Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 1 (3-2026)
J Res Dent Maxillofac Sci 2026, 11(1): 75-83 |
Back to browse issues page
Ethics code: IR.SSU.DENTISTRY.REC.1400.007
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soltanianzadeh M, Qorbani F, kazemipoor M. Impact of Contact Time on Push-out Bond Strength of Intra-orifice Barrier Materials in Temporary Restorations. J Res Dent Maxillofac Sci 2026; 11 (1) :75-83
URL: http://jrdms.dentaliau.ac.ir/article-1-955-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-955-en.html


1- Assistant Professor, Department of Restorative Dentistry, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2- Department of Restorative Dentistry, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3- Department of Endodontic, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,dr.kazemipoor@gmail.com
2- Department of Restorative Dentistry, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3- Department of Endodontic, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,
Keywords: Bond Strength, Dental Bonding, Dental Restoration, Endodontics, Temporary Dental Restoration, Root Canal Filling Materials
Full-Text [PDF 436 kb]
(28 Downloads)
| Abstract (HTML) (40 Views)
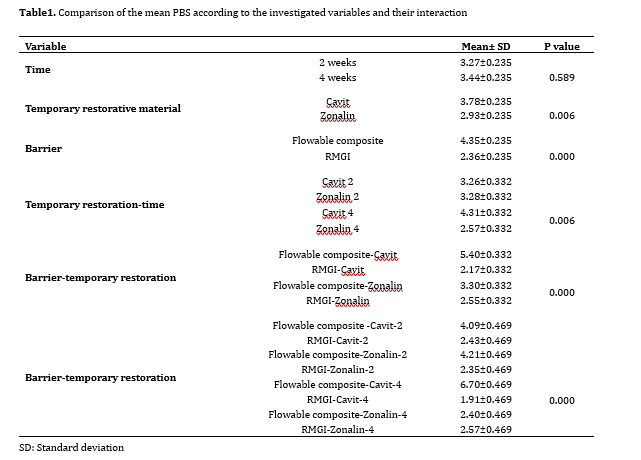
Table1. Comparison of the mean PBS according to the investigated variables and their interaction
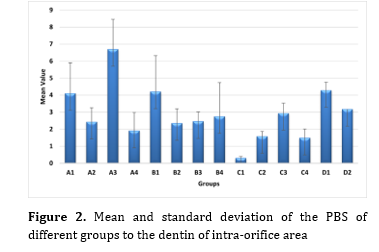
Figure 2. Mean and standard deviation of the PBS of different groups to the dentin of intra-orifice area
Effect of time and temporary restorative material:
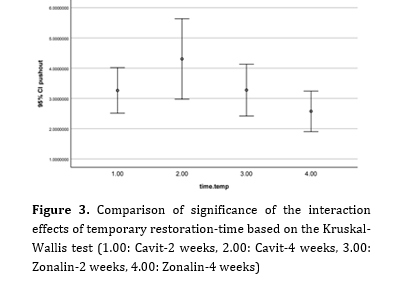
The interaction between time and temporary restorative material was significant (P=0.006). Cavit applied for 4 weeks resulted in the highest PBS (4.31±0.332 MPa), significantly greater than Zonalin at 4 weeks (2.57±0.332 MPa; P=0.002). No significant difference was observed between Cavit and Zonalin at 2 weeks (3.26±0.332 MPa vs. 3.28±0.332 MPa; P=0.912), nor between Zonalin at 2 and 4 weeks (P=0.083) (Figure 3).
Figure 3. Comparison of significance of the interaction effects of temporary restoration-time based on the Kruskal-Wallis test (1.00: Cavit-2 weeks, 2.00: Cavit-4 weeks, 3.00: Zonalin-2 weeks, 4.00: Zonalin-4 weeks)
Effect of temporary restorative material and barrier material:
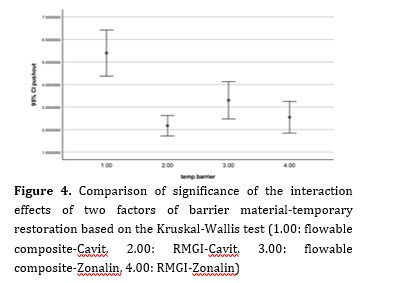
The interaction between temporary restorative material and barrier material was significant (P=0.000). Cavit combined with flowable composite showed the highest PBS (5.40±0.332 MPa), significantly greater than Cavit-RMGI (2.17±0.332 MPa; P=0.000), Zonalin-flowable composite (3.30±0.332 MPa; P=0.001), and Zonalin-RMGI (2.55±0.332 MPa; P=0.001) (Figure 4).
Figure 4. Comparison of significance of the interaction effects of two factors of barrier material-temporary restoration based on the Kruskal-Wallis test (1.00: flowable composite-Cavit, 2.00: RMGI-Cavit, 3.00: flowable composite-Zonalin, 4.00: RMGI-Zonalin)
Effect of time, temporary restorative material, and barrier material:
The three-way interaction was significant (P=0.000). The Cavit-4 weeks-flowable composite subgroup exhibited the highest PBS (6.70±0.469 MPa), significantly greater than all other combinations (P=0.000). The lowest value was observed in the positive control group (cotton with eugenol-2 weeks-flowable composite: 0.302±0.101 MPa) (Figure 5). Other notable comparisons included:
Full-Text: (35 Views)
Abstract
Background and Aim: The use of intra-orifice barriers helps reduce coronal leakage, enhances sealing of the intra-orifice area, and improves the success rate of root canal therapy. This study aimed to investigate the effect of contact time on pushout bond strength (PBS) of intra-orifice barrier materials in temporary restorations.
Materials and Methods: This in vitro study used 110 single-rooted teeth decoronated at 2 mm below their cementoenamel junction. After access cavity preparation, the samples were divided into two experimental groups of Cavit and Zonalin and two control groups of positive control and negative control. The Cavit and Zonalin groups were further divided into subgroups based on the duration of temporary restoration application (2 weeks and 4 weeks) and type of barrier material [flowable composite and resin-modified glass ionomer (RMGI)]. Dentinal blocks were prepared, and samples were subjected to a PBS test. Data were analyzed using a generalized linear model and the Kruskal-Wallis test (alpha=0.05).
Results: General comparison revealed a statistically significant difference among the experimental groups in PBS (P=0.000). Pairwise comparisons showed that the Cavit-4 weeks-flowable composite subgroup exhibited the highest PBS (6.70 ± 1.76 MPa), which was significantly greater than the PBS of all other combinations (P=0.000). The positive control group (cotton pellet dipped in eugenol-2 weeks-flowable composite) showed the lowest PBS (0.302 ± 0.101 MPa).
Conclusion: Cavit temporary restorative material significantly enhanced the PBS of flowable composite barrier after 4 weeks, outperforming other materials and time combinations.
Keywords: Dental Bonding; Dental Restoration, Temporary; Endodontics; Root Canal Filling Materials
Introduction
Endodontic pain is a prevalent cause of orofacial discomfort. The advent of root canal therapy has revolutionized dental care, allowing dental clinicians to preserve teeth that would have been extracted in the past. However, due to the increased susceptibility of endodontically treated teeth to fracture compared to vital teeth, it is crucial to restore and protect the remaining tooth structure following completion of root canal therapy [1]. Evidence shows that secondary microleakage caused by inadequate coronal sealing is one of the most important factors that causes root canal treatment failure [2-4]. Thus, there is a need for different materials and techniques known as intra-orifice barriers to promote sealing of the coronal area. Application of intra-orifice barriers has become an efficient alternative to reduce coronal leakage in endodontically treated teeth. This method includes placing additional materials in the canal opening immediately after removing the coronal part of gutta-percha and sealer [1,2].
Various restorative materials have been employed to seal the intra-orifice area and prevent microleakage, including Cavit, amalgam, Interim Restorative Material, Super-EBA, composite resins, glass ionomer cement, and mineral trioxide aggregate [2,4]. In many cases, after a root canal is obturated, the tooth is not permanently restored in the same session; thus, the recently obturated root canal becomes infected following exposure to the oral environment. As a result, it is necessary to apply a temporary restorative material with optimal properties to prevent marginal microleakage [5].
Temporary restorative materials are divided into two general types of eugenol-based [zinc oxide eugenol (ZOE)] and non-eugenol based (Cavit) materials. Eugenol reacts with free radicals and thus inhibits the polymerization of methacrylate monomers. Despite numerous studies on the inhibitory effects of eugenol, the dynamics and inhibition mechanism of eugenol are not well known [5-7]. Nevertheless, there are conflicting findings on whether the previous use of eugenol-containing temporary restorative materials would affect the bond strength of composite resin to dentin or not. Several studies have shown that eugenol-containing temporary cements do not reduce the bond strength to dentin [5,8]. However, other studies have reported conflicting results [6,7,9]. This difference in the results can be justified by the difference in adhesive systems and methods used and the duration of exposure of dentin to eugenol [6]. A previous study showed that none of the tested temporary restorative materials (Cavit, Interim Restorative Material, Temp Bond) could prevent bacterial leakage into the canal for a long time (30 days). For this reason, the maximum period of using a temporary restoration before final restoration of tooth should not exceed 30 days [10]. Microtensile test, pushout test, and shear test are all used to measure the bond strength. The pushout bond strength (PBS) test yields more reliable results since it is closer to clinical conditions [11].
The adhesive bond to dentin in the orifice area plays a crucial role in preventing bacterial leakage into the root canal and ensuring the success of root canal therapy [12-14]. Thus, factors that interfere with this bonding process are of utmost clinical importance. The aim of this study was to evaluate the impact of the type and contact time of temporary restorative materials on the PBS of intra-orifice barrier materials. The null hypothesis was that neither the type of temporary restorative material nor the duration of its placement would significantly affect the PBS of intra-orifice barrier materials.
Materials and Methods
This study was approved by the Research Ethic Committee of Shahid Sadoughi University of Medical Sciences, Yazd, Iran:
(IR.SSU.DENTISTRY.REC.1400.007).
This in vitro experimental study evaluated 110 single-rooted teeth without cracks, fractures, severe crown or root caries, extensive crown restoration, or previous root canal treatment that had been extracted for purposes not related to this study. The sample size was calculated using PASS-15 based on data from previous studies [3,13] evaluating the PBS of intra-orifice barrier materials. Assuming a two-sided test with a significance level (α) of 0.05, statistical power (1–β) of 80%, and an estimated effect size of 1.2 derived from prior literature [3,13], the minimum required sample size was determined to be 10 specimens per each experimental subgroup and 5 specimens per each control group. This calculation accounted for variability in dentin morphology and experimental conditions. A total of 110 teeth were selected by convenience sampling from available teeth to ensure adequate power for detecting clinically meaningful differences.
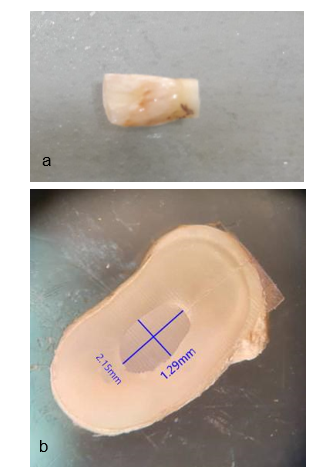
To control cross-infection and eliminate the remaining periodontal tissues, the teeth were immersed in a 5.25% sodium hypochlorite solution (Fa Company, Iran) for 6 hours, after which the residual tissues were removed from the tooth surface. The teeth were then stored in a 0.5% chloramine solution (Iran Discus, Iran). The teeth were transferred to a saline solution one week before the experiment. For sample preparation, the teeth were decoronated at 2 mm below the cementoenamel junction using a cutting disc (Microdont, Brazil) under water cooling (Figure 1a) [3,6].
Access cavity preparation:
A standard access cavity was prepared using fissure and round diamond burs (IQ Dent, Poland) with a high-speed handpiece and ample water cooling. After cleaning and rinsing with 0.9% saline solution (Shahid Ghazi, Iran), the samples were dried with sterile cotton pellets (Figure 1a).
Sample preparation:
After preparing the access cavities, the teeth were randomly divided into two study groups:
Group A: temporary restoration with Cavit (Golchai Chemical Industry Co., Tehran, Iran)
Group B: temporary restoration with Zonalin (Golchai Chemical Industry Co., Tehran, Iran)
Positive and negative control groups were also considered. Each of the two study groups was further divided into four subgroups (n=10) based on the duration of temporary restoration placement and type of barrier material used:
Background and Aim: The use of intra-orifice barriers helps reduce coronal leakage, enhances sealing of the intra-orifice area, and improves the success rate of root canal therapy. This study aimed to investigate the effect of contact time on pushout bond strength (PBS) of intra-orifice barrier materials in temporary restorations.
Materials and Methods: This in vitro study used 110 single-rooted teeth decoronated at 2 mm below their cementoenamel junction. After access cavity preparation, the samples were divided into two experimental groups of Cavit and Zonalin and two control groups of positive control and negative control. The Cavit and Zonalin groups were further divided into subgroups based on the duration of temporary restoration application (2 weeks and 4 weeks) and type of barrier material [flowable composite and resin-modified glass ionomer (RMGI)]. Dentinal blocks were prepared, and samples were subjected to a PBS test. Data were analyzed using a generalized linear model and the Kruskal-Wallis test (alpha=0.05).
Results: General comparison revealed a statistically significant difference among the experimental groups in PBS (P=0.000). Pairwise comparisons showed that the Cavit-4 weeks-flowable composite subgroup exhibited the highest PBS (6.70 ± 1.76 MPa), which was significantly greater than the PBS of all other combinations (P=0.000). The positive control group (cotton pellet dipped in eugenol-2 weeks-flowable composite) showed the lowest PBS (0.302 ± 0.101 MPa).
Conclusion: Cavit temporary restorative material significantly enhanced the PBS of flowable composite barrier after 4 weeks, outperforming other materials and time combinations.
Keywords: Dental Bonding; Dental Restoration, Temporary; Endodontics; Root Canal Filling Materials
Introduction
Endodontic pain is a prevalent cause of orofacial discomfort. The advent of root canal therapy has revolutionized dental care, allowing dental clinicians to preserve teeth that would have been extracted in the past. However, due to the increased susceptibility of endodontically treated teeth to fracture compared to vital teeth, it is crucial to restore and protect the remaining tooth structure following completion of root canal therapy [1]. Evidence shows that secondary microleakage caused by inadequate coronal sealing is one of the most important factors that causes root canal treatment failure [2-4]. Thus, there is a need for different materials and techniques known as intra-orifice barriers to promote sealing of the coronal area. Application of intra-orifice barriers has become an efficient alternative to reduce coronal leakage in endodontically treated teeth. This method includes placing additional materials in the canal opening immediately after removing the coronal part of gutta-percha and sealer [1,2].
Various restorative materials have been employed to seal the intra-orifice area and prevent microleakage, including Cavit, amalgam, Interim Restorative Material, Super-EBA, composite resins, glass ionomer cement, and mineral trioxide aggregate [2,4]. In many cases, after a root canal is obturated, the tooth is not permanently restored in the same session; thus, the recently obturated root canal becomes infected following exposure to the oral environment. As a result, it is necessary to apply a temporary restorative material with optimal properties to prevent marginal microleakage [5].
Temporary restorative materials are divided into two general types of eugenol-based [zinc oxide eugenol (ZOE)] and non-eugenol based (Cavit) materials. Eugenol reacts with free radicals and thus inhibits the polymerization of methacrylate monomers. Despite numerous studies on the inhibitory effects of eugenol, the dynamics and inhibition mechanism of eugenol are not well known [5-7]. Nevertheless, there are conflicting findings on whether the previous use of eugenol-containing temporary restorative materials would affect the bond strength of composite resin to dentin or not. Several studies have shown that eugenol-containing temporary cements do not reduce the bond strength to dentin [5,8]. However, other studies have reported conflicting results [6,7,9]. This difference in the results can be justified by the difference in adhesive systems and methods used and the duration of exposure of dentin to eugenol [6]. A previous study showed that none of the tested temporary restorative materials (Cavit, Interim Restorative Material, Temp Bond) could prevent bacterial leakage into the canal for a long time (30 days). For this reason, the maximum period of using a temporary restoration before final restoration of tooth should not exceed 30 days [10]. Microtensile test, pushout test, and shear test are all used to measure the bond strength. The pushout bond strength (PBS) test yields more reliable results since it is closer to clinical conditions [11].
The adhesive bond to dentin in the orifice area plays a crucial role in preventing bacterial leakage into the root canal and ensuring the success of root canal therapy [12-14]. Thus, factors that interfere with this bonding process are of utmost clinical importance. The aim of this study was to evaluate the impact of the type and contact time of temporary restorative materials on the PBS of intra-orifice barrier materials. The null hypothesis was that neither the type of temporary restorative material nor the duration of its placement would significantly affect the PBS of intra-orifice barrier materials.
Materials and Methods
This study was approved by the Research Ethic Committee of Shahid Sadoughi University of Medical Sciences, Yazd, Iran:
(IR.SSU.DENTISTRY.REC.1400.007).
This in vitro experimental study evaluated 110 single-rooted teeth without cracks, fractures, severe crown or root caries, extensive crown restoration, or previous root canal treatment that had been extracted for purposes not related to this study. The sample size was calculated using PASS-15 based on data from previous studies [3,13] evaluating the PBS of intra-orifice barrier materials. Assuming a two-sided test with a significance level (α) of 0.05, statistical power (1–β) of 80%, and an estimated effect size of 1.2 derived from prior literature [3,13], the minimum required sample size was determined to be 10 specimens per each experimental subgroup and 5 specimens per each control group. This calculation accounted for variability in dentin morphology and experimental conditions. A total of 110 teeth were selected by convenience sampling from available teeth to ensure adequate power for detecting clinically meaningful differences.
To control cross-infection and eliminate the remaining periodontal tissues, the teeth were immersed in a 5.25% sodium hypochlorite solution (Fa Company, Iran) for 6 hours, after which the residual tissues were removed from the tooth surface. The teeth were then stored in a 0.5% chloramine solution (Iran Discus, Iran). The teeth were transferred to a saline solution one week before the experiment. For sample preparation, the teeth were decoronated at 2 mm below the cementoenamel junction using a cutting disc (Microdont, Brazil) under water cooling (Figure 1a) [3,6].
Access cavity preparation:
A standard access cavity was prepared using fissure and round diamond burs (IQ Dent, Poland) with a high-speed handpiece and ample water cooling. After cleaning and rinsing with 0.9% saline solution (Shahid Ghazi, Iran), the samples were dried with sterile cotton pellets (Figure 1a).
Sample preparation:
After preparing the access cavities, the teeth were randomly divided into two study groups:
Group A: temporary restoration with Cavit (Golchai Chemical Industry Co., Tehran, Iran)
Group B: temporary restoration with Zonalin (Golchai Chemical Industry Co., Tehran, Iran)
Positive and negative control groups were also considered. Each of the two study groups was further divided into four subgroups (n=10) based on the duration of temporary restoration placement and type of barrier material used:
- Group A1: Cavit, 2 weeks, flowable composite (Kulzer, Germany)
- Group A2: Cavit, 2 weeks, resin-modified glass ionomer (RMGI; Fuji II LC GC, Japan)
- Group A3: Cavit, 4 weeks, flowable composite
- Group A4: Cavit, 4 weeks, RMGI
- Group B1: Zonalin, 2 weeks, flowable composite
- Group B2: Zonalin, 2 weeks, RMGI
- Group B3: Zonalin, 4 weeks, flowable composite
- Group B4: Zonalin, 4 weeks, RMGI
The positive control group included:
- Group C1: Cotton pellet dipped in eugenol, 2 weeks, flowable composite
- Group C2: Cotton pellet dipped in eugenol, 2 weeks, RMGI
- Group C3: Cotton pellet dipped in eugenol, 4 weeks, flowable composite
- Group C4: Cotton pellet dipped in eugenol, 4 weeks, RMGI
The negative control group included:
- Group D1: Flowable composite
- Group D2: RMGI
Temporary restorative materials were applied into the access cavities according to the manufacturers’ instructions. The samples were then kept in an incubator at 37˚C for 2 or 4 weeks, depending on the subgroup. After the specified duration, the temporary restorative material was removed, and the desired barrier material (RMGI or flowable composite) was placed in the orifice area (Figure 1b) [3,9].
To prepare RMGI, the powder and liquid were mixed per the manufacturer's instructions and placed into the intra-orifice area with a plugger. Excess material was removed, and the barrier material was cured for 20 seconds using a curing light (Coltolux, USA) with a light intensity of 800 mW/cm². For the flowable composite, the dentinal surface of the intra-orifice area was conditioned with 37% phosphoric acid (Ultradent, USA) for 15 seconds, then washed and dried for 10 seconds. A fifth-generation bonding agent (Kulzer, Germany) was applied for 15 seconds with a microbrush, followed by gentle air spray for 5 seconds. A second layer of bonding agent was applied, air-thinned, and cured for 20 seconds. Flowable composite (Kulzer, Germany) was placed in the barrier area and cured for 20 seconds [3].
In the positive control group (20 samples), a cotton pellet dipped in eugenol was placed inside the access cavity for 2 or 4 weeks before applying the RMGI or flowable composite barrier. In the negative control group (10 samples), no material was placed in the access cavity, and the samples were immediately restored with flowable composite or RMGI barrier material. The teeth were stored at 37ºC and approximately 100% humidity for 24 hours to ensure complete setting of the intra-orifice material.
Figure 1. Representative images of sample preparation and intra-orifice barrier placement. (a) A 2-mm-thick root slice sectioned 2 mm below the cementoenamel junction, used for PBS testing. (b) Stereomicroscopic view (×32 magnification) of the same sample showing the intra-orifice barrier material placed inside the canal orifice
PBS testing:
The coronal portion of the samples was sectioned at the cementoenamel junction using a diamond disc, leaving a 2 mm segment of the tooth root for the PBS test. The samples were securely mounted in an acrylic cylinder aligned parallel to the longitudinal axis of the tooth (in the apico-coronal direction). A transverse section, 1 mm thick, was cut 2 mm below the cementoenamel junction using an automatic CNC cutting machine. The PBS test was conducted on this section in a universal testing machine (Zwick Reall ZO50, Germany). The samples were subjected to force application in the apico-coronal direction, centered on the barrier, at a speed of 0.5 mm per minute until fracture occurred. The maximum force for each sample was recorded in Newtons (N) [3]. The following formula was used to calculate the force required to break the samples:
PBS (MPa) = lateral surface area (mm2)/force (N).
To calculate the cross-sectional area of the samples, all the samples were photographed under a stereomicroscope (Nikon, Japan) before the PBS measurement process, and then using the mean of the large and small diameters, the lateral surface area was calculated according to the following formula:
Lateral surface area = height x 13.4 [2/(large diameter + small diameter)]
The mode of failure of the samples was also determined under a stereomicroscope (Nikon, Japan) at x32 magnification and categorized as adhesive, cohesive or mixed (Figure 1b).
Statistical analysis:
Statistical analyses were conducted using SPSS version 26. The Kruskal-Wallis test, a non-parametric test, was applied to compare the overall difference in PBS among multiple independent groups, since the data did not meet the assumptions of normality. When significant differences were detected, pairwise comparisons were performed using the Dunn’s post-hoc test with Bonferroni correction to identify specific group differences. Additionally, a generalized linear model was employed to assess the interaction effects between variables such as temporary restorative material, barrier material, and contact time, allowing for adjustment of potential confounders and evaluation of main and interaction effects. The significance level was set at P<0.05.
Results
In the positive control group (20 samples), a cotton pellet dipped in eugenol was placed inside the access cavity for 2 or 4 weeks before applying the RMGI or flowable composite barrier. In the negative control group (10 samples), no material was placed in the access cavity, and the samples were immediately restored with flowable composite or RMGI barrier material. The teeth were stored at 37ºC and approximately 100% humidity for 24 hours to ensure complete setting of the intra-orifice material.
Figure 1. Representative images of sample preparation and intra-orifice barrier placement. (a) A 2-mm-thick root slice sectioned 2 mm below the cementoenamel junction, used for PBS testing. (b) Stereomicroscopic view (×32 magnification) of the same sample showing the intra-orifice barrier material placed inside the canal orifice
{kind=link}
PBS testing:
The coronal portion of the samples was sectioned at the cementoenamel junction using a diamond disc, leaving a 2 mm segment of the tooth root for the PBS test. The samples were securely mounted in an acrylic cylinder aligned parallel to the longitudinal axis of the tooth (in the apico-coronal direction). A transverse section, 1 mm thick, was cut 2 mm below the cementoenamel junction using an automatic CNC cutting machine. The PBS test was conducted on this section in a universal testing machine (Zwick Reall ZO50, Germany). The samples were subjected to force application in the apico-coronal direction, centered on the barrier, at a speed of 0.5 mm per minute until fracture occurred. The maximum force for each sample was recorded in Newtons (N) [3]. The following formula was used to calculate the force required to break the samples:
PBS (MPa) = lateral surface area (mm2)/force (N).
To calculate the cross-sectional area of the samples, all the samples were photographed under a stereomicroscope (Nikon, Japan) before the PBS measurement process, and then using the mean of the large and small diameters, the lateral surface area was calculated according to the following formula:
Lateral surface area = height x 13.4 [2/(large diameter + small diameter)]
The mode of failure of the samples was also determined under a stereomicroscope (Nikon, Japan) at x32 magnification and categorized as adhesive, cohesive or mixed (Figure 1b).
Statistical analysis:
Statistical analyses were conducted using SPSS version 26. The Kruskal-Wallis test, a non-parametric test, was applied to compare the overall difference in PBS among multiple independent groups, since the data did not meet the assumptions of normality. When significant differences were detected, pairwise comparisons were performed using the Dunn’s post-hoc test with Bonferroni correction to identify specific group differences. Additionally, a generalized linear model was employed to assess the interaction effects between variables such as temporary restorative material, barrier material, and contact time, allowing for adjustment of potential confounders and evaluation of main and interaction effects. The significance level was set at P<0.05.
Results
Statistical analysis revealed significant differences in PBS among the experimental groups (P=0.000). All interaction effects including temporary restoration material, barrier type, duration, and their combinations were statistically significant and were interpreted through subgroup analysis (Table 1, Figure 2).
Table1. Comparison of the mean PBS according to the investigated variables and their interaction
{kind=link}
Figure 2. Mean and standard deviation of the PBS of different groups to the dentin of intra-orifice area
{kind=link}
Effect of time and temporary restorative material:
The interaction between time and temporary restorative material was significant (P=0.006). Cavit applied for 4 weeks resulted in the highest PBS (4.31±0.332 MPa), significantly greater than Zonalin at 4 weeks (2.57±0.332 MPa; P=0.002). No significant difference was observed between Cavit and Zonalin at 2 weeks (3.26±0.332 MPa vs. 3.28±0.332 MPa; P=0.912), nor between Zonalin at 2 and 4 weeks (P=0.083) (Figure 3).
Figure 3. Comparison of significance of the interaction effects of temporary restoration-time based on the Kruskal-Wallis test (1.00: Cavit-2 weeks, 2.00: Cavit-4 weeks, 3.00: Zonalin-2 weeks, 4.00: Zonalin-4 weeks)
{kind=link}
Effect of temporary restorative material and barrier material:
The interaction between temporary restorative material and barrier material was significant (P=0.000). Cavit combined with flowable composite showed the highest PBS (5.40±0.332 MPa), significantly greater than Cavit-RMGI (2.17±0.332 MPa; P=0.000), Zonalin-flowable composite (3.30±0.332 MPa; P=0.001), and Zonalin-RMGI (2.55±0.332 MPa; P=0.001) (Figure 4).
Figure 4. Comparison of significance of the interaction effects of two factors of barrier material-temporary restoration based on the Kruskal-Wallis test (1.00: flowable composite-Cavit, 2.00: RMGI-Cavit, 3.00: flowable composite-Zonalin, 4.00: RMGI-Zonalin)
{kind=link}
Effect of time, temporary restorative material, and barrier material:
The three-way interaction was significant (P=0.000). The Cavit-4 weeks-flowable composite subgroup exhibited the highest PBS (6.70±0.469 MPa), significantly greater than all other combinations (P=0.000). The lowest value was observed in the positive control group (cotton with eugenol-2 weeks-flowable composite: 0.302±0.101 MPa) (Figure 5). Other notable comparisons included:
- Cavit-4 weeks-RMGI (1.91±0.469 MPa; P=0.000)
- Zonalin-4 weeks-flowable composite (2.40±0.469 MPa; P=0.000)
- RMGI-4 weeks-Zonalin (2.57±0.469 MPa; P=0.000)
Figure 5. Mean PBS of intra-orifice barriers to dentin in the experimental groups
Failure mode analysis:
Group A3 (Cavit-4 weeks-flowable composite) exhibited the highest frequency of cohesive and mixed failures (87.5%); while, group C1 (positive control) showed the highest rate of adhesive failures (66.7%).
Discussion
{kind=link}
Failure mode analysis:
Group A3 (Cavit-4 weeks-flowable composite) exhibited the highest frequency of cohesive and mixed failures (87.5%); while, group C1 (positive control) showed the highest rate of adhesive failures (66.7%).
Discussion
This study investigated the effect of 2 and 4 weeks of temporary restoration placement (Cavit-Zonalin) on PBS of barrier material (flowable composite and RMGI) to the dentin of intra-orifice area. Different materials are used as intra-orifice barriers [15,16]. Aboobaker et al. [17] showed that GI and flowable composite as an intra-orifice barrier materials increase the fracture resistance of endodontically treated teeth compared to endodontically treated teeth without an intra-orifice barrier. Moazzami et al. [18] revealed that RMGI had a significantly higher microleakage compared to flowable composite, which is consistent with the findings of the present study. In some studies, no significant difference was observed in microleakage between flowable composite and RMGI as an intra-orifice barrier [4, 17, 19]. In the present study, flowable composite demonstrated a significantly higher PBS than RMGI. This discrepancy with previous studies may be attributed to the viscosity and application technique of the materials. The injection technique, along with the lower viscosity of RMGI, result in a continuous and integrated restoration with greater homogeneity.
The PBS test is recognized as a reliable and practical method for assessing the bond strength between adhesive materials and root dentin. Several factors influence the measurement of dentin bond strength under in vitro conditions, including tooth type, degree of dentin demineralization, bonding surface, type of bond strength test, tooth storage environment, and test conditions [3]. According to a previous study, none of the temporary restorative materials could prevent bacterial leakage into the root canal for a long time (30 days) [10]. In the present study, two-time intervals of 2 and 4 weeks were considered between the root canal therapy and placement of the barrier, to investigate the impact of maximum duration of placement of temporary restoration on PBS of the barrier.
Eugenol-containing materials offer several advantages for temporary restorations. However, they are believed to interfere with the polymerization process of composite restorations [20,21]. Silva et al. [6], and Bezerra et al. [8] showed that the time of exposure to ZOE affects the adhesive bond strength of total-etch and self-etch systems to dentin. According to these studies, the use of ZOE as a temporary restoration for 24 hours resulted in the lowest bond strength. However, this negative effect was not observed when ZOE was used for 1 or 2 weeks. Furthermore, the study indicated that the concentration of eugenol decreased as it approached the pulp chamber, suggesting that the inhibitory effect on polymerization is likely more pronounced near the surface [6, 8]. In the present study, it was also observed that the temporary restoration of ZOE for a period of 2 and 4 weeks did not have any significant effect on PBS of flowable composite. Based on the results of Koch et al. [20], the bond strength of two adhesive systems decreased when the dentin was exposed to ZOE before adhesive placement. They also observed that the exposure time to ZOE did not affect the adhesive bond strength [20], which is contrary to our findings. It should be noted that in their study, micro-tensile test was performed on coronal dentin, and the reason for this discrepancy with the present study could be the structural differences between the root canal dentin and the coronal dentin in terms of the number and diameter of dentinal tubules and the volume of peritubular dentin. Several studies have shown that the effect of eugenol on bond strength depends on the adhesive system used [5,22,23]. Khaitan et al. [5] emphasized that the use of phosphoric acid can remove the eugenol-contaminated layer when using a conventional etch-and-rinse system. In the present study, an etch-and-rinse system was also used, which can be one reason for the increase in PBS of flowable composite compared to RMGI after removal of the temporary Zonalin restoration. Ganss and Jung [23] concluded that the mean composite shear bond strength in the ZOE group was lower than that in the control group after 10 days, while the shear bond strength of the Temp Bond group (containing eugenol) was comparable to that of the control group. In the present study, it was also observed that the bond strength of the flowable composite was insignificantly greater after 2 weeks of placement of temporary Zonalin restoration compared to 4 weeks. Ajaj et al. [24], in their systematic review showed that temporary materials containing eugenol did not affect the bond strength of resin restorations after 7 days. Hence, it is possible that the reason for the increased bond strength of flowable composite after a period of 2 weeks compared to 4 weeks of placement of temporary Zonalin restoration is one of the ingredients of Zonalin other than eugenol, which affects the resin bond strength.
Ganss and Jung [23] showed that the temporary composite group exhibited the lowest adhesive bond strength after 10 days among all groups, while the Provicol group (containing calcium hydroxide) also showed lower bond strength than the control group after 10 days. In the present study, the A3 group (Cavit, 4 weeks, flowable composite) demonstrated the highest bond strength, with a significant difference observed compared to the A1 group (Cavit, 2 weeks, flowable composite). This difference may be attributed to the ingredients of Cavisol (zinc oxide, zinc sulfate, calcium sulfate, and resin), which influence the bond strength of composite resin.
In this study, we evaluated the effect of the duration of temporary restoration placement on PBS of the barrier to the intra-orifice dentin under in vitro conditions. The results suggest that other ingredients and conditions could affect the bond strength to the cervical dentin. Therefore, to better understand the interaction of different materials used in the restoration of endodontically treated teeth, further investigations, particularly under clinical conditions, are needed.
The present study was limited by its in vitro design, which may not fully replicate clinical conditions such as thermal fluctuations, occlusal forces, and microbial interactions. Variability in dentin morphology despite standardization may affect generalizability, and the restricted range of materials and time intervals evaluated may not encompass all clinically relevant scenarios.
Conclusion
The PBS test is recognized as a reliable and practical method for assessing the bond strength between adhesive materials and root dentin. Several factors influence the measurement of dentin bond strength under in vitro conditions, including tooth type, degree of dentin demineralization, bonding surface, type of bond strength test, tooth storage environment, and test conditions [3]. According to a previous study, none of the temporary restorative materials could prevent bacterial leakage into the root canal for a long time (30 days) [10]. In the present study, two-time intervals of 2 and 4 weeks were considered between the root canal therapy and placement of the barrier, to investigate the impact of maximum duration of placement of temporary restoration on PBS of the barrier.
Eugenol-containing materials offer several advantages for temporary restorations. However, they are believed to interfere with the polymerization process of composite restorations [20,21]. Silva et al. [6], and Bezerra et al. [8] showed that the time of exposure to ZOE affects the adhesive bond strength of total-etch and self-etch systems to dentin. According to these studies, the use of ZOE as a temporary restoration for 24 hours resulted in the lowest bond strength. However, this negative effect was not observed when ZOE was used for 1 or 2 weeks. Furthermore, the study indicated that the concentration of eugenol decreased as it approached the pulp chamber, suggesting that the inhibitory effect on polymerization is likely more pronounced near the surface [6, 8]. In the present study, it was also observed that the temporary restoration of ZOE for a period of 2 and 4 weeks did not have any significant effect on PBS of flowable composite. Based on the results of Koch et al. [20], the bond strength of two adhesive systems decreased when the dentin was exposed to ZOE before adhesive placement. They also observed that the exposure time to ZOE did not affect the adhesive bond strength [20], which is contrary to our findings. It should be noted that in their study, micro-tensile test was performed on coronal dentin, and the reason for this discrepancy with the present study could be the structural differences between the root canal dentin and the coronal dentin in terms of the number and diameter of dentinal tubules and the volume of peritubular dentin. Several studies have shown that the effect of eugenol on bond strength depends on the adhesive system used [5,22,23]. Khaitan et al. [5] emphasized that the use of phosphoric acid can remove the eugenol-contaminated layer when using a conventional etch-and-rinse system. In the present study, an etch-and-rinse system was also used, which can be one reason for the increase in PBS of flowable composite compared to RMGI after removal of the temporary Zonalin restoration. Ganss and Jung [23] concluded that the mean composite shear bond strength in the ZOE group was lower than that in the control group after 10 days, while the shear bond strength of the Temp Bond group (containing eugenol) was comparable to that of the control group. In the present study, it was also observed that the bond strength of the flowable composite was insignificantly greater after 2 weeks of placement of temporary Zonalin restoration compared to 4 weeks. Ajaj et al. [24], in their systematic review showed that temporary materials containing eugenol did not affect the bond strength of resin restorations after 7 days. Hence, it is possible that the reason for the increased bond strength of flowable composite after a period of 2 weeks compared to 4 weeks of placement of temporary Zonalin restoration is one of the ingredients of Zonalin other than eugenol, which affects the resin bond strength.
Ganss and Jung [23] showed that the temporary composite group exhibited the lowest adhesive bond strength after 10 days among all groups, while the Provicol group (containing calcium hydroxide) also showed lower bond strength than the control group after 10 days. In the present study, the A3 group (Cavit, 4 weeks, flowable composite) demonstrated the highest bond strength, with a significant difference observed compared to the A1 group (Cavit, 2 weeks, flowable composite). This difference may be attributed to the ingredients of Cavisol (zinc oxide, zinc sulfate, calcium sulfate, and resin), which influence the bond strength of composite resin.
In this study, we evaluated the effect of the duration of temporary restoration placement on PBS of the barrier to the intra-orifice dentin under in vitro conditions. The results suggest that other ingredients and conditions could affect the bond strength to the cervical dentin. Therefore, to better understand the interaction of different materials used in the restoration of endodontically treated teeth, further investigations, particularly under clinical conditions, are needed.
The present study was limited by its in vitro design, which may not fully replicate clinical conditions such as thermal fluctuations, occlusal forces, and microbial interactions. Variability in dentin morphology despite standardization may affect generalizability, and the restricted range of materials and time intervals evaluated may not encompass all clinically relevant scenarios.
Conclusion
Within the limitations of this in vitro study, the results indicated that the highest bond strength of intra-orifice barrier materials in endodontically treated teeth may be achieved by using Cavit temporary restorative material for 4 weeks in combination with a flowable composite.
Type of Study: Original article |
Subject:
Restorative Dentistry
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |