Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 2 (6-2025)
J Res Dent Maxillofac Sci 2025, 10(2): 159-167 |
Back to browse issues page

Ethics code: IR.IAU.DENTAL.REC.1400.181
Clinical trials code: not applicable
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tahmasebi M, Heidarkhan Tehrani S, Mehmani F, Mesgari H, Mehdizadeh A. Anatomical Correlation Between Mandibular Third Molar Position and Retromolar Nerve Variations: A CBCT Study. J Res Dent Maxillofac Sci 2025; 10 (2) :159-167
URL: http://jrdms.dentaliau.ac.ir/article-1-866-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-866-en.html
Mahdis Tahmasebi1 
 , Sanaz Heidarkhan Tehrani2 , Fatemeh Mehmani *3 , Hassan Mesgari4 , Amirreza Mehdizadeh2
, Sanaz Heidarkhan Tehrani2 , Fatemeh Mehmani *3 , Hassan Mesgari4 , Amirreza Mehdizadeh2
, Sanaz Heidarkhan Tehrani2 , Fatemeh Mehmani *3 , Hassan Mesgari4 , Amirreza Mehdizadeh2
1- Dentist, Private Practice, Tehran.
2- Oral and Maxillofacial Radiology Department, TeMS.C, Islamic Azad University, Tehran, Iran.
3- Oral and Maxillofacial Radiology Department, TeMS.C, Islamic Azad University, Tehran, Iran. ,fatiii72mehmani@gmail.com
4- Oral and Maxillofacial Surgery Department, TeMS.C, Islamic Azad University, Tehran, Iran.
2- Oral and Maxillofacial Radiology Department, TeMS.C, Islamic Azad University, Tehran, Iran.
3- Oral and Maxillofacial Radiology Department, TeMS.C, Islamic Azad University, Tehran, Iran. ,
4- Oral and Maxillofacial Surgery Department, TeMS.C, Islamic Azad University, Tehran, Iran.
Full-Text [PDF 324 kb]
(823 Downloads)
| Abstract (HTML) (1777 Views)
Recommendations for future research:
Full-Text: (384 Views)
Abstract
Background and Aim: Variations in the retromolar canal (RMC) and retromolar nerve can cause complications. This study aimed to evaluate the relationship between the anatomical position of mandibular third molars and variations of the retromolar nerve using cone-beam computed tomography (CBCT) imaging.
Materials and Methods: A descriptive analytical study was conducted on CBCT images of the mandible from 126 individuals (82 females, 44 males) over the age of 25 years. The impaction status of the mandibular third molars was classified using Pell and Gregory's classification, while angulation was determined according to Winter's classification. The presence of the retromolar nerve, its buccal or lingual position relative to the mandibular third molar, and the distance between the RMC and mandibular third molar were evaluated.
Results: The retromolar nerve was present in 53 cases (42.1%). It was positioned buccally in 36 cases (28.6%) and lingually in 17 cases (13.5%) relative to the mandibular third molar. The mean distance between the RMC and the cementoenamel junction (CEJ) of the mandibular third molar was 5.41 mm. A significant relationship was found between the third molar impaction status and presence and position of the retromolar nerve (P=0.002).
Conclusion: The retromolar nerve was more frequently present in non-impacted mandibular third molars. In presence of semi-impacted third molars, the nerve was significantly more likely to be positioned buccally. These findings highlight the importance of preoperative CBCT imaging to identify anatomical variations, aiding in surgical planning and reducing the risk of neurological complications during mandibular third molar extractions.
Keywords: Cone-Beam Computed Tomography; Mandible; Nerve; Molar, Third
Introduction
Neurological complications are a major concern following mandibular third molar extraction due to close proximity of third molars to important nerve branches [1,2]. One anatomical region of particular relevance is the retromolar area, a triangular space located distal to the mandibular third molar. This area is bordered anteriorly by the third molar itself, laterally by the buccinator muscle, and medially by the tendon of the temporal muscle [3]. Variations within this region, notably the presence of the retromolar foramen and the retromolar canal (RMC), can have profound clinical implications [4]. The retromolar foramen can serve as the external opening of the RMC, an anatomical variation that extends from the mandibular canal to the retromolar area [5]. The RMC contains the retromolar nerve, which may provide accessory innervation to the mandibular molar region. Presence of the RMC poses several clinical challenges. One such issue is the potential failure of mandibular nerve block anesthesia. Accessory innervation through the RMC can lead to insufficient anesthesia during dental procedures, complicating treatments and increasing patient discomfort [6]. Additionally, surgical interventions in this area, such as third molar extraction or dental implant placement, carry the risk of injuring the contents of the RMC. Trauma to the retromolar nerve may result in sensory impairments, including paresthesia or numbness in the buccal mucosa and third molar region [7,8].
Cone-beam computed tomography (CBCT) has emerged as a valuable imaging modality in dentistry, offering three-dimensional, high-resolution images of dental and maxillofacial structures [9]. CBCT is particularly effective in detection of anatomical variations such as the RMC, providing detailed visualization that surpasses traditional two-dimensional imaging techniques [10]. The use of CBCT in preoperative assessments can be crucial for identifying the presence and trajectory of the RMC, thereby aiding in surgical planning and reducing the risk of intraoperative complications [11]. Understanding the variations of the RMC and the retromolar nerve is essential to improve clinical outcomes. Variations in the anatomical properties of the mandibular third molar, such as its angulation and depth of impaction, may influence the occurrence and position of the RMC [12,13]. However, limited research has comprehensively explored this relationship. Therefore, this study aimed to evaluate the relationship between the anatomical position of mandibular third molars and variations of the retromolar nerve using CBCT imaging.
Materials and Methods
This descriptive analytical study was conducted at the Radiology Department of Islamic Azad University Dental School, Tehran, Iran. The study was approved by the Ethics Committee of Islamic Azad University-Dental Branch, Tehran, Iran, with the identification number IR.IAU.DENTAL.REC.1400.181. All procedures conformed to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments.
Study population:
The study included all available CBCT images of patients over 25 years, both males and females, who had undergone mandibular CBCT imaging at the Radiology Department during the study period. The inclusion criteria were:
Background and Aim: Variations in the retromolar canal (RMC) and retromolar nerve can cause complications. This study aimed to evaluate the relationship between the anatomical position of mandibular third molars and variations of the retromolar nerve using cone-beam computed tomography (CBCT) imaging.
Materials and Methods: A descriptive analytical study was conducted on CBCT images of the mandible from 126 individuals (82 females, 44 males) over the age of 25 years. The impaction status of the mandibular third molars was classified using Pell and Gregory's classification, while angulation was determined according to Winter's classification. The presence of the retromolar nerve, its buccal or lingual position relative to the mandibular third molar, and the distance between the RMC and mandibular third molar were evaluated.
Results: The retromolar nerve was present in 53 cases (42.1%). It was positioned buccally in 36 cases (28.6%) and lingually in 17 cases (13.5%) relative to the mandibular third molar. The mean distance between the RMC and the cementoenamel junction (CEJ) of the mandibular third molar was 5.41 mm. A significant relationship was found between the third molar impaction status and presence and position of the retromolar nerve (P=0.002).
Conclusion: The retromolar nerve was more frequently present in non-impacted mandibular third molars. In presence of semi-impacted third molars, the nerve was significantly more likely to be positioned buccally. These findings highlight the importance of preoperative CBCT imaging to identify anatomical variations, aiding in surgical planning and reducing the risk of neurological complications during mandibular third molar extractions.
Keywords: Cone-Beam Computed Tomography; Mandible; Nerve; Molar, Third
Introduction
Neurological complications are a major concern following mandibular third molar extraction due to close proximity of third molars to important nerve branches [1,2]. One anatomical region of particular relevance is the retromolar area, a triangular space located distal to the mandibular third molar. This area is bordered anteriorly by the third molar itself, laterally by the buccinator muscle, and medially by the tendon of the temporal muscle [3]. Variations within this region, notably the presence of the retromolar foramen and the retromolar canal (RMC), can have profound clinical implications [4]. The retromolar foramen can serve as the external opening of the RMC, an anatomical variation that extends from the mandibular canal to the retromolar area [5]. The RMC contains the retromolar nerve, which may provide accessory innervation to the mandibular molar region. Presence of the RMC poses several clinical challenges. One such issue is the potential failure of mandibular nerve block anesthesia. Accessory innervation through the RMC can lead to insufficient anesthesia during dental procedures, complicating treatments and increasing patient discomfort [6]. Additionally, surgical interventions in this area, such as third molar extraction or dental implant placement, carry the risk of injuring the contents of the RMC. Trauma to the retromolar nerve may result in sensory impairments, including paresthesia or numbness in the buccal mucosa and third molar region [7,8].
Cone-beam computed tomography (CBCT) has emerged as a valuable imaging modality in dentistry, offering three-dimensional, high-resolution images of dental and maxillofacial structures [9]. CBCT is particularly effective in detection of anatomical variations such as the RMC, providing detailed visualization that surpasses traditional two-dimensional imaging techniques [10]. The use of CBCT in preoperative assessments can be crucial for identifying the presence and trajectory of the RMC, thereby aiding in surgical planning and reducing the risk of intraoperative complications [11]. Understanding the variations of the RMC and the retromolar nerve is essential to improve clinical outcomes. Variations in the anatomical properties of the mandibular third molar, such as its angulation and depth of impaction, may influence the occurrence and position of the RMC [12,13]. However, limited research has comprehensively explored this relationship. Therefore, this study aimed to evaluate the relationship between the anatomical position of mandibular third molars and variations of the retromolar nerve using CBCT imaging.
Materials and Methods
This descriptive analytical study was conducted at the Radiology Department of Islamic Azad University Dental School, Tehran, Iran. The study was approved by the Ethics Committee of Islamic Azad University-Dental Branch, Tehran, Iran, with the identification number IR.IAU.DENTAL.REC.1400.181. All procedures conformed to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments.
Study population:
The study included all available CBCT images of patients over 25 years, both males and females, who had undergone mandibular CBCT imaging at the Radiology Department during the study period. The inclusion criteria were:
- Presence of a sound mandibular third molar without radiographic artifacts due to metal restorations in adjacent teeth.
- Complete visibility of the retromolar area on both sides of the mandible.
The exclusion criteria were images with poor quality or artifacts interfering with evaluation, and patients with any pathology or previous surgical intervention in the mandibular molar region.
Sample size and sampling method:
Using PASS 11 software (α=0.05, β=0.2, w=0.5, degree of freedom=9), the minimum required sample size was determined to be 126 CBCT images. A total of 126 CBCT images meeting the eligibility criteria were collected through convenience sampling from the Radiology Department.
Data collection:
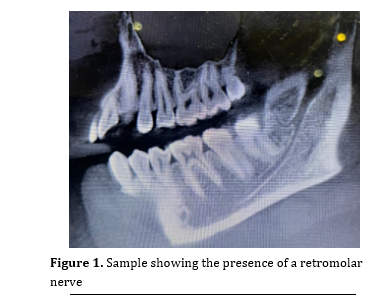
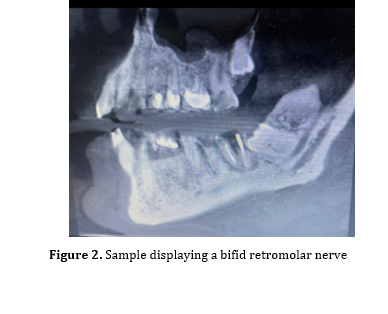
CBCT images had been obtained using a PaX-i3D CBCT scanner (Vatech, Korea) with a voxel size of 0.175 mm and a field of view of 8.5 × 8.5 cm. Images were initially processed using Dental Studio software and then imported to OnDemand3D software (Cybermed, South Korea) for analysis (Figures 1 and 2).
Figure 1. Sample showing the presence of a retromolar nerve
Figure 2. Sample displaying a bifid retromolar nerve
Image analysis:
Mandibular third molar classification:
Depth of impaction: According to the Pell and Gregory classification [14], the teeth were categorized into non-impacted, semi-impacted, and impacted teeth.
Angulation: Based on the Winter's classification [15], the teeth were categorized into:
Sample size and sampling method:
Using PASS 11 software (α=0.05, β=0.2, w=0.5, degree of freedom=9), the minimum required sample size was determined to be 126 CBCT images. A total of 126 CBCT images meeting the eligibility criteria were collected through convenience sampling from the Radiology Department.
Data collection:
CBCT images had been obtained using a PaX-i3D CBCT scanner (Vatech, Korea) with a voxel size of 0.175 mm and a field of view of 8.5 × 8.5 cm. Images were initially processed using Dental Studio software and then imported to OnDemand3D software (Cybermed, South Korea) for analysis (Figures 1 and 2).
Figure 1. Sample showing the presence of a retromolar nerve
{kind=link}
Figure 2. Sample displaying a bifid retromolar nerve
{kind=link}
Image analysis:
Mandibular third molar classification:
Depth of impaction: According to the Pell and Gregory classification [14], the teeth were categorized into non-impacted, semi-impacted, and impacted teeth.
Angulation: Based on the Winter's classification [15], the teeth were categorized into:
- Vertical: Vertically impacted teeth were aligned parallel to the longitudinal axis of the second molar.
- Horizontal: The crown was oriented horizontally, making eruption difficult.
- Mesioangular: In this type, the crown of the tooth was angled towards the front of the mouth.
- Distoangular: The tooth was angled towards the back of the mouth.
Retromolar nerve evaluation:
- Presence of RMC: Determined in the corrected sagittal plane and multiplanar reconstruction views.
- Position relative to third molar: Assessed in sagittal, coronal, and axial planes to determine if the retromolar nerve was buccal or lingual to the mandibular third molar.
- Distance measurement: The distance from the RMC to the cementoenamel junction (CEJ) of the mandibular third molar of the same side was measured in millimeters.
- Laterality: Recorded as left, right, or bilateral.
Data reliability:
To ensure measurement reliability, 20% of the samples were randomly re-evaluated by the same researcher after 2 weeks. The intra-examiner reliability was assessed using the kappa statistics and intraclass correlation coefficient.
Statistical analysis:
Data were analyzed using SPSS version 26. Descriptive statistics were calculated for all variables. The Pearson's Chi-square test was used to assess the relationship between the categorical variables; while, the Pearson's correlation coefficient was used for continuous variables. A P value of less than 0.05 was considered statistically significant.
Results
A total of 126 mandibular third molars of patients over 25 years of age were evaluated on CBCT scans. The sample consisted of CBCT images of 82 females (65.1%) and 44 males (34.9%), with a mean age of 35.3 years (range 25 to 70 years).
Mandibular third molar characteristics:
The mandibular third molars were assessed based on their angulation and depth of impaction to understand their anatomical relationship with the retromolar nerve.
Angulation (Winter's classification):
According to the Winter's classification, the distribution of third molar angulation in the study population was as follows:
To ensure measurement reliability, 20% of the samples were randomly re-evaluated by the same researcher after 2 weeks. The intra-examiner reliability was assessed using the kappa statistics and intraclass correlation coefficient.
Statistical analysis:
Data were analyzed using SPSS version 26. Descriptive statistics were calculated for all variables. The Pearson's Chi-square test was used to assess the relationship between the categorical variables; while, the Pearson's correlation coefficient was used for continuous variables. A P value of less than 0.05 was considered statistically significant.
Results
A total of 126 mandibular third molars of patients over 25 years of age were evaluated on CBCT scans. The sample consisted of CBCT images of 82 females (65.1%) and 44 males (34.9%), with a mean age of 35.3 years (range 25 to 70 years).
Mandibular third molar characteristics:
The mandibular third molars were assessed based on their angulation and depth of impaction to understand their anatomical relationship with the retromolar nerve.
Angulation (Winter's classification):
According to the Winter's classification, the distribution of third molar angulation in the study population was as follows:
- Vertical impactions were observed in 43 cases (34.1%), and were the second most common type.
- Mesioangular impactions were the most prevalent angulation type, found in 66 cases (52.4%).
- Horizontal impactions were detected in 14 cases (11.1%).
- Distoangular impactions were the least common, present in 3 cases (2.4%).
Depth of impaction (Pell and Gregory classification):
Based on the Pell and Gregory classification for the depth of impaction, the third molars were categorized as:
Based on the Pell and Gregory classification for the depth of impaction, the third molars were categorized as:
- Non-impacted: 51 cases (40.5%) had fully erupted third molars with no impaction.
- Semi-impacted: 49 cases (38.9%) showed partial eruption.
- Impacted: 26 cases (20.6%) had third molars that were completely impacted.
Presence and position of the retromolar nerve:
The retromolar nerve was identified in 53 out of 126 cases, indicating a prevalence of 42.1% in the study population.
Position relative to the mandibular third molar:
Among the cases where the retromolar nerve was present:
The retromolar nerve was identified in 53 out of 126 cases, indicating a prevalence of 42.1% in the study population.
Position relative to the mandibular third molar:
Among the cases where the retromolar nerve was present:
- Buccal position: In 36 cases (28.6%), the nerve was located in the buccal side of the mandibular third molar.
- Lingual position: In 17 cases (13.5%), the nerve was found in the lingual side.
Laterality:
Presence of retromolar nerve was also analyzed concerning the side of the mandible:
Presence of retromolar nerve was also analyzed concerning the side of the mandible:
- Right side: The nerve was present in 22 cases (41.5%). Specifically, 16 cases had the nerve positioned buccally, and 6 cases had it positioned lingually.
- Left side: The nerve was present in 31 cases (58.5%), with 20 buccal and 11 lingual positions.
Although the nerve was more frequently observed in the left side, statistical analysis showed no significant difference between the right and left sides regarding the presence or position of the retromolar nerve (P>0.05).
Distance between the RMC and third molar:
The proximity of the RMC to the mandibular third molar was assessed by measuring the distance from the RMC to the CEJ of the third molar of the same side. The mean distance was found to be 5.41 mm (range 2.30 to 10.67 mm).
Relationship between the retromolar nerve and third molar angulation:
The study explored whether the angulation of the mandibular third molar influenced the presence or position of the retromolar nerve.
Distance between the RMC and third molar:
The proximity of the RMC to the mandibular third molar was assessed by measuring the distance from the RMC to the CEJ of the third molar of the same side. The mean distance was found to be 5.41 mm (range 2.30 to 10.67 mm).
Relationship between the retromolar nerve and third molar angulation:
The study explored whether the angulation of the mandibular third molar influenced the presence or position of the retromolar nerve.
- In vertical impactions, the retromolar nerve was present in 21 out of 43 cases (48.8%), with 14 buccal and 7 lingual positions.
- For mesioangular impactions, the nerve was present in 25 out of 66 cases (37.9%), with 18 buccal and 7 lingual positions.
- Among horizontal impactions, 6 out of 14 cases (42.9%) had the nerve present (4 buccal and 2 lingual).
- In distoangular impactions, the nerve was present in 1 out of 3 cases (33.3%), positioned lingually.
Statistical analysis revealed no significant association between the angulation of third molar and presence or position of the retromolar nerve (P>0.05).
Relationship between retromolar nerve and depth of impaction:
A significant relationship was found between the depth of impaction of the mandibular third molar and presence and position of the retromolar nerve (P=0.002).
Relationship between retromolar nerve and depth of impaction:
A significant relationship was found between the depth of impaction of the mandibular third molar and presence and position of the retromolar nerve (P=0.002).
- Non-impacted third molars: The nerve was present in 14 out of 26 cases (53.8%), with 6 buccal and 8 lingual positions. This group had the highest prevalence of the retromolar nerve.
- Semi-impacted third molars: The nerve was identified in 23 out of 49 cases (46.9%), predominantly positioned buccally (21 cases) compared to lingually (2 cases).
- Impacted third molars: The nerve was present in 16 out of 51 cases (31.4%), with 9 buccal and 7 lingual positions.
Correlation with age and sex:
Age: The mean age of patients with the retromolar nerve was similar to that of the total study population (35.3 years). Statistical analysis showed no significant correlation between age and presence or position of the retromolar nerve (P>0.05).
Sex: Among the 53 cases with the retromolar nerve, 34 cases (64.2%) were females and 19 cases (35.8%) were males. Statistical analysis showed that there was no significant difference between males and females regarding the presence or position of the retromolar nerve (P>0.05).
Intra-examiner reliability:
Categorical variables: The kappa statistic was used to evaluate agreement for variables such as the presence and position of the retromolar nerve. The kappa values ranged from 0.85 to 0.90, indicating excellent agreement and high consistency in observations.
Continuous variables: The intraclass correlation coefficient was used for continuous measurements like the distance from the RMC to the third molar. The intraclass correlation coefficient was calculated to be 0.92, reflecting excellent reliability.
Discussion
The present study investigated the anatomical relationship and position of the mandibular third molar concerning variations of the retromolar nerve using CBCT images. The findings revealed that the retromolar nerve was present in 42.1% of the cases, a prevalence that holds significant clinical importance for dental practitioners, particularly oral surgeons involved in procedures in the mandibular molar region. Comparatively, this prevalence rate aligns closely with that reported by Moreno Rabie et al. [5], who found the retromolar nerve present in 56.7% of their study population. This similarity may stem from comparable methodologies and similar population characteristics of the two studies. However, the present results differ notably from those of Nikkerdar et al. [16], who reported a lower prevalence of 22% in their study on 200 CBCT images, and Sisman et al. [12], who found a prevalence of 26.7% in their analysis on panoramic and CBCT images of 632 patients. Such discrepancies could be attributed to several factors, including differences in sample size, imaging modalities, inclusion criteria, and population demographics. Additionally, Park et al. [17] conducted a study in South Korea and reported a significantly lower prevalence of the retromolar nerve at 11.5%. This considerable variation suggests that racial or ethnic differences may influence the occurrence of the retromolar nerve. Anatomical variations influenced by genetics could account for such differences in prevalence across different populations. Despite the variation in prevalence rates, it is noteworthy that the mean distance between the RMC and CEJ of mandibular third molars in the current study (5.41 mm) closely aligns with that reported by Park et al. [17], which was 5.8 mm. This consistency indicates that while the prevalence of the retromolar nerve may vary, the anatomical relationship between the RMC and third molar remains relatively constant across different ethnic groups.
The current study did not find a significant association between third molar angulation and presence of the retromolar nerve. The distribution of the retromolar nerve across different angulations—vertical, mesioangular, horizontal, and distoangular—mirrored the findings of Vranckx et al. [13] who reported a similar distribution in Belgium, with vertical impactions exhibiting the highest prevalence. Moreno Rabie et al. [5], also observed a similar trend in their study. Such consistent findings suggest that third molar angulation does not significantly influence the presence of the retromolar nerve. Consequently, clinicians should consider the potential for the nerve's presence regardless of the tooth's orientation during surgical planning.
The current observation that the retromolar nerve was positioned buccally in 57.1% of the cases and lingually in 42.9% aligns with the findings of Nikkerdar et al. [16], who reported buccal positioning in 52.7% of the cases, and Park et al. [17] who found a buccal position in 55.3% of the cases. The slight predominance of buccal positioning may have practical implications, as buccal surgical approaches are commonly employed in mandibular procedures. While the difference in positioning was not statistically significant, knowledge about the potential for the nerve to be located buccally or lingually is crucial to minimize the risk of nerve injury during surgical interventions.
Regarding demographic factors, the current study found no significant relationship between the presence of the retromolar nerve and patients' age or sex. This finding is consistent with the results of Motamedi et al, [18] who conducted an anthropomorphic evaluation of the retromolar foramen and retromolar nerve in the Iranian population and reported no significant association with age or sex. Similarly, Nikkerdar et al. [16] and Puche-Roses et al. [19] studied Iranian and Spanish populations, respectively, and concluded that demographic factors did not significantly influence the occurrence of the retromolar nerve. These consistent observations across different populations suggest that the presence of the retromolar nerve is an anatomical variation that is independent of age and sex.
A significant finding of the current study was the association between the depth of impaction of mandibular third molars and presence and position of the retromolar nerve. The current study found a statistically significant relationship, with the nerve being more prevalent in non-impacted teeth (53.8%), followed by semi-impacted (46.9%) and impacted teeth (31.4%). Notably, in semi-impacted cases, the buccal positioning of the nerve was significantly more common than lingual positioning. This observation suggests that the degree of impaction may influence the development or positioning of the retromolar nerve.
This finding contrasts with the findings of a study by Demire et al. [20], who evaluated the relationship between mandibular third molar impaction and presence and position of the retromolar nerve and reported no significant association between these variables. The discrepancy between the current results and those of Demire et al. [20] could be due to differences in study design, sample size, population characteristics, or the criteria used to classify impaction levels. Additionally, racial and genetic differences may play a role in anatomical variations of the mandible that influence the relationship between third molar impaction and the retromolar nerve. The significant association observed may be explained by considering the anatomical and developmental changes that occur during tooth eruption and impaction. Non-impacted and semi-impacted third molars may exert different pressures on the surrounding bone and soft tissues compared to impacted teeth, potentially affecting the formation or trajectory of the RMC [21]. The process of tooth eruption involves bone remodeling and alterations in the mandibular architecture, which could influence the development of accessory canals like the RMC [22]. Further research exploring the biological mechanisms underlying this association would enhance our understanding of mandibular anatomy and its clinical implications.
Clinically, the high prevalence of the retromolar nerve and its significant association with the depth of third molar impaction underscore the importance of comprehensive preoperative assessment. CBCT imaging offers detailed visualization of the mandibular anatomy and should be considered an essential tool in surgical planning for procedures involving the mandibular molar region [2]. Knowledge about the potential presence and position of the retromolar nerve allows clinicians to modify surgical techniques, such as altering incision locations, flap designs, and osteotomy procedures, to reduce the risk of nerve injury [8]. Injury to the retromolar nerve can result in postoperative complications such as altered sensation, paresthesia, or dysesthesia, which can have significant impacts on the quality of life [23].
Moreover, presence of the retromolar nerve has implications beyond surgical procedures. It may affect the efficacy of local anesthesia in the mandibular region. Failure to achieve adequate anesthesia may be due to unrecognized anatomical variations like the retromolar nerve [24]. Therefore, anesthetists and dental practitioners should consider the possibility of such variations when planning anesthetic blocks to ensure effective pain management during dental procedures [25].
Limitations
Sample size and population: This study was conducted on patients from a single institute, which may limit the generalizability of the findings to other populations or ethnic groups.
Age: The mean age of patients with the retromolar nerve was similar to that of the total study population (35.3 years). Statistical analysis showed no significant correlation between age and presence or position of the retromolar nerve (P>0.05).
Sex: Among the 53 cases with the retromolar nerve, 34 cases (64.2%) were females and 19 cases (35.8%) were males. Statistical analysis showed that there was no significant difference between males and females regarding the presence or position of the retromolar nerve (P>0.05).
Intra-examiner reliability:
Categorical variables: The kappa statistic was used to evaluate agreement for variables such as the presence and position of the retromolar nerve. The kappa values ranged from 0.85 to 0.90, indicating excellent agreement and high consistency in observations.
Continuous variables: The intraclass correlation coefficient was used for continuous measurements like the distance from the RMC to the third molar. The intraclass correlation coefficient was calculated to be 0.92, reflecting excellent reliability.
Discussion
The present study investigated the anatomical relationship and position of the mandibular third molar concerning variations of the retromolar nerve using CBCT images. The findings revealed that the retromolar nerve was present in 42.1% of the cases, a prevalence that holds significant clinical importance for dental practitioners, particularly oral surgeons involved in procedures in the mandibular molar region. Comparatively, this prevalence rate aligns closely with that reported by Moreno Rabie et al. [5], who found the retromolar nerve present in 56.7% of their study population. This similarity may stem from comparable methodologies and similar population characteristics of the two studies. However, the present results differ notably from those of Nikkerdar et al. [16], who reported a lower prevalence of 22% in their study on 200 CBCT images, and Sisman et al. [12], who found a prevalence of 26.7% in their analysis on panoramic and CBCT images of 632 patients. Such discrepancies could be attributed to several factors, including differences in sample size, imaging modalities, inclusion criteria, and population demographics. Additionally, Park et al. [17] conducted a study in South Korea and reported a significantly lower prevalence of the retromolar nerve at 11.5%. This considerable variation suggests that racial or ethnic differences may influence the occurrence of the retromolar nerve. Anatomical variations influenced by genetics could account for such differences in prevalence across different populations. Despite the variation in prevalence rates, it is noteworthy that the mean distance between the RMC and CEJ of mandibular third molars in the current study (5.41 mm) closely aligns with that reported by Park et al. [17], which was 5.8 mm. This consistency indicates that while the prevalence of the retromolar nerve may vary, the anatomical relationship between the RMC and third molar remains relatively constant across different ethnic groups.
The current study did not find a significant association between third molar angulation and presence of the retromolar nerve. The distribution of the retromolar nerve across different angulations—vertical, mesioangular, horizontal, and distoangular—mirrored the findings of Vranckx et al. [13] who reported a similar distribution in Belgium, with vertical impactions exhibiting the highest prevalence. Moreno Rabie et al. [5], also observed a similar trend in their study. Such consistent findings suggest that third molar angulation does not significantly influence the presence of the retromolar nerve. Consequently, clinicians should consider the potential for the nerve's presence regardless of the tooth's orientation during surgical planning.
The current observation that the retromolar nerve was positioned buccally in 57.1% of the cases and lingually in 42.9% aligns with the findings of Nikkerdar et al. [16], who reported buccal positioning in 52.7% of the cases, and Park et al. [17] who found a buccal position in 55.3% of the cases. The slight predominance of buccal positioning may have practical implications, as buccal surgical approaches are commonly employed in mandibular procedures. While the difference in positioning was not statistically significant, knowledge about the potential for the nerve to be located buccally or lingually is crucial to minimize the risk of nerve injury during surgical interventions.
Regarding demographic factors, the current study found no significant relationship between the presence of the retromolar nerve and patients' age or sex. This finding is consistent with the results of Motamedi et al, [18] who conducted an anthropomorphic evaluation of the retromolar foramen and retromolar nerve in the Iranian population and reported no significant association with age or sex. Similarly, Nikkerdar et al. [16] and Puche-Roses et al. [19] studied Iranian and Spanish populations, respectively, and concluded that demographic factors did not significantly influence the occurrence of the retromolar nerve. These consistent observations across different populations suggest that the presence of the retromolar nerve is an anatomical variation that is independent of age and sex.
A significant finding of the current study was the association between the depth of impaction of mandibular third molars and presence and position of the retromolar nerve. The current study found a statistically significant relationship, with the nerve being more prevalent in non-impacted teeth (53.8%), followed by semi-impacted (46.9%) and impacted teeth (31.4%). Notably, in semi-impacted cases, the buccal positioning of the nerve was significantly more common than lingual positioning. This observation suggests that the degree of impaction may influence the development or positioning of the retromolar nerve.
This finding contrasts with the findings of a study by Demire et al. [20], who evaluated the relationship between mandibular third molar impaction and presence and position of the retromolar nerve and reported no significant association between these variables. The discrepancy between the current results and those of Demire et al. [20] could be due to differences in study design, sample size, population characteristics, or the criteria used to classify impaction levels. Additionally, racial and genetic differences may play a role in anatomical variations of the mandible that influence the relationship between third molar impaction and the retromolar nerve. The significant association observed may be explained by considering the anatomical and developmental changes that occur during tooth eruption and impaction. Non-impacted and semi-impacted third molars may exert different pressures on the surrounding bone and soft tissues compared to impacted teeth, potentially affecting the formation or trajectory of the RMC [21]. The process of tooth eruption involves bone remodeling and alterations in the mandibular architecture, which could influence the development of accessory canals like the RMC [22]. Further research exploring the biological mechanisms underlying this association would enhance our understanding of mandibular anatomy and its clinical implications.
Clinically, the high prevalence of the retromolar nerve and its significant association with the depth of third molar impaction underscore the importance of comprehensive preoperative assessment. CBCT imaging offers detailed visualization of the mandibular anatomy and should be considered an essential tool in surgical planning for procedures involving the mandibular molar region [2]. Knowledge about the potential presence and position of the retromolar nerve allows clinicians to modify surgical techniques, such as altering incision locations, flap designs, and osteotomy procedures, to reduce the risk of nerve injury [8]. Injury to the retromolar nerve can result in postoperative complications such as altered sensation, paresthesia, or dysesthesia, which can have significant impacts on the quality of life [23].
Moreover, presence of the retromolar nerve has implications beyond surgical procedures. It may affect the efficacy of local anesthesia in the mandibular region. Failure to achieve adequate anesthesia may be due to unrecognized anatomical variations like the retromolar nerve [24]. Therefore, anesthetists and dental practitioners should consider the possibility of such variations when planning anesthetic blocks to ensure effective pain management during dental procedures [25].
Limitations
Sample size and population: This study was conducted on patients from a single institute, which may limit the generalizability of the findings to other populations or ethnic groups.
- Imaging limitations: Although CBCT provides high-resolution images, there may still be limitations in detecting very small anatomical structures or variations.
Recommendations for future research:
- Larger multicenter studies: Conducting studies on larger and more diverse populations can help validate these findings and explore potential racial or ethnic differences.
- Comprehensive anatomical mapping: Including assessments of other anatomical landmarks, such as the second molar and the dimensions of the retromolar area, can provide a more detailed understanding of the retromolar nerve's anatomical relationships.
Clinical outcome studies: Investigating the correlation between the presence of the retromolar nerve and postoperative complications can help establish clinical guidelines for surgical practice.
Conclusion
The retromolar nerve was present in a notable proportion of the study population, with a higher prevalence in non-impacted mandibular third molars and a tendency to be positioned buccally in semi-impacted teeth. No significant associations were found with age, sex, or third molar angulation. These findings emphasize the need for careful preoperative evaluation using CBCT imaging to identify anatomical variations that may affect surgical planning. Knowledge about the retromolar nerve's presence and position can help clinicians minimize the risk of nerve injury, enhancing patient care during mandibular third molar surgery. Further research on larger and more diverse populations is recommended to expand upon these findings and improve clinical guidelines.
Declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Islamic Azad University-Dental Branch, Tehran, Iran, with the identification number IR.IAU.DENTAL.REC.1400.181. All procedures conformed to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Informed consent for publication was obtained from all individual participants included in the study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
The authors declare that they received no funding for this study.
Conclusion
The retromolar nerve was present in a notable proportion of the study population, with a higher prevalence in non-impacted mandibular third molars and a tendency to be positioned buccally in semi-impacted teeth. No significant associations were found with age, sex, or third molar angulation. These findings emphasize the need for careful preoperative evaluation using CBCT imaging to identify anatomical variations that may affect surgical planning. Knowledge about the retromolar nerve's presence and position can help clinicians minimize the risk of nerve injury, enhancing patient care during mandibular third molar surgery. Further research on larger and more diverse populations is recommended to expand upon these findings and improve clinical guidelines.
Declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Islamic Azad University-Dental Branch, Tehran, Iran, with the identification number IR.IAU.DENTAL.REC.1400.181. All procedures conformed to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Informed consent for publication was obtained from all individual participants included in the study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
The authors declare that they received no funding for this study.
Type of Study: Original article |
Subject:
Radiology
References
1. Leung YY. Management and prevention of third molar surgery-related trigeminal nerve injury: time for a rethink. J Korean Assoc Oral Maxillofac Surg. 2019 Oct;45(5):233-40. [DOI:10.5125/jkaoms.2019.45.5.233] [PMID] []
2. Bigagnoli S, Greco C, Costantinides F, Porrelli D, Bevilacqua L, Maglione M. CBCT Radiological Features as Predictors of Nerve Injuries in Third Molar Extractions: Multicenter Prospective Study on a Northeastern Italian Population. Dent J (Basel). 2021 Feb 21;9(2):23. [DOI:10.3390/dj9020023] [PMID] []
3. Truong MK, He P, Adeeb N, Oskouian RJ, Tubbs RS, Iwanaga J. Clinical Anatomy and Significance of the Retromolar Foramina and Their Canals: A Literature Review. Cureus. 2017 Oct 17;9(10):e1781. [DOI:10.7759/cureus.1781]
4. Luangchana P, Pornprasertsuk-Damrongsri S, Kitisubkanchana J, Wongchuensoontorn C. The retromolar canal and its variations: Classification using cone beam computed tomography. Quintessence Int. 2018;49(1):61-7.
5. Moreno Rabie C, Vranckx M, Rusque MI, Deambrosi C, Ockerman A, Politis C, Jacobs R. Anatomical relation of third molars and the retromolar canal. Br J Oral Maxillofac Surg. 2019 Oct;57(8):765-70. [DOI:10.1016/j.bjoms.2019.07.006] [PMID]
6. Gamieldien MY, Van Schoor A. Retromolar foramen: an anatomical study with clinical considerations. Br J Oral Maxillofac Surg. 2016 Sep;54(7):784-7. [DOI:10.1016/j.bjoms.2016.05.011] [PMID]
7. von Arx T, Hänni A, Sendi P, Buser D, Bornstein MM. Radiographic study of the mandibular retromolar canal: an anatomic structure with clinical importance. J Endod. 2011 Dec;37(12):1630-5. [DOI:10.1016/j.joen.2011.09.007] [PMID]
8. Kikuta S, Iwanaga J, Nakamura K, Hino K, Nakamura M, Kusukawa J. The retromolar canals and foramina: radiographic observation and application to oral surgery. Surg Radiol Anat. 2018 Jun;40(6):647-52. [DOI:10.1007/s00276-018-2005-5] [PMID]
9. Reia VCB, de Toledo Telles-Araujo G, Peralta-Mamani M, Biancardi MR, Rubira CMF, Rubira-Bullen IRF. Diagnostic accuracy of CBCT compared to panoramic radiography in predicting IAN exposure: a systematic review and meta-analysis. Clin Oral Investig. 2021 Aug;25(8):4721-33. [DOI:10.1007/s00784-021-03942-4] [PMID]
10. Neves FS, Souza TC, Almeida SM, Haiter-Neto F, Freitas DQ, Bóscolo FN. Correlation of panoramic radiography and cone beam CT findings in the assessment of the relationship between impacted mandibular third molars and the mandibular canal. Dentomaxillofac Radiol. 2012 Oct;41(7):553-7. [DOI:10.1259/dmfr/22263461] [PMID] []
11. Naitoh M, Hiraiwa Y, Aimiya H, Gotoh M, Ariji Y, Izumi M, et al. Bifid mandibular canal in Japanese. Implant Dent. 2007 Mar;16(1):24-32. [DOI:10.1097/ID.0b013e3180312323] [PMID]
12. Sisman Y, Ercan-Sekerci A, Payveren-Arikan M, Sahman H. Diagnostic accuracy of cone-beam CT compared with panoramic images in predicting retromolar canal during extraction of impacted mandibular third molars. Med Oral Patol Oral Cir Bucal. 2015 Jan 1;20(1):e74-81. [DOI:10.4317/medoral.19930] [PMID] []
13. Vranckx M, Ockerman A, Coucke W, Claerhout E, Grommen B, Miclotte A, Van Vlierberghe M, Politis C, Jacobs R. Radiographic prediction of mandibular third molar eruption and mandibular canal involvement based on angulation. Orthod Craniofac Res. 2019 May;22(2):118-23. [DOI:10.1111/ocr.12297] [PMID]
14. Pell GJ. Impacted mandibular third molars, classification and modified technique for removal. Dental Digest. 1933;39:330-8.
15. Winter GB. Impacted mandibular third molars. St Louis: American Medical Book Co. 1926;79.
16. Nikkerdar N, Golshah A, Norouzi M, Falah-Kooshki S. Incidence and Anatomical Properties of Retromolar Canal in an Iranian Population: A Cone‐Beam Computed Tomography Study. International journal of dentistry. 2020;2020(1):9178973. [DOI:10.1155/2020/9178973] [PMID] []
17. Park MK, Jung W, Bae JH, Kwak HH. Anatomical and radiographic study of the mandibular retromolar canal. J Dent Sci. 2016 Dec;11(4):370-6. [DOI:10.1016/j.jds.2016.04.002] [PMID] []
18. Motamedi MH, Gharedaghi J, Mehralizadeh S, Navi F, Badkoobeh A, Valaei N, Azizi T. Anthropomorphic assessment of the retromolar foramen and retromolar nerve: anomaly or variation of normal anatomy? Int J Oral Maxillofac Surg. 2016 Feb;45(2):241-4. [DOI:10.1016/j.ijom.2015.10.017] [PMID]
19. Puche-Roses M, Blasco-Serra A, Valverde-Navarro AA, Puche-Torres M. Prevalence and morphometric analysis of the retromolar canal in a Spanish population sample: a helical CT scan study. Med Oral Patol Oral Cir Bucal. 2022 Mar 1;27(2):e142-9. [DOI:10.4317/medoral.25069] [PMID] []
20. Demire O, Akbulut A. Retromolar canals and mandibular third molar position: Is there a possible connection?. Journal of the Anatomical Society of India. 2022 Jan 1;71(1):47-53. [DOI:10.4103/jasi.jasi_194_20]
21. Antic S, Markovic-Vasiljkovic B, Radivojević O, Janovic A, Bracanovic D. Can lower third molar position indicate the need for preoperative cone beam computed tomography exploration of retromolar canal? Oral Radiol. 2022 Oct;38(4):618-24. [DOI:10.1007/s11282-022-00597-z] [PMID]
22. Kawai T, Asaumi R, Sato I, Kumazawa Y, Yosue T. Observation of the retromolar foramen and canal of the mandible: a CBCT and macroscopic study. Oral Radiology. 2012 Mar;28:10-4. [DOI:10.1007/s11282-011-0074-9]
23. Shah SP, Mehta D. Mandibular Retromolar Foramen and Canal - A Systematic Review and Meta-Analysis. Ann Maxillofac Surg. 2020 Jul-Dec;10(2):444-9. [DOI:10.4103/ams.ams_19_20] [PMID] []
24. Costa E, Fortes J, Cruvinel P, Gaêta-Araujo H, Mendonça L, de Freitas B, et al. Retromolar Canal Diagnosed by Cone-Beam Computed Tomography and its Influence in Inferior Alveolar Nerve Block. Odovtos - International Journal of Dental Sciences. 2022;25:480-6. [DOI:10.15517/ijds.2022.52179]
25. Roi CI, Roi A, Nicoară A, Motofelea AC, Riviș M. Retromolar Triangle Anesthesia Technique: A Feasible Alternative to Classic?. Journal of Clinical Medicine. 2023 Sep 7;12(18):5829. [DOI:10.3390/jcm12185829] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |