

Volume 2, Issue 1 (3-2017)
J Res Dent Maxillofac Sci 2017, 2(1): 1-5 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Lesan S, Goudarzi N, Heidarnezhad H, Hassan Galyaie M. Comparison of the Prevalence of Geographic Tongue in Asthmatic Patients and Healthy Subjects in Masih Daneshvari Hospital in 2014. J Res Dent Maxillofac Sci 2017; 2 (1) :1-5
URL: http://jrdms.dentaliau.ac.ir/article-1-146-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-146-en.html


1- Assistant Professor, Oral and Maxillofacial Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran
2- , Oral Medecine Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran ,nastaran008@gmail.com
3- Professor of Chronic Respiratory Disease Research Center, Masih Daneshvari Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Dentist
2- , Oral Medecine Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran ,
3- Professor of Chronic Respiratory Disease Research Center, Masih Daneshvari Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Dentist
Full-Text [PDF 274 kb]
(2301 Downloads)
| Abstract (HTML) (5616 Views)
Abstract
Background and aim: Geographic tongue is a recurrent disorder with several associated etiologies. It is believed to be a common occurrence in the patients suffering from recurrent, acute inflammatory diseases. The purpose of this study was to compare the prevalence of geographic tongue between asthmatic patients and healthy subjects.
Materials and Methods: This descriptive-analytic study was conducted on 80 asthmatic patients and 80 healthy controls. The asthmatics were selected from among the patients presenting to Masih Daneshvari hospital with a confirmed diagnosis of asthma, while the healthy controls were selected from among patients' companions. The case and control subjects were matched according to age, sex and cigarette smoking status. The presence of geographic tongue was evaluated in the subjects by clinical examination and also by using a questionnaire. The data were entered into SPSS software version 22 and were evaluated using Chi-Square test.
Results: The prevalence of geographic tongue was 21.2% (n=17) in the asthmatic patients and 5% (n=4) in the healthy controls. A significant association was found between asthma and occurrence of geographic tongue (P<0.002). The incidence of geographic tongue in the asthmatics was 4.2 times greater than that in the healthy individuals with a relative risk (RR) equal to 4.2 and an attributable risk (AR) of 16%. In both groups, the dorsal and lateral surfaces of the tongue were more commonly affected than the ventral surface. No significant association was found between the involvement of a specific tongue surface and asthma (P=0.748).
Conclusion: According to the results, the asthmatic patients showed a significant higher prevalence of geographic tongue compared with the healthy controls.
Key words: Asthma; Geographic tongue; Prevalence
Introduction
Geographic tongue also known as benign migratory glossitis or erythema migrans is a recurrent disorder of the tongue. It is characterized by atrophy of the tongue epithelium and particularly the filiform papillae. It manifests as erythematous patches with yellowish-white prominent borders, commonly affecting the anterior two-thirds of the dorsal surface of the tongue (1,2,3). Geographic tongue rarely involves the ventral surface or other parts of the tongue. In the latter case, it is referred to as geographic stomatitis. The prevalence of geographic tongue has reported to be 2.4 to 28% in adults (2). Several factors such as hormonal changes, use of contraceptives, diabetes mellitus, allergic conditions i.e. atopy, hay fever, asthma and dermatological conditions such as psoriasis and Reiter's syndrome are believed to play a role in the occurrence of geographic tongue (1,4,5). Also, the association between geographic tongue and fissured tongue has been confirmed with a prevalence of 6-45% (6-11). Moreover, geographic tongue is a common sign in patients suffering from acute inflammatory diseases such as allergic rhinitis and asthma (4,5,12)
Asthma is a chronic inflammatory disease of the airways, characterized by hyperresponsiveness of airways to different stimuli. Physiologically, it is characterized by narrowing of the airways against the airflow, which resolves spontaneously or with treatment. Clinically, it manifests with dyspnea attacks, cough and wheezing. It is a periodic disease with attacks lasting for a few minutes to a couple of hours. In rare cases, it may even result in death (13-16).
Shulman et al assessed the prevalence and risk factors of geographic tongue among American adults and found no correlation between geographic tongue and age, sex, use of contraceptives, diabetes mellitus, allergy or dermatological conditions. They correlated the occurrence of geographic tongue to race (2). Miloglu et al demonstrated that geographic tongue is more prevalent in young nonsmokers and in atopic or allergic subjects and that it has no significant correlation with gender, dermatological conditions or systemic diseases. (17) However, Marks et al confirmed that geographic tongue was a sign of atopy (1). Marks et al stated that patients with atopy were more likely to develop inflammation of the fungiform papillae of the tongue than the general population (4). Also, in another study on 102 atopic patients, Marks et al reported a higher prevalence of geographic tongue associated with extrinsic asthma and/or rhinitis compared to healthy controls (5). Goregen et al revealed the correlation between geographic tongue and allergy by using patch and prick tests (18). Honarmand et al found a significant correlation between the incidence of geographic tongue and allergy in a group of Iranian population. (19) Ghapanchi et al showed that geographic tongue is one of the most prevalent oral lesions in asthmatic patients (20).
Based on the controversy regarding the prevalence of geographic tongue and its association with asthma as well as the high prevalence of geographic tongue in asthmatic patients reported in previous studies (5), this study aimed to compare the prevalence of geographic tongue between asthmatic patients and healthy subjects.
Materials and Methods
This cross-sectional study was conducted on 80 asthmatic patients and 80 healthy controls. A pilot study was conducted on 20 asthmatic patients to calculate the sample size, and the frequency of geographic tongue was found to be 35% (n=7) in the asthmatics and 5% in the healthy controls. Considering the 95% confidence interval, error of 5% and power of 90%, the sample size was calculated to be 80 subjects in each group. The asthmatic subjects were selected from among the patients presenting to Masih Daneshvari hospital, a referral center for respiratory diseases, while the healthy controls were selected from among patients' companions using targeted sampling. All the subjects signed written informed consent forms prior to participation in the study. The two groups of patients and controls were matched according to age, sex and cigarette smoking status (2, 17). Cigarette smoking was defined as smoking over 20 cigarettes a day for at least 10 years (21).
Asthmatic patients with a confirmed diagnosis of asthma recorded by a pulmonologist using the standard method (22) at the asthma department of Masih Daneshvari hospital, were selected and the required data were extracted from patients' files. The patients were also interviewed. The examined asthmatic patients had allergic rhinitis (sneezing, congestion, rhinorrhea and itchy nose) and reported no drug intake except for asthma medications (eg: beta 2 receptor agonist, Anticholinergic, Steroid, and Theophylline). Other systemic diseases such as diabetes mellitus, psoriasis, Reiter's syndrome, anemia, seborrheic dermatitis, hormonal disorders, eczema and oral mucosal lesions (other than geographic tongue) such as fissured tongue, depapillated tongue, extensive erythema of the tongue and median rhomboid glossitis were among the exclusion criteria in both groups.
Clinical oral examination of both the case and control groups was carried out for detection of geographic tongue, according to the World Health Organization’s guidelines (23). Geographic tongue was defined as multiple erythematous patches with white serpiginous borders and an atrophic center mainly involving the dorsal surface of the tongue. An expert examiner evaluated the ventral, dorsal and lateral surfaces of the tongue using a dental mirror under flash light and recorded the data in a questionnaire.
The data were entered into SPSS software version 22 (Microsoft, IL, USA) and were analyzed using Chi-Square test. The level of statistical significance was set at P<0/05.
Results
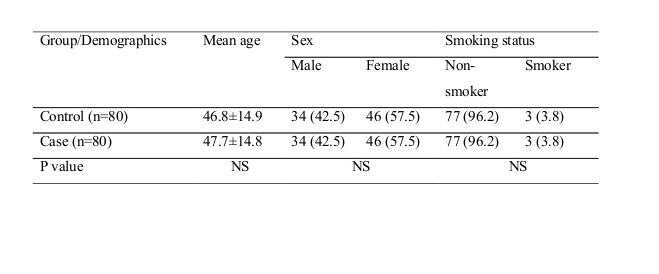
A total of 160 subjects including 80 asthmatic patients and 80 healthy controls were assessed. The case and control groups were matched according to age, sex and smoking status. (Table 1)
Table 1- Demographic information of subjects in the case (asthmatic) and control (healthy) groups
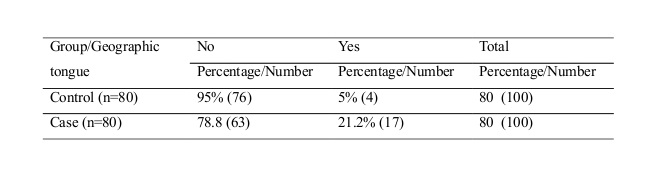
Table 2 shows the frequency distribution of geographic tongue based on asthma status. According to Chi-Square test, the difference was statistically significant (P<0.002).
Table 2-The frequency of geographic tongue in the case (asthmatic) and control (healthy) groups
The incidence of geographic tongue in the asthmatics was 4.2 times greater than that in the healthy individuals (relative risk, RR=4.2) with an attributable risk (AR) of 16%.
The frequency of involvement was 60% in the dorsal, 40% in the lateral and 0% in the ventral surface of the tongue for the control group and 56% in the dorsal, 40% in the lateral and 4% in the ventral surface of the tongue for the case group. No significant association was found between the involvement of a particular surface of the tongue and asthma (P=0.748).
Discussion
The etiology of geographic tongue has not been clearly understood. However, several factors such as stress, atopy, nutritional deficiency, candidiasis, diabetes mellitus, lichen planus and psoriasis are believed to play a role in its occurrence (1,3,4,5). Geographic tongue is an inflammatory disorder of the tongue. It is often asymptomatic and is an incidental finding during routine dental examinations (4,9). However, some patients complain of minor discomfort and burning sensation. Severe pain has been rarely reported. (24,25,26)
The current study evaluated the frequency of geographic tongue in two groups of asthmatic patients and healthy controls, matched for confounding factors such as age, sex and smoking status. The results revealed a significant association between asthma and occurrence of geographic tongue. This finding was in accord with the results of the studies by Marks et al (1) and Miloglu et al (17). Also, Alikhani et al (27) revealed that elevation of salivary levels of inflammatory cytokines was associated with the incidence of geographic tongue. However, the results of the present study were in contrast to the findings of Jainkittivong et al (28). This difference between our results and the results achieved by Jainkittivong et al is probably due to the difference in the population under study. In the study by Jainkittivong et al, the subjects with geographic tongue were evaluated to determine the presence of possible etiologic factors such as asthma (28).
In the present study, the prevalence of geographic tongue in the healthy controls was 5%. The prevalence of geographic tongue in the general population has been reported to be 6% (3, 19), which is in accordance with the value obtained in the current research. However, Shulman et al reported a prevalence rate of 1.8%. This difference in the obtained values can be probably attributed to the racial, ethnic and genetic differences of the populations under study (2).
One of the strength points of the current study was the evaluation of asthmatic patients and exclusion of subjects with other systemic conditions such as psoriasis, dermatitis, anemia, Reiter's syndrome, eczema, fissured tongue, etc. The subjects that reported intake of drugs such as antibiotics or hormonal medications were also excluded. Therefore, asthma and allergic rhinitis were the only variables that their effects on the development of geographic tongue were evaluated. This may explain the lower prevalence rate of geographic tongue in our study compared to other studies.
Our findings, as well as those of the above-mentioned studies indicate that the prevalence of geographic tongue is significantly higher in asthmatic patients compared to healthy individuals. However, it cannot be stated with certainty that whether this higher prevalence is due to the nature of asthma and allergic rhinitis or is the result of the use of medications for controlling asthma such as bronchodilators and inhaled or systemic corticosteroids (which also affect the oral mucosa and tongue) (29). However, the higher prevalence of geographic tongue in the patients suffering from other allergic conditions such as eczema, rash and hay fever compared to the healthy population elucidates this topic to some extent, since asthma medications are not prescribed for the above-mentioned conditions.
In the present study, the frequency of involvement of tongue surfaces was 56% in the dorsal, 40% in the lateral and 4% in the ventral surface of the tongue. These values were in line with the findings of Jainkittivong et al (28). The dorsal and lateral surfaces of the tongue were more commonly involved, while involvement of the ventral surface was only detected in one patient. This pattern of involvement has also been mentioned in previous studies (26). The current study found no association between the involved surface of the tongue and asthma (P=0.748). This assessment was another strength point in our study, since no previous study has evaluated this correlation.
Further studies with larger sample sizes and in different geographical locations are required to better elucidate the correlation between asthma and geographic tongue. Also, assessment of the serum level of IgE in asthmatic patients with geographic tongue and in otherwise healthy controls may yield interesting findings.
Conclusion
In the present study, the asthmatic patients showed a significant higher prevalence of geographic tongue than the healthy controls. Since the etiology of geographic tongue is yet unknown, this study can be considered as a scientific viewpoint.
Full-Text: (1074 Views)
Abstract
Background and aim: Geographic tongue is a recurrent disorder with several associated etiologies. It is believed to be a common occurrence in the patients suffering from recurrent, acute inflammatory diseases. The purpose of this study was to compare the prevalence of geographic tongue between asthmatic patients and healthy subjects.
Materials and Methods: This descriptive-analytic study was conducted on 80 asthmatic patients and 80 healthy controls. The asthmatics were selected from among the patients presenting to Masih Daneshvari hospital with a confirmed diagnosis of asthma, while the healthy controls were selected from among patients' companions. The case and control subjects were matched according to age, sex and cigarette smoking status. The presence of geographic tongue was evaluated in the subjects by clinical examination and also by using a questionnaire. The data were entered into SPSS software version 22 and were evaluated using Chi-Square test.
Results: The prevalence of geographic tongue was 21.2% (n=17) in the asthmatic patients and 5% (n=4) in the healthy controls. A significant association was found between asthma and occurrence of geographic tongue (P<0.002). The incidence of geographic tongue in the asthmatics was 4.2 times greater than that in the healthy individuals with a relative risk (RR) equal to 4.2 and an attributable risk (AR) of 16%. In both groups, the dorsal and lateral surfaces of the tongue were more commonly affected than the ventral surface. No significant association was found between the involvement of a specific tongue surface and asthma (P=0.748).
Conclusion: According to the results, the asthmatic patients showed a significant higher prevalence of geographic tongue compared with the healthy controls.
Key words: Asthma; Geographic tongue; Prevalence
Introduction
Geographic tongue also known as benign migratory glossitis or erythema migrans is a recurrent disorder of the tongue. It is characterized by atrophy of the tongue epithelium and particularly the filiform papillae. It manifests as erythematous patches with yellowish-white prominent borders, commonly affecting the anterior two-thirds of the dorsal surface of the tongue (1,2,3). Geographic tongue rarely involves the ventral surface or other parts of the tongue. In the latter case, it is referred to as geographic stomatitis. The prevalence of geographic tongue has reported to be 2.4 to 28% in adults (2). Several factors such as hormonal changes, use of contraceptives, diabetes mellitus, allergic conditions i.e. atopy, hay fever, asthma and dermatological conditions such as psoriasis and Reiter's syndrome are believed to play a role in the occurrence of geographic tongue (1,4,5). Also, the association between geographic tongue and fissured tongue has been confirmed with a prevalence of 6-45% (6-11). Moreover, geographic tongue is a common sign in patients suffering from acute inflammatory diseases such as allergic rhinitis and asthma (4,5,12)
Asthma is a chronic inflammatory disease of the airways, characterized by hyperresponsiveness of airways to different stimuli. Physiologically, it is characterized by narrowing of the airways against the airflow, which resolves spontaneously or with treatment. Clinically, it manifests with dyspnea attacks, cough and wheezing. It is a periodic disease with attacks lasting for a few minutes to a couple of hours. In rare cases, it may even result in death (13-16).
Shulman et al assessed the prevalence and risk factors of geographic tongue among American adults and found no correlation between geographic tongue and age, sex, use of contraceptives, diabetes mellitus, allergy or dermatological conditions. They correlated the occurrence of geographic tongue to race (2). Miloglu et al demonstrated that geographic tongue is more prevalent in young nonsmokers and in atopic or allergic subjects and that it has no significant correlation with gender, dermatological conditions or systemic diseases. (17) However, Marks et al confirmed that geographic tongue was a sign of atopy (1). Marks et al stated that patients with atopy were more likely to develop inflammation of the fungiform papillae of the tongue than the general population (4). Also, in another study on 102 atopic patients, Marks et al reported a higher prevalence of geographic tongue associated with extrinsic asthma and/or rhinitis compared to healthy controls (5). Goregen et al revealed the correlation between geographic tongue and allergy by using patch and prick tests (18). Honarmand et al found a significant correlation between the incidence of geographic tongue and allergy in a group of Iranian population. (19) Ghapanchi et al showed that geographic tongue is one of the most prevalent oral lesions in asthmatic patients (20).
Based on the controversy regarding the prevalence of geographic tongue and its association with asthma as well as the high prevalence of geographic tongue in asthmatic patients reported in previous studies (5), this study aimed to compare the prevalence of geographic tongue between asthmatic patients and healthy subjects.
Materials and Methods
This cross-sectional study was conducted on 80 asthmatic patients and 80 healthy controls. A pilot study was conducted on 20 asthmatic patients to calculate the sample size, and the frequency of geographic tongue was found to be 35% (n=7) in the asthmatics and 5% in the healthy controls. Considering the 95% confidence interval, error of 5% and power of 90%, the sample size was calculated to be 80 subjects in each group. The asthmatic subjects were selected from among the patients presenting to Masih Daneshvari hospital, a referral center for respiratory diseases, while the healthy controls were selected from among patients' companions using targeted sampling. All the subjects signed written informed consent forms prior to participation in the study. The two groups of patients and controls were matched according to age, sex and cigarette smoking status (2, 17). Cigarette smoking was defined as smoking over 20 cigarettes a day for at least 10 years (21).
Asthmatic patients with a confirmed diagnosis of asthma recorded by a pulmonologist using the standard method (22) at the asthma department of Masih Daneshvari hospital, were selected and the required data were extracted from patients' files. The patients were also interviewed. The examined asthmatic patients had allergic rhinitis (sneezing, congestion, rhinorrhea and itchy nose) and reported no drug intake except for asthma medications (eg: beta 2 receptor agonist, Anticholinergic, Steroid, and Theophylline). Other systemic diseases such as diabetes mellitus, psoriasis, Reiter's syndrome, anemia, seborrheic dermatitis, hormonal disorders, eczema and oral mucosal lesions (other than geographic tongue) such as fissured tongue, depapillated tongue, extensive erythema of the tongue and median rhomboid glossitis were among the exclusion criteria in both groups.
Clinical oral examination of both the case and control groups was carried out for detection of geographic tongue, according to the World Health Organization’s guidelines (23). Geographic tongue was defined as multiple erythematous patches with white serpiginous borders and an atrophic center mainly involving the dorsal surface of the tongue. An expert examiner evaluated the ventral, dorsal and lateral surfaces of the tongue using a dental mirror under flash light and recorded the data in a questionnaire.
The data were entered into SPSS software version 22 (Microsoft, IL, USA) and were analyzed using Chi-Square test. The level of statistical significance was set at P<0/05.
Results
A total of 160 subjects including 80 asthmatic patients and 80 healthy controls were assessed. The case and control groups were matched according to age, sex and smoking status. (Table 1)
Table 1- Demographic information of subjects in the case (asthmatic) and control (healthy) groups
{kind=link}
Table 2 shows the frequency distribution of geographic tongue based on asthma status. According to Chi-Square test, the difference was statistically significant (P<0.002).
Table 2-The frequency of geographic tongue in the case (asthmatic) and control (healthy) groups
{kind=link}
The incidence of geographic tongue in the asthmatics was 4.2 times greater than that in the healthy individuals (relative risk, RR=4.2) with an attributable risk (AR) of 16%.
The frequency of involvement was 60% in the dorsal, 40% in the lateral and 0% in the ventral surface of the tongue for the control group and 56% in the dorsal, 40% in the lateral and 4% in the ventral surface of the tongue for the case group. No significant association was found between the involvement of a particular surface of the tongue and asthma (P=0.748).
Discussion
The etiology of geographic tongue has not been clearly understood. However, several factors such as stress, atopy, nutritional deficiency, candidiasis, diabetes mellitus, lichen planus and psoriasis are believed to play a role in its occurrence (1,3,4,5). Geographic tongue is an inflammatory disorder of the tongue. It is often asymptomatic and is an incidental finding during routine dental examinations (4,9). However, some patients complain of minor discomfort and burning sensation. Severe pain has been rarely reported. (24,25,26)
The current study evaluated the frequency of geographic tongue in two groups of asthmatic patients and healthy controls, matched for confounding factors such as age, sex and smoking status. The results revealed a significant association between asthma and occurrence of geographic tongue. This finding was in accord with the results of the studies by Marks et al (1) and Miloglu et al (17). Also, Alikhani et al (27) revealed that elevation of salivary levels of inflammatory cytokines was associated with the incidence of geographic tongue. However, the results of the present study were in contrast to the findings of Jainkittivong et al (28). This difference between our results and the results achieved by Jainkittivong et al is probably due to the difference in the population under study. In the study by Jainkittivong et al, the subjects with geographic tongue were evaluated to determine the presence of possible etiologic factors such as asthma (28).
In the present study, the prevalence of geographic tongue in the healthy controls was 5%. The prevalence of geographic tongue in the general population has been reported to be 6% (3, 19), which is in accordance with the value obtained in the current research. However, Shulman et al reported a prevalence rate of 1.8%. This difference in the obtained values can be probably attributed to the racial, ethnic and genetic differences of the populations under study (2).
One of the strength points of the current study was the evaluation of asthmatic patients and exclusion of subjects with other systemic conditions such as psoriasis, dermatitis, anemia, Reiter's syndrome, eczema, fissured tongue, etc. The subjects that reported intake of drugs such as antibiotics or hormonal medications were also excluded. Therefore, asthma and allergic rhinitis were the only variables that their effects on the development of geographic tongue were evaluated. This may explain the lower prevalence rate of geographic tongue in our study compared to other studies.
Our findings, as well as those of the above-mentioned studies indicate that the prevalence of geographic tongue is significantly higher in asthmatic patients compared to healthy individuals. However, it cannot be stated with certainty that whether this higher prevalence is due to the nature of asthma and allergic rhinitis or is the result of the use of medications for controlling asthma such as bronchodilators and inhaled or systemic corticosteroids (which also affect the oral mucosa and tongue) (29). However, the higher prevalence of geographic tongue in the patients suffering from other allergic conditions such as eczema, rash and hay fever compared to the healthy population elucidates this topic to some extent, since asthma medications are not prescribed for the above-mentioned conditions.
In the present study, the frequency of involvement of tongue surfaces was 56% in the dorsal, 40% in the lateral and 4% in the ventral surface of the tongue. These values were in line with the findings of Jainkittivong et al (28). The dorsal and lateral surfaces of the tongue were more commonly involved, while involvement of the ventral surface was only detected in one patient. This pattern of involvement has also been mentioned in previous studies (26). The current study found no association between the involved surface of the tongue and asthma (P=0.748). This assessment was another strength point in our study, since no previous study has evaluated this correlation.
Further studies with larger sample sizes and in different geographical locations are required to better elucidate the correlation between asthma and geographic tongue. Also, assessment of the serum level of IgE in asthmatic patients with geographic tongue and in otherwise healthy controls may yield interesting findings.
Conclusion
In the present study, the asthmatic patients showed a significant higher prevalence of geographic tongue than the healthy controls. Since the etiology of geographic tongue is yet unknown, this study can be considered as a scientific viewpoint.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Marks R, Simons MJ. Geographic tongue--a manifestation of atopy. Br J Dermatol 1979;101(2):159-62.
2. Shulman JD, Carpenter WM. Prevalence and risk factors associated with geographic tongue among US adults. Oral Dis 2006;12(4):381-6.
3. Scariot R, Batista TB, Olandoski M, Souza CM, souza PH, Lima AA, et al. Host and clinical aspects in patients with benign migratory glossitis. Arch Oral Biol 2017; 73:259-268.
4. Marks R, Scarff CE, Yap LM, Verlinden V, Jolley D, Campbell J. Fungiform papillary glossitis: atopic disease in the mouth? Br J Dermatol 2005;153(4):740-5.
5. Marks R, Czarny D. Geographic tongue: sensitivity to the environment. Oral Surg Oral Med Oral Pathol 1984;58(2):156-9.
6. Sedano HO, Carreon Freyre I, Garza de la Garza ML, Gomar Franco CM, Grimaldo Hernandez C, Hernandez Montoya ME, et al. Clinical orodental abnormalities in Mexican children. Oral Surg Oral Med Oral Pathol 1989;68(3):300-11.
7. Darwazeh AM, Pillai K. Prevalence of tongue lesions in 1013 Jordanian dental outpatients. Community Dent Oral Epidemiol 1993;21(5):323-4.
8. Ghosack A, Zadik D, Eidelman E. The prevalence of scrotal tongue and geographic tongue n 70,359 israeli school children. Community Dent Oral Epidemiol 1974;2(5):253-7.
9. Redman RS. Prevalence of geographic tongue, fissured tongue, median rhomboid glossitis, and hairy tongue among 3,611 Minnesota schoolchildren. Oral Surg Oral Med Oral Pathol 1970;30(3):390-5.
10. Aboyans V, Ghaemmaghami A. The incidence of fissured tongue among 4,009 Iranian dental outpatients. Oral Surg Oral Med Oral Pathol 1973;36(1):34-8.
11. Correll RW, Wescott WB, Jensen JL. Nonpainful, erythematous, circinate lesions of a protean nature on a fissured tongue. J Am Dent Assoc 1984;109(1):90-1.
12. Hashemi pour MAS, Zarei MR, Farokh giso E, Dastbous A. Study of the relations between inflammatory condition of geographic tongue and allergy. daneshvarmed 2008;15(74):77-84
13. Murdoch JR, Lloyd CM. Chronic inflammation and asthma. Mutat Res 2010 7;690(1-2):24-39.
14. Sheffer AL. Death due to asthma. Allergology International 1996;45(2):67-71.
15. Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, et al."Trends in asthma prevalence, health care use, and mortality in the United States, 2001-2010. NCHS Data Brief 2012;(94):1-8.
16. De Souza-Machado C, Souza-Machado A, Cruz AA. Asthma mortality inequalities in Brazil: tolerating the unbearable. ScientificWorldJournal 2012;2012:625829.
17. Miloglu O, Goergen M, Akgul HM, Acemoglu H. The prevalence and risk factors associated with benign migratory glossitis in 7619 Turkish dental outpatients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107(2):e29-33.
18. Goregen M, Melikoglu M, Miloglu O, Erdem T. Predisposition of allergy in patients with benign migratory glossitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110(4):470-4.
19. Honarmand M, FarhadMollashahi L, Shirzaiy M, Sehhatpour M. Geographic Tongue and Associated Risk Factors among Iranian Dental Patients. Iran J Public Health 2013;42(2):215-9.
20. Ghapanchi J, Rezazadeh F, Kamali F, Rezaee M, Ghodrati M, Amanpour S. Oral manifestations of asthmatic patients. J Pak Med Assoc 2015; 65(11),1226-7.
21. Reznick AZ, Klein I, Eiserich JP, Cross CE, Nagler RM. Inhibition of oral peroxidase activity by cigarette smoke: in vivo and in vitro studies. Free radic biol med 2003;34(3): 377-84.
22. Bousquet J, Mantzouranis E, Cruz AA, Ait-Khaled N, Baena-Cagnani CE, Bleecker ER, et al. Uniform definition of asthma severity, control, and exacerbations: document presented for the World Health Organization consultation on sever asthma. J Allergy Clin Immunol 2010;126(5): 926-38.
23. Kramer IR, Pindborg JJ, Bezroukov V, Infirri JS. Guide to epidemiology and diagnosis of oral mucosal diseases and conditions. World Health Organization. Community Dent Oral Epidemiol 1980;8(1):1-26.
24. Kuffer R, Brochériou C, Cernéa P. [Exfoliatoareata linguae et mucosae oris]. Rev StomatolChirMaxillofac 1971;72(1):109-19.
25. Pass B, Brown RS, Childers EL. Geographic tongue: literature review and case reports. Dent Today 2005;24(8): 56-7.
26. Goswami M, Verma A, Verma M. Benign migratory glossitis with fissured tongue. J Indian Soc Pedod Prev Dent 2012;30(2):173-5.
27. Alikhani M, Khalighinejad N, Ghalaiani P, khaleghi MA, Askari E, Gorsky M. Immunologic and psychologic parameters associated with geographic tongue. Oral Surg Oral Med Oral Pathol Oral Radiol 2014;118(1):68-71.
28. Jainkittivong A, Langlais RP. Geographic tongue: clinical characteristics of 188 cases. J Contemp Dent Pract 2005;6(1):123-35.
29. Godara N, Godara R, Khullar M. Impact of inhalation therapy on oral health. Lung India 2011;28(4):272-5.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
