Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 1 (3-2026)
J Res Dent Maxillofac Sci 2026, 11(1): 1-7 |
Back to browse issues page
Ethics code: IR.IAU.DENTAL.REC.1401.006.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yaghoubi Baghlouei S K, Fazlyab M, Esnaashari E, PourHajiBagher M, Kamali S. Antibacterial Effect of Low-Level Laser on Four-Week-Old Biofilm of Enterococcus faecalis in Presence of Intracanal Medicaments: An In Vitro Study. J Res Dent Maxillofac Sci 2026; 11 (1) :1-7
URL: http://jrdms.dentaliau.ac.ir/article-1-964-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-964-en.html
Seyed Khalegh Yaghoubi Baghlouei1 
 , Mahta Fazlyab1 , Ehsan Esnaashari1 , Maryam PourHajiBagher2 , Siavash Kamali *3
, Mahta Fazlyab1 , Ehsan Esnaashari1 , Maryam PourHajiBagher2 , Siavash Kamali *3
, Mahta Fazlyab1 , Ehsan Esnaashari1 , Maryam PourHajiBagher2 , Siavash Kamali *3
1- Department of Endodontics, TeMS.C., Islamic Azad University, Tehran, Iran
2- Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran
3- Department of Endodontics, TeMS.C., Islamic Azad University, Tehran, Iran ,Siavash199x@gmail.com
2- Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran
3- Department of Endodontics, TeMS.C., Islamic Azad University, Tehran, Iran ,
Keywords: Calcium Hydroxide, Drug Resistance, Microbial, Enterococcus faecalis, Low-Level Light Therapy
Full-Text [PDF 410 kb]
(38 Downloads)
| Abstract (HTML) (55 Views)
Full-Text: (21 Views)
Abstract
Background and Aim: This in vitro study assessed the impact of low-level laser irradiation (LLLI) on resistance of Enterococcus faecalis (E. faecalis) to calcium hydroxide (CH) and triple antibiotic paste (TAP) intracanal medicaments.
Materials and Methods: In this in vitro study, 44 extracted single-rooted human teeth were categorized into 6 groups of negative control (n=2), positive control (n=2), TAP (n=10), CH (n=10), TAP+LLLI (n=10), and CH+LLLI (n=10). Following preparation, the samples were transferred to brain heart infusion (BHI) broth and incubated at 37°C for 24 hours; 1 mL of E. faecalis (ATCC 29212) suspension was injected into the canals and incubated for 4 weeks for biofilm formation. CH and TAP were introduced into the canals, depending on group allocation of the teeth, and LLLI with performed for 15 seconds using 980 nm diode laser with an energy density of 6.89 J/cm², power-output of 0.5 W, and a tip diameter of 10 mm. After 2 weeks, canal debris was removed using #4 Gates-Glidden drills and incubated in BHI at 37°C for 8 hours. Then, 100 μL of the dilution was cultured to determine the number of colony-forming units (CFUs), indicating the effectiveness of disinfection, after 12 hours. Data were analyzed with one-way ANOVA (alpha=0.05).
Results: The four groups had no significant difference in colony count (P=0.483).
Conclusion: The results of this study indicated that LLLI in combination with CH or TAP did not lead to a significant reduction in colony count compared to the use of CH or TAP alone.
Keywords: Calcium Hydroxide; Drug Resistance, Microbial; Enterococcus faecalis; Low-Level Light Therapy
Introduction
Indiscriminate use of antibiotics is contributing to escalating drug resistance in bacteria, resulting in life-threatening diseases and a rising economic burden. The escalating threat of drug-resistant bacteria has generated an urgent need for novel antibacterial therapies and effective agents. In root canal therapy, physiological alterations induced by cells may contribute to microbial resistance to antiseptic drugs [1]. During root canal therapy, medicaments like triple antibiotic paste (TAP) or calcium hydroxide (CH) are often used to eradicate microorganisms from the root canal system. These medicaments remain in the root canal system for a duration ranging from 1 week to 1 month. During this time interval, they may induce antibiotic resistance [2].
Low-level laser irradiation (LLLI) was first used for treatment of severe enamel and dentin caries in 1960 [3]. Low-power or low-level lasers are defined as Class 3 lasers with an output power below 0.5 W. They are non-invasive and do not produce heat, noise, or vibrations during treatment [4]. Currently, LLLI is commonly performed for pain management following endodontic procedures. The mechanism of pain control by LLLI involves reduction of prostaglandin, interleukin-1 beta, and tumor necrosis factor-alpha production [5]. LLLI modulates fibroblast function at the tissue level, facilitating connective tissue repair and exerting anti-inflammatory effects [6,7]. Furthermore, it expedites angiogenesis while simultaneously enhancing cellular metabolism. While LLLI is effective in alleviating pain, it may potentially enhance bacterial resistance to antimicrobial drugs by inducing processes such as the filamentation phenotype [8]. Studies have shown that LLLI can induce resistance of bacterial strains such as Escherichia coli susceptible to H2O2, [9, 10].
Enterococcus faecalis (E. faecalis) is the main microorganism found in endodontically treated teeth with periradicular lesions. It is isolated from the root canals of 24% to 77% of patients with persistent endodontic infections [11]. E. faecalis is a common, potentially pathogenic strain with a confirmed resistance to different disinfectants and medicaments [12]. LLLI may upregulate anti-inflammatory phenomena in host cells and reduce post-treatment pain [5-7]. Thus, using LLLI to control pain after root canal treatment may make intracanal bacteria more resistant to antimicrobial agents through its photo-biomodulation effects on bacterial cells. Several studies have shown that various laser-based methods for root canal disinfection can effectively reduce the bacterial count within the canal [13,14]. No information exists regarding the combined effects of LLLI and intracanal medicament application on bacterial count in the canal. Thus, this study aimed to evaluate the impact of LLLI on the resistance of E. faecalis to CH and TAP intracanal medicaments in the root canal system. The null hypothesis tested was that LLLI would not increase the resistance of E. faecalis to CH and TAP intracanal medicaments.
Materials and Methods
This in vitro study received approval from the Research Ethics Committees of Islamic Azad University-Dental Branch, Tehran, under protocol number IR.IAU.DENTAL.REC.1401.006.
Single-rooted human teeth with straight canals that had been extracted as part of an orthodontic/periodontal treatment plan were selected for this study. Teeth with calcified canals, root caries, open apices, canal curvatures of more than 15 degrees according to the method described by Schneider [15], internal or external root resorption, and cracks were excluded through visual inspection and periapical radiography [16].
Sample size calculation:
Considering the power of β=0.2, α=0.05, a standard deviation of 1.2%, and an effect size of 0.28 obtained from a previous study [16], the sample size was calculated to be 10 in each group.
Tooth sample preparation:
This study involved 44 human single-rooted teeth extracted due to unfavorable periodontal prognosis or orthodontic treatment plan. The teeth were cleaned by removing calculus and soft tissue debris using a scaler, followed by immersion in 5.25% NaOCl (Golrang, Tehran, Iran) for 10 minutes [17]. The teeth were then rinsed with distilled water for 5 minutes. The crowns were cut just below the cementoenamel junction using a high-speed handpiece and a cylindrical diamond bur under water cooling. The apical foramina were sealed with light-cure glass ionomer cement (Fuji 2 LC; GC, Tokyo, Japan). The samples were then divided into six groups: one negative control group (n=2), one positive control group (n=2), and four experimental groups (n=10). All samples were placed in 1.5 mL Eppendorf tubes and sterilized with 40 kGy gamma radiation (GC-220 Gamacell, Nordion, Canada) [16].
In all groups, root canal patency was confirmed before instrumentation. A #15 K-file (Dentsply, Maillefer, Tulsa, OK, USA) was inserted into the canal until the tip was visible at the apex; then, the working length was set by withdrawing 0.5 mm. Root canal preparation was performed with the crown-down technique using the ProTaper rotary system (Dentsply Maillefer, Ballaigues, Switzerland) from S1 to F3, operating with a torque-limited electric motor (Endo IT motor; VDW, Munich, Germany) at 300 rpm and 3 N/cm torque. Irrigation was performed with 5.25% sodium hypochlorite (Golrang, Tehran, Iran), followed by 3 mL of 17% EDTA (Morva Bon, Tehran, Iran) to remove the smear layer. This was followed by a 5-minute rinse with an additional 3 mL of 5.25% sodium hypochlorite. To neutralize residual hypochlorite, the canals were irrigated with sodium thiosulfate (Sigma-Aldrich, St. Louis, MO, USA) and finally rinsed with 10 mL of sterile saline for 5 minutes [18,19]. The samples were then transferred to brain heart infusion (BHI) broth and incubated at 37°C for 24 hours. Absence of bacterial growth indicated effective sterilization.
E. faecalis (ATCC 29212; Pasteur Institute of Iran) was cultured in BHI broth for 8 hours, and a suspension with a concentration of 108 bacteria/mL was prepared spectrophotometrically at 600 nm. One milliliter of this suspension was injected into the sterile root canals using a 30-gauge irrigation needle (ProRinse; Dentsply Sirona, PA, USA) under sterile conditions in all experimental groups. The samples were then immersed in BHI broth and incubated aerobically at 37°C for 4 weeks to allow mature biofilm formation.
Two samples were randomly selected from the groups and examined under a scanning electron microscope at ×1500 magnification to confirm the presence of E. faecalis biofilm within the root canal system [17] (Figure 1). The samples were then randomly assigned to six groups of one negative and one positive control, and four experimental groups according to the canal disinfection protocol: group 1: TAP (n=10), group 2: CH (n=10), group 3: TAP+LLLI (n=10), and group 4: CH+LLLI (n=10).
In the negative control group, the root canals were not contaminated, and the orifices were sealed with glass ionomer to prevent external microbial contamination during the study.
Background and Aim: This in vitro study assessed the impact of low-level laser irradiation (LLLI) on resistance of Enterococcus faecalis (E. faecalis) to calcium hydroxide (CH) and triple antibiotic paste (TAP) intracanal medicaments.
Materials and Methods: In this in vitro study, 44 extracted single-rooted human teeth were categorized into 6 groups of negative control (n=2), positive control (n=2), TAP (n=10), CH (n=10), TAP+LLLI (n=10), and CH+LLLI (n=10). Following preparation, the samples were transferred to brain heart infusion (BHI) broth and incubated at 37°C for 24 hours; 1 mL of E. faecalis (ATCC 29212) suspension was injected into the canals and incubated for 4 weeks for biofilm formation. CH and TAP were introduced into the canals, depending on group allocation of the teeth, and LLLI with performed for 15 seconds using 980 nm diode laser with an energy density of 6.89 J/cm², power-output of 0.5 W, and a tip diameter of 10 mm. After 2 weeks, canal debris was removed using #4 Gates-Glidden drills and incubated in BHI at 37°C for 8 hours. Then, 100 μL of the dilution was cultured to determine the number of colony-forming units (CFUs), indicating the effectiveness of disinfection, after 12 hours. Data were analyzed with one-way ANOVA (alpha=0.05).
Results: The four groups had no significant difference in colony count (P=0.483).
Conclusion: The results of this study indicated that LLLI in combination with CH or TAP did not lead to a significant reduction in colony count compared to the use of CH or TAP alone.
Keywords: Calcium Hydroxide; Drug Resistance, Microbial; Enterococcus faecalis; Low-Level Light Therapy
Introduction
Indiscriminate use of antibiotics is contributing to escalating drug resistance in bacteria, resulting in life-threatening diseases and a rising economic burden. The escalating threat of drug-resistant bacteria has generated an urgent need for novel antibacterial therapies and effective agents. In root canal therapy, physiological alterations induced by cells may contribute to microbial resistance to antiseptic drugs [1]. During root canal therapy, medicaments like triple antibiotic paste (TAP) or calcium hydroxide (CH) are often used to eradicate microorganisms from the root canal system. These medicaments remain in the root canal system for a duration ranging from 1 week to 1 month. During this time interval, they may induce antibiotic resistance [2].
Low-level laser irradiation (LLLI) was first used for treatment of severe enamel and dentin caries in 1960 [3]. Low-power or low-level lasers are defined as Class 3 lasers with an output power below 0.5 W. They are non-invasive and do not produce heat, noise, or vibrations during treatment [4]. Currently, LLLI is commonly performed for pain management following endodontic procedures. The mechanism of pain control by LLLI involves reduction of prostaglandin, interleukin-1 beta, and tumor necrosis factor-alpha production [5]. LLLI modulates fibroblast function at the tissue level, facilitating connective tissue repair and exerting anti-inflammatory effects [6,7]. Furthermore, it expedites angiogenesis while simultaneously enhancing cellular metabolism. While LLLI is effective in alleviating pain, it may potentially enhance bacterial resistance to antimicrobial drugs by inducing processes such as the filamentation phenotype [8]. Studies have shown that LLLI can induce resistance of bacterial strains such as Escherichia coli susceptible to H2O2, [9, 10].
Enterococcus faecalis (E. faecalis) is the main microorganism found in endodontically treated teeth with periradicular lesions. It is isolated from the root canals of 24% to 77% of patients with persistent endodontic infections [11]. E. faecalis is a common, potentially pathogenic strain with a confirmed resistance to different disinfectants and medicaments [12]. LLLI may upregulate anti-inflammatory phenomena in host cells and reduce post-treatment pain [5-7]. Thus, using LLLI to control pain after root canal treatment may make intracanal bacteria more resistant to antimicrobial agents through its photo-biomodulation effects on bacterial cells. Several studies have shown that various laser-based methods for root canal disinfection can effectively reduce the bacterial count within the canal [13,14]. No information exists regarding the combined effects of LLLI and intracanal medicament application on bacterial count in the canal. Thus, this study aimed to evaluate the impact of LLLI on the resistance of E. faecalis to CH and TAP intracanal medicaments in the root canal system. The null hypothesis tested was that LLLI would not increase the resistance of E. faecalis to CH and TAP intracanal medicaments.
Materials and Methods
This in vitro study received approval from the Research Ethics Committees of Islamic Azad University-Dental Branch, Tehran, under protocol number IR.IAU.DENTAL.REC.1401.006.
Single-rooted human teeth with straight canals that had been extracted as part of an orthodontic/periodontal treatment plan were selected for this study. Teeth with calcified canals, root caries, open apices, canal curvatures of more than 15 degrees according to the method described by Schneider [15], internal or external root resorption, and cracks were excluded through visual inspection and periapical radiography [16].
Sample size calculation:
Considering the power of β=0.2, α=0.05, a standard deviation of 1.2%, and an effect size of 0.28 obtained from a previous study [16], the sample size was calculated to be 10 in each group.
Tooth sample preparation:
This study involved 44 human single-rooted teeth extracted due to unfavorable periodontal prognosis or orthodontic treatment plan. The teeth were cleaned by removing calculus and soft tissue debris using a scaler, followed by immersion in 5.25% NaOCl (Golrang, Tehran, Iran) for 10 minutes [17]. The teeth were then rinsed with distilled water for 5 minutes. The crowns were cut just below the cementoenamel junction using a high-speed handpiece and a cylindrical diamond bur under water cooling. The apical foramina were sealed with light-cure glass ionomer cement (Fuji 2 LC; GC, Tokyo, Japan). The samples were then divided into six groups: one negative control group (n=2), one positive control group (n=2), and four experimental groups (n=10). All samples were placed in 1.5 mL Eppendorf tubes and sterilized with 40 kGy gamma radiation (GC-220 Gamacell, Nordion, Canada) [16].
In all groups, root canal patency was confirmed before instrumentation. A #15 K-file (Dentsply, Maillefer, Tulsa, OK, USA) was inserted into the canal until the tip was visible at the apex; then, the working length was set by withdrawing 0.5 mm. Root canal preparation was performed with the crown-down technique using the ProTaper rotary system (Dentsply Maillefer, Ballaigues, Switzerland) from S1 to F3, operating with a torque-limited electric motor (Endo IT motor; VDW, Munich, Germany) at 300 rpm and 3 N/cm torque. Irrigation was performed with 5.25% sodium hypochlorite (Golrang, Tehran, Iran), followed by 3 mL of 17% EDTA (Morva Bon, Tehran, Iran) to remove the smear layer. This was followed by a 5-minute rinse with an additional 3 mL of 5.25% sodium hypochlorite. To neutralize residual hypochlorite, the canals were irrigated with sodium thiosulfate (Sigma-Aldrich, St. Louis, MO, USA) and finally rinsed with 10 mL of sterile saline for 5 minutes [18,19]. The samples were then transferred to brain heart infusion (BHI) broth and incubated at 37°C for 24 hours. Absence of bacterial growth indicated effective sterilization.
E. faecalis (ATCC 29212; Pasteur Institute of Iran) was cultured in BHI broth for 8 hours, and a suspension with a concentration of 108 bacteria/mL was prepared spectrophotometrically at 600 nm. One milliliter of this suspension was injected into the sterile root canals using a 30-gauge irrigation needle (ProRinse; Dentsply Sirona, PA, USA) under sterile conditions in all experimental groups. The samples were then immersed in BHI broth and incubated aerobically at 37°C for 4 weeks to allow mature biofilm formation.
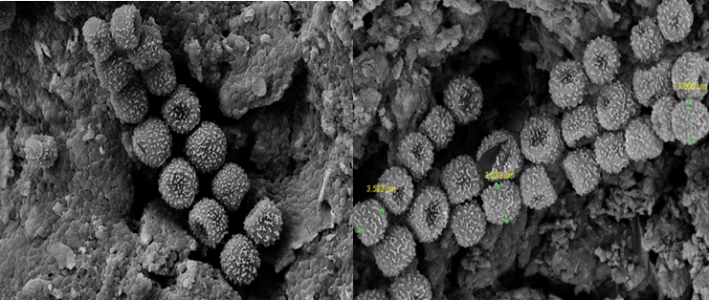
Two samples were randomly selected from the groups and examined under a scanning electron microscope at ×1500 magnification to confirm the presence of E. faecalis biofilm within the root canal system [17] (Figure 1). The samples were then randomly assigned to six groups of one negative and one positive control, and four experimental groups according to the canal disinfection protocol: group 1: TAP (n=10), group 2: CH (n=10), group 3: TAP+LLLI (n=10), and group 4: CH+LLLI (n=10).
In the negative control group, the root canals were not contaminated, and the orifices were sealed with glass ionomer to prevent external microbial contamination during the study.
Figure 1. Confirmation of bacterial biofilm formation under a scanning electron microscope at ×1500 magnification
Preparation of intracanal medicament:
After 4 weeks, groups 2 and 4 received CH, and groups 1 and 3 received TAP. For preparation of TAP, commercially available ciprofloxacin (250 mg; Ariadari.co, Tehran, Iran), metronidazole (250 mg; Parsdaru.co, Tehran, Iran), and minocycline (100 mg; Teopharma.co, Italy) were used. Their enteric coating was removed with a sterile sharp scalpel, and the tablets were subsequently ground into a fine powder using a sterile porcelain mortar and pestle. Prior to application, each powdered drug was measured in a ratio of 1:1:1 (one part ciprofloxacin, one part metronidazole, and one part minocycline) utilizing an electronic balance, and subsequently combined with propylene glycol and polyethylene glycol to create an ointment.
To prepare CH paste, a typical scoop of CH powder (Golchadent, Tehran, Iran) was combined with three drops of saline to obtain a creamy consistency, which was subsequently introduced into the canal using a lentulo spiral. In all groups, the medicament combination was introduced into the canal using a lentulo spiral (Mani, Tochigi, Japan) [20,21].
LLLI:
In groups 3 and 4, the root canals were irradiated with 980 nm diode laser (Doctor Smile; Wiser, Lambda, Italy) for 10 seconds with an energy density of 6.89 J/cm², a power output of 0.5 W, and a tip diameter of 10 mm. The laser was directed from the buccal side, with the handpiece tip positioned approximately 10 mm away from the apices [5].
Following 2 weeks, the antibacterial medicament within the canal was rinsed with 10 mL of sterile distilled water. Subsequently, the canals were dried with sterile paper points, and a Gates Glidden drill size 4 (Mani, Tochigi, Japan) was employed to collect dentinal chips from the entire root canal system. To enhance bacterial survival, dentinal chips were added to BHI broth, which was subsequently incubated at 37°C for 8 hours. The suspension was serially diluted in tenfold increments, and 100 μL of each dilution was cultured on BHI broth agar plates to determine the colony count in colony-forming units (CFUs) after 12 hours of incubation at 37°C. The colony count reflected the efficacy of the disinfection method in removing mature biofilms [13].
Statistical analysis:
The Shapiro-Wilk test was used to assess the normality of data distribution in the study groups. Considering the normality of data distribution and homogeneity of variances, one-way ANOVA was used for data analysis at 0.05 level of significance.
Results
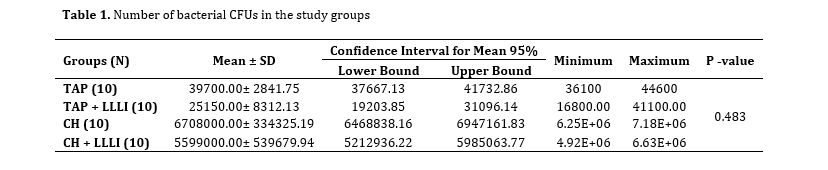
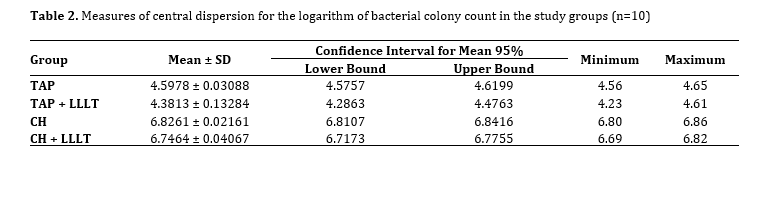
The four experimental groups had no significant difference in colony count (P=0.483, Table 1). Table 2 shows the measures of central dispersion for the logarithm of colony count in the study groups.
{kind=link}
Preparation of intracanal medicament:
After 4 weeks, groups 2 and 4 received CH, and groups 1 and 3 received TAP. For preparation of TAP, commercially available ciprofloxacin (250 mg; Ariadari.co, Tehran, Iran), metronidazole (250 mg; Parsdaru.co, Tehran, Iran), and minocycline (100 mg; Teopharma.co, Italy) were used. Their enteric coating was removed with a sterile sharp scalpel, and the tablets were subsequently ground into a fine powder using a sterile porcelain mortar and pestle. Prior to application, each powdered drug was measured in a ratio of 1:1:1 (one part ciprofloxacin, one part metronidazole, and one part minocycline) utilizing an electronic balance, and subsequently combined with propylene glycol and polyethylene glycol to create an ointment.
To prepare CH paste, a typical scoop of CH powder (Golchadent, Tehran, Iran) was combined with three drops of saline to obtain a creamy consistency, which was subsequently introduced into the canal using a lentulo spiral. In all groups, the medicament combination was introduced into the canal using a lentulo spiral (Mani, Tochigi, Japan) [20,21].
LLLI:
In groups 3 and 4, the root canals were irradiated with 980 nm diode laser (Doctor Smile; Wiser, Lambda, Italy) for 10 seconds with an energy density of 6.89 J/cm², a power output of 0.5 W, and a tip diameter of 10 mm. The laser was directed from the buccal side, with the handpiece tip positioned approximately 10 mm away from the apices [5].
Following 2 weeks, the antibacterial medicament within the canal was rinsed with 10 mL of sterile distilled water. Subsequently, the canals were dried with sterile paper points, and a Gates Glidden drill size 4 (Mani, Tochigi, Japan) was employed to collect dentinal chips from the entire root canal system. To enhance bacterial survival, dentinal chips were added to BHI broth, which was subsequently incubated at 37°C for 8 hours. The suspension was serially diluted in tenfold increments, and 100 μL of each dilution was cultured on BHI broth agar plates to determine the colony count in colony-forming units (CFUs) after 12 hours of incubation at 37°C. The colony count reflected the efficacy of the disinfection method in removing mature biofilms [13].
Statistical analysis:
The Shapiro-Wilk test was used to assess the normality of data distribution in the study groups. Considering the normality of data distribution and homogeneity of variances, one-way ANOVA was used for data analysis at 0.05 level of significance.
Results
The four experimental groups had no significant difference in colony count (P=0.483, Table 1). Table 2 shows the measures of central dispersion for the logarithm of colony count in the study groups.
Table 1. Number of bacterial CFUs in the study groups
Table 2. Measures of central dispersion for the logarithm of bacterial colony count in the study groups (n=10)
Discussion
The goal of this study was to find out how LLLI may affect antimicrobial resistance of E. faecalis in the canal. It was found that using a low-power laser along with CH and TAP reduced the number of E. faecalis colonies, but the difference in colony count among the groups was not statistically significant. Thus, the null hypothesis of the study was accepted.
Research indicates that E. faecalis is more frequently associated with root canal treatment failures than with primary root canal infections [11]. E. faecalis is a resilient microorganism that, despite being a minor component of the bacterial flora in untreated canals, significantly contributes to the etiology of recurrent apical lesions following root canal therapy, and is present in a substantial proportion of root canal treatment failures [22].
CH is well-known for its antimicrobial properties, primarily due to its high pH, which disrupts bacterial cell membrane and denatures proteins [23]. However, its effectiveness can be limited against certain resistant bacteria, such as E. faecalis, particularly in biofilm contexts [24]. LLLI, on the other hand, has been shown to enhance cellular functions and promote healing through photobiomodulation, which can also lead to increased ATP production and modulation of inflammation [25]. In a case study, Yadav et al. [26] demonstrated that the sequential use of CH and LLLI can significantly enhance the healing of periapical lesions due to promoting cellular proliferation and reducing inflammation. Similarly, the present study showed that combination of LLLI and intracanal medicaments, i.e., TAP and CH, provided a synergistic effect, improving antimicrobial action, although the difference did not reach statistical significance. Furthermore, LLLI has been shown to increase the release of growth factors such as transforming growth factor-β from dentin, which is crucial for tissue regeneration [27].
{kind=link}
Table 2. Measures of central dispersion for the logarithm of bacterial colony count in the study groups (n=10)
{kind=link}
Discussion
The goal of this study was to find out how LLLI may affect antimicrobial resistance of E. faecalis in the canal. It was found that using a low-power laser along with CH and TAP reduced the number of E. faecalis colonies, but the difference in colony count among the groups was not statistically significant. Thus, the null hypothesis of the study was accepted.
Research indicates that E. faecalis is more frequently associated with root canal treatment failures than with primary root canal infections [11]. E. faecalis is a resilient microorganism that, despite being a minor component of the bacterial flora in untreated canals, significantly contributes to the etiology of recurrent apical lesions following root canal therapy, and is present in a substantial proportion of root canal treatment failures [22].
CH is well-known for its antimicrobial properties, primarily due to its high pH, which disrupts bacterial cell membrane and denatures proteins [23]. However, its effectiveness can be limited against certain resistant bacteria, such as E. faecalis, particularly in biofilm contexts [24]. LLLI, on the other hand, has been shown to enhance cellular functions and promote healing through photobiomodulation, which can also lead to increased ATP production and modulation of inflammation [25]. In a case study, Yadav et al. [26] demonstrated that the sequential use of CH and LLLI can significantly enhance the healing of periapical lesions due to promoting cellular proliferation and reducing inflammation. Similarly, the present study showed that combination of LLLI and intracanal medicaments, i.e., TAP and CH, provided a synergistic effect, improving antimicrobial action, although the difference did not reach statistical significance. Furthermore, LLLI has been shown to increase the release of growth factors such as transforming growth factor-β from dentin, which is crucial for tissue regeneration [27].
Moradi Eslami et al. [28] evaluated the efficacy of intracanal medicaments, diode laser, and photodynamic therapy for removing E. faecalis and Candida albicans biofilms from the root canal system. The results showed that all three groups experienced a significant decrease in bacterial colonies. The TAP group showed the most significant reduction, with no statistically significant difference among the study groups. Their findings are consistent with the current results.
The dentinal tubules' small diameter and the elevated surface tension of the disinfectant solutions within the canal allow penetration into the tubules to a depth of approximately 100 µm [29]; while, bacteria can infiltrate up to 1000 µm within the tubules [30]. Given that evidence indicates that the walls of the root canal remain intact post-preparation by manual or rotary instruments in approximately 35%–45% of the cases, and that irrigating solutions may fail to contact all canal walls because of the anatomical complexities, bacterial resistance becomes a common challenge that negatively impacts the effectiveness of the disinfection techniques employed. Consequently, it is necessary to employ supplementary methods [16]. One of the reasons for the greater effectiveness of LLLI in reducing intracanal bacteria is its ability to enhance the penetration of intracanal medicaments into the dentinal tubules, thereby increasing their efficacy against biofilms [31]. Laser use represents a novel antibacterial intervention. Evidence indicates that employing a laser in conjunction with a non-toxic photosensitizer can yield enhanced antibacterial effects [32]. The laser settings, factors such as limited oxygen levels inside the canal, type and concentration of photosensitizer, its ability to diffuse within the dentin tubules, and the structural differences of the root canal system all affect this effectiveness [33].
The dentinal tubules' small diameter and the elevated surface tension of the disinfectant solutions within the canal allow penetration into the tubules to a depth of approximately 100 µm [29]; while, bacteria can infiltrate up to 1000 µm within the tubules [30]. Given that evidence indicates that the walls of the root canal remain intact post-preparation by manual or rotary instruments in approximately 35%–45% of the cases, and that irrigating solutions may fail to contact all canal walls because of the anatomical complexities, bacterial resistance becomes a common challenge that negatively impacts the effectiveness of the disinfection techniques employed. Consequently, it is necessary to employ supplementary methods [16]. One of the reasons for the greater effectiveness of LLLI in reducing intracanal bacteria is its ability to enhance the penetration of intracanal medicaments into the dentinal tubules, thereby increasing their efficacy against biofilms [31]. Laser use represents a novel antibacterial intervention. Evidence indicates that employing a laser in conjunction with a non-toxic photosensitizer can yield enhanced antibacterial effects [32]. The laser settings, factors such as limited oxygen levels inside the canal, type and concentration of photosensitizer, its ability to diffuse within the dentin tubules, and the structural differences of the root canal system all affect this effectiveness [33].
One limitation of this study was its in vitro design. Lack of complete simulation of the clinical setting may limit the generalization of the results to clinical scenarios. Also, in an in vitro setup, finding samples with standard similarity in terms of curvature, apical size, etc., is another limitation for standardizing the variables. Future studies should incorporate other types of low-power lasers to obtain more comprehensive results, in addition to using low-power lasers as a standalone intervention group.
Conclusion
Conclusion
The research results showed that LLLI not only did not cause the emergence or increase of antibacterial resistance but, when combined with TAP or CH medicaments, reduced the microbial load in the root canal system; however, this observed reduction was not statistically significant.
Type of Study: Original article |
Subject:
Endodontics
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |