


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-83-en.html


2- Post Graduate Student, Orthodontics Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran.
3- Dentist
4- MSc National Nutrition and Food Technology Research Institute, Faculty of Nutrition Sciences and Food Technology, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5- Professor, Fellow of Orthognathic Surgery, Orthodontics Dept, Member of Craniomaxillofacial Research Center, Islamic Azad University, Tehran, Iran. , info@jamilian.net
Abstract
Background and aim: The aim of the present study was to evaluate the cephalometric changes in Class II division I mandibular deficient patients treated with Farmand functional appliance.
Materials and methods: The samples of this study included twenty-seven subjects (17 girls, 10 boys) with the mean age of 11.1 (SD 1.4) years. All the subjects were treated with Farmand appliance. Paired t-test and Wilcoxon test were used to evaluate the data. P value was set at P<0.005.
Results: A skeletal Class I relationship and a marked reduction in overjet were achieved with Farmand appliance. ANB decreased significantly by 3.2 (SD 1.7) degrees and SNB increased from 74.3 (SD 1.7) degrees to 77.6 (SD 2.3) degrees. (P<0.001)
Conclusion: The results showed that Farmand appliance is effective in the treatment of mandibular deficiency in class II division 1 patients.
Introduction
A Class II malocclusion may result from a mandibular deficiency, maxillary excess or a combination of both, but the most common finding is mandibular skeletal retrusion.1,2 Approximately 15% of American children have Class II malocclusion; however, It seems that Class II problems are most prevalent in Caucasians of Northern European descent (for instance, 25% of children in Denmark are reported to be Class II).3 Different removable functional appliances such as Activator, Bionator, Fränkel-2, Herbst, R-appliance, and Twin Block have been used to treat Class II division 1 malocclusions and mandibular deficiency.4-12 Functional appliances put the mandible in forward position and result in stretches of the related attached muscular groups of the mandible, which create bone remodeling and muscular adaptation. Investigators have also proposed that class II correction observed with functional appliances was the result of a headgear effect on nasomaxillary growth.13
One functional appliance used for correction of mandibular deficiency is “Farmand Appliance”.14 This appliance has been shown to cause significant changes in the position and anterior displacement of the hyoid bone, resulting in improved airway and respiratory status of the patients.14
An electronic search in the literature shows that very few studies have evaluated the treatment effects of Farmand appliance, therefore, the aim of this study was to assess the dentoskeletal effects of Farmand appliance on the treatment of prepubertal Class II division 1 malocclusion patients with mandibular deficiency.
Materials and Methods
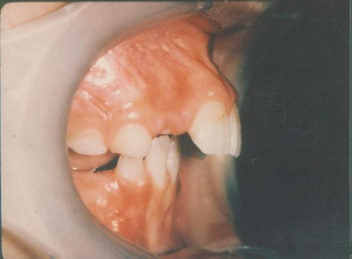
Twenty-seven subjects (17 girls, 10 boys) were selected from among the subjects treated with Farmand appliance (Figures 1 and 2). The mean age of the patients was 11.1 (SD 1.4) years. All the patients and their parents were informed of the procedures involved and they gave written consent to the study procedure. The procedures were carried out according to the criteria of the local Ethics Commission and the Helsinki Declaration.
At the beginning of treatment, all the patients were in prepubertal stage (CS1 and CS2), according to the recently improved version of cervical vertebral maturation (CVM) method described by Franchi et al15 and Baccetti et al.16
All subjects met the following inclusion criteria:
1- ANB>5°, SNB<77°, overjet>5 mm at the initial lateral cephalograms
2- No syndromic or medically compromised patients;
3- No previous surgical intervention;
4- No use of other appliances before or during the period of functional treatment.
5- A normal mandibular growth pattern; neither horizontal nor vertical growers.
6- No skeletal asymmetry
The patients were instructed to wear the appliances full-time except for eating, contact sports and tooth brushing (Figure 3). The average treatment time was 16 (SD 1.7) months. The Farmand appliance is a passive tooth borne appliance. It consists of two extended labial bows, a tongue bow, two rests (stops), and an acrylic plate. The acrylic plate extends form the occlusal surface to lingual shields. A heavy wire (1mm diameter), which acts as a tongue bow, is positioned posterior to connect the right and left acrylic parts on the palatal aspect in order to reinforce the appliance. Upper and lower labial bows are constructed of 0.7 mm stainless steel wire extended from canine to canine with horizontal loops in the canine region. The rests (stops) are placed on the mesial surface of the upper and lower first molars. The construction bites of the patients were taken with the upper and lower anterior teeth in an edge to edge occlusion with 2 to 3 mm posterior clearance.
Lateral cephalograms were taken in centric occlusion at the start (T1) and completion (T2) of functional treatment. Each film was traced by one investigator on 0.003-inch frosted acetate with a 0.3 mm lead pencil and checked by another investigator to verify the accuracy of the anatomical landmark placement. Images of bilateral structures were bisected. Measurements were taken to the nearest 0.5 mm or degrees[M1] . Disagreements were resolved by retracing the landmark or the structure to the satisfaction of both observers.
SNA, SNB, ANB, Witts (connecting points A and B perpendicular to the occlusal plane), GoGn (the distance between gonion and gnathion representing mandibular length), CoGn (distance from condyle to gnathion), Co-Pog (distance from condyle to pogonion), overjet, Jarabak index (the ratio between posterior and anterior face heights; S–Go/N–Me), GoGn-Sn (angle between SN and mandibular plane), Palatal-GoGn (angle between palatal and mandibular plane), facial angle (angle formed by the intersection of the Frankfort plane with the nasion-pogonion line), 1 to SN (angle between long axis of the upper central incisor and anterior cranial base), IMPA (angle between the long axis of the lower central incisor and mandibular plane), and interincisal angle (angle between upper and lower incisors) were measured on T1, and T2 radiographs.
The reliability of measurements was determined by randomly selecting 10 cephalograms at the beginning and at the end of the treatment. Cephalograms were re-measured by 2 other blinded investigators. The method error was calculated using Dahlberg's formula17. Values of error study ranged from 0.21 and 0.64, indicating that there was a good reliability of measurements.
The Kolmogorov-Smirnov normality test was applied to the cephalometric data. Statistical significance was set at P<0.05. The magnification factor of the cephalograms was standardized at 8 per cent. The Statistical Package for Social Sciences, Version 20 (SPSS Inc. Chicago, Illinois, USA) was used to analyze the data. Paired T-test was used for evaluation if the distribution was normal; otherwise, Wilcoxon test was used.
Results
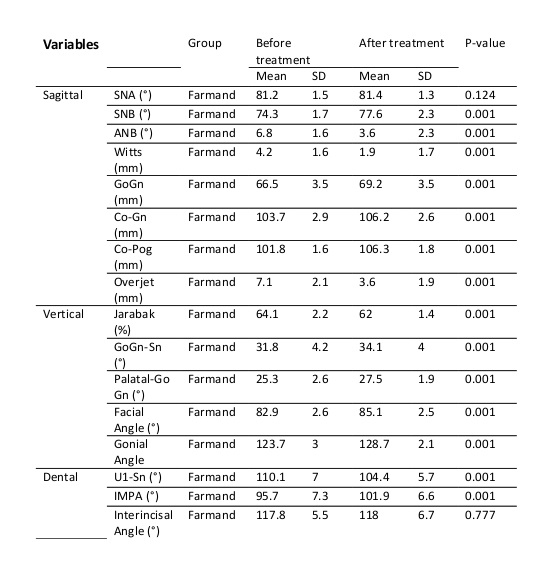
Paired T-test showed that SNA decreased from 81.2 (SD 1.5) degrees to 81.4 (SD 1.3) degrees (P<0.124), while, SNB significantly increased from 74.3 (SD 1.7) degrees to 77.6 (SD 2.3) degrees. ANB decreased by 3.2 (SD 1.7) degrees. (P<0.617) Upper 1 to SN decreased significantly from 110.1 (SD 7) degrees to 104.4 (SD 5.7) degrees; while, IMPA increased by 6.2 (SD 3.8) degrees (P<0.001). GoGn increased from 66.5 (SD 3.5) mm to 69.2 (SD 3.5) mm. (P<0.001)
Tables 1 and 2 show the pre and post treatment values of the patients. P value was set at P<0.005.
Table 2: Changes of the cephalometric data
Figure 1- Pretreatment intra oral images
Figure 2- Pretreatment intra oral images
Figure 3- Post treatment intra oral images
Figure 4- Post treatment intra oral images
Figure 5- Pretreatment cephalometric image
Figure 6- Pretreatment cephalometric image
Discussion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment of Class II Division 1 malocclusions have been abundantly reported in the literature. Treatment can include extra oral headgear, removable or fixed functional appliances, and maxillary molar distalization appliances, followed by anterior retraction. It can be camouflaged by extraction of the maxillary premolars to eliminate overjet by establishing a Class II molar relationship.18,19
The findings of this study showed that, Farmand appliance could successfully improve the intermaxillary discrepancy in Class II growing patients with mandibular deficiency. After treatment, SNB and ANB showed significant changes. The Increase of SNB and decrease of ANB are indicative of favorable changes in the mandibular growth. The increase of GoGn, Co-Gn, and Co-Pog also indicates favorable mandibular growth.
Farmand appliance is a passive tooth-borne appliance composed of one extended labial bow on each jaw, two rests (stops) on each dental arch, a tongue bow and an acrylic plate. The labial bows with a distance of 1 mm from the labial surfaces of the upper and lower anterior teeth, act as an eruptive guidance for the incisors and eliminate the perioral muscles’ forces, especially in case of severe mentalis muscle contraction. The tongue bow, with its loop in a distal direction, helps the patient to redirect his/her tongue to a distal position, thus removing the tongue pressure from the anterior part of the upper jaw. In addition, the patient is instructed to open and close his/her mandible while stabilizing the appliance on the maxillary arch by the tongue tip. This kind of exercise will improve the patient’s adaptation in the new advanced mandibular position. The rests (stops), which are placed on the mesial surfaces of the first molars, restrict first molars mesial movement and assist in achieving Class I molar relationship by forward movement of the mandible. Treatment success was defined as an improvement in molar relationship of at least a half to three-quarters cusp width depending on whether or not the leeway space was used during treatment. One of the factors that influenced treatment success in the present study was the level of co-operation of the patients which was due to the small size of Farmand appliance.
In two recent studies, Yassaei and Soroush 14 and Yassaei et al. 20 studied the effects of Farmand functional appliance on hyoid bone position in Class II division 1 malocclusion patients. They found that hyoid bone shifted significantly forward in the horizontal dimension.
Farmand functional appliance, similar to the bionator functional appliance is not as bulky as many other functional appliances and shows a better patient tolerance and does not interfere as much with their speech.
The treatment in this study was for skeletal correction and further treatment in all patients was continued with fixed orthodontics.
Conclusion
Farmand functional appliance was successful in the correction of mandibular deficiency in class II division 1 patients and can be used as an alternative functional appliance.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
