Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 2 (6-2025)
J Res Dent Maxillofac Sci 2025, 10(2): 144-151 |
Back to browse issues page

Ethics code: IR.SBMU.RIDS.REC.1396.608
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Farahiparizi S, Tabari K, Torabzadeh H, Panahandeh N. Flexural Strength and Microshear Bond Strength of Conventional and Flowable Composite Resins to Dentin. J Res Dent Maxillofac Sci 2025; 10 (2) :144-151
URL: http://jrdms.dentaliau.ac.ir/article-1-774-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-774-en.html


1- Dental Research Center, Research Institute of Dental Sciences, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Dental Research Center, Research Institute of Dental Sciences, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,nargespanahandeh@yahoo.com
2- Department of Restorative Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Dental Research Center, Research Institute of Dental Sciences, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 365 kb]
(1226 Downloads)
| Abstract (HTML) (1897 Views)
Introduction
Composite resins were introduced in response to patient demands for tooth- colored restorations [1]. They require less tooth
preparation, do not have thermal and electrical conductivity, and are more esthetically pleasant than amalgam restorations [2].
The bond strength of composite to tooth structure is an important parameter in success of composite restorations. For an ideal bond strength, close contact of the substrate and adhesive is imperative. Also, the surface tension of adhesive should be lower than the free surface energy of the substrate [3]. In the etch-and-rinse systems, adhesion is based on resin penetration between the unsupported collagen fibers after smear layer removal, and subsequent formation of a hybrid layer [4]. However, in self-etch systems, optimal bond strength is achieved by etching and simultaneous penetration of acidic monomers that play a key role in resin-dentin adhesion, and do not completely dissolve the smear layer and mineral dentin components.
Dentin bonding depends on stress and tension at the resin-dentin interface and properties of the hybrid layer [5]. Several clinical methods have been proposed to achieve a high bond strength, such as incremental application of composite and increasing the contact time of dental substrate and the bonding agent; these methods improve the quality of the hybrid layer [6]. The size of specimen, type of composite, and type of test can affect the bond strength [7]. Also, lower filler content to increase flowability of composite can degrade the physical and mechanical properties of composite resins, such as their microshear bond strength (µSBS) [8].
Flexural strength (FS) is another important property of restorative materials that depends on material composition, environment, and failure mode. Structural defects in composite materials can also decrease their FS, and lead to microleakage and gap formation [9-11]. Evidence shows that nano-size filler particles can increase the FS [12]. Also, flowable composites have shown fewer voids and lower leakage than other composite types in some studies [2, 13, 14] while some others found no significant difference [2, 15]. In general, flowable composite resins have a FS lower than that of conventional composite resins by approximately 20%, mainly due to their lower filler content [16]. Thus, they should not be used in extensive cavities under heavy occlusal forces [2]. Also, lower filler content of flowable composite resins can increase their polymerization shrinkage, which increases the stress level, lowers the FS, and can eventually lead to restoration fracture [17].
The manufacturer of Clearfil AP-X Esthetics Flow (CEF), as a newly introduced flowable composite, claims that it has optimal mechanical properties for restoration of Class II cavities due to high filler content and silanization of its fillers. However, information in this regard is lacking. Thus, this study aimed to assess the FS and µSBS of Filtek Z250 and Clearfil AP-X Esthetics (CE) conventional, and CEF and Clearfil AP-X Flow (CF) flowable composite resins to dentin. The null hypothesis of this study was that no significant difference would be found in FS and µSBS of the tested conventional and flowable composite resins to dentin.
Materials and Methods
This in vitro, experimental study was conducted on 4 types of composite resins including 2 flowable composite resins, namely CEF and CF, and two conventional composite resins namely Filtek Z250 and CE (Table 1). Also, 20 extracted premolars were used for preparation of dentin discs for measurement of µSBS. The study protocol was approved by the ethics committee of the university (IR.SBMU.RIDS.REC.1396.608).
Sample size:
The sample size was calculated to be 10 in each group considering the presence of 4 independent groups using one-way ANOVA feature of PASS 11 assuming alpha=0.05, beta=0.2, study power of 80%, and mean FS of 76 MPa, 87 MPa, 55 MPa, and 88 MPa in the four groups with a standard deviation of 14 according to a previous study [18].
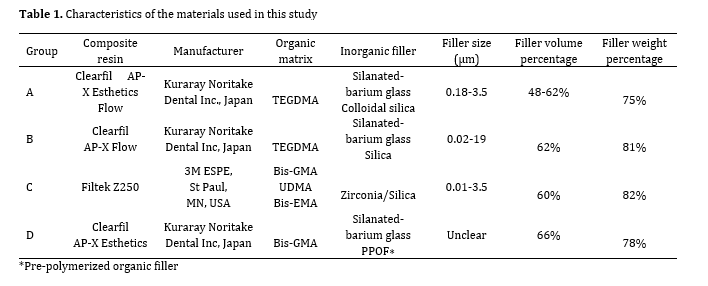
Table 1. Characteristics of the materials used in this study
Specimen fabrication for the 3-point bending test:
The 3-point bending test was performed according to ISO-4049. A two-piece stainless-steel mold measuring 2 x 2 x 25 mm was used for this purpose. The two pieces were placed next to each other and fixed with an adhesive tape. The assembly was then placed on a clean glass slab, and composite resin was applied into the mold. A transparent polyester matrix band (TDV Dental Ltd., Germany) with 0.05 mm thickness was placed over it, and gently compressed with a glass slab in order for the excess composite to leak out. Each specimen was cured from 3 directions of left, right, and middle by a light curing unit (Demetron LC, SDS Kerr, Germany) for 20 seconds per each direction (a total of 60 seconds). The tip of the curing unit was directly placed on the glass slab. The center was light-cured first and then the left and right sides. The specimens were removed from the mold and incubated in distilled water at 37°C (PECO Incubator PI-455G, Iran) for 24 hours. The dimensions of each specimen were then measured by a digital caliper (Mitutoyo, Japan). The FS of the specimens was then measured in a universal testing machine (Z020; Zwick Roell, Ulm, Germany) with three parallel rods with a circular cross-section with 2 mm diameter. Two rods were in the lower compartment with 20 mm distance from each other, and the third rod was in the upper compartment at the midpoint of the distance between the two lower rods. Load was applied at a crosshead speed of 0.5 mm/minute according to ISO-4049 and continued until specimen fracture. The load at fracture was recorded in Newtons (N), and FS in megapascals (MPs) was calculated using the following formula:
σ=3FI/2bh2
Where F is the maximum load in Newtons, b is the specimen width in millimeters, I is the distance between the two supports in millimeters, and h is the specimen height in millimeters.
Specimen preparation for µSBS test:
Twenty freshly extracted sound premolars were immersed in 0.2% thymol (Merck, Germany) solution for 48 hours for disinfection. They were then stored in saline at room temperature. The time interval between the extraction and the experiment was less than 2 months. The teeth were sectioned by a diamond disc (Bosch, Germany) to eliminate the occlusal enamel and expose the underlying dentin. The upper surface of the sections was etched with 37% phosphoric acid (Morva Etch, Morvabon, Iran), rinsed with water spray after 10 seconds, and dried with air spray. One layer of bonding agent (Tetric N-Bond; Ivoclar Vivadent, Schaan, Liechtenstein) was applied on each specimen, and air-sprayed in order for the solvent to evaporate. Light curing was then performed for 20 seconds using a light-curing unit (Demetron LC, SDS Kerr, Germany) with a light intensity of 600 mW/cm². Tygon tubes with an internal diameter of 0.7 mm and 1 mm height were filled with the respective composite, placed on dentin discs, and cured for 20 seconds. Five dentin discs were used for each composite group, and two Tygon tubes (Miami Lakes, FL, USA) were bonded to each disc (n=10 specimens for each composite type) (Figure 1). The specimens were then incubated at 37°C for 24 hours.
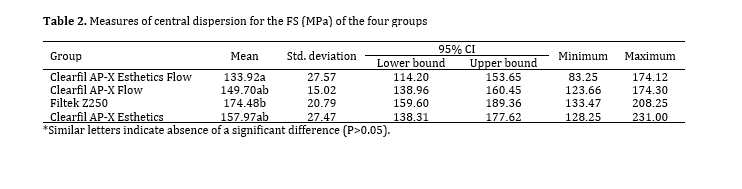
Table 2. Measures of central dispersion for the FS (MPa) of the four groups
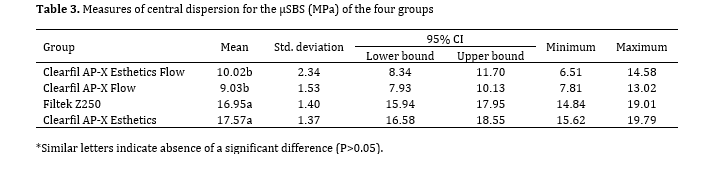
Table 3. Measures of central dispersion for the µSBS (MPa) of the four groups
Discussion
This study assessed the FS and µSBS of four conventional and flowable composite resins to dentin. The results showed that Z250 had a significantly higher FS than CEF. Also, the conventional composites had a significantly higher µSBS than the flowable composites. Thus, the null hypothesis of the study was rejected.
The manufacturer of CEF claims that it has excellent mechanical and physical properties and may be reliably used for restoration of Class I and II cavities. All tested composites in this study except for Z250 have silanated fillers. The results regarding FS showed that the mean FS of all tested composites was higher than the minimum required threshold of 80 MPa according to ISO-4049 [19]. The FS of Z250 was significantly higher than that of CEF but no other significant differences were found. High FS protects the restoration against fracture and preserves the tooth structure as such [20]. Previous studies attributed the lower mechanical and physical properties of flowable composites compared with conventional composites to their lower filler content [17, 21, 22]. However, in the present study, the filler volume of both tested flowable composites was comparable to the filler volume of the tested conventional composites. Thus, this difference may be attributed to different types and composition of monomers used in Z250 and CEF. Z250 has a combination of bis-GMA, UDMA copolymer, and TEGDMA and bis-EMA co-monomers while CEF only contains TEGDMA. Since CEF is a flowable composite with high filler volume, it requires a low molecular weight monomer in order not to increase its viscosity and also in order to allow a high filler content [23]. TEGDMA has a lower molecular weight than bis-GMa and is therefore used as a diluting agent to lower the viscosity of composite resins and allow for incorporation of a higher filler content [23-26]. However, it lowers the mechanical properties such as FS of composite resins due to its lower molecular weight and higher number of double bonds [26, 27]. It has been reported that composite resins with a combination of bis-GMA, UDMA, and TEGDMA monomers have superior physical and mechanical properties compared to those that only contain TEGDMA [28].
CEF, CF, and CE all have silanated fillers. However, no information is available regarding the silanization process of their fillers. In general, information about the effect of silanization on composite properties is controversial. Some studies showed that silanization of fillers increased their adhesion to the matrix and resulted in more homogenous dispersion of fillers in the matrix, leading to improvement of physical and mechanical properties such as FS compared with composites devoid of silanated fillers [29-31]. However, Beatty et al. [32] demonstrated that addition of silane to filler surface had no significant effect on physicomechanical properties. Also, it has been stated that silane can decrease homogenous dispersion of fillers due to formation of non-homogenous granules [33]. Since the three tested composites with silanated fillers had no significant difference in FS, it may be stated that silanization of fillers in flowable composites can improve their FS to the level of a silanated conventional composite; however, information is not sufficient for comparison with a non-silanated conventional composite (i.e., Z250), and further investigations are required in this regard.
Assessment of µSBS in the present study revealed no significant difference in µSBS of the two flowable and the two conventional composite resins. However, the two conventional composite resins showed a significantly higher µSBS than the two flowable composite resins. Both flowable composites tested in the present study are highly filled as stated by the manufacturer. Highly-filled flowable composites reportedly have a lower polymerization shrinkage and lower stress at the interface, and therefore, yield higher bond strength. However, studies found no significant difference in bond strength of highly-filled and normally-filled flowable composites [34, 35]. Also, the present study showed lower µSBS of flowable composites than conventional composites. The same results were reported by Sagsoz et al. [35] who showed that higher filler content of flowable composites did not cause a higher bond strength to dentin compared with the conventional and bulk-fill composite resins. On the other hand, it has been widely reported that stresses due to polymerization shrinkage and their concentration at the composite-tooth interface are responsible for debonding [8, 35, 36]. This shrinkage mainly depends on monomer composition, type and volume of fillers, and the initiation mechanism of polymerization reaction [36]. As mentioned earlier, flowable composites tested in the present study contain TEGDMA, which increases the degree of conversion and subsequently the polymerization shrinkage [26, 37]. Also, according to Alonso et al, [38] TEGDMA causes greater stress in composite resins due to the presence of aliphatic group in its structure [38, 39]. Thus, the presence of TEGDMA in flowable composites evaluated in the present study may explain their lower µSBS than that of conventional composites.
In vitro design and no simulation of the clinical setting by aging were the main limitations of this study, which should be addressed in future studies.
Conclusion
According to the results of this study, the FS of CEF was significantly lower than that of Z250, and comparable to that of other tested composite resins. All tested composites had a FS higher than 80 MPa recommended by ISO-4049 for restorations under occlusal forces. Both CEF and CF showed significantly lower µSBS than the tested conventional composite resins.
Full-Text: (463 Views)
Abstract
Background and Aim: This study aimed to evaluate the flexural strength (FS) and microshear bond strength (µSBS) of conventional and flowable composite resins to dentin.
Materials and Methods: This in vitro study was conducted on composite specimens fabricated from Filtek Z250 and Clearfil AP-X Esthetics (CE) conventional, and Clearfil AP-X Esthetics Flow (CEF) and Clearfil AP-X Flow (CF) flowable composite resins in 4 groups (n=10). The specimens underwent a 3-point bending test for measurement of their FS. For assessment of µSBS, dentin discs with 2 mm thickness were obtained from the coronal third of the crowns of 20 extracted premolars. Composite resins were bonded to dentin discs in Tygon tubes (1 mm height, 0.7 mm internal diameter) using Tetric N-Bond 5th generation bonding agent, and a universal testing machine measured their µSBS. Data were analyzed by ANOVA and Tukey test (alpha=0.05).
Results: Z250 showed a significantly higher FS than CEF (P=0.002); no other significant difference was found in FS. The two conventional composites (P=0.847) and the two flowable composites (P=0.575) had no significant difference with each other in µSBS. However, the conventional composites had a significantly higher µSBS than the flowable composites (P<0.001).
Conclusion: The FS of CEF was significantly lower than that of Z250, and comparable to that of other tested composite resins. All tested composites had a FS higher than 80 MPa recommended by ISO-4049 for restorations under occlusal forces. Both CEF and CF showed significantly lower µSBS than the tested conventional composite resins.
Keywords: Composite Resins; Dental Bonding; Flexural Strength
Background and Aim: This study aimed to evaluate the flexural strength (FS) and microshear bond strength (µSBS) of conventional and flowable composite resins to dentin.
Materials and Methods: This in vitro study was conducted on composite specimens fabricated from Filtek Z250 and Clearfil AP-X Esthetics (CE) conventional, and Clearfil AP-X Esthetics Flow (CEF) and Clearfil AP-X Flow (CF) flowable composite resins in 4 groups (n=10). The specimens underwent a 3-point bending test for measurement of their FS. For assessment of µSBS, dentin discs with 2 mm thickness were obtained from the coronal third of the crowns of 20 extracted premolars. Composite resins were bonded to dentin discs in Tygon tubes (1 mm height, 0.7 mm internal diameter) using Tetric N-Bond 5th generation bonding agent, and a universal testing machine measured their µSBS. Data were analyzed by ANOVA and Tukey test (alpha=0.05).
Results: Z250 showed a significantly higher FS than CEF (P=0.002); no other significant difference was found in FS. The two conventional composites (P=0.847) and the two flowable composites (P=0.575) had no significant difference with each other in µSBS. However, the conventional composites had a significantly higher µSBS than the flowable composites (P<0.001).
Conclusion: The FS of CEF was significantly lower than that of Z250, and comparable to that of other tested composite resins. All tested composites had a FS higher than 80 MPa recommended by ISO-4049 for restorations under occlusal forces. Both CEF and CF showed significantly lower µSBS than the tested conventional composite resins.
Keywords: Composite Resins; Dental Bonding; Flexural Strength
Introduction
Composite resins were introduced in response to patient demands for tooth- colored restorations [1]. They require less tooth
preparation, do not have thermal and electrical conductivity, and are more esthetically pleasant than amalgam restorations [2].
The bond strength of composite to tooth structure is an important parameter in success of composite restorations. For an ideal bond strength, close contact of the substrate and adhesive is imperative. Also, the surface tension of adhesive should be lower than the free surface energy of the substrate [3]. In the etch-and-rinse systems, adhesion is based on resin penetration between the unsupported collagen fibers after smear layer removal, and subsequent formation of a hybrid layer [4]. However, in self-etch systems, optimal bond strength is achieved by etching and simultaneous penetration of acidic monomers that play a key role in resin-dentin adhesion, and do not completely dissolve the smear layer and mineral dentin components.
Dentin bonding depends on stress and tension at the resin-dentin interface and properties of the hybrid layer [5]. Several clinical methods have been proposed to achieve a high bond strength, such as incremental application of composite and increasing the contact time of dental substrate and the bonding agent; these methods improve the quality of the hybrid layer [6]. The size of specimen, type of composite, and type of test can affect the bond strength [7]. Also, lower filler content to increase flowability of composite can degrade the physical and mechanical properties of composite resins, such as their microshear bond strength (µSBS) [8].
Flexural strength (FS) is another important property of restorative materials that depends on material composition, environment, and failure mode. Structural defects in composite materials can also decrease their FS, and lead to microleakage and gap formation [9-11]. Evidence shows that nano-size filler particles can increase the FS [12]. Also, flowable composites have shown fewer voids and lower leakage than other composite types in some studies [2, 13, 14] while some others found no significant difference [2, 15]. In general, flowable composite resins have a FS lower than that of conventional composite resins by approximately 20%, mainly due to their lower filler content [16]. Thus, they should not be used in extensive cavities under heavy occlusal forces [2]. Also, lower filler content of flowable composite resins can increase their polymerization shrinkage, which increases the stress level, lowers the FS, and can eventually lead to restoration fracture [17].
The manufacturer of Clearfil AP-X Esthetics Flow (CEF), as a newly introduced flowable composite, claims that it has optimal mechanical properties for restoration of Class II cavities due to high filler content and silanization of its fillers. However, information in this regard is lacking. Thus, this study aimed to assess the FS and µSBS of Filtek Z250 and Clearfil AP-X Esthetics (CE) conventional, and CEF and Clearfil AP-X Flow (CF) flowable composite resins to dentin. The null hypothesis of this study was that no significant difference would be found in FS and µSBS of the tested conventional and flowable composite resins to dentin.
Materials and Methods
This in vitro, experimental study was conducted on 4 types of composite resins including 2 flowable composite resins, namely CEF and CF, and two conventional composite resins namely Filtek Z250 and CE (Table 1). Also, 20 extracted premolars were used for preparation of dentin discs for measurement of µSBS. The study protocol was approved by the ethics committee of the university (IR.SBMU.RIDS.REC.1396.608).
Sample size:
The sample size was calculated to be 10 in each group considering the presence of 4 independent groups using one-way ANOVA feature of PASS 11 assuming alpha=0.05, beta=0.2, study power of 80%, and mean FS of 76 MPa, 87 MPa, 55 MPa, and 88 MPa in the four groups with a standard deviation of 14 according to a previous study [18].
Table 1. Characteristics of the materials used in this study
{kind=link}
Specimen fabrication for the 3-point bending test:
The 3-point bending test was performed according to ISO-4049. A two-piece stainless-steel mold measuring 2 x 2 x 25 mm was used for this purpose. The two pieces were placed next to each other and fixed with an adhesive tape. The assembly was then placed on a clean glass slab, and composite resin was applied into the mold. A transparent polyester matrix band (TDV Dental Ltd., Germany) with 0.05 mm thickness was placed over it, and gently compressed with a glass slab in order for the excess composite to leak out. Each specimen was cured from 3 directions of left, right, and middle by a light curing unit (Demetron LC, SDS Kerr, Germany) for 20 seconds per each direction (a total of 60 seconds). The tip of the curing unit was directly placed on the glass slab. The center was light-cured first and then the left and right sides. The specimens were removed from the mold and incubated in distilled water at 37°C (PECO Incubator PI-455G, Iran) for 24 hours. The dimensions of each specimen were then measured by a digital caliper (Mitutoyo, Japan). The FS of the specimens was then measured in a universal testing machine (Z020; Zwick Roell, Ulm, Germany) with three parallel rods with a circular cross-section with 2 mm diameter. Two rods were in the lower compartment with 20 mm distance from each other, and the third rod was in the upper compartment at the midpoint of the distance between the two lower rods. Load was applied at a crosshead speed of 0.5 mm/minute according to ISO-4049 and continued until specimen fracture. The load at fracture was recorded in Newtons (N), and FS in megapascals (MPs) was calculated using the following formula:
σ=3FI/2bh2
Where F is the maximum load in Newtons, b is the specimen width in millimeters, I is the distance between the two supports in millimeters, and h is the specimen height in millimeters.
Specimen preparation for µSBS test:
Twenty freshly extracted sound premolars were immersed in 0.2% thymol (Merck, Germany) solution for 48 hours for disinfection. They were then stored in saline at room temperature. The time interval between the extraction and the experiment was less than 2 months. The teeth were sectioned by a diamond disc (Bosch, Germany) to eliminate the occlusal enamel and expose the underlying dentin. The upper surface of the sections was etched with 37% phosphoric acid (Morva Etch, Morvabon, Iran), rinsed with water spray after 10 seconds, and dried with air spray. One layer of bonding agent (Tetric N-Bond; Ivoclar Vivadent, Schaan, Liechtenstein) was applied on each specimen, and air-sprayed in order for the solvent to evaporate. Light curing was then performed for 20 seconds using a light-curing unit (Demetron LC, SDS Kerr, Germany) with a light intensity of 600 mW/cm². Tygon tubes with an internal diameter of 0.7 mm and 1 mm height were filled with the respective composite, placed on dentin discs, and cured for 20 seconds. Five dentin discs were used for each composite group, and two Tygon tubes (Miami Lakes, FL, USA) were bonded to each disc (n=10 specimens for each composite type) (Figure 1). The specimens were then incubated at 37°C for 24 hours.
Figure 1. Composite cylinders bonded to dentin disc for measurement of µSBS
After 24 hours, the Tygon tubes were cut by a scalpel. The specimens were fixed to the jig of a microtensile tester (Quantrol by Dillon, USA) by cyanoacrylate glue (Jalafix 123, Jalasanj Company, Iran). A wire was tied around the cylinder, and load was applied until debonding. The load causing debonding was recorded in Newtons (N). The following formula was used for its conversion to megapascals (MPa):
µSBS (MPa)=N/mm2
The diameter of all specimens was 0.7 mm. Thus, the surface area of all specimens was calculated to be 0.384 mm2.
Statistical analysis:
Normal distribution of data was ensured by the Kolmogorov-Smirnov test, while equality of the variances was confirmed by the Levene test. Thus, FS and µSBS of the four groups were compared by one-way ANOVA, followed by pairwise comparisons with the Tukey test. All statistical analyses were performed using SPSS version 20 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
FS:
Table 2 presents the measures of central dispersion for the FS of the four groups. Filtek Z250 showed the highest, and CEF showed the lowest mean FS. The four groups had a significant difference in FS (P=0.004). Pairwise comparisons showed that the FS of Z250 was significantly higher than that of CEF (P=0.002). No other significant differences were found (P>0.05).
µSBS:
Table 3 presents the measures of central dispersion for the µSBS of the four groups. The four groups had a significant difference in µSBS (P<0.001). Pairwise comparisons showed no significant difference in µSBS of the two flowable (P=0.575), and the two conventional (P=0.847) composite resins. However, the two conventional composite resins showed a significantly higher µSBS than the two flowable composite resins (P<0.001).
{kind=link}
After 24 hours, the Tygon tubes were cut by a scalpel. The specimens were fixed to the jig of a microtensile tester (Quantrol by Dillon, USA) by cyanoacrylate glue (Jalafix 123, Jalasanj Company, Iran). A wire was tied around the cylinder, and load was applied until debonding. The load causing debonding was recorded in Newtons (N). The following formula was used for its conversion to megapascals (MPa):
µSBS (MPa)=N/mm2
The diameter of all specimens was 0.7 mm. Thus, the surface area of all specimens was calculated to be 0.384 mm2.
Statistical analysis:
Normal distribution of data was ensured by the Kolmogorov-Smirnov test, while equality of the variances was confirmed by the Levene test. Thus, FS and µSBS of the four groups were compared by one-way ANOVA, followed by pairwise comparisons with the Tukey test. All statistical analyses were performed using SPSS version 20 (SPSS Inc., IL, USA) at 0.05 level of significance.
Results
FS:
Table 2 presents the measures of central dispersion for the FS of the four groups. Filtek Z250 showed the highest, and CEF showed the lowest mean FS. The four groups had a significant difference in FS (P=0.004). Pairwise comparisons showed that the FS of Z250 was significantly higher than that of CEF (P=0.002). No other significant differences were found (P>0.05).
µSBS:
Table 3 presents the measures of central dispersion for the µSBS of the four groups. The four groups had a significant difference in µSBS (P<0.001). Pairwise comparisons showed no significant difference in µSBS of the two flowable (P=0.575), and the two conventional (P=0.847) composite resins. However, the two conventional composite resins showed a significantly higher µSBS than the two flowable composite resins (P<0.001).
Table 2. Measures of central dispersion for the FS (MPa) of the four groups
{kind=link}
Table 3. Measures of central dispersion for the µSBS (MPa) of the four groups
{kind=link}
Discussion
This study assessed the FS and µSBS of four conventional and flowable composite resins to dentin. The results showed that Z250 had a significantly higher FS than CEF. Also, the conventional composites had a significantly higher µSBS than the flowable composites. Thus, the null hypothesis of the study was rejected.
The manufacturer of CEF claims that it has excellent mechanical and physical properties and may be reliably used for restoration of Class I and II cavities. All tested composites in this study except for Z250 have silanated fillers. The results regarding FS showed that the mean FS of all tested composites was higher than the minimum required threshold of 80 MPa according to ISO-4049 [19]. The FS of Z250 was significantly higher than that of CEF but no other significant differences were found. High FS protects the restoration against fracture and preserves the tooth structure as such [20]. Previous studies attributed the lower mechanical and physical properties of flowable composites compared with conventional composites to their lower filler content [17, 21, 22]. However, in the present study, the filler volume of both tested flowable composites was comparable to the filler volume of the tested conventional composites. Thus, this difference may be attributed to different types and composition of monomers used in Z250 and CEF. Z250 has a combination of bis-GMA, UDMA copolymer, and TEGDMA and bis-EMA co-monomers while CEF only contains TEGDMA. Since CEF is a flowable composite with high filler volume, it requires a low molecular weight monomer in order not to increase its viscosity and also in order to allow a high filler content [23]. TEGDMA has a lower molecular weight than bis-GMa and is therefore used as a diluting agent to lower the viscosity of composite resins and allow for incorporation of a higher filler content [23-26]. However, it lowers the mechanical properties such as FS of composite resins due to its lower molecular weight and higher number of double bonds [26, 27]. It has been reported that composite resins with a combination of bis-GMA, UDMA, and TEGDMA monomers have superior physical and mechanical properties compared to those that only contain TEGDMA [28].
CEF, CF, and CE all have silanated fillers. However, no information is available regarding the silanization process of their fillers. In general, information about the effect of silanization on composite properties is controversial. Some studies showed that silanization of fillers increased their adhesion to the matrix and resulted in more homogenous dispersion of fillers in the matrix, leading to improvement of physical and mechanical properties such as FS compared with composites devoid of silanated fillers [29-31]. However, Beatty et al. [32] demonstrated that addition of silane to filler surface had no significant effect on physicomechanical properties. Also, it has been stated that silane can decrease homogenous dispersion of fillers due to formation of non-homogenous granules [33]. Since the three tested composites with silanated fillers had no significant difference in FS, it may be stated that silanization of fillers in flowable composites can improve their FS to the level of a silanated conventional composite; however, information is not sufficient for comparison with a non-silanated conventional composite (i.e., Z250), and further investigations are required in this regard.
Assessment of µSBS in the present study revealed no significant difference in µSBS of the two flowable and the two conventional composite resins. However, the two conventional composite resins showed a significantly higher µSBS than the two flowable composite resins. Both flowable composites tested in the present study are highly filled as stated by the manufacturer. Highly-filled flowable composites reportedly have a lower polymerization shrinkage and lower stress at the interface, and therefore, yield higher bond strength. However, studies found no significant difference in bond strength of highly-filled and normally-filled flowable composites [34, 35]. Also, the present study showed lower µSBS of flowable composites than conventional composites. The same results were reported by Sagsoz et al. [35] who showed that higher filler content of flowable composites did not cause a higher bond strength to dentin compared with the conventional and bulk-fill composite resins. On the other hand, it has been widely reported that stresses due to polymerization shrinkage and their concentration at the composite-tooth interface are responsible for debonding [8, 35, 36]. This shrinkage mainly depends on monomer composition, type and volume of fillers, and the initiation mechanism of polymerization reaction [36]. As mentioned earlier, flowable composites tested in the present study contain TEGDMA, which increases the degree of conversion and subsequently the polymerization shrinkage [26, 37]. Also, according to Alonso et al, [38] TEGDMA causes greater stress in composite resins due to the presence of aliphatic group in its structure [38, 39]. Thus, the presence of TEGDMA in flowable composites evaluated in the present study may explain their lower µSBS than that of conventional composites.
In vitro design and no simulation of the clinical setting by aging were the main limitations of this study, which should be addressed in future studies.
Conclusion
According to the results of this study, the FS of CEF was significantly lower than that of Z250, and comparable to that of other tested composite resins. All tested composites had a FS higher than 80 MPa recommended by ISO-4049 for restorations under occlusal forces. Both CEF and CF showed significantly lower µSBS than the tested conventional composite resins.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Yap AU, Yap SH, Teo CK, Ng JJ. Finishing/polishing of composite and compomer restoratives: effectiveness of one-step systems. Oper Dent. 2004 May-Jun;29(3):275-9.
2. Attar N, Tam LE, McComb D. Flow, strength, stiffness and radiopacity of flowable resin composites. J Can Dent Assoc. 2003 Sep;69(8):516-21.
3. Dubernard C, Raynal P, Tramini P. Comparative study of enamel adhesion between RelyX™ Unicem® (3M), a self-adhesive bonding agent, and the combination of MIP® (3M), a hydrophilic adhesive, and Transbond Supreme Low Viscosity® (3M), a traditional hydrophobic adhesive. Int Orthod. 2013 Sep;11(3):247-61. [DOI:10.1016/j.ortho.2013.06.009] [PMID]
4. Pinzon LM, Watanabe LG, Reis AF, Powers JM, Marshall SJ, Marshall GW. Analysis of interfacial structure and bond strength of self-etch adhesives. Am J Dent. 2013 Dec;26(6):335-40.
5. Klein-Júnior CA, Zander-Grande C, Amaral R, Stanislawczuk R, Garcia EJ, Baumhardt-Neto R, et al. Evaporating solvents with a warm air-stream: effects on adhesive layer properties and resin-dentin bond strengths. J Dent. 2008 Aug;36(8):618-25. [DOI:10.1016/j.jdent.2008.04.014] [PMID]
6. Reis A, Klein-Júnior CA, Accorinte Mde L, Grande RH, dos Santos CB, Loguercio AD. Effects of adhesive temperature on the early and 6-month dentin bonding. J Dent. 2009 Oct;37(10): 791-8. [DOI:10.1016/j.jdent.2009.06.007] [PMID]
7. Phrukkanon S, Burrow MF, Tyas MJ. The influence of cross-sectional shape and surface area on the microtensile bond test. Dent Mater. 1998 Jun;14(3):212-21. [DOI:10.1016/S0109-5641(98)00034-7] [PMID]
8. Andrade AM, Moura SK, Reis A, Loguercio AD, Garcia EJ, Grande RH. Evaluating resin-enamel bonds by microshear and microtensile bond strength tests: effects of composite resin. J Appl Oral Sci. 2010 Dec;18(6):591-8. [DOI:10.1590/S1678-77572010000600010] [PMID] []
9. Della Bona A. Characterizing ceramics and the interfacial adhesion to resin: I - The relationship of microstructure, composition, properties and fractography. J Appl Oral Sci. 2005 Mar;13(1):1-9. [DOI:10.1590/S1678-77572005000100002] [PMID]
10. Rodrigues SA, Jr., Ferracane JL, Della Bona A. Flexural strength and Weibull analysis of a microhybrid and a nanofill composite evaluated by 3- and 4-point bending tests. Dent Mater. 2008 Mar;24(3):426-31. [DOI:10.1016/j.dental.2007.05.013] [PMID]
11. Zeng K, Odén A, Rowcliffe D. Flexure tests on dental ceramics. Int J Prosthodont. 1996 Sep-Oct;9(5):434-9.
12. Musanje L, Ferracane JL. Effects of resin formulation and nanofiller surface treatment on the properties of experimental hybrid resin composite. Biomaterials. 2004 Aug;25(18): 4065-71. [DOI:10.1016/j.biomaterials.2003.11.003] [PMID]
13. Ferdianakis K. Microleakage reduction from newer esthetic restorative materials in permanent molars. J Clin Pediatr Dent. 1998 Spring;22(3):221-9.
14. Payne JHt. The marginal seal of Class II restorations: flowable composite resin compared to injectable glass ionomer. J Clin Pediatr Dent. 1999 Winter;23(2):123-30.
15. Boruziniat A, Gharaee S, Sarraf Shirazi A, Majidinia S, Vatanpour M. Evaluation of the efficacy of flowable composite as lining material on microleakage of composite resin restorations: A systematic review and meta-analysis. Quintessence Int. 2016 Feb;47(2):93-101.
16. Lazarchik DA, Hammond BD, Sikes CL, Looney SW, Rueggeberg FA. Hardness comparison of bulk-filled/transtooth and incremental-filled/occlusally irradiated composite resins. J Prosthet Dent. 2007 Aug;98(2):129-40. [DOI:10.1016/S0022-3913(07)60046-8] [PMID]
17. Bayne SC, Thompson JY, Swift EJ, Jr., Stamatiades P, Wilkerson M. A characterization of first-generation flowable composites. J Am Dent Assoc. 1998 May;129(5):567-77. [DOI:10.14219/jada.archive.1998.0274] [PMID]
18. Irie M, Tjandrawinata R, E L, Yamashiro T, Kazuomi S. Flexural performance of flowable versus conventional light-cured composite resins in a long-term in vitro study. Dent Mater J. 2008 Mar;27(2):300-9. [DOI:10.4012/dmj.27.300] [PMID]
19. Standardization IOf. Dentistry-Polymer-based Restorative Materials, ISO, 2019.
20. Goracci C, Cadenaro M, Fontanive L, Giangrosso G, Juloski J, Vichi A, et al. Polymerization efficiency and flexural strength of low-stress restorative composites. Dent Mater. 2014 Jun;30(6):688-94. [DOI:10.1016/j.dental.2014.03.006] [PMID]
21. Chung SM, Yap AU, Chandra SP, Lim CT. Flexural strength of dental composite restoratives: comparison of biaxial and three-point bending test. J Biomed Mater Res B Appl Biomater. 2004 Nov 15;71(2):278-83. [DOI:10.1002/jbm.b.30103] [PMID]
22. Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent. 2008 Jul-Aug;33(4):408-12. [DOI:10.2341/07-104] [PMID]
23. Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties and wear behavior of light-cured packable composite resins. Dent Mater. 2000 Jan;16(1):33-40. [DOI:10.1016/S0109-5641(99)00082-2] [PMID]
24. Moszner N, Salz U. New developments of polymeric dental composites. Progress in polymer science. 2001;26(4):535-76. [DOI:10.1016/S0079-6700(01)00005-3]
25. Atai M, Watts DC. A new kinetic model for the photopolymerization shrinkage-strain of dental composites and resin-monomers. Dent Mater. 2006 Aug;22(8):785-91. [DOI:10.1016/j.dental.2006.02.009] [PMID]
26. Floyd CJ, Dickens SH. Network structure of Bis-GMA- and UDMA-based resin systems. Dent Mater. 2006 Dec;22(12): 1143-9. [DOI:10.1016/j.dental.2005.10.009] [PMID]
27. Lemon MT, Jones MS, Stansbury JW. Hydrogen bonding interactions in methacrylate monomers and polymers. J Biomed Mater Res A. 2007 Dec 1;83(3):734-46. [DOI:10.1002/jbm.a.31448] [PMID]
28. Barszczewska-Rybarek I, Jurczyk S. Comparative Study of Structure-Property Relationships in Polymer Networks Based on Bis-GMA, TEGDMA and Various Urethane-Dimethacrylates. Materials (Basel). 2015 Mar 19;8(3):1230-48. [DOI:10.3390/ma8031230] [PMID] []
29. Mair LH, Stolarski TA, Vowles RW, Lloyd CH. Wear: mechanisms, manifestations and measurement. Report of a workshop. J Dent. 1996 Jan-Mar;24(1-2):141-8. [DOI:10.1016/0300-5712(95)00043-7] [PMID]
30. Aydınoğlu A, Yoruç ABH. Effects of silane-modified fillers on properties of dental composite resin. Mater Sci Eng C Mater Biol Appl. 2017 Oct 1;79:382-9. [DOI:10.1016/j.msec.2017.04.151] [PMID]
31. Venhoven BA, de Gee AJ, Werner A, Davidson CL. Influence of filler parameters on the mechanical coherence of dental restorative resin composites. Biomaterials. 1996 Apr;17(7): 735-40. [DOI:10.1016/0142-9612(96)86744-5] [PMID]
32. Beatty MW, Swartz ML, Moore BK, Phillips RW, Roberts TA. Effect of microfiller fraction and silane treatment on resin composite properties. J Biomed Mater Res. 1998 Apr; 40(1):12-23.
https://doi.org/10.1002/(SICI)1097-4636(199804)40:1<12::AID-JBM2>3.0.CO;2-U [DOI:10.1002/(SICI)1097-4636(199804)40:13.0.CO;2-U]
33. Soderholm K-JM. Filler systems an resin interface. Posterior composite resin dental restorative materials. 1985:139-59.
34. Nikolaenko SA, Lohbauer U, Roggendorf M, Petschelt A, Dasch W, Frankenberger R. Influence of c-factor and layering technique on microtensile bond strength to dentin. Dent Mater. 2004 Jul;20(6):579-85. [DOI:10.1016/j.dental.2003.08.001] [PMID]
35. Sagsoz O, Ilday NO, Karatas O, Cayabatmaz M, Parlak H, Olmez MH, et al. The bond strength of highly filled flowable composites placed in two different configuration factors. J Conserv Dent. 2016 Jan-Feb;19(1):21-5. [DOI:10.4103/0972-0707.173188] [PMID] []
36. Lu H, Lee YK, Oguri M, Powers JM. Properties of a dental resin composite with a spherical inorganic filler. Oper Dent. 2006 Nov-Dec;31(6):734-40. [DOI:10.2341/05-154] [PMID]
37. Dewaele M, Truffier-Boutry D, Devaux J, Leloup G. Volume contraction in photocured dental resins: the shrinkage-conversion relationship revisited. Dent Mater. 2006 Apr;22(4):359-65. [DOI:10.1016/j.dental.2005.03.014] [PMID]
38. Alonso RC, Cunha LG, Correr GM, Cunha Brandt W, Correr-Sobrinho L, Sinhoreti MA. Relationship between bond strength and marginal and internal adaptation of composite restorations photocured by different methods. Acta Odontol Scand. 2006 Oct;64(5):306-13. [DOI:10.1080/00016350600791744] [PMID]
39. Emami N, Söderholm KJ. How light irradiance and curing time affect monomer conversion in light-cured resin composites. Eur J Oral Sci. 2003 Dec;111(6):536-42. [DOI:10.1111/j.0909-8836.2003.00082.x] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |