



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-94-en.html


2- Assistant Professor و University of Medical Sciences, Babol, Iran
3- Assistant Professor, Periodontology Dept, School of Dentistry, Kurdistan University of Medical Sciences, Sanandaj, IranKurdistan University of Medical Sciences, Sanandaj, Iran
4- Associate Professor, Periodontology Dept, Dental Branch of Tehran
5- Associate Professor , Periodontology Dept, Dental Branch of Tehran
Abstract
Background and aim: Micro-ultrasonic tips are similar to hand instruments in their clinical application of subgingival scaling. In spite of their favorable results, excessive penetration of mini-insert ultrasonic scalers to the bottom of gingival pocket may cause harmful effects. The aim of this study was to evaluate the immediate effect of root instrumentation with Gracey curettes and Mini-insert ultrasonic scalers on clinical attachment level.
Materials and Methods: In this single-blind split mouth study, fifteen patients with moderate chronic periodontitis and at least five periodontal pockets around incisors and canines with clinical attachment level ranging from 2 to 4 mm were randomly allocated to one of the following groups: Curette scaling (CS) and Ultrasonic scaling (US).The Teeth were probed with a pressure sensitive probe using an occlusal stent. Immediately after scaling and root planing, the teeth were probed again. The difference in Relative Attachment Level (RAL) immediately before and after instrumentation was considered trauma from instrumentation. The mean values recorded before and after root instrumentation were compared by student’s paired t-test and the differences in RAL measurements between the groups were compared by student’s non-paired t-test.
Results: There were statistically significant differences between the two groups regarding RAL before and after scaling and root planing (0.43+0.65 mm for US and 0.47+ 0.6 mm for CS) (P<0.001). However, no statistically significant difference was observed in RAL changes between the two groups (P=0.77).
Conclusion: Within the limitations of this study, it seems that use of thin tip ultrasonic scaler for periodontal nonsurgical treatment will result in immediate attachment loss at a level equal to hand instruments.
Key words: Dental Scaling; Periodontal Attachment Loss; Root Planing
Introduction
Periodontal treatment must include supragingival plaque control and subgingival scaling. Subgingival scaling is a mechanical treatment aimed at removing plaque, calculus and food debris, whether inside pockets, free or on root surface. 1 Subgingival scaling may be accomplished with different instruments such as hand and ultrasonic instruments. Manual scaling and root planing can often be difficult and time-consuming due to complex and unfavorable root morphology when working blindly at deep pocket sites. 2 Many clinical studies have reported equal clinical outcomes of root debridement with hand instruments, ultrasonic and sonic scalers 3-5, even in smokers, although less favorable results have been achieved compared with those of nonsmokers. 6 One major advantage of power-driven scalers is better access to difficult areas, such as deep narrow defects, root grooves and furcations, using newly designed micro-ultrasonic tips, which are smaller in diameter and able to penetrate the pocket approximately 1 mm farther than hand instruments.7,8 These new mini-inserts were first introduced in 1992 .9 Since then many manufacturers have offered a wide variety of these fine inserts. Although longitudinal follow-up studies have reported favorable results following subgingival scaling, with both hand and ultrasonic instruments , excessive penetration of the periodontal scaler to the bottom of gingival pocket causes harmful effects . However, clinical data relating to the immediate attachment loss after ultrasonic scaling with these newly designed tips are scarce. 10,11 Claffey et al reported an average attachment loss of 0.5-0.6 mm immediately after a single session of ultrasonic instrumentation with conventional ultrasonic tips.12Alves et al in 2004 reported a mean attachment loss of 0.76-1.06 mm after scaling and root planing with hand instruments.13 In 2005, Alves et al reported a mean immediate attachment loss of 0.75 mm after scaling and root planing with either curettes or conventional ultrasonic scalers. 3 To our knowledge, there is only one study measuring the immediate attachment loss after scaling caused by thin ultrasonic tips.14 Casarin et al have reported a higher immediate clinical attachment loss with tin tip rather than traditional tip. 14 There are no data comparing the attachment loss occurring after subgingival scaling performed with hand instruments and thin tip ultrasonic scaler. The objective of this single-blind split mouth study was to compare the immediate attachment loss caused by instrumentation using Gracey curettes and Mini-insert ultrasonic scalers.
MATERIALS AND METHODS
Study design:
This single-blind split mouth clinical trial included 15 subjects, 30-44 years old with moderate chronic periodontitis that referred to the Department of Periodontics, Dental Branch, Islamic Azad University. They presented at least five periodontal pockets around incisors and canines (upper and /or lower) with clinical attachment levels ranging from 2 to 4 mm. All the subjects were chosen based on specific selection criteria: good general health, at least 30 years of age, presence of at least 5 periodontal pockets around lower and/or upper incisors. Exclusion criteria included: use of antibiotics within 3 months prior to or during the study, use of any drugs interfering with tissue metabolism such as Niphedipine, Verapamil, and Phenytoin. Patients undergoing orthodontic therapy and patients with any systemic diseases were also excluded from the study. All the subjects signed an informed consent. The study protocol has been approved by the ethical committee of Dental Branch, Islamic Azad University.
Initial preparation:
On the first visit, all the subjects received oral hygiene instructions and were subjected to supragingival scaling with an ultrasonic scaler. Individual acrylic occlusal stents were made from plaster casts to standardize Relative Attachment Level measurements.
Relative attachment level (RAL) measurement:
One week later, the patients were probed by a calibrated examiner. Calibration was performed prior to the study and on the basis of duplicate clinical recordings in 3 patients. This procedure was done with a pressure sensitive probe (Aesculap DB764R, UNC 15, Meslungen, Germany) with defined probing force of 0.2 N (20 g). RAL was measured by the probe from a groove at the occlusal stent to the bottom of the pocket at four sites per tooth (mesiobuccal, midbuccal, distobuccal & midlingual). The attachment loss due to trauma from instrumentation was calculated by the difference between RAL measurements registered immediately before and after scaling and root planing.14
Scaling and root planing:
After the probing, the selected anterior teeth were anesthetized and were randomly assigned to one of the two groups: Curette scaling (CS) and Ultrasonic scaling (US). The selected anterior teeth of CS group were scaled and root planed with Gracey 5-6 conventional curettes (Hufriedy, Chicago, IL, USA). The curettes were sharpened whenever necessary. The selected anterior teeth of US group were scaled and root planed with an ultrasonic scaler (#100 thin tip, UI30SF100 Hufriedy, Chicago, IL, USA). For US group, each selected site was scaled by 30 movements. Similarly, each site received 30 strokes in CS group. Scaling and root planing in this study was done by one clinician other than the one who measured the RAL. Immediately following scaling and root planing, the teeth were probed again by the same blinded calibrated examiner and new measurements of RAL were recorded.
IBM SPSS ver. 19 (IBM Co., Armonk, NY, USA) was used for statistical analysis. Mean values of RAL were calculated for each patient of the two groups (US and CS). The mean values recorded before and after root instrumentation were compared by student’s paired t-test and the differences in RAL measurements between the groups were compared by student’s non-paired t-test. The level of statistical significance was set at 0.05.
Results
Fifteen eligible patients (8 males and 7 females) with moderate chronic periodontitis (Clinical attachment level of 2-4 mm) with the mean age of 37.1+ 8 years were involved in the study. Duplicate recordings on RAL were registered prior to the study in three patients. Intra-examiner repeatability was suitable (Spearman correlation coefficient equal to 0.892, P<0.001).
As shown in table 1, in US group mean RAL was 13.6+ 1.4 mm immediately before scaling and 14+ 1.4 mm immediately after instrumentation. The mean difference in RAL for this group was 0.43+ 0.65 mm and this difference was statistically significant (P<0.0001). In CS group, mean RAL was 13.6+ 1.7 mm immediately before scaling and 14.1+ 1.7mm immediately after it. The mean difference in RAL was 0.4 7+ 0.6 mm and this difference was statistically significant (P<0.0001). No statistically significant difference was observed in RAL changes between the two groups. (P=0.77)
The percentage of sites that showed immediate attachment loss between 0.1 and 1.0 mm was 95% for both US and CS groups. The percentage of sites that showed immediate attachment loss of over 1mm was 5% for both groups.
Table 2 shows the mean RAL immediately before and after instrumentation in each group at each measurement site (mesiobuccal, midbuccal, distobuccal and midlingual). The mean difference in each area was statistically significant. (mesiobuccal; P=0.041 for CS group and P=0.048 for US group, midbuccal; P=0.14 for CS group and P=0.007 for US group, distobuccal; P=0.014 for CS group and P=0.041 for US group, midlingual; P=0.001 for CS group and P=0.009 for US group ).
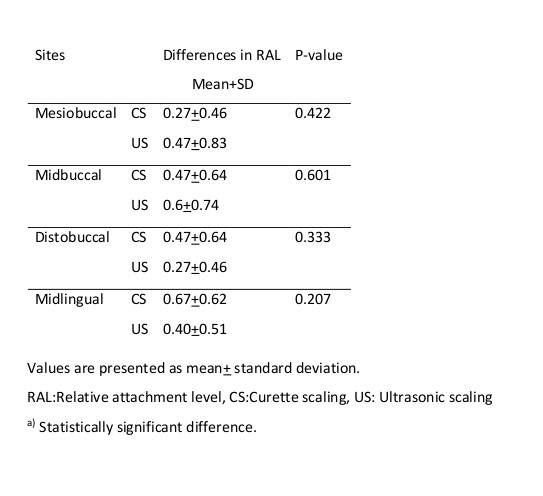
Table 3 shows the mean differences in RAL between the two groups at each measurement site (mesiobuccal, midbuccal, distobuccal and midlingual). No Statistically significant difference was observed in RAL changes between the two groups in each area. (mesiobuccal; P=0.422, midbuccal ;P=0.601, distobuccal; P=0.33 and midlingual; P=0.207).
Table 1: RAL measurements in mm (mean+ standard deviation) before and immediately after scaling in two groups
Table 2: RAL measurements in mm (mean + SD) before and immediately after scaling in study groups at different areas of the teeth (Mesiobuccal, Midbuccal, Distobuccal & Midlingual)
Table 3: Mean + SD differences in RAL before and immediately after scaling in two groups at different areas of the teeth (Mesiobuccal, Midbuccal, Distobuccal & Midlingual)
Discussion
{kind=link}
{kind=link}
{kind=link}
Our study compared the immediate attachment loss caused by instrumentation using Gracey curettes and Mini-insert ultrasonic scalers. Our results indicate a mean relative attachment loss of about 0.45 mm regarding both instruments.
The main comparable trials that we have been able to detect in the literature are the studies by Claffey et al, Alves et al and Casarin et al.12-14 Alves et al used the conventional type of ultrasonic tip. 3 Although they also reported no difference between the trauma from instrumentation produced by Gracey curettes and ultrasonic scalers, they showed a mean attachment loss of 0.75 mm. Claffey et al also used the conventional type of ultrasonic tip in their study and reported a mean attachment loss of 0.5-0.6 mm after instrumentation with ultrasonic scaler. 12 They studied on both single and multi-rooted teeth while the present study, similar to the study by Alves et al, included the anterior teeth only.13 Moreover, we included an initial preparation visit accompanied by oral hygiene instruction and supragingival debridement to reduce inflammation before probing as described previously by Alves et al. 13 Inflamed tissues are less resistant to probe penetration .15 In our study, the selected sites were scaled by 30 movements in ultrasonic group and 30 strokes in curette group, while Claffey et al have reported no certain limit for their debridement procedure. 12 In our study, the occurrence of sites with immediate attachment loss between 0.1 and 1 mm was 95% in both groups and this percentage was much higher than the percentages reported by Alves et al 3 (72.9% in ultrasonic group and 81.3% in curette group). Casarin et al have reported higher immediate attachment loss by thin ultrasonic tips (0.85 mm) compared to traditional tips (0.15 mm). 14 This can be simply interpreted by the fact that these new Mini-inserts have been designed to provide better access to deep pockets, so as they penetrate more deeply, they can cause more attachment loss than conventional tips. They have also reported similar healing after ultrasonic therapy either with thin tips or conventional tips. The differences between these studies could be attributed to methodological variations.
None of these studies have measured the immediate RAL at four sites per tooth. This allowed us to be able to compare the RAL all around the selected teeth, and the results showed that there were no statistically significant differences between these sites. In the present study, all the measurements were performed by the same calibrated clinician. Scaling and root planing in this study was done by one clinician to eliminate inter-operator variability and to minimize variations in factors such as stroke length, applied force and pressure during instrumentation.
The major shortcoming of this study is lack of a longitudinal evaluation. According to Obeid et al, the choice among various available nonsurgical techniques should be made on the basis of personal experience or preference; and any other consideration would not be based on proper analysis. 16 Although a recent study has reported that an experienced operator did not remove simulated plaque more efficiently, but they concluded that the operator induced less root surface destruction. 17 All these studies show that there is no difference among correct scaling and root planing methods, irrespective of the applied instrument. The choice between instruments depends on the experience of the clinician. This study emphasizes that thin ultrasonic tips and curettes cause equal immediate attachment loss, although more recent studies have tried to identify the appropriate power setting and operation time for ultrasonic slim-line plain insert scalers.18
Conclusion
The results of this study showed that there were no differences between relative attachment loss caused by either thin ultrasonic tips or curettes after instrumentation and both groups showed the same level of attachment loss. Overall, it appears that use of thin tip ultrasonic scaler for periodontal nonsurgical treatment will result in immediate attachment loss at a level equal to hand instruments.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
