Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 1 (3-2025)
J Res Dent Maxillofac Sci 2025, 10(1): 25-33 |
Back to browse issues page


Ethics code: IR.MUS.SD.REC.1393.922008
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Parisay I, Borouzi Niat A, Toumaj A, Bahramian L, Tarkhani M, Fallah Toosi F et al . Fracture Resistance and Esthetic Appearance of Reattached Incisor Tooth Fragments with Different Preparation Techniques in Simulated Crown Fractures. J Res Dent Maxillofac Sci 2025; 10 (1) :25-33
URL: http://jrdms.dentaliau.ac.ir/article-1-768-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-768-en.html
Iman Parisay1 

 , Alireza Borouzi Niat2 , Ahmad Toumaj3 , Lida Bahramian4 , Mahdieh Tarkhani5 , Fatemeh Fallah Toosi5 , Homeira Mohammadi *6
, Alireza Borouzi Niat2 , Ahmad Toumaj3 , Lida Bahramian4 , Mahdieh Tarkhani5 , Fatemeh Fallah Toosi5 , Homeira Mohammadi *6
, Alireza Borouzi Niat2 , Ahmad Toumaj3 , Lida Bahramian4 , Mahdieh Tarkhani5 , Fatemeh Fallah Toosi5 , Homeira Mohammadi *6
1- Pediatric Dentistry Department, Dental Research Center, Faculty of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
2- Restorative Dentistry Department, Dental Research Center, Faculty of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
3- Department of Prosthodontics, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
4- Pediatric Dentist, Copenhagen, Denmark
5- Dentist, Mashhad, Iran
6- Pediatric Dentistry Department, Faculty of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran ,Homeira.mohamadi72@gmail.com
2- Restorative Dentistry Department, Dental Research Center, Faculty of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran
3- Department of Prosthodontics, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
4- Pediatric Dentist, Copenhagen, Denmark
5- Dentist, Mashhad, Iran
6- Pediatric Dentistry Department, Faculty of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran ,
Full-Text [PDF 446 kb]
(817 Downloads)
| Abstract (HTML) (2607 Views)
Full-Text: (605 Views)
Abstract
Background and Aim: This study compared the fracture resistance and esthetic appearance of reattached incisor tooth fragments with different preparation techniques in simulated crown fractures (CFs).
Materials and Methods: In this in vitro study, 50 permanent maxillary incisors were randomly divided into five groups (n=10). After induction of uncomplicated CFs, the fractured teeth were restored using five methods: (I) simple reattachment (SR), (II) circumferential chamfer (CC), (III) buccal scalloped bevel and lingual bevel (BSB&LB), (IV) buccal and lingual overcontour (BO&LO), and (V) buccal scalloped bevel and lingual overcontour (BSB&LO). After thermocycling, the fracture resistance of the teeth was measured, and their esthetic appearance was assessed using Easyshade spectrophotometer and the United States Public Health Service (USPHS) visual scale. One-way ANOVA, Tukey’s post-hoc test, and paired t-test were used to analyze the data (alpha=0.05).
Results: The secondary fracture resistance was significantly lower than the primary fracture resistance in the control (P=0.000), CC (P=0.01), BSB&LB (P=0.004), BO&LO (P<0.001), and BSB&LO (P<0.001) groups. The CC group showed a significantly higher secondary fracture resistance than the BO&LO group (P=0.02). Although a more favorable esthetic appearance was observed in the BSB&LB group, no significant difference was found in color difference (∆E) among the groups. Moreover, no statistically significant difference was detected among the study groups regarding the USPHS scale (P>0.05).
Conclusion: Restoration with the CC method may improve the fracture resistance of reattached fragments in simulated CFs in maxillary incisors. However, no considerable difference was found regarding the esthetic appearance among the tested techniques.
Keywords: Esthetics, Dental; Dental Prosthesis; Tooth Crown
Introduction
Materials and Methods: In this in vitro study, 50 permanent maxillary incisors were randomly divided into five groups (n=10). After induction of uncomplicated CFs, the fractured teeth were restored using five methods: (I) simple reattachment (SR), (II) circumferential chamfer (CC), (III) buccal scalloped bevel and lingual bevel (BSB&LB), (IV) buccal and lingual overcontour (BO&LO), and (V) buccal scalloped bevel and lingual overcontour (BSB&LO). After thermocycling, the fracture resistance of the teeth was measured, and their esthetic appearance was assessed using Easyshade spectrophotometer and the United States Public Health Service (USPHS) visual scale. One-way ANOVA, Tukey’s post-hoc test, and paired t-test were used to analyze the data (alpha=0.05).
Results: The secondary fracture resistance was significantly lower than the primary fracture resistance in the control (P=0.000), CC (P=0.01), BSB&LB (P=0.004), BO&LO (P<0.001), and BSB&LO (P<0.001) groups. The CC group showed a significantly higher secondary fracture resistance than the BO&LO group (P=0.02). Although a more favorable esthetic appearance was observed in the BSB&LB group, no significant difference was found in color difference (∆E) among the groups. Moreover, no statistically significant difference was detected among the study groups regarding the USPHS scale (P>0.05).
Conclusion: Restoration with the CC method may improve the fracture resistance of reattached fragments in simulated CFs in maxillary incisors. However, no considerable difference was found regarding the esthetic appearance among the tested techniques.
Keywords: Esthetics, Dental; Dental Prosthesis; Tooth Crown
Introduction
Traumatic dental injury is a challenging oral health problem that encompasses a broad variety of injuries, each requiring a particular treatment [1]. As the fifth most common condition, 22.7% of the people experience dental trauma worldwide [1, 2]. Impaired esthetics, mastication, and speech, and financial burden caused by dental injuries may all have adverse effects on psychological health [3, 4]. Additionally, if not managed timely, it can adversely affect the social activities and quality of life of patients [3]. Simple crown fracture (CF) without pulp exposure is the most common type of dental injury, affecting almost 900 million individuals between 7 to 65 years worldwide [1, 5]. The majority of CFs occur in maxillary central incisors due to their position and protrusion [6]. Currently, CFs are usually treated by full-coverage composite restorations, laminate veneers, and ceramic crowns; however, their effectiveness is limited due to substantial sacrifice of the remaining tooth structure during preparation [6]. Moreover, it has been documented that the natural esthetic appearance of traumatized teeth cannot be fully restored with the abovementioned treatments [7].
Evidence shows that patients with CF may benefit from the fragment reattachment technique using composite resin as a simple, low-cost, and fast treatment option with minimal complications [8, 9]. This approach has several therapeutic benefits compared to the conventional composite restorations, such as improved esthetics due to preservation of the shape, color, transparency, and surface texture of natural tooth and an incisal edge wear comparable to that of the adjacent teeth [7]. In this regard, clinicians have employed a variety of preparation techniques to increase the fracture resistance of reattached fragments such as enamel bevel, external chamfer, dentinal groove, overcontour, and simple reattachment without any preparation [7, 10, 11]. There are certain indications, benefits, and drawbacks associated with each of these preparation techniques. Earlier investigations have revealed that reattached teeth without any preparation have a lower fracture resistance than those restored with beveled, chamfered, and circumferentially beveled methods [12, 13]. On the other hand, dental esthetics may be adversely affected by replacement of dentin with composite resin in the dentinal groove technique [7]. In addition, it has been suggested that the external chamfer procedure may facilitate the repositioning procedure of the fractured fragment compared to other preparation methods [14]. However, the composite resin used in the external chamfer and overcontour methods may negatively affect the esthetic appearance of the teeth in the long-term due to color change or wear of composite resin [14].
Although several preparation methods have been previously examined, only a few have investigated the fracture resistance and esthetic appearance of reattached fragments. Therefore, the current study aimed to evaluate and compare the fracture resistance and esthetic appearance of reattached incisor tooth fragments with different preparation techniques in simulated CFs.
Materials and Methods
Evidence shows that patients with CF may benefit from the fragment reattachment technique using composite resin as a simple, low-cost, and fast treatment option with minimal complications [8, 9]. This approach has several therapeutic benefits compared to the conventional composite restorations, such as improved esthetics due to preservation of the shape, color, transparency, and surface texture of natural tooth and an incisal edge wear comparable to that of the adjacent teeth [7]. In this regard, clinicians have employed a variety of preparation techniques to increase the fracture resistance of reattached fragments such as enamel bevel, external chamfer, dentinal groove, overcontour, and simple reattachment without any preparation [7, 10, 11]. There are certain indications, benefits, and drawbacks associated with each of these preparation techniques. Earlier investigations have revealed that reattached teeth without any preparation have a lower fracture resistance than those restored with beveled, chamfered, and circumferentially beveled methods [12, 13]. On the other hand, dental esthetics may be adversely affected by replacement of dentin with composite resin in the dentinal groove technique [7]. In addition, it has been suggested that the external chamfer procedure may facilitate the repositioning procedure of the fractured fragment compared to other preparation methods [14]. However, the composite resin used in the external chamfer and overcontour methods may negatively affect the esthetic appearance of the teeth in the long-term due to color change or wear of composite resin [14].
Although several preparation methods have been previously examined, only a few have investigated the fracture resistance and esthetic appearance of reattached fragments. Therefore, the current study aimed to evaluate and compare the fracture resistance and esthetic appearance of reattached incisor tooth fragments with different preparation techniques in simulated CFs.
Materials and Methods
Study samples:
This in vitro study evaluated 50 human maxillary central incisors freshly extracted for periodontal reasons. The study was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUS.SD.REC.1393.922008). A digital microscope (Dino Lite Pro 8c2937, Taiwan) was used to inspect the samples at 40x magnification. Sound teeth with no caries, cracks, or fractures were included in the study. An ultrasonic scaler (Guilin Woodpecker Medical Instrument Co., Ltd. Guangxi, China) was used to eliminate the remaining periodontal tissues. Before the experiment, all samples were disinfected with 0.2% thymol (Adonis Gol Darou Co., Tehran, Iran) and stored in saline (Samen Pharmaceutical Co., Mashhad, Iran) which was refreshed weekly. In order to assess the primary esthetic appearance of the teeth, their color was spectrophotometrically analyzed using Easyshade spectrophotometer (VITA Zahnfabrik, Bad Säckingen, Germany). Finally, the tooth crowns were sectioned into equal thirds using both horizontal and vertical lines. Specimens were then mounted in a cylinder containing auto-polymerizing acrylic resin (Acropars 200, Marlic Medical Industries Co., Tehran, Iran) to 1 mm below their cementoenamel junction to simulate CF.
Measurement of primary fracture resistance:
Load was applied to the intersection of the incisal third and mesial third of the enamel surface in a universal testing machine (Santam, Tehran, Iran) with a crosshead speed of 0.6 mm/minute in buccolingual direction (Figure 1). The fracture resistance was then measured in Newtons (N) [15]. All fractured segments were stored in distilled water for 24 hours before the restoration procedure.
Figure 1. Load application for measurement of fracture resistance
Sample restoration:
Initially, 37% phosphoric acid (3M ESPE, St Paul, MN, USA) was used for 30 seconds to etch the enamel surface, and for 10 seconds to etch the dentin surface, followed by rinsing and air drying for 10 seconds [16]. Next, Adper Singlebond 2 adhesive (3M ESPE, St Paul, MN, USA) was applied according to the manufacturer’s instructions [16], and light-cured (Blue Phase C8; Ivoclar Vivadent, Schaan, Lichtenstein) with a light intensity of 500 mW/cm2 for 20 seconds. The light curing unit was calibrated for each study group according to the manufacturer's instructions. A thin coating of flowable composite resin (Z350 Filtek; 3M ESPE, St Paul, MN, USA) matching the tooth color was applied to reattach the fractured fragment, and light-cured for 40 seconds from the buccal and lingual directions [15].
Study groups:
The specimens were randomly divided into five groups (n=10) as follows:
Control group: Simple reattachment without any preparation.
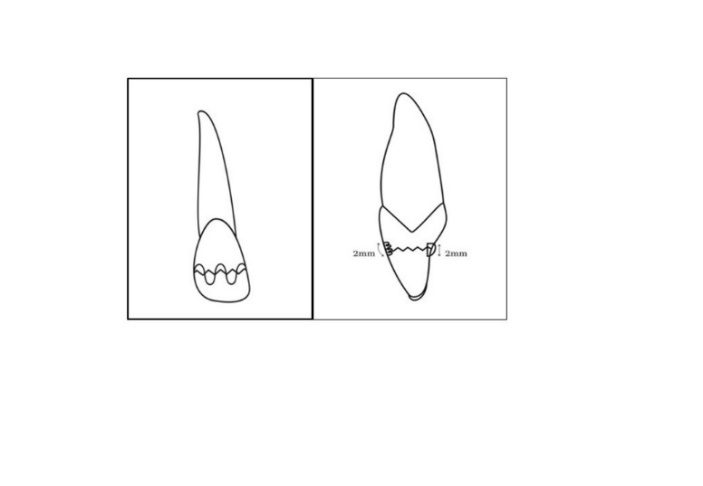
Circumferential chamfer (CC) preparation: A circumferential chamfer was prepared with 0.5 mm depth and 2 mm width around the fracture line using a No.2 round diamond bur (D&Z GmbH, Frankfurt, Germany), followed by the restoration procedure (Figure 2).
Figure 2. Circumferential chamfer preparation from the buccal and mesial views in a maxillary incisor
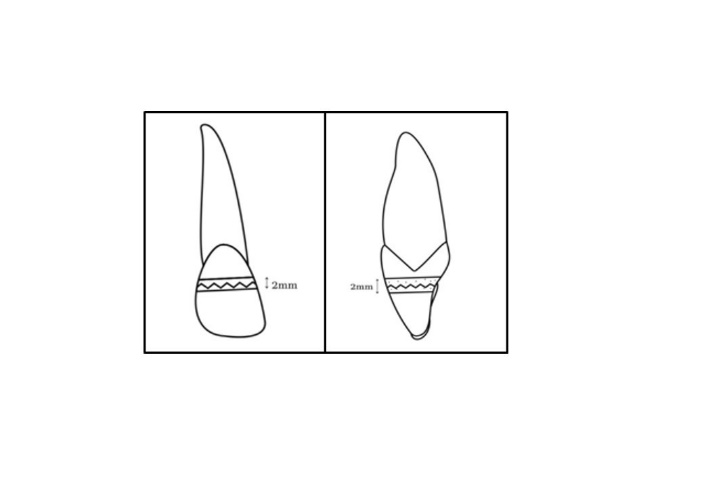
Buccal scalloped bevel and lingual bevel (BSB&LB) preparation: A scalloped bevel (0.5 mm depth, 2 mm width) was prepared in the buccal surface using a flame bur. Moreover, another bevel (0.5 mm depth, 2 mm width) was prepared around the fracture line in the lingual surface by a No.2 round diamond bur. Finally, restoration was performed as explained earlier (Figure 3).
Figure 3. Buccal scalloped bevel and lingual bevel preparation from the buccal and mesial views in a maxillary incisor
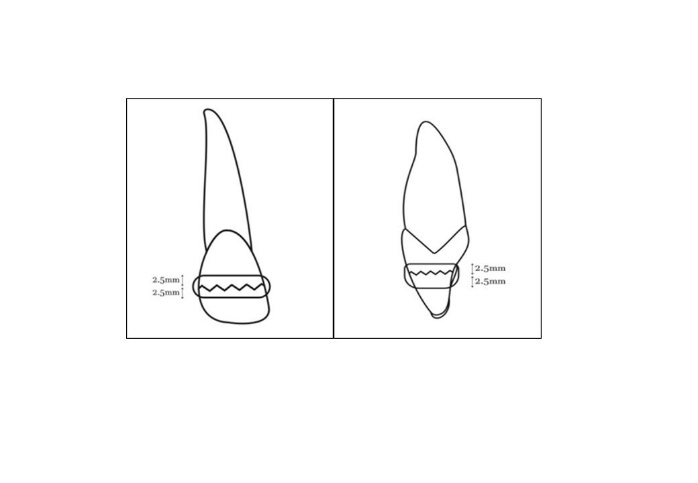
Buccal and lingual overcontour (BO&LO) preparation: An overcontour in the buccal and lingual surfaces was prepared using a thin layer of green wax (0.5 mm thickness, 2.5 mm coronoapical extension) sticking to the fracture line and then an impression was made using putty impression material. After etching and bonding, composite resin was applied on the putty index and placed on the tooth; light curing was then performed (Figure 4).
Figure 4. Buccal and lingual overcontour preparation from the buccal and mesial views
Buccal scalloped bevel and lingual overcontour (BSB&LO) preparation: A scalloped bevel (0.5 mm depth, 2 mm width) was prepared in the buccal surface as explained earlier. An overcontour (0.5 mm thickness, 2.5 mm coronoapical extension) was prepared in the lingual surface. Finally, restoration was performed as explained earlier (Figure 5).
This in vitro study evaluated 50 human maxillary central incisors freshly extracted for periodontal reasons. The study was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUS.SD.REC.1393.922008). A digital microscope (Dino Lite Pro 8c2937, Taiwan) was used to inspect the samples at 40x magnification. Sound teeth with no caries, cracks, or fractures were included in the study. An ultrasonic scaler (Guilin Woodpecker Medical Instrument Co., Ltd. Guangxi, China) was used to eliminate the remaining periodontal tissues. Before the experiment, all samples were disinfected with 0.2% thymol (Adonis Gol Darou Co., Tehran, Iran) and stored in saline (Samen Pharmaceutical Co., Mashhad, Iran) which was refreshed weekly. In order to assess the primary esthetic appearance of the teeth, their color was spectrophotometrically analyzed using Easyshade spectrophotometer (VITA Zahnfabrik, Bad Säckingen, Germany). Finally, the tooth crowns were sectioned into equal thirds using both horizontal and vertical lines. Specimens were then mounted in a cylinder containing auto-polymerizing acrylic resin (Acropars 200, Marlic Medical Industries Co., Tehran, Iran) to 1 mm below their cementoenamel junction to simulate CF.
Measurement of primary fracture resistance:
Load was applied to the intersection of the incisal third and mesial third of the enamel surface in a universal testing machine (Santam, Tehran, Iran) with a crosshead speed of 0.6 mm/minute in buccolingual direction (Figure 1). The fracture resistance was then measured in Newtons (N) [15]. All fractured segments were stored in distilled water for 24 hours before the restoration procedure.
Figure 1. Load application for measurement of fracture resistance
{kind=link}
Sample restoration:
Initially, 37% phosphoric acid (3M ESPE, St Paul, MN, USA) was used for 30 seconds to etch the enamel surface, and for 10 seconds to etch the dentin surface, followed by rinsing and air drying for 10 seconds [16]. Next, Adper Singlebond 2 adhesive (3M ESPE, St Paul, MN, USA) was applied according to the manufacturer’s instructions [16], and light-cured (Blue Phase C8; Ivoclar Vivadent, Schaan, Lichtenstein) with a light intensity of 500 mW/cm2 for 20 seconds. The light curing unit was calibrated for each study group according to the manufacturer's instructions. A thin coating of flowable composite resin (Z350 Filtek; 3M ESPE, St Paul, MN, USA) matching the tooth color was applied to reattach the fractured fragment, and light-cured for 40 seconds from the buccal and lingual directions [15].
Study groups:
The specimens were randomly divided into five groups (n=10) as follows:
Control group: Simple reattachment without any preparation.
Circumferential chamfer (CC) preparation: A circumferential chamfer was prepared with 0.5 mm depth and 2 mm width around the fracture line using a No.2 round diamond bur (D&Z GmbH, Frankfurt, Germany), followed by the restoration procedure (Figure 2).
Figure 2. Circumferential chamfer preparation from the buccal and mesial views in a maxillary incisor
{kind=link}
Buccal scalloped bevel and lingual bevel (BSB&LB) preparation: A scalloped bevel (0.5 mm depth, 2 mm width) was prepared in the buccal surface using a flame bur. Moreover, another bevel (0.5 mm depth, 2 mm width) was prepared around the fracture line in the lingual surface by a No.2 round diamond bur. Finally, restoration was performed as explained earlier (Figure 3).
Figure 3. Buccal scalloped bevel and lingual bevel preparation from the buccal and mesial views in a maxillary incisor
{kind=link}
Buccal and lingual overcontour (BO&LO) preparation: An overcontour in the buccal and lingual surfaces was prepared using a thin layer of green wax (0.5 mm thickness, 2.5 mm coronoapical extension) sticking to the fracture line and then an impression was made using putty impression material. After etching and bonding, composite resin was applied on the putty index and placed on the tooth; light curing was then performed (Figure 4).
Figure 4. Buccal and lingual overcontour preparation from the buccal and mesial views
{kind=link}
Buccal scalloped bevel and lingual overcontour (BSB&LO) preparation: A scalloped bevel (0.5 mm depth, 2 mm width) was prepared in the buccal surface as explained earlier. An overcontour (0.5 mm thickness, 2.5 mm coronoapical extension) was prepared in the lingual surface. Finally, restoration was performed as explained earlier (Figure 5).
Figure 5. Buccal scalloped bevel and lingual overcontour preparation from the buccal and mesial views in a maxillary incisor
All teeth were stored in distilled water for 24 hours and were then thermocycled for 1000 cycles between 5℃-55℃ with a dwell time of 15 seconds under controlled conditions. All the experimental procedures, such as tooth preparation, restoration, fracture resistance testing, and esthetic appearance assessments were made by one skillful operator.
Assessment of esthetic appearance:
The color of restored samples was evaluated spectrophotometrically using Easyshade spectrophotometer (VITA Zahnfabrik, Bad Säckingen, Germany) in daylight (10:00 a.m.). The color difference (ΔE) between the sound and restored teeth was analyzed using the following formula:
ΔE*ab (L*a*b*) = [(ΔL*)2 + (Δa*)2 + (Δb*)2] ½
In this formula, L ∗, a ∗, and b ∗ represent the CIE L*a*b* color coordinates [17].
Three operative dentists with proper color perception, as determined by the Ishihara test, inspected all the study samples. They were first calibrated by color assessment of 10 teeth other than the research samples. The kappa test was used to verify their inter-examiner reliability (K=0.8). To assess their intra-examiner reliability, they were asked to reassess the color of the same 10 teeth after a 2-week period. The visual esthetic assessments were performed using the United States Public Health Service (USPHS) visual scale [18]. The following scoring system was used:
Alpha score: indicated that the fracture line was invisible and that the dental composite and natural teeth had an acceptable color match.
Bravo score: indicated that the fracture line was detectable but not clearly visible.
Charlie score: indicated a fully visible fracture line and a clinically unacceptable appearance. Each visual score was assigned a numerical value: 1 for Alpha, 2 for Bravo, and 3 for Charlie. The group with the closest average numerical value to 1 was the most satisfactory group according to the USPHS visual scale.
Measurement of secondary fracture resistance:
The fracture resistance of all specimens was measured again using a universal testing machine (Santam, Tehran, Iran) with a crosshead speed of 0.6 mm/minute at the same points specified in the first evaluation [15].
Statistical analysis:
All statistical analyses were carried out using SPSS version 11.5 (SPSS Inc., Chicago, IL, USA). Normal distribution of data was confirmed by the Kolmogorov-Smirnov test. One-way ANOVA, followed by the Tukey’s post-hoc test were used to compare the study groups regarding the mean difference. In addition, the paired t-test was used to analyze the change in each group after the experiment. P<0.05 was considered statistically significant.
Results
{kind=link}
All teeth were stored in distilled water for 24 hours and were then thermocycled for 1000 cycles between 5℃-55℃ with a dwell time of 15 seconds under controlled conditions. All the experimental procedures, such as tooth preparation, restoration, fracture resistance testing, and esthetic appearance assessments were made by one skillful operator.
Assessment of esthetic appearance:
The color of restored samples was evaluated spectrophotometrically using Easyshade spectrophotometer (VITA Zahnfabrik, Bad Säckingen, Germany) in daylight (10:00 a.m.). The color difference (ΔE) between the sound and restored teeth was analyzed using the following formula:
ΔE*ab (L*a*b*) = [(ΔL*)2 + (Δa*)2 + (Δb*)2] ½
In this formula, L ∗, a ∗, and b ∗ represent the CIE L*a*b* color coordinates [17].
Three operative dentists with proper color perception, as determined by the Ishihara test, inspected all the study samples. They were first calibrated by color assessment of 10 teeth other than the research samples. The kappa test was used to verify their inter-examiner reliability (K=0.8). To assess their intra-examiner reliability, they were asked to reassess the color of the same 10 teeth after a 2-week period. The visual esthetic assessments were performed using the United States Public Health Service (USPHS) visual scale [18]. The following scoring system was used:
Alpha score: indicated that the fracture line was invisible and that the dental composite and natural teeth had an acceptable color match.
Bravo score: indicated that the fracture line was detectable but not clearly visible.
Charlie score: indicated a fully visible fracture line and a clinically unacceptable appearance. Each visual score was assigned a numerical value: 1 for Alpha, 2 for Bravo, and 3 for Charlie. The group with the closest average numerical value to 1 was the most satisfactory group according to the USPHS visual scale.
Measurement of secondary fracture resistance:
The fracture resistance of all specimens was measured again using a universal testing machine (Santam, Tehran, Iran) with a crosshead speed of 0.6 mm/minute at the same points specified in the first evaluation [15].
Statistical analysis:
All statistical analyses were carried out using SPSS version 11.5 (SPSS Inc., Chicago, IL, USA). Normal distribution of data was confirmed by the Kolmogorov-Smirnov test. One-way ANOVA, followed by the Tukey’s post-hoc test were used to compare the study groups regarding the mean difference. In addition, the paired t-test was used to analyze the change in each group after the experiment. P<0.05 was considered statistically significant.
Results
Fracture resistance:
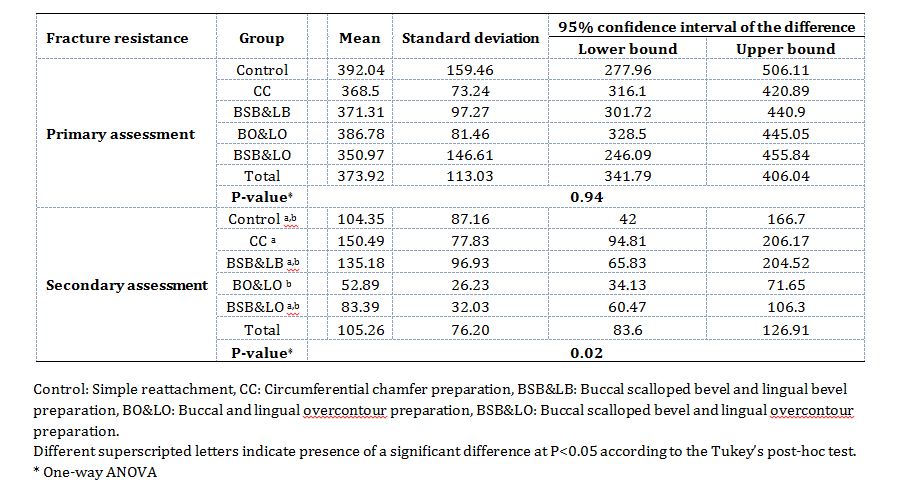
The primary and secondary fracture resistance values of the study groups are presented in Table 1. As shown, no significant difference was detected among the groups for primary fracture resistance (P>0.05). However, a statistically significant difference was observed in the secondary fracture resistance among the groups (P=0.02, F= 3.110). The CC group showed a significantly higher secondary fracture resistance than the BO&LO group (P=0.02).
The secondary fracture resistance was significantly lower than the primary fracture resistance in the control (P=0.000), CC (P=0.01), BSB&LB (P=0.004), BO&LO (P<0.001), and BSB&LO (P<0.001) groups.
Table 2 presents the percentage of reduction in fracture resistance after the reattachment procedure compared to sound teeth in the five study groups. The BO&LO group had the highest, and the CC group had the lowest reduction in fracture resistance.
Esthetic appearance:
Spectrophotometry:
All groups had a mean ∆E greater than 3.3 (CC showed the highest and BSB&LB showed the lowest value), indicating the visibility of the fracture line (Table 3). Although a more favorable esthetic appearance was observed in the BSB&LB group, no significant difference was seen in terms of ∆E among the groups.
USPHS scale:
The esthetic appearance scores according to the USPHS scale are reported in Table 4. At the end of the study, the experts gave the highest score to the BO&LO group; while the CC group acquired the lowest score. However, the difference in this regard was not significant among the study groups.
The primary and secondary fracture resistance values of the study groups are presented in Table 1. As shown, no significant difference was detected among the groups for primary fracture resistance (P>0.05). However, a statistically significant difference was observed in the secondary fracture resistance among the groups (P=0.02, F= 3.110). The CC group showed a significantly higher secondary fracture resistance than the BO&LO group (P=0.02).
The secondary fracture resistance was significantly lower than the primary fracture resistance in the control (P=0.000), CC (P=0.01), BSB&LB (P=0.004), BO&LO (P<0.001), and BSB&LO (P<0.001) groups.
Table 2 presents the percentage of reduction in fracture resistance after the reattachment procedure compared to sound teeth in the five study groups. The BO&LO group had the highest, and the CC group had the lowest reduction in fracture resistance.
Esthetic appearance:
Spectrophotometry:
All groups had a mean ∆E greater than 3.3 (CC showed the highest and BSB&LB showed the lowest value), indicating the visibility of the fracture line (Table 3). Although a more favorable esthetic appearance was observed in the BSB&LB group, no significant difference was seen in terms of ∆E among the groups.
USPHS scale:
The esthetic appearance scores according to the USPHS scale are reported in Table 4. At the end of the study, the experts gave the highest score to the BO&LO group; while the CC group acquired the lowest score. However, the difference in this regard was not significant among the study groups.
Table 1. Primary and secondary fracture resistance (N) of the study groups (n=10)
Table 2. Percentage of reduction in fracture resistance after reattachment (secondary-primary)
Table 3. Mean ∆E of the study groups (n=10)
Table 4. Visual assessment of esthetic appearance using the USPHS scale
Discussion
This study assessed the fracture resistance and esthetic appearance of reattached incisor tooth fragments with various preparation methods in simulated CFs. The maxillary incisors were used in the present study to simulate CFs. The anatomy and anterior position of these teeth make them more susceptible to traumatic dental injuries compared to other teeth [6]. The maxillary incisors bear a high strain, requiring strong and esthetically pleasant restorations, if damaged [19]. In order to induce CFs, a vertical load was applied to the teeth at a crosshead speed of 0.6 mm/min, which was in accordance with previous studies [14, 20].
The fractured segments were stored in distilled water for 24 hours since it has been documented that the bond strength of a fractured tooth may decrease if left in a dry environment for more than one hour [21]. Similarly, Lee et al. [22] found a notable reduction in bond strength of fractured teeth stored in %0.9 saline compared to the samples kept in distilled water before the reattachment process. Also, it has been reported that storing the fractured segments in a dry environment may play an important role in color mismatch of the restored teeth [20]. In this regard, Andreasen JO and Andreasen FM [23] reported that application of chemical-cure composite resins may also contribute to this issue. Since no differences have been found between light-cure and self-cure materials in the literature [14], light-cure composite was used for the restoration procedure in the present study due to its simple application. Besides, an adhesive system was applied after etching in the present study to improve the durability of the reattached fragment [23].
In the current study, the restoration procedure with the CC method was associated with the highest secondary fracture resistance among all the study groups. In agreement with the present findings, Bruschi‐Alonso et al. [24] reported the superior impact strength of the CC technique for fragment reattachment in fractured anterior teeth. The suggested reasons for this finding include a) expanding the bonding surface area and allowing for a stronger bond between the fragment and the residual tooth structure due to changes in enamel prisms caused by chamfer preparation, and b) application of a composite in the chamfer area with exceptional mechanical qualities to strengthen the bonding interface [20, 25]. Besides, there are convincing reports regarding the improvement of fracture resistance with a 2-mm chamfer compared to a 1-mm chamfer [26].
However, in the present study, the secondary fracture resistance of the samples did not reach their primary fracture resistance (sound teeth) in any group, which was in line with the findings of previous studies [15, 20]. Likewise, a previous study reported that the fracture resistance of repaired teeth with the chamfer approach was 60.6% of that of intact teeth [14]. It is worth mentioning that the fracture resistance of reattached specimens is mostly determined by the preparation design and the restoration material [27]. It can be assumed that the low flexural strength of resin may explain the present results regarding lower secondary fracture resistance than the fracture resistance of sound teeth [20]. Furthermore, another study reported that all teeth with reattached fragments required additional restorations after 7 years [28]. Thus, the patients have to take extra care of the restored teeth [20].
In the current study, although the fracture lines were visually detectable in all groups, the esthetic appearance of the BSB&LB samples was acceptable spectrophotometrically, which may be due to larger etched surface and superior optical properties caused by the scalloped bevel in comparison with other preparation techniques. Differences between the results of the two esthetic assessment methods may be due to their different nature. As mentioned earlier, all teeth were evaluated at 10 a.m., at the same distance from the spectrophotometer tube. Conversely, the ambient light may affect the results of the USPHS due to the fact that assessments were performed at different times of the day.
The main strength of the present study was comparison of four different conventional fragment reattachment methods. However, limitations of this study should also be taken into account when interpreting the results. This study had an in vitro design while the oral cavity is the ideal setting to evaluate the fracture resistance and esthetic appearance of the restored teeth. Also, performing visual esthetic evaluation in different lighting conditions may cause errors. Additionally, the present study did not assess the long-term changes in the specimens or their durability, microleakage or color stability, which may affect the interpretation of the results.
Conclusion
Restoration with the CC method may improve the fracture resistance of reattached fragments in simulated CFs in maxillary incisors. However, no considerable difference was found regarding the esthetic appearance among the tested techniques.
{kind=link}
Table 2. Percentage of reduction in fracture resistance after reattachment (secondary-primary)
{kind=link}
Table 3. Mean ∆E of the study groups (n=10)
{kind=link}
Table 4. Visual assessment of esthetic appearance using the USPHS scale
{kind=link}
Discussion
This study assessed the fracture resistance and esthetic appearance of reattached incisor tooth fragments with various preparation methods in simulated CFs. The maxillary incisors were used in the present study to simulate CFs. The anatomy and anterior position of these teeth make them more susceptible to traumatic dental injuries compared to other teeth [6]. The maxillary incisors bear a high strain, requiring strong and esthetically pleasant restorations, if damaged [19]. In order to induce CFs, a vertical load was applied to the teeth at a crosshead speed of 0.6 mm/min, which was in accordance with previous studies [14, 20].
The fractured segments were stored in distilled water for 24 hours since it has been documented that the bond strength of a fractured tooth may decrease if left in a dry environment for more than one hour [21]. Similarly, Lee et al. [22] found a notable reduction in bond strength of fractured teeth stored in %0.9 saline compared to the samples kept in distilled water before the reattachment process. Also, it has been reported that storing the fractured segments in a dry environment may play an important role in color mismatch of the restored teeth [20]. In this regard, Andreasen JO and Andreasen FM [23] reported that application of chemical-cure composite resins may also contribute to this issue. Since no differences have been found between light-cure and self-cure materials in the literature [14], light-cure composite was used for the restoration procedure in the present study due to its simple application. Besides, an adhesive system was applied after etching in the present study to improve the durability of the reattached fragment [23].
In the current study, the restoration procedure with the CC method was associated with the highest secondary fracture resistance among all the study groups. In agreement with the present findings, Bruschi‐Alonso et al. [24] reported the superior impact strength of the CC technique for fragment reattachment in fractured anterior teeth. The suggested reasons for this finding include a) expanding the bonding surface area and allowing for a stronger bond between the fragment and the residual tooth structure due to changes in enamel prisms caused by chamfer preparation, and b) application of a composite in the chamfer area with exceptional mechanical qualities to strengthen the bonding interface [20, 25]. Besides, there are convincing reports regarding the improvement of fracture resistance with a 2-mm chamfer compared to a 1-mm chamfer [26].
However, in the present study, the secondary fracture resistance of the samples did not reach their primary fracture resistance (sound teeth) in any group, which was in line with the findings of previous studies [15, 20]. Likewise, a previous study reported that the fracture resistance of repaired teeth with the chamfer approach was 60.6% of that of intact teeth [14]. It is worth mentioning that the fracture resistance of reattached specimens is mostly determined by the preparation design and the restoration material [27]. It can be assumed that the low flexural strength of resin may explain the present results regarding lower secondary fracture resistance than the fracture resistance of sound teeth [20]. Furthermore, another study reported that all teeth with reattached fragments required additional restorations after 7 years [28]. Thus, the patients have to take extra care of the restored teeth [20].
In the current study, although the fracture lines were visually detectable in all groups, the esthetic appearance of the BSB&LB samples was acceptable spectrophotometrically, which may be due to larger etched surface and superior optical properties caused by the scalloped bevel in comparison with other preparation techniques. Differences between the results of the two esthetic assessment methods may be due to their different nature. As mentioned earlier, all teeth were evaluated at 10 a.m., at the same distance from the spectrophotometer tube. Conversely, the ambient light may affect the results of the USPHS due to the fact that assessments were performed at different times of the day.
The main strength of the present study was comparison of four different conventional fragment reattachment methods. However, limitations of this study should also be taken into account when interpreting the results. This study had an in vitro design while the oral cavity is the ideal setting to evaluate the fracture resistance and esthetic appearance of the restored teeth. Also, performing visual esthetic evaluation in different lighting conditions may cause errors. Additionally, the present study did not assess the long-term changes in the specimens or their durability, microleakage or color stability, which may affect the interpretation of the results.
Conclusion
Restoration with the CC method may improve the fracture resistance of reattached fragments in simulated CFs in maxillary incisors. However, no considerable difference was found regarding the esthetic appearance among the tested techniques.
Type of Study: Original article |
Subject:
pediatric
References
1. Lauridsen E, Andersson L, Suresh N. The dental trauma guide: an evidence-based treatment guide. Endodontology. 2023 Apr;35(2):79-84. [DOI:10.4103/endo.endo_46_23]
2. Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent Traumatol. 2018 Apr;34(2):71-86. [DOI:10.1111/edt.12389] [PMID]
3. Bendo CB, Paiva SM, Varni JW, Vale MP. Oral health-related quality of life and traumatic dental injuries in Brazilian adolescents. Community Dent Oral Epidemiol. 2014 Jun;42(3):216-23. [DOI:10.1111/cdoe.12078] [PMID]
4. Pujita C, Nuvvula S, Shilpa G, Nirmala S, Yamini V. Informative promotional outcome on school teachers' knowledge about emergency management of dental trauma. J Conserv Dent. 2013 Jan;16(1):21-7. [DOI:10.4103/0972-0707.105293] [PMID] []
5. Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000 Mar;45(1):2-9. [DOI:10.1111/j.1834-7819.2000.tb00234.x] [PMID]
6. Stellini E, Stomaci D, Stomaci M, Petrone N, Favero L. Fracture strength of tooth fragment reattachments with postpone bevel and overcontour reconstruction. Dent Traumatol. 2008 Jun;24(3):283-8. [DOI:10.1111/j.1600-9657.2007.00539.x] [PMID]
7. Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: a review of literature regarding techniques and materials. Oper Dent. 2004 Mar-Apr;29(2):226-33.
8. Rigo L, Baratieri L, Maia H, Arcari G. Ceramic fragment restoration of a traumatized tooth in a young patient. American Journal of Esthetic Dentistry. 2013 Dec 1;3(4):248-54. [DOI:10.11607/ajed.0071]
9. Garcia FCP, Poubel DLN, Almeida JCF, Toledo IP, Poi WR, Guerra ENS, Rezende LVML. Tooth fragment reattachment techniques-A systematic review. Dent Traumatol. 2018 Jun;34(3):135-43. [DOI:10.1111/edt.12392] [PMID]
10. Pusman E, Cehreli ZC, Altay N, Unver B, Saracbasi O, Ozgun G. Fracture resistance of tooth fragment reattachment: effects of different preparation techniques and adhesive materials. Dent Traumatol. 2010 Feb;26(1):9-15. [DOI:10.1111/j.1600-9657.2009.00855.x] [PMID]
11. Lo Giudice G, Lipari F, Lizio A, Cervino G, Cicciù M. Tooth fragment reattachment technique on a pluri traumatized tooth. J Conserv Dent. 2012 Jan;15(1):80-3. [DOI:10.4103/0972-0707.92613] [PMID] []
12. Goenka P, Sarawgi A, Dutta S. A conservative approach toward restoration of fractured anterior tooth. Contemp Clin Dent. 2012 Apr;3(Suppl 1):S67-70. [DOI:10.4103/0976-237X.95109] [PMID] []
13. Abdulkhayum A, Munjal S, Babaji P, Chaurasia VR, Munjal S, Lau H, et al. In-vitro Evaluation of Fracture Strength Recovery of Reattached Anterior Fractured Tooth Fragment Using Different Re-Attachment Techniques. J Clin Diagn Res. 2014 Mar;8(3):208-11. [DOI:10.7860/JCDR/2014/7161.4164] [PMID] []
14. Reis A, Francci C, Loguercio AD, Carrilho MR, Rodriques Filho LE. Re-attachment of anterior fractured teeth: fracture strength using different techniques. Oper Dent. 2001 May-Jun;26(3): 287-94.
15. Mahale VD, Solete P, Priscilla Antony D, Adimulapu HS, M H, Sambandam V. Analyzing the Impact of Different Bonding Protocol Strategies to Improve the Fracture Resistance of Uncomplicated Crown Fractures on Tooth Fracture Reattachment in Permanent Anterior Teeth: An In-vitro Study. Cureus. 2024 Mar 13;16(3):e56127. [DOI:10.7759/cureus.56127]
16. Karaman E, Yazici AR, Aksoy B, Karabulut E, Ozgunaltay G, Dayangac B. Effect of operator variability on microleakage with different adhesive systems. Eur J Dent. 2013 Sep;7(Suppl 1):S060-S065. [DOI:10.4103/1305-7456.119075] [PMID] []
17. Suzuki T, Ito C, Kitano K, Yamaguchi T. CIELAB Color Space as a Field for Tracking Color-Changing Chemical Reactions of Polymeric pH Indicators. ACS Omega. 2024 Aug 15;9(34):36682-36689. [DOI:10.1021/acsomega.4c05320] [PMID] []
18. Raluca DI. Visual versus colorimetric data analysis for color determination in resin veneers. Applied Medical Informatics. 2012 Mar 10;30(1):49-54.
19. Khawaja N, Punjabi SK, Kalhoro FA. Fractured maxillary central incisors: restoration with pins retained restoration: 2 case reports. The Professional Medical Journal. 2016 Feb 10;23(02):233-7. [DOI:10.17957/TPMJ/16.3070]
20. Demarco FF, Fay RM, Pinzon LM, Powers JM. Fracture resistance of re‐attached coronal fragments-influence of different adhesive materials and bevel preparation. Dental Traumatology. 2004 Jun;20(3):157-63. [DOI:10.1111/j.1600-4469.2004.00221.x] [PMID]
21. Capp CI, Roda MI, Tamaki R, Castanho GM, Camargo MA, de Cara AA. Reattachment of rehydrated dental fragment using two techniques. Dent Traumatol. 2009 Feb;25(1):95-9. [DOI:10.1111/j.1600-9657.2008.00715.x] [PMID]
22. Lee JJ, Nettey-Marbell A, Cook A Jr, Pimenta LA, Leonard R, Ritter AV. Using extracted teeth for research: the effect of storage medium and sterilization on dentin bond strengths. J Am Dent Assoc. 2007 Dec;138(12):1599-603. [DOI:10.14219/jada.archive.2007.0110] [PMID]
23. Andreasen JO, Andreasen FM. Textbook and color atlas of traumatic injuries to the teeth. Munksgaard; 1994.
24. Bruschi-Alonso RC, Alonso RC, Correr GM, Alves MC, Lewgoy HR, Sinhoreti MA, et al. Reattachment of anterior fractured teeth: effect of materials and techniques on impact strength. Dent Traumatol. 2010 Aug;26(4):315-22. [DOI:10.1111/j.1600-9657.2010.00906.x] [PMID]
25. De Santis R, Prisco D, Nazhat SN, Riccitiello F, Ambrosio L, Rengo S, et al. Mechanical strength of tooth fragment reattachment. J Biomed Mater Res. 2001 Jun 15;55(4):629-36.
https://doi.org/10.1002/1097-4636(20010615)55:4<629::AID-JBM1057>3.0.CO;2-2 [DOI:10.1002/1097-4636(20010615)55:43.0.CO;2-2] [PMID]
26. Patil SG, Verma S, Kumar S. An In vitro study to compare the effect of chamfer and shoulder on the Fracture resistance of all ceramic Restorations. J Cardiovasc Dis Res. 2023; 14(5): 2289-91.
27. Chandran R, Rayar S, Ravi AB, Haridas K. Comparative Evaluation of Fracture Resistance of Incisor Fragments Using Simple, Bevel, Internal Groove Preparation Designs and Reattached with Nanocomposites: An In Vitro Study. J Pharm Bioallied Sci. 2020 Aug;12(Suppl 1):S373-7. [DOI:10.4103/jpbs.JPBS_110_20] [PMID] []
28. Spinas E. Longevity of composite restorations of traumatically injured teeth. Am J Dent. 2004 Dec;17(6):407-11.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |