Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 4 (12-2025)
J Res Dent Maxillofac Sci 2025, 10(4): 321-329 |
Back to browse issues page

Ethics code: Pr. 142/IEC/SIBAR/2022
Clinical trials code: not applicable
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gavarraju D N, Chalasani J, A.J S S, Prathigudupu R S, Ramayanapu D. In Vitro Efficacy of Potassium Iodide and Glutathione in Masking Silver Diamine Fluoride-Induced Staining in Primary Molars. J Res Dent Maxillofac Sci 2025; 10 (4) :321-329
URL: http://jrdms.dentaliau.ac.ir/article-1-801-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-801-en.html
Deepthi Nirmal Gavarraju *1 

 , Jahnavi Chalasani2 , Sai Sankar A.J3 , Raja Satish Prathigudupu4 , Dhanush Ramayanapu2
, Jahnavi Chalasani2 , Sai Sankar A.J3 , Raja Satish Prathigudupu4 , Dhanush Ramayanapu2
, Jahnavi Chalasani2 , Sai Sankar A.J3 , Raja Satish Prathigudupu4 , Dhanush Ramayanapu2
1- Department of Pediatric and Preventive Dentistry, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India , drdeepthipedo@sids.ac.in
2- Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
3- Department of Pediatric and Preventive Dentistry, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
4- Department of Oral & Maxillofacial Surgery, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
2- Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
3- Department of Pediatric and Preventive Dentistry, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
4- Department of Oral & Maxillofacial Surgery, Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India
Full-Text [PDF 369 kb]
(177 Downloads)
| Abstract (HTML) (565 Views)
Full-Text: (261 Views)
Abstract
Background and Aim: Silver diamine fluoride (SDF) is an effective cariostatic agent used in minimally invasive dentistry. However, one major drawback of SDF is dark staining after its application, limiting its clinical use. This study quantified the color change associated with the application of SDF on extracted carious primary molars, the potential masking effects of potassium iodide (KI) and glutathione, and the effect of aging on their masking effect.
Materials and Methods: In this in vitro experimental study, 45 extracted primary carious molars with International Caries Detection Assessment System scores 5 and 6 were collected, cleaned of debris, and stored in distilled water until use. Previously restored teeth and those with pulpal involvement were excluded. The selected teeth were randomly categorized into 3 groups (n=15) for the application of SDF (group 1), SDF+ KI (group 2), and SDF+ glutathione (group 3). Test materials were applied, and images were captured immediately and on day 14. The mean gray values were calculated using Image J software and tabulated. Statistical analysis was done using paired t-test, one-way ANOVA, and Tukey’s test (alpha=0.05).
Results: KI and glutathione were able to mask the staining of SDF compared to SDF alone. SDF+ KI showed the least staining compared to other groups after a 14-day period, which was statistically significant (P<0.05).
Conclusion: Within the study limitations, KI can be considered as a potential masking agent that can overcome the black staining caused by SDF, which is the main barrier to parental acceptance of SDF treatment.
Keywords: Dental Caries; Glutathione; Potassium Iodide; Tooth, Deciduous; Silver Compounds
Introduction
Materials and Methods: In this in vitro experimental study, 45 extracted primary carious molars with International Caries Detection Assessment System scores 5 and 6 were collected, cleaned of debris, and stored in distilled water until use. Previously restored teeth and those with pulpal involvement were excluded. The selected teeth were randomly categorized into 3 groups (n=15) for the application of SDF (group 1), SDF+ KI (group 2), and SDF+ glutathione (group 3). Test materials were applied, and images were captured immediately and on day 14. The mean gray values were calculated using Image J software and tabulated. Statistical analysis was done using paired t-test, one-way ANOVA, and Tukey’s test (alpha=0.05).
Results: KI and glutathione were able to mask the staining of SDF compared to SDF alone. SDF+ KI showed the least staining compared to other groups after a 14-day period, which was statistically significant (P<0.05).
Conclusion: Within the study limitations, KI can be considered as a potential masking agent that can overcome the black staining caused by SDF, which is the main barrier to parental acceptance of SDF treatment.
Keywords: Dental Caries; Glutathione; Potassium Iodide; Tooth, Deciduous; Silver Compounds
Introduction
Early childhood caries (ECC) presents a significant public health challenge across both developing and industrialized nations. The consequences of untreated ECC extend far beyond dental discomfort, encompassing a range of adverse effects such as persistent pain, recurrent infections, impaired growth, and developmental delays. Additionally, untreated caries often leads to exorbitant treatment costs, increased school absenteeism, and diminished self-esteem in affected children [1]. Therefore, timely and appropriate prevention and management of ECC are crucial not only to alleviate this widespread burden but also to enhance the overall quality of life of children worldwide [2]. In light of the potentially severe outcomes associated with untreated caries, it is imperative to identify an effective and low-cost method of addressing caries in children. Fluoride has emerged as the most potent and reliable agent in the relatively limited arsenal of anticaries interventions. Among the various fluoride-based therapies, silver diamine fluoride (SDF) has garnered particular attention due to its dual-action mechanism, combining the potent antibacterial properties of silver with the re-mineralizing effects of fluoride. This combination makes SDF a highly effective tool in the fight against dental caries. SDF has been employed in various clinical scenarios, including management of dental caries in children, arrest of root caries in elderly patients, prevention of pit and fissure caries, inhibition of secondary caries, and desensitization of teeth affected by hypersensitivity [1]. Its widespread use is driven by several factors, particularly its simplicity in application—requiring only a "paint-on" technique—its affordability, minimal demands on personnel time and training, and its noninvasive nature [3]. These findings further highlight SDF as a valuable alternative to restorative treatments, particularly in cases where conventional interventions for primary teeth are either unavailable or not feasible. One of the primary drawbacks of SDF is the discoloration it causes on demineralized or cavitated tooth surfaces, resulting in a blackened appearance. This esthetic concern is frequently cited as the most significant barrier to its clinical use, particularly due to the reluctance of parents or caregivers to accept the color change associated with caries arrest [2,4]. The cosmetic impact often overshadows the clinical benefits of SDF, limiting its wider adoption in pediatric dentistry. As a result, there is ongoing research aimed at discovering an effective masking agent that can reduce unsightly discoloration while preserving the therapeutic properties of SDF.
Potassium iodide (KI), commonly used as a nutritional supplement, has also been introduced as a potential solution to address the staining issue associated with the application of SDF. However, its concurrent use with SDF has been shown to reduce the availability of free silver ions. This reduction may, over time, compromise the therapeutic benefits of SDF, potentially diminishing its long-term efficacy in caries arrest [5]. An alternative method proposed to minimize staining while preserving the silver content within the solution and on the tooth, surface involves the incorporation of glutathione (20%) with SDF. Glutathione has previously been employed as a biomimetic coating for silver particles, enhancing their interactions with complex biological systems and improving their water solubility [6]. Despite its promising potential, research on the efficacy of glutathione in reducing SDF-induced staining remains in its early stages, and further studies are needed to validate its effectiveness in clinical applications. Hence, the present study was envisioned to evaluate the color change associated with the application of SDF on extracted carious primary molars, the potential masking by KI and glutathione, and the effect of aging on their color masking effect. The null hypothesis of the study was that KI and glutathione would show equivalent efficacy in preventing SDF-induced staining.
Materials and Methods
Potassium iodide (KI), commonly used as a nutritional supplement, has also been introduced as a potential solution to address the staining issue associated with the application of SDF. However, its concurrent use with SDF has been shown to reduce the availability of free silver ions. This reduction may, over time, compromise the therapeutic benefits of SDF, potentially diminishing its long-term efficacy in caries arrest [5]. An alternative method proposed to minimize staining while preserving the silver content within the solution and on the tooth, surface involves the incorporation of glutathione (20%) with SDF. Glutathione has previously been employed as a biomimetic coating for silver particles, enhancing their interactions with complex biological systems and improving their water solubility [6]. Despite its promising potential, research on the efficacy of glutathione in reducing SDF-induced staining remains in its early stages, and further studies are needed to validate its effectiveness in clinical applications. Hence, the present study was envisioned to evaluate the color change associated with the application of SDF on extracted carious primary molars, the potential masking by KI and glutathione, and the effect of aging on their color masking effect. The null hypothesis of the study was that KI and glutathione would show equivalent efficacy in preventing SDF-induced staining.
Materials and Methods
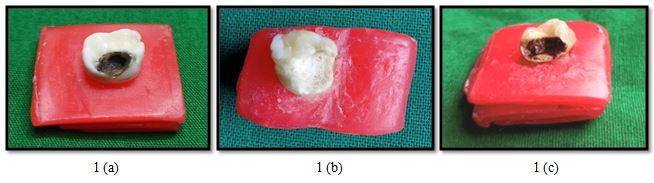
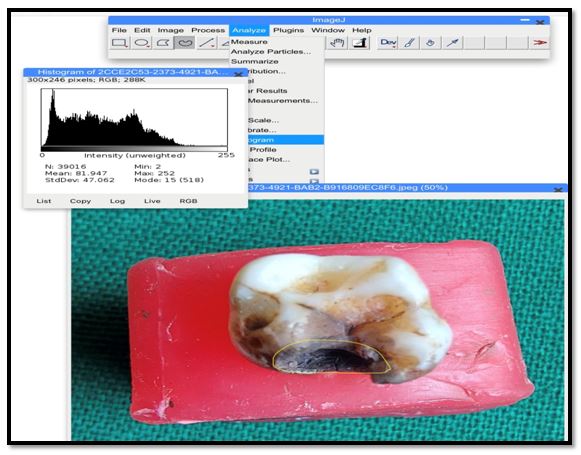
The present in vitro study (Protocol No- Pr. 142/IEC/SIBAR/2022) was conducted in the Department of Pediatric & Preventive Dentistry of a Sibar Institute of Dental Sciences, Takkellapadu, Guntur, India. after obtaining clearance from the Institutional Ethical Committee (Registration No: ECR/1362/Inst/ AP/2020). The sample size was determined as 45 using G*power 3.1.9.2 software with an effect size of 0.5, alpha error of 5%, and power of 85%. Totally, 45 human primary carious molars extracted for purposes not related to this study with the International Caries Detection Assessment System scores 5 and 6 were collected from the tooth bank of the Department of Pediatric and Preventive Dentistry and other private clinics in and around Guntur, India, cleaned of debris and stored in distilled water until use. Previously restored teeth and those with pulpal involvement were excluded. The selected teeth for the study were individually mounted to provide a base for the samples and then randomly categorized using simple randomization method, categorized into three groups (n=15): Group I: SDF (RIVASTAR; SDI, Bay waters, Australia), group II: SDF+ KI (RIVASTAR, SDI, Bay waters, Australia), and group III: SDF+ glutathione (ASESCHEM L-Glutathione Reduced, Jodhpur, Rajasthan, India). In group I, SDF was applied to carious lesions for 1 minute as per the manufacturer’s instructions. Images were captured immediately with a phase detection autofocus camera (Canon EOS 850D DSLR camera; Canon Inc., Tokyo, Japan), and baseline gray values were recorded. In group II, SDF was applied for 1 minute, and KI was applied immediately as per the manufacturer’s instructions until the precipitate was removed, and then the sample was washed thoroughly with distilled water and air dried. Subsequently, images of the treated lesions were captured, and baseline gray values were recorded [4]. For group III (SDF + glutathione), 20% glutathione was prepared by mixing 200 mg of glutathione with 1 mL of sterile water until it was completely dissolved. The prepared solution (20% glutathione) was mixed with an equal quantity of SDF until the solution became clear without any precipitates [4]. The carious surfaces were treated with the solution (20% glutathione + SDF) using a micro-brush and rinsed with copious distilled water for 30 seconds and air‑dried. The images of the treated samples were captured, and initial grey values were recorded. In all 3 groups, images were captured with the same camera under the standard conditions of afternoon light at a fixed distance from the sample immediately after the application of SDF, KI, and glutathione in the respective groups, on day 1 and after 2 weeks (Figure 1a-c). During the 2 weeks, the teeth were stored in a dry environment at room temperature. The captured images were imported individually to the ImageJ software, which is an open-source Java image processing program (Wayne Rasband and inspired by NIH Image, Bethesda, MD, USA), in which individual lesions of each tooth were selected and the mean gray values were calculated (Figure 2). As per the software, the mean gray values represent the extent of staining: 0=black, 127=gray, and 255=white. This scoring criterion suggests that the higher the mean gray value, the lower the staining. The whole procedure was conducted by a single investigator, and the scores were recorded. To avoid bias in the results, a second investigator who was unaware of the prior results randomly evaluated the samples in the software. As the inter-examiner variability was not significant, the scores given by the first investigator were only considered. The mean grey values obtained were tabulated and subjected to statistical analysis using paired t-test and one-way ANOVA with the Tukey’s post-hoc test using SPSS version 20 (SPSS Inc., IBM, Armonk, NY, USA). A P-value < 0.05 was considered statistically significant for all analyses.
Figure 1. Images captured immediately after applying the test materials. a) SDF group; b) SDF+ KI group; c) SDF+ glutathione group
Figure 2. Analysis of the captured images using ImageJ software
Results
Figure 1. Images captured immediately after applying the test materials. a) SDF group; b) SDF+ KI group; c) SDF+ glutathione group
{kind=link}
Figure 2. Analysis of the captured images using ImageJ software
{kind=link}
Results
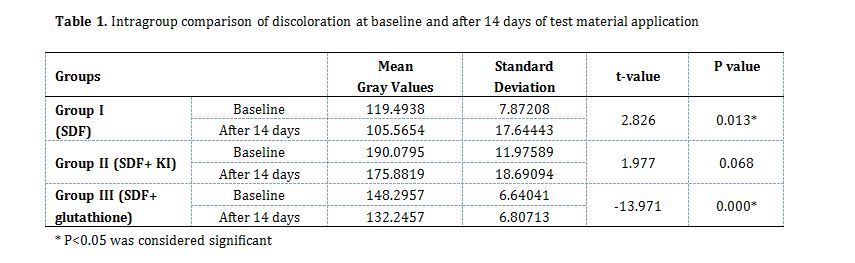
The intragroup comparison of the mean gray values, assessed at baseline and on day 14, indicated that following immediate application of the test materials, the mean gray values ranged from 119.49±7.8 to 190.079±11.97. On day 1, these values shifted to a range between 105.56±17.6 and 175.88±18.6. Group II consistently exhibited the highest mean gray values, while group I demonstrated the lowest, both on day 1 and day 14. Although a general decline in the mean gray values was observed across all groups over time, group II maintained the highest value (175.88) on day 14, suggesting minimal staining. The data also underscored the stability of the KI group's mean gray values, with no statistically significant change observed between day 1 and day 14 (P = 0.068), implying that the effect of KI was sustained throughout the observation period (Table 1).
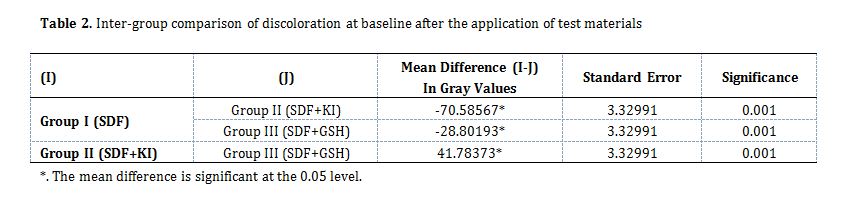
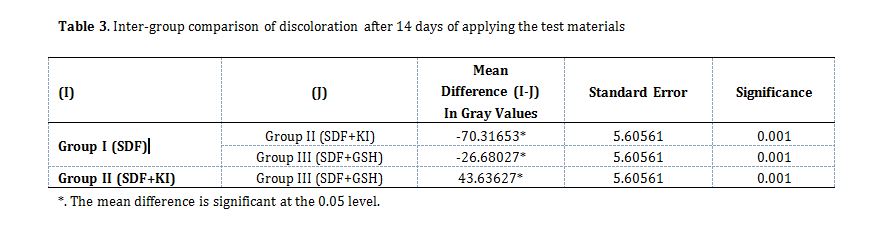
The intergroup comparison of discoloration, represented by the mean gray values, revealed a statistically significant difference among the study groups at baseline (P=0.001). The most pronounced difference in the mean gray values was observed between groups I and II, with a notable mean difference of 70.585. Conversely, the smallest mean difference, recorded between groups I and III, was 28.801 (Table 2). The intergroup comparison of the mean gray values on day 14 demonstrated that they were consistent with the observations on day 1 with a significant difference noted among all groups (P=0.001). The largest mean difference was observed between groups I and II (70.316, P=0.001), which was statistically significant, while the smallest mean difference was between groups I and III (26.68, P=0.001), which was also statistically significant. These results further emphasized the distinct variations in discoloration across the groups, with a statistically significant difference between groups I and II (P=0.001, Table 3).
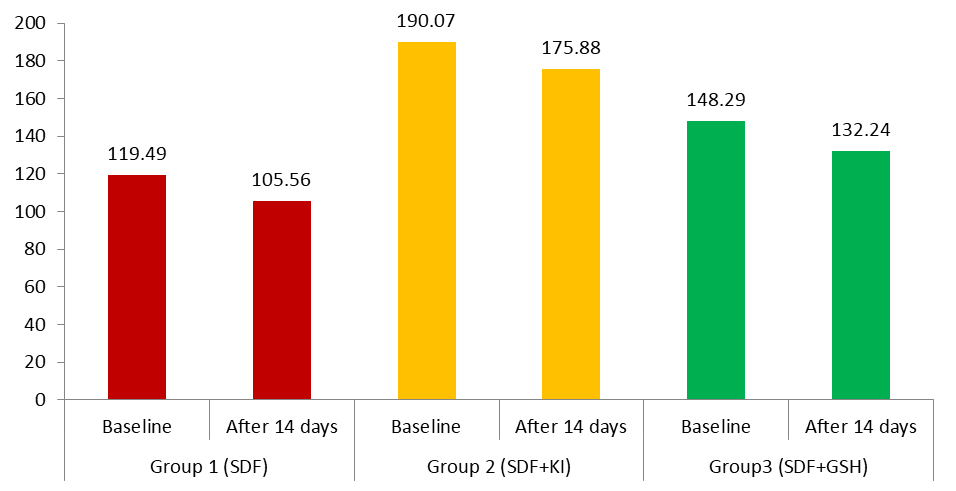
The mean gray values in different test groups at baseline and on day 14 are graphically represented in Figure 3. The differences among the groups were statistically significant both at baseline (P=0.001) and on day 14 (P=0.001), with the highest mean gray value on day 14 observed in group II (SDF + KI; 175.88), followed by group III and group I. Both masking agents reduced SDF staining to some extent compared with SDF alone, with the KI group outperforming the glutathione group in this regard.
The intergroup comparison of discoloration, represented by the mean gray values, revealed a statistically significant difference among the study groups at baseline (P=0.001). The most pronounced difference in the mean gray values was observed between groups I and II, with a notable mean difference of 70.585. Conversely, the smallest mean difference, recorded between groups I and III, was 28.801 (Table 2). The intergroup comparison of the mean gray values on day 14 demonstrated that they were consistent with the observations on day 1 with a significant difference noted among all groups (P=0.001). The largest mean difference was observed between groups I and II (70.316, P=0.001), which was statistically significant, while the smallest mean difference was between groups I and III (26.68, P=0.001), which was also statistically significant. These results further emphasized the distinct variations in discoloration across the groups, with a statistically significant difference between groups I and II (P=0.001, Table 3).
The mean gray values in different test groups at baseline and on day 14 are graphically represented in Figure 3. The differences among the groups were statistically significant both at baseline (P=0.001) and on day 14 (P=0.001), with the highest mean gray value on day 14 observed in group II (SDF + KI; 175.88), followed by group III and group I. Both masking agents reduced SDF staining to some extent compared with SDF alone, with the KI group outperforming the glutathione group in this regard.
{kind=link}
Table 1. Intragroup comparison of discoloration at baseline and after 14 days of test material application
Table 2. Inter-group comparison of discoloration at baseline after the application of test materials
Table 3. Inter-group comparison of discoloration after 14 days of applying the test materials
Discussion
{kind=link}
Table 2. Inter-group comparison of discoloration at baseline after the application of test materials
{kind=link}
Table 3. Inter-group comparison of discoloration after 14 days of applying the test materials
{kind=link}
Discussion
This in vitro study compared the efficacy of KI and glutathione in minimizing SDF-induced staining on human primary molars at two time points (day 1 and day 14). The results demonstrated that KI application following SDF treatment yielded superior esthetic outcomes, maintaining remarkable color stability throughout the observation period. Conversely, glutathione provided only a transient reduction in discoloration intensity, with gradual darkening occurring over time. The SDF alone group exhibited the most pronounced staining progression. Statistically significant differences were observed among all experimental groups at both assessment time points. Therefore, the null hypothesis that KI and glutathione would show equivalent efficacy in preventing staining was rejected due to KI’s superior and sustained performance profile.
SDF represents a significant advancement in non-invasive caries management, but its propensity for causing unsightly tooth discoloration remains a substantial barrier to its widespread clinical adoption. Glutathione, a potent antioxidant and widely used skin-whitening agent, has been proposed as a potential adjunct to SDF. In the present study, KI and glutathione were compared as adjunctive agents for mitigating staining caused by SDF on primary molars. A 38% SDF concentration was selected based on its established efficacy in arresting caries and promoting remineralization [3,7]. For KI, a 10% solution was used as the optimal concentration for reducing staining, supported by the existing evidence [8,9]. Glutathione was tested at 20% concentration, consistent with concentrations demonstrating efficacy in minimizing SDF-induced color change [6]. In this study, the specimens were stored in distilled water prior to the study, while dry specimens were used during the experimental phase to assess the absolute staining potential of SDF. This approach aimed to avoid undesirable reactions between SDF and storage media [2,10,11]. This study focused on the darkening of carious lesions over time. The gray value corresponding to L* parameter of the CIE system was selected as the standard for comparative analysis, aligning with findings in colorimetry that underscore the efficacy of grayscale measurements, particularly when paired with digital image analysis [11]. Therefore, the ImageJ software was employed in this study to ensure precise evaluation.
The mean gray values obtained in this study align with those reported by Patel et al. [11], who used time-lapse photography and ImageJ software, and Vennela et al. [2], who utilized still photography of dried samples. The biochemical basis for the results lies in the redox chemistry of silver ions. The lower mean gray value in the SDF group is attributed to the formation of black silver phosphate precipitate on the surface of carious dentin, resulting from the reaction of unreacted silver ions with partially denatured collagen. Excess silver ions precipitate as silver sulfide (Ag₂S), further contributing to staining. Within 2 weeks, the carious tooth structure darkens from initial staining to a brown-black hue, as reflected by the mean gray value dropping to 105.56 from a baseline value of 119.49, likely intensified by light exposure [2]. This photochemical degradation process involves silver ions progressively penetrating deeper into demineralized dentin through dentinal tubules, where they undergo reduction to metallic silver nanoparticles.
These nanoparticles aggregate and cause intense light scattering through surface plasmon resonance, amplifying the characteristic discoloration [12,13]. In contrast, the SDF+ KI group exhibited higher gray values, indicating reduced staining. This effect is due to the formation of a creamy white silver iodide (AgI) precipitate when KI is applied after SDF, which limits the availability of free silver ions responsible for darkening of dentin, resulting in improved color retention [4,6].
The thermodynamic stability of AgI effectively sequesters Ag⁺ ions, preventing their participation in further discoloration reactions. This inert complex adheres to hydroxyapatite as a microlayer, creating a physical barrier against oxidative darkening [14]. While the SDF+ glutathione group showed reduced staining compared to SDF alone, the intensity of discoloration gradually increased over time. This may be due to glutathione’s homeostatic properties, which regulate the release of silver ions, potentially causing a delayed increase in color intensity [15].
The glutathione’s thiol group (-SH) initially forms Ag-S coordination bonds with silver nanoparticles, but this protection is transient. The tripeptide undergoes gradual oxidation to glutathione disulfide, releasing bound Ag⁺ ions that subsequently form Ag₂S – explaining the progressive grayscale [16]. The differential performance of KI and glutathione reflects fundamental differences in their interaction kinetics. KI’s immediate precipitation reaction occurs within seconds, while glutathione’s thiol binding is a dynamic equilibrium process influenced by pH and concentration gradients [6,16]. When contextualizing these findings, the results demonstrate strong concordance with the broader literature. These findings align with studies by Vennela et al. [2], Patel et al. [11], and Zhao et al. [13], who demonstrated that KI significantly reduced SDF-induced staining of demineralized dentin. Nguyen et al. [8] reported minimal to no staining in teeth treated with SDF+KI over 4 weeks, while SDF-treated teeth showed noticeable darkening within hours. However, an in vitro study by Miller et al. [17] found no difference in staining between the SDF+ KI and control groups. This discrepancy likely stems from the use of hydrated bovine dentin in their study, a model where water content accelerates Ag⁺ diffusion and oxidation. Bovine substrates have 30% fewer dentinal tubules than human primary molars, reducing silver penetration depth and altering discoloration dynamics. Similarly, Li et al. [18] observed that KI did not significantly reduce black staining on root caries in a long-term in vivo study. Their null finding may reflect the complex pellicle-biofilm interface on root surfaces, where protein adsorption competes with AgI precipitation.
For glutathione, the literature presents greater heterogeneity. Gupte et al. [15] found that adding glutathione did not significantly impact SDF staining, contrasting with the present study, where glutathione showed a notable, albeit less pronounced, effect than KI. This divergence may originate from their lower glutathione concentration and use of artificial saliva containing chloride ions that promote AgCl formation – a compound more prone to photodegradation than Ag₂S. Contradictory results were also reported by Sayed et al. [6] and Priya et al. [4], who concluded that glutathione effectively minimized color change following SDF application. Their positive outcomes align with our day 1 data but conflict with our day 14 observations, likely because both studies terminated assessment at 72 hours, before glutathione’s protective capacity diminished. Variations in findings across different studies may be attributed to discrepancies in study design, sample type and preparation, exposure parameters (e.g., artificial saliva), follow-up duration, and methods used for analyzing the color change [19].
This in vitro study had limitations that restrict generalization of the results to the dynamic oral environment, which is influenced by factors such as brushing, saliva, presence of chromogenic and non-chromogenic bacteria, and mastication. Since dry samples were utilized to assess the mean gray values, the degree of staining in the oral environment may differ due to the presence of saliva. Additionally, potential interactions between the test materials and various restorative materials were not examined, and the impact of KI on the antimicrobial and caries-arresting properties of SDF was not addressed. Although a substantial body of literature supports the safety and efficacy of SDF as a caries-arresting agent, significant esthetic concerns limit its acceptance among adults, particularly given the contemporary emphasis on esthetic outcomes in dental care. The findings of this study advocate the use of KI following SDF treatment to mitigate staining and enhance the clinical applicability of SDF. However, further in vitro and in vivo studies with larger sample sizes and extended experimental durations are necessary to confirm these results and comprehensively investigate the potential outcomes.
Conclusion
SDF represents a significant advancement in non-invasive caries management, but its propensity for causing unsightly tooth discoloration remains a substantial barrier to its widespread clinical adoption. Glutathione, a potent antioxidant and widely used skin-whitening agent, has been proposed as a potential adjunct to SDF. In the present study, KI and glutathione were compared as adjunctive agents for mitigating staining caused by SDF on primary molars. A 38% SDF concentration was selected based on its established efficacy in arresting caries and promoting remineralization [3,7]. For KI, a 10% solution was used as the optimal concentration for reducing staining, supported by the existing evidence [8,9]. Glutathione was tested at 20% concentration, consistent with concentrations demonstrating efficacy in minimizing SDF-induced color change [6]. In this study, the specimens were stored in distilled water prior to the study, while dry specimens were used during the experimental phase to assess the absolute staining potential of SDF. This approach aimed to avoid undesirable reactions between SDF and storage media [2,10,11]. This study focused on the darkening of carious lesions over time. The gray value corresponding to L* parameter of the CIE system was selected as the standard for comparative analysis, aligning with findings in colorimetry that underscore the efficacy of grayscale measurements, particularly when paired with digital image analysis [11]. Therefore, the ImageJ software was employed in this study to ensure precise evaluation.
The mean gray values obtained in this study align with those reported by Patel et al. [11], who used time-lapse photography and ImageJ software, and Vennela et al. [2], who utilized still photography of dried samples. The biochemical basis for the results lies in the redox chemistry of silver ions. The lower mean gray value in the SDF group is attributed to the formation of black silver phosphate precipitate on the surface of carious dentin, resulting from the reaction of unreacted silver ions with partially denatured collagen. Excess silver ions precipitate as silver sulfide (Ag₂S), further contributing to staining. Within 2 weeks, the carious tooth structure darkens from initial staining to a brown-black hue, as reflected by the mean gray value dropping to 105.56 from a baseline value of 119.49, likely intensified by light exposure [2]. This photochemical degradation process involves silver ions progressively penetrating deeper into demineralized dentin through dentinal tubules, where they undergo reduction to metallic silver nanoparticles.
These nanoparticles aggregate and cause intense light scattering through surface plasmon resonance, amplifying the characteristic discoloration [12,13]. In contrast, the SDF+ KI group exhibited higher gray values, indicating reduced staining. This effect is due to the formation of a creamy white silver iodide (AgI) precipitate when KI is applied after SDF, which limits the availability of free silver ions responsible for darkening of dentin, resulting in improved color retention [4,6].
The thermodynamic stability of AgI effectively sequesters Ag⁺ ions, preventing their participation in further discoloration reactions. This inert complex adheres to hydroxyapatite as a microlayer, creating a physical barrier against oxidative darkening [14]. While the SDF+ glutathione group showed reduced staining compared to SDF alone, the intensity of discoloration gradually increased over time. This may be due to glutathione’s homeostatic properties, which regulate the release of silver ions, potentially causing a delayed increase in color intensity [15].
The glutathione’s thiol group (-SH) initially forms Ag-S coordination bonds with silver nanoparticles, but this protection is transient. The tripeptide undergoes gradual oxidation to glutathione disulfide, releasing bound Ag⁺ ions that subsequently form Ag₂S – explaining the progressive grayscale [16]. The differential performance of KI and glutathione reflects fundamental differences in their interaction kinetics. KI’s immediate precipitation reaction occurs within seconds, while glutathione’s thiol binding is a dynamic equilibrium process influenced by pH and concentration gradients [6,16]. When contextualizing these findings, the results demonstrate strong concordance with the broader literature. These findings align with studies by Vennela et al. [2], Patel et al. [11], and Zhao et al. [13], who demonstrated that KI significantly reduced SDF-induced staining of demineralized dentin. Nguyen et al. [8] reported minimal to no staining in teeth treated with SDF+KI over 4 weeks, while SDF-treated teeth showed noticeable darkening within hours. However, an in vitro study by Miller et al. [17] found no difference in staining between the SDF+ KI and control groups. This discrepancy likely stems from the use of hydrated bovine dentin in their study, a model where water content accelerates Ag⁺ diffusion and oxidation. Bovine substrates have 30% fewer dentinal tubules than human primary molars, reducing silver penetration depth and altering discoloration dynamics. Similarly, Li et al. [18] observed that KI did not significantly reduce black staining on root caries in a long-term in vivo study. Their null finding may reflect the complex pellicle-biofilm interface on root surfaces, where protein adsorption competes with AgI precipitation.
For glutathione, the literature presents greater heterogeneity. Gupte et al. [15] found that adding glutathione did not significantly impact SDF staining, contrasting with the present study, where glutathione showed a notable, albeit less pronounced, effect than KI. This divergence may originate from their lower glutathione concentration and use of artificial saliva containing chloride ions that promote AgCl formation – a compound more prone to photodegradation than Ag₂S. Contradictory results were also reported by Sayed et al. [6] and Priya et al. [4], who concluded that glutathione effectively minimized color change following SDF application. Their positive outcomes align with our day 1 data but conflict with our day 14 observations, likely because both studies terminated assessment at 72 hours, before glutathione’s protective capacity diminished. Variations in findings across different studies may be attributed to discrepancies in study design, sample type and preparation, exposure parameters (e.g., artificial saliva), follow-up duration, and methods used for analyzing the color change [19].
This in vitro study had limitations that restrict generalization of the results to the dynamic oral environment, which is influenced by factors such as brushing, saliva, presence of chromogenic and non-chromogenic bacteria, and mastication. Since dry samples were utilized to assess the mean gray values, the degree of staining in the oral environment may differ due to the presence of saliva. Additionally, potential interactions between the test materials and various restorative materials were not examined, and the impact of KI on the antimicrobial and caries-arresting properties of SDF was not addressed. Although a substantial body of literature supports the safety and efficacy of SDF as a caries-arresting agent, significant esthetic concerns limit its acceptance among adults, particularly given the contemporary emphasis on esthetic outcomes in dental care. The findings of this study advocate the use of KI following SDF treatment to mitigate staining and enhance the clinical applicability of SDF. However, further in vitro and in vivo studies with larger sample sizes and extended experimental durations are necessary to confirm these results and comprehensively investigate the potential outcomes.
Conclusion
The findings indicated that SDF alone produced marked discoloration; whereas, addition of KI significantly mitigated staining and demonstrated superior performance to glutathione. Color change increased with specimen aging, underscoring the importance of long-term evaluation. SDF+ KI offers a minimally invasive, esthetic, and effective approach for caries management, particularly in pediatric and underserved populations. Its integration into clinical protocols may enhance treatment acceptance, reduce oral health disparities, and improve overall dental outcomes.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Chaurasiya A, Gojanur S. Evaluation of the clinical efficacy of 38% silver diamine fluoride in arresting dental caries in primary teeth and its parental acceptance. J Indian Soc Pedod Prev Dent. 2021 Jan-Mar;39(1):85-9. [DOI:10.4103/jisppd.jisppd_34_21] [PMID]
2. Vennela E, Sharada J, Hasanuddin S, Suhasini K, Hemachandrika I, Singh PT. Comparison of staining potential of silver diamine fluoride versus silver diamine fluoride and potassium iodide under tooth-colored restorations: an in vitro study. J Indian Soc Pedod Prev Dent. 2021 Jan- Mar;39(1):47-52. [DOI:10.4103/jisppd.jisppd_533_20] [PMID]
3. Crystal YO, Marghalani AA, Ureles SD, Wright JT, Sulyanto R, Divaris K, et al. Use of silver diamine fluoride for dental caries management in children and adolescents, including those with special health care needs. Pediatr Dent. 2017 Sep 15;39(5):135-45.
4. Priya D, Karale R, Prashanth B, Raj A, Hegde KV. Effect of silver diamine fluoride, potassium iodide, and glutathione on micro-shear bond strength of glass ionomer cement to caries affected dentine. J Indian Soc Pedod Prev Dent. 2022 Jan-Mar;40(1):62-6. [DOI:10.4103/jisppd.jisppd_96_21] [PMID]
5. Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust Dent J. 2005 Dec;50(4):242-5. [DOI:10.1111/j.1834-7819.2005.tb00367.x] [PMID]
6. Sayed M, Matsui N, Hiraishi N, Nikaido T, Burrow MF, Tagami J. Effect of glutathione bio-molecule on tooth discoloration associated with silver diammine fluoride. Int J Mol Sci. 2018 Apr 29;19(5):1322. [DOI:10.3390/ijms19051322] [PMID] []
7. Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res. 2009 Jul;88(7):644-7. [DOI:10.1177/0022034509338671] [PMID]
8. Nguyen V, Neill C, Felsenfeld J, Primus C. Potassium iodide: the solution to silver diamine fluoride discoloration. Health. 2017;5(1):555655. [DOI:10.19080/ADOH.2017.05.555655]
9. Detsomboonrat P, Thongmak P, Lertpayab P, Aiemsri W, Sooampon S. Optimal concentration of potassium iodide to reduce the black staining of silver diamine fluoride. J Dent Sci. 2022 Jan;17(1):300-7. [DOI:10.1016/j.jds.2021.03.014] [PMID] []
10. Hamdy D, Giraki M, Abd Elaziz A, Badran A, Allam G, Ruettermann S. Laboratory evaluation of the potential masking of color changes produced by silver diamine fluoride in primary molars. BMC Oral Health. 2021Jul 9;21(1):337. [DOI:10.1186/s12903-021-01697-8] [PMID] []
11. Patel J, Anthonappa RP, King NM. Evaluation of the staining potential of silver diamine fluoride: in vitro. Int J Paediatr Dent. 2018;28(5):514-22. [DOI:10.1111/ipd.12401] [PMID]
12. Mei ML, Ito L, Cao Y, Li QL, Lo ECM, Chu CH. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J Dent. 2013 Sep;41(9):809-17. [DOI:10.1016/j.jdent.2013.06.009] [PMID]
13. Zhao IS, Chu S, Yu OY, Mei ML, Chu CH, Lo ECM. Effect of silver diamine fluoride and potassium iodide on shear bond strength of glass ionomer cements to caries-affected dentine. Int Dent J. 2019 Oct 1;69(5):341-7. [DOI:10.1111/idj.12478] [PMID] []
14. Hunwin K, Page G, Edgar M, Botana A, Armitage R, Bhogadia M, et al. Physicochemical properties, biological chemistry and mechanisms of action of caries-arresting diammine-silver(I) fluoride and silver(I)-fluoride solutions for clinical use: a critical review. Front Oral Health. 2024 Jul 23;5:1412751. [DOI:10.3389/froh.2024.1412751] [PMID] []
15. Gupte M, Saraf T, Jawdekar A, Khare S, Tiku A. A comparative analysis of staining propensity of SDF, SDF with potassium iodide and SDF with glutathione biomolecule on demineralized enamel: an in-vitro study. Int J Appl Dent Sci. 2021;7(3):297-301. [DOI:10.22271/oral.2021.v7.i3e.1314]
16. Taglietti A, Diaz Fernandez YA, Amato E, Cucca L, Dacarro G, Grisoli P, et al. Antibacterial activity of glutathione-coated silver nanoparticles against gram positive and gram negative bacteria. Langmuir. 2012 May 29;28(21):8140-8. [DOI:10.1021/la3003838] [PMID]
17. Miller MB, López LA, Quock RL. Silver diamine fluoride, potassium iodide, and esthetic perception: an in vitro pilot study. Am J Dent. 2016 Oct;29(5):248-50.
18. Li R, Lo ECM, Liu BY, Wong MCM, Chu CH. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J Dent. 2016 Aug; 51:15-20. [DOI:10.1016/j.jdent.2016.05.005] [PMID]
19. Roberts A, Bradley J, Merkley S, Pachal T, Gopal JV, Sharma D. Does potassium iodide application following silver diamine fluoride reduce staining of tooth? A systematic review. Aust Dent J. 2020 Jun;65(2):109-17. [DOI:10.1111/adj.12743] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |