radiographic films, while enhanced digital images have a significantly lower accuracy in the detection of caries, and numerous factors influence the diagnostic ability of an observer, including the imaging system (digital or conventional). (14,15)
Considering the known complications of false positive (FP) and false negative (FN) diagnoses and the information gap with regard to the diagnostic ability of digital intraoral sensors (CMOS and PSP) in the diagnosis of secondary caries, the purpose of the present study was to compare the diagnostic ability of CMOS and PSP sensors in the detection of secondary caries adjacent to amalgam restorations.
Materials and Methods
In this in-vitro diagnostic study, 40 human permanent premolars without caries, cracks, cavities, previous restorations, or fractures were selected. A class II cavity was prepared in each tooth by using a #08 bur (D&Z, Germany) and a high-speed handpiece. To equalize the final depth of the cavities, the bur was placed on the occlusal surface of each tooth such that the shank of the bur prevented extra preparations after reaching the surface of the tooth (the long axis of the bur was perpendicular to the long axis of the tooth). The prepared cavities (DO or MO) were filled with amalgam (Tytin FC, Kerr, USA) prepared by a Degussa Dentomat 3 amalgamator with the speed of 3500 rpm (revolutions per minute). After regulating the density and contrast, periapical radiography was performed by using PSP (Digora Optime, DXR-50 001, Soredex, Orion Corp., Helsinki, Finland) and CMOS (Rayence Co., Ltd., South Korea) sensors. Afterwards, another small cavity was created underneath the amalgam restorations by using a 0.5-mm round bur (D&Z, Germany). The bur was exchanged after five preparations. (16) Next, to simulate secondary gingival caries at the cementoenamel junction (CEJ), the samples were placed inside 0.1M lactic acid solution and were incubated at 37°C for three weeks (dental surfaces, except for the area prepared by the round bur, were covered with a layer of nail polish to protect them from acid). (9) The teeth were placed in gypsum blocks and were radiographed by using the CMOS sensor with the resolution of 14.2 lp/mm and active pixel array: size 1.5:686×944 pixels (24.01×33.04 mm), and then, they were radiographed once again by using Digora Optime sensor with bit depth of 14 bits, pixel size of 35 µm, resolution of 14.3 lp/mm, plate size of 41×31 mm, and matrix dimensions of 886×1171 pixels. The CMOS sensor was exposed by the use of AET-Orix 70 x-ray unit (ARDET Dental, Buccinasco, Italy) with the exposure parameters of 70 kilovoltage peak (kVp) and 9 milliamperes (mA), while the PSP sensor was exposed by the use of Minray x-ray machine (Soredex, Orion Corp., Helsinki, Finland) with the same exposure parameters. The duration of exposure was 0.2 seconds. The periapical radiographs were taken via parallel technique. Next, the images were shown on a 17" LCD monitor (LG Flatron W1752S, South Korea). An oral and maxillofacial radiologist with at least five years of experience in radiographic interpretation of carious lesions assessed the presence or absence of secondary caries. The observer-monitor distance was 50 cm. To prevent eye fatigue, the observer assessed the images at different time intervals. The observer was blind to the presence and absence of caries. The presence and absence of caries were registered in special datasheets according to a three-point scale (carious, without caries, indiscernible). To compare the data with the gold standard, an agreement table was used, and the level of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of these techniques were calculated according to the related formulae. To determine the level of each of the abovementioned indices, the ratio test was used. Statistical analyses were performed by using SPSS version 13 software program (IBM Co., Chicago, IL, USA).
Results
This study was performed on 80 samples, including 40 teeth with secondary caries and 40 teeth without secondary caries. CMOS and PSP sensors were used for radiography.
The distribution of the samples according to caries detection by using the PSP sensor shows that the level of sensitivity of this sensor in the detection of caries is 52.5%, and the specificity is 77.5%. Correct diagnoses (TP+TN) were equal to 65%, while incorrect diagnoses (FP+FN) were equal to 35%.
The distribution of the samples according to caries diagnosis by using the CMOS sensor shows that the level of sensitivity of this sensor in the detection of caries is 57.5%, and the specificity is 82.5%. Correct diagnoses (TP+TN) were equal to 70%, while incorrect diagnoses (FP+FN) were equal to 30%. The sensitivity and specificity of these two sensors were not significantly different (P=0.625).
The distribution of the samples according to correct diagnoses (TP+TN) and incorrect diagnoses (FP+FN) and categorized by the type of sensor is shown in Table 1, which shows that the value is 35% for PSP and 30% for CMOS, and the ratio test showed that the difference in incorrect diagnoses between the two sensors was not significant (P=0.89).
Table 1: Distribution of the samples according to correct diagnoses (TP+TN) and incorrect diagnoses (FP+FN) and categorized by the type of sensor
{kind=link}
Discussion
This research showed that PSP and CMOS sensors have similar diagnostic abilities in the detection of secondary caries. Syriopoulos et al compared dental radiographic films (Dentus Comfort E and E plus), charge-coupled device (CCD) digital intraoral systems (Sidexis and Visualix), and digital intraoral PSP systems (Digora and DenOptix) in the detection of proximal caries. The results showed no significant difference in the diagnostic accuracy of radiographic films, Digora system, and Sidexis system, (9) which is in line with our results.
Castro et al compared conventional radiography (Ekta Speed and Ekta Speed Plus) and direct digital imaging (CMOS and PSP) in the diagnosis of proximal caries and concluded that the three modalities had no significant difference in this regard, (10) which is in agreement with our findings.
Ilguy et al evaluated the diagnosis of artificial occlusal caries with PSP system on two types of LCD monitors in comparison with three types of radiographic films and concluded that the images obtained by the use of D-speed films and Digora sensor on both types of LCD monitors rendered a higher diagnostic ability compared to E-speed and F-speed films. (11)
Murat et al assessed the diagnosis of artificial secondary buccal caries under restorations with the use of different radiographic modalities and observed that CBCT images have a significantly higher diagnostic ability compared to PSP and conventional radiography. (12)
Nair et al evaluated the diagnostic accuracy of intraoral films (Ekta Speed) and different digital images including enhanced PSP and CCD for the detection of secondary caries; this study on 24 extracted posterior teeth showed that higher levels of contrast and brightness in digital images improved the diagnosis of secondary caries compared to conventional films. They also declared that the performance of CCD and PSP is not significantly different in the detection of secondary caries, (13) which is similar to the results of the current study.
De Araujo et al evaluated the presence of caries in 52 premolars (104 proximal surfaces) by using original and enhanced digital methods and E-speed and F-speed films. The results indicated that there is no significant difference between original digital images and radiographic films, while enhanced digital images had a significantly lower diagnostic accuracy in the detection of caries. (14)
One of the limitations of the present study was its small sample size. It seems that with increasing the number of samples, there might be a possibility of extracting significant statistical results. Since in-vitro conditions are different from oral conditions and it is impossible to precisely simulate the oral cavity in in-vitro studies, it seems that these conditions create some limitations in the extraction of significant statistical results, and only the results of in-vivo studies can be generalized to clinical situations.
One of the advantages of the present study was the use of a single software to eliminate interferences caused by different software programs. Our goal in using advanced technologies is to reach a better caries diagnosis. Therefore, in the present study, we used two sensors that are extremely new and popular among radiologists and dentists.
Considering the extensive research on the diagnosis of secondary caries and the importance of this topic, finding a more reliable method in line with the advancement of technology is a necessity. Overall, numerous factors influence the diagnostic ability of the observer, including the type of imaging modality (digital or conventional), the type of monitor or radiographic film, image enhancements, viewing conditions, and the experience of the observer. (15,16) Therefore, in addition to visual conditions, it seems that implementing the latest technology of monitor and sensor and best software programs with suitable designs is effective in making an accurate diagnosis of different lesions including carious lesions.
Since both PSP and CMOS systems are digital and two-dimensional (2D), they have similar advantages and disadvantages (similar sensitivity and specificity). We aimed to show that whether CMOS, as a superior technology, has some advantages over PSP; however, we did not find such advantages. An important issue in digital imaging is the experience of the observer, which can greatly influence the diagnosis of different lesions. It seems that an observer who has a greater experience in assessing digital images and is familiar with the related software programs has a higher diagnostic ability compared to an observer who has more experience in working with radiographic films. To reach more accurate and reliable diagnoses, the combined use of different radiographic systems and diagnostic tools such as DIAGNOdent is recommended. (17)
Conclusions
The results of the present study indicated that PSP and CMOS sensors are similar in the diagnosis of secondary caries under amalgam restorations. In addition, none of these sensors has the necessary diagnostic ability for the accurate and thorough diagnosis of secondary caries. It seems that further studies are necessary to reach a definitive conclusion.
Type of Study: Original article |
Subject:
Radiology
References
1. Mjör IA , Toffenetti F:secondary caries,a literatures review with case reports. Quintessence Int. 2000 Mar;31(3):165-79.
2. Jokstad A. Secondary caries and microleakage. Dent Mater. 2016 Jan;32(1):11-25.
3. Okida RC, Mandarino F, Sundfeld RH, de Alexandre RS, Sundefeld ML. In vitro evaluation of secondary caries formation around restoration. Bull Tokyo Dent Coll. 2008 Aug;49(3):121-8.
4. Jaberi Ansari Z, Valizadeh Haghi H. Secondary Caries in the Posterior Teeth of Patients Presenting to the Department of Operative Dentistry, Shahid Beheshti Dental School. J Dent Sch. 2014;32(3):125-31.
5. Fracaro MS, Seow WK, McAllan LH, Purdie DM. The sensitivity and specificity of clinical assessment compared with bitewing radiography for detection of occlusal dentin caries. Pediatr Dent. 2001 May-Jun;23(3):204-10.
6. Brouwer F, Askar H, Paris S, Schwendicke F. Detecting Secondary Caries Lesions. A Systematic Review and Meta-analysis J Dent Res. 2016 Feb;95(2):143-51.
7. Anas A, Asaad J, Tarboush K. A Comparison of intra-oral digital imaging modalities. Charged Couple Device versus Storage Phosphor Plate. Int J Health Sci (Qassim). 2010 Nov;4(2):156–67.
8. Williams CP. Digital radiography sensors: CCD, CMOS, and PSP. Pract Proced Aesthet Dent. 2001 Jun-Jul;13(5):395-6.
9. Syriopoulos K , Sanderink GC, Velders XL, van der Stelt PF.Radiographic detection of approximal caries: a comparison of dental films and digital imaging systems.Dentomaxillofac Radiol. 2000 Sep;29(5):312-8.
10. Castro VM , Katz JO, Hardman PK, Glaros AG, Spencer P. In vitro comparison of conventional film and direct digital imaging in the detection of approximal caries.Dentomaxillofac Radiol. 2007 Mar;36(3):138-42.
11. Ilgüy M , Dinçer S, Ilgüy D, Bayirli G.Detection of artificial occlusal caries in a phosphor imaging plate system with two types of LCD monitors versus three different films.J Digit Imaging. 2009 Jun;22(3):242-9.
12. Murat S, Kamburoğlu K, Isayev A, Kurşun S, Yüksel S. Visibility of artificial buccal recurrent caries under restorations using different radiographic techniques.Oper Dent 2013 Mar-Apr;38(2):197-207.
13. Nair MK , Ludlow JB, May KN, Nair UP, Johnson MP, Close JM.Diagnostic accuracy of intraoral film and direct digital images for detection of simulated recurrent decay.Oper Dent. 2001 May-Jun;26(3):223-30.
14. de Araujo EA , Castilho JC, Medici Filho E, de Moraes ME.Comparison of direct digital and conventional imaging with Ekta Speed Plus and INSIGHT films for the detection of approximal caries.Am J Dent. 2005 Aug;18(4):241-4.
15. Künzel A, Scherkowski D, Willers R, Becker J. Visually detectable resolution of intraoral dental films. Dentomaxillofac Radiol. 2003 Nov;32(6):385-9.
16. Møystad A, Svanaes DB, Risnes S, Larheim TA, Gröndahl HG. Detection of approximal caries with a storage phosphor system. A comparison of enhanced digital images with dental X-ray film. Dentomaxillofac Radiol. 1996 Sep;25(4):202-6.
17. Pedrosa RF, Brasileiro IV, dos Anjos Pontual ML, dos Anjos Pontual A, da Silveira MM. Influence of materials radiopacity in the radiographic diagnosis of secondary caries: evaluation in film and two digital systems. Dentomaxillofac Radiol. 2011 Sep;40(6):344-50.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |