

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-137-en.html


2- Professor, Department of Oral Pathology, Faculty of Dentistry, mashhad University of Medical Sciences, Mashhad, Iran
3- Assistant professor,Oral Pathology Dept, Faculty of Dentistry,urmia University of Medical Sciences, Urmia, Iran ,
Abstract
Background and aim: Basal Cell Carcinoma (BCC) is the most common skin neoplasm and the most common type of cancer. Since the incidence of injury is taken into consideration in the pathologic diagnosis, the study of clinical and microscopic views of BCC is of particular importance. The present study aimed at determining the frequency of clinical and microscopic views of BCC in a 10-year period in Ilam province.
Materials and Methods: This study is descriptive. The study population consisted of all the subjects with BCC in the head and neck area referring to the pathology department of Imam Khomeini hospital in Ilam province in a 10-year period. The data were entered into SPSS 19 software and were analyzed using descriptive statistical methods and Chi-Square test.
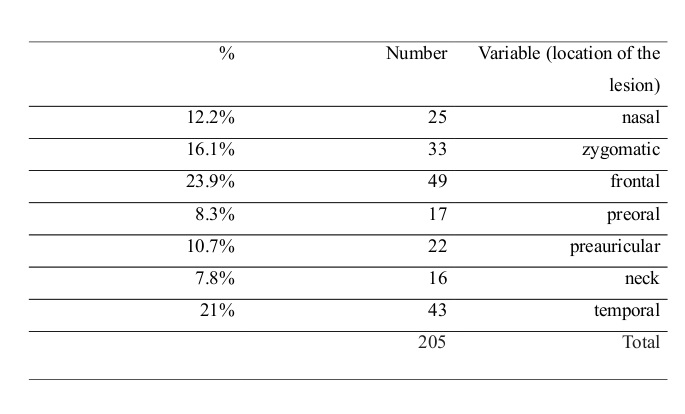
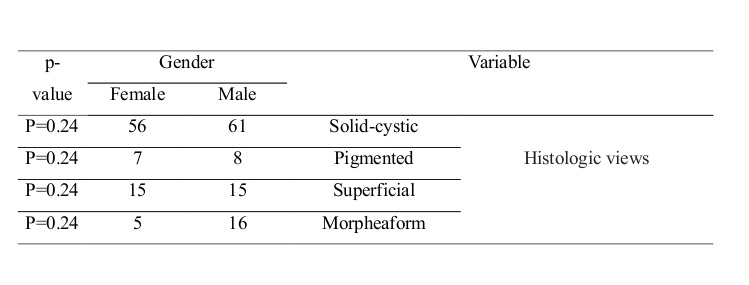
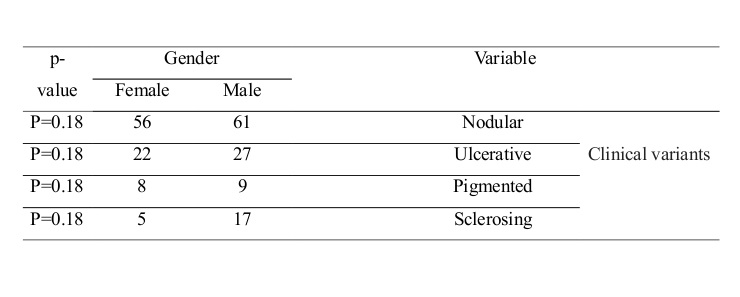
Results: In the present study, 205 patients were diagnosed with BCC. The maximum and minimum frequency rates of the lesion were detected in the frontal area (9.23%) and neck (8.7%), respectively. The maximum frequency was related to the nodular type (57.1%), while the pigmented variant showed the lowest rate (8.3%). Among the evaluated microscopic variants, maximum views were related to the solid-cystic type (57.1%), while minimum views were related to the pigmented variant (37.3%). There was no significant correlation between the location of the lesion in males and females (p=0.14) or between the location of the lesion and age (p=0.16).
Conclusion: The results of this study showed that the nodular type was the most common clinical variant of BCC, while the least common type was the pigmented variant. The most common histological type was the solid-cystic type, while the pigmented variant was the least common type.
Keywords: skin neoplasms, Basal Cell Carcinoma, cancer
Introduction
The term "head and neck cancer" encompasses various tumors appearing in the throat, larynx, nose, sinuses, and mouth. Malignant tumors in the head and neck may be of epithelial or mesenchymal origin (1). Basal Cell Carcinoma (BCC) is the most common skin neoplasm and the most common type of cancer. This tumor is a primary epithelial malignant lesion with local invasion and slow growth that arises from the basal layer of the skin and its appurtenances (2). It involves the scalp and neck in about 85% of cases, and white adults are most frequently involved, especially those with fair skin, blond hair and blue or green eyes over 40 years of age (3). More than 800,000 new cases of BCC are diagnosed in the United States every year. The incidence of lesions is increasing by 10% annually worldwide. Generally, the incidence increases with age (4,5). This cancer mainly occurs after long-term exposure to ultraviolet radiation. Repeated sunburns in childhood, immunosuppressive therapy, arsenic ingestion, and multiple genodermatoses are associated with the formation of BCC (6).The most common clinical type of the lesion is the ulcerative nodular type, which starts as a stiff and painless papule that grows slowly and causes an expanding wound at the center of the lesion that can destroy the underlying structures if being left untreated (7). Other clinical and pathological types of the lesion are the pigmented, sclerosing, and superficial types. The treatment methods are excisional surgery, lasers, radiotherapy, and frozen section, and depend on the size and location of the lesions (8, 9). Recurrence of a properly treated BCC is uncommon, and metastasis is extremely rare (10). Patients with uncontrolled disease usually lose their lives due to local invasion of the lesion to critical organs (11). Considering the importance of early detection and the necessity of treating this carcinoma, epidemiological study, timely diagnosis, and quick treatment of the tumor are mandatory. Knowledge about the prevalence of different types of this tumor and their clinical characteristics, such as age, gender predilection, and location of occurrence, helps clinicians to reach a correct diagnosis.
Since the incidence of injury is taken into consideration in the pathological diagnosis, the study of clinical and microscopic views of BCC is of particular importance, as accurate and timely diagnosis of BCC is crucial (12). The results of the conducted studies can help in early diagnosis and treatment of the lesions and consequently can prevent further side effects (13). This study examined the frequency of clinical and microscopic views of BCC in a 10-year period in Ilam province to gather comprehensive information regarding the frequency of clinical and microscopic variants of BCC.
Materials and Methods
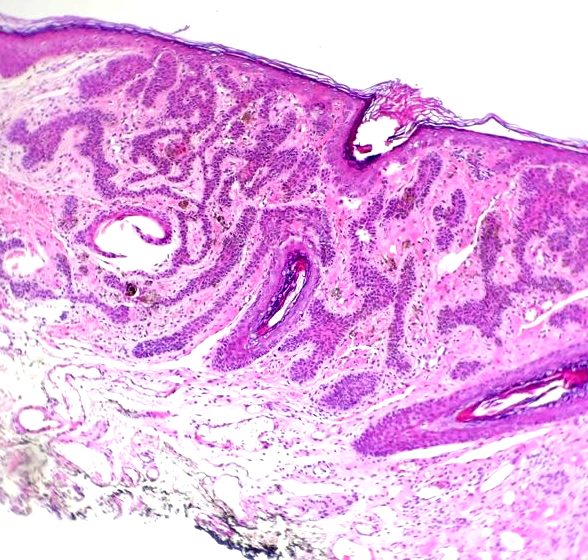
This study is descriptive. All the pathology files of the patients with BCC in the head and neck admitted to, hospitalized and treated in Ilam’s Imam Khomeini Hospital from 2004 to 2015 were studied. After selecting the files, the required information such as age, sex, location of the lesion, and microscopic diagnosis of the lesions were recorded in designated tables. Afterwards, the incidence and types of microscopic views of BCC in the head and neck were examined based on age, sex, location of the lesion and tumor type. Several clinicopathologic variants of BCC have been described. The most common form of this lesion is the nodular BCC which is a firm painless papule that slowly enlarges and develops a central depression and an umbilicated appearance. Pigmented BCC is a noduloulcerative tumor colonized by benign melanocytes. Sclerosing type (morpheaform) of BCC often mimics scar tissue. The superficial BCC is comprised of multiple and well-demarcated, erythematous scaly patches that may be clinically misdiagnosed as psoriasis (1, 2). The solid-cystic type of BCC is comprised of uniform ovoid dark-staining basaloid cells with moderate-sized nuclei and little cytoplasm. The cells are arranged into well-demarcated islands and strands, which appear to arise from the basal cell layer of the overlying epidermis that invade the underlying dermal connective tissue. Epithelial islands typically demonstrate palisading of the peripheral cells. A clear zone of artifactual retraction is seen between the epithelial islands and the connective tissue. In pigmented type of BCC, melanocytes are seen within tumor islands. Sclerosing BCC is characterized by strands of basaloid tumor cells in a densely collagenous background. Superficial BCC includes lobules of tumor cells that drop from the epidermis in a multifocal pattern (3, 4). The patient files with incomplete information and without definite diagnosis of the lesions and the ones related to the recurrence of the lesion were excluded. The data were entered into SPSS 19 software and were analyzed using descriptive statistical methods (mean, standard deviation, frequency and percentage), mean comparisons, and Chi-Square test.
Results
In this study, 205 subjects with the average age of 69.7±10.2 years were examined. Minimum and maximum ages of the patients were 47 and 95 years, respectively. Most cases were between 63 to 78 years old (47.3%). 114 cases (55.6%) were males and 91 subjects (44.4%) were females (Table 1). The highest incidence of the lesion was detected in the frontal region (23.9%), while the lowest incidence was found in the neck (7.8%) (Table 2). The most frequently encountered clinical variant of BCC was the nodular type (57.1%), while the lowest incidence was related to the pigmented type (8.3%). Among the microscopic variants, the highest frequency was related to the solid-cystic variant (57.1%), while the pigmented type showed the lowest frequency (7.3%). (Table 3) (Figures 1 to 4) There was no significant correlation between the location of the lesion in men and women (p=0.14) or between the location of the lesion and age (p=0.16). (Table 4) The correlation between the microscopic variants of BCC and gender was statistically significant (p=0.03). Likewise, the correlation between the clinical variants of BCC and gender was statistically significant (p=0.01). The statistical approach of the present study was to assess the degree of 95%.
Tabel 1- The age group under review
Table 2- Incidence rates of BCC in different regions of the head and neck
Table 3- Microscopic variants of BCC in the head and neck based on gender
Table 4- Clinical variants of BCC in the head and neck based on gender
Figure 1- Solid-cystic BCC (H&E staining, magnification×20)
Figure 2- Pigmented BCC (H&E staining, magnification×20)
Figure 3- Superficial BCC (H&E staining, magnification×20)
Figure 4- Sclerosing (morpheaform) BCC (H&E staining,magnification ×20)
Discussion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
The results of the current study showed that most patients were between 63 to 78 years old (47.3%). Some studies have indicated that the disease is more common in those aged over 40 years (14,15). Jurciukonyte et al and Vantuchová et al have reported the incidence rates of 75% and 65% in men, respectively (16-17), which is consistent with the results of the present study. 55.6% of the subjects were males, similar to the study that has reported the prevalence of the lesion to be 30% higher in males (3, 18). This is also consistent with the results of the studies that have reported higher incidence rates of this cancer in men (4, 15, 19). The results of the present study indicated that the most common location of BCC was the frontal region (23.9%), which contradicts the results of the study that has reported the nasal area as the most common location for this lesion (27.4%) (15). In the present study, the most frequent microscopic view of BCC was related to the nodular type (57.1%), which was also the most common variant in both women and men. This result confirms the results of previous studies, which indicated that the most common clinical form of the lesion is the nodular type (1, 6, 15, 18,20).
The most common location of the lesions was the temporal area in men, which was similar to the results of the study by Puizina-Ivic et al that reported the incidence of 14.6% (14). The most common location of the lesion in women was the forehead, similar to the results of a study that declared the incidence of 8.7% (13). This result was incompatible with the results of the study that reported the cheeks to be the most common location of the lesion in women (16). The results indicated that due to direct exposure to sunlight, the temporal area in men tends to show the highest incidence of the lesions, whereas the incidence of the lesions in this area is low in women, as it is often covered by hair or a scarf. The most common microscopic variant of BCC was the solid-cystic type in both males and females, similar to the results of previous studies (13, 15, 17). Most authors believe that the nodular type of BCC has a low tendency for local recurrence, while the superficial type is high risk in this regard. According to previous studies, the nodular type comprises 75% of all BCCs (4, 10, 11). Similar results were achieved in the present study. Treatment methods for BCC include: surgical excision, mohs surgery, cryosurgery, chemotherapy and radiation (1, 9, 13). The nodular variant has a better prognosis than the other subtypes (4, 8).
Conclusion
The results of this study showed that the most common clinical variant of BCC was the nodular type, while the least common type was the pigmented variant. The most common histological type was the solid-cystic type, while the pigmented form was the least common variant.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |