Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 2 (6-2025)
J Res Dent Maxillofac Sci 2025, 10(2): 134-143 |
Back to browse issues page

Ethics code: IR.TUMS.DENTISTRY.REC.1398.145
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi Mahounak F, Chiniforush N, Anagnostaki E A, Bazari Jamkhaneh A, Moradi Z. Effects of Laser-Assisted and LED-Assisted Bleaching Techniques on Color Parameters. J Res Dent Maxillofac Sci 2025; 10 (2) :134-143
URL: http://jrdms.dentaliau.ac.ir/article-1-755-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-755-en.html
Farzaneh Sadeghi Mahounak1 
 , Nasim Chiniforush2
, Nasim Chiniforush2  , Eugenia Anagnostaki Anagnostaki , Abolfazl Bazari Jamkhaneh3 , Zohreh Moradi *4
, Eugenia Anagnostaki Anagnostaki , Abolfazl Bazari Jamkhaneh3 , Zohreh Moradi *4
, Nasim Chiniforush2 , Eugenia Anagnostaki Anagnostaki , Abolfazl Bazari Jamkhaneh3 , Zohreh Moradi *4
1- Restorative Department, Dental School, Tehran University of Medical Sciences, Tehran, Iran
2- Laser Research Center of Dentistry, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran
3- Orthodontics Department, Dental School, Tehran University of Medical Sciences, Tehran, Iran
4- Laser Research Center of Dentistry, Restorative Department, Dental School, Tehran University of Medical Sciences, Tehran, Iran ,zohrehmoradi2003@yahoo.com
2- Laser Research Center of Dentistry, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran
3- Orthodontics Department, Dental School, Tehran University of Medical Sciences, Tehran, Iran
4- Laser Research Center of Dentistry, Restorative Department, Dental School, Tehran University of Medical Sciences, Tehran, Iran ,
Full-Text [PDF 446 kb]
(964 Downloads)
| Abstract (HTML) (1769 Views)
Full-Text: (979 Views)
Abstract
Background and Aim: This study assessed the effects of laser-assisted and light emitting diode (LED)-assisted bleaching on color parameters.
Materials and Methods: This in vitro study evaluated 40 sound central incisors and premolars immersed in tea solution for 6 days. They were then randomly divided into 4 groups: (I) Bleaching with White Smile containing 40% hydrogen peroxide gel + LED irradiation (Monitex; 4 blue lights with 420-490 nm wavelength and 1 red light with 620-630 nm wavelength), (II) Opalescence Boost containing 40% hydrogen peroxide gel without activation, (III) Opalescence Boost activated by LED, and (IV) Opalescence Boost activated by 980 nm diode laser with 2 W/cm2 power. The color parameters of the teeth were measured at baseline, after staining, immediately after bleaching, and 1 week after bleaching. Color change (∆E) was calculated and analyzed by one-way ANOVA and Tukey’s test (alpha=0.05).
Results: Discoloration was significantly resolved in all groups with significant ∆E values (P<0.05). All modalities had a comparable performance regarding the changes in value in the middle and coronal thirds, and caused tooth shade lightening. Opalescence Boost was superior to laser-assisted Opalescence Boost in the incisal third. The changes in a* and b* parameters were not significant and were within the range of lower chroma.
Conclusion: The results showed that laser-assisted bleaching with Opalescence Boost had the poorest performance regarding changes in L* parameter. The performance of the conventional Opalescence Boost, LED-assisted Opalescence Boost, and LED-assisted White Smile was the same regarding ∆L, ∆a, and ∆b.
Keywords: Bleaching Agents; Color; Lasers; Tooth Bleaching
Introduction
Tooth discoloration may occur due to several reasons, such as smoking (extrinsic staining), or endodontic treatment (intrinsic staining).
Bleaching is an effective and relatively safe dental procedure for correction of discoloration [1,2]. Chemical bleaching agents include oxidizing and reducing agents. The majority of the bleaching agents are oxidizing agents with different compositions. The bleaching mechanism is based on oxidation of hydrogen peroxide or its derivatives in the presence of activating agents such as heat and light [3]. The bleaching agents penetrate the enamel and dentin and remove the pigments by chemical reactions [4]. Bleaching corrects tooth discoloration and lightens the inherent color shade of dentin [5]. Hydrogen peroxide, due to its low molecular weight, can diffuse into the organic matrix of enamel and dentin; the generated free radicals attack the organic molecules and are eventually stabilized. This reaction results in further release of free radicals. At the same time, free radicals react with unsaturated bonds, cause cleavage of bonds, and change the energy level of enamel organic molecules. Resultantly, simpler molecules are formed that reflect less light and appear lighter [6].
Different light sources may be used for light-activated bleaching, such as light emitting diode (LED) and laser. LEDs (430-490 nm) usually have an output energy density of 200-2000 mW/cm2. Diode lasers with different wavelengths can also be used in continuous-wave or gated mode. Depending on the wavelength, lasers may have slight absorption in water and mineral phase of the tooth structure, and high absorption by pigments and penetrate deep into the hard tooth structure [7].
At present, different instruments are available for clinical shade matching and tooth color assessment such as spectrophotometers, colorimeters, and imaging systems. Dental clinicians may select any of these modalities based on their advantages and disadvantages. Spectrophotometers provide a colored digital map of the incisal, middle, and cervical thirds. They can be used with a smaller window size to detect color change (∆E) using the CIE L*a*b* color space [8]. In this system, the reflected light from an object is analyzed automatically and then the respective reflectance curve is drawn by the system and the Z, Y, and X parameters which are equivalent to L*, a*, and b* color parameters, respectively, are measured as such [9].
Dionysopoulos et al. [10] evaluated the efficacy of Er,Cr:YSGG laser-assisted bleaching spectrophotometrically and showed that laser-assisted bleaching can provide superior results with respect to ∆E and correction of discoloration. Also, Kiomars et al. [11] evaluated the efficacy of 810 and 980 nm diode laser irradiation for correction of tooth discolorations after external bleaching and showed that all bleaching techniques equally caused a significant ∆E. Fekrazad et al. [12] evaluated the efficacy of bleaching with Opalescence Xtra Boost® in comparison with the use of LaserSmile gel + 810 nm diode laser. The results showed that ∆E of the teeth in the laser-assisted bleaching group was 1.88 times greater than that in the conventional bleaching group. They showed that both bleaching methods with and without laser activation, caused significant ∆E, but laser-assisted bleaching had higher efficacy for this purpose.
This study aimed to assess the effects of laser-assisted bleaching versus LED-assisted bleaching on different color parameters such as ∆E, L*, a*, and b*. The null hypothesis of the study was that the performance of laser-assisted bleaching would not be significantly different from that of LED-assisted bleaching.
Materials and Methods
In this in vitro experimental study, the required sample size for each group was calculated to be 10 according to a study by Kiomars et al. [11] using one-way ANOVA power analysis feature of PASS 11, assuming α=0.05, β=0.2, mean standard deviation of 3.09, and effect size of 0.53. The study protocol was approved by the ethics committee of the university (IR.TUMS.DENTISTRY.REC.1398.145). Forty human central incisors and premolars, extracted as part of orthodontic treatment or due to periodontal disease, were used in this study. Teeth with cracks or structural defects were excluded. The teeth were selected by convenience sampling and were then randomly divided (by simple randomization) into four groups (n=10). The specimens were immersed in 0.5% chloramine T solution (Wako Pure Chemical Industry, Osaka, Japan) for 24 hours [10]. To standardize the specimens, the crowns were cut at 2 mm below the cementoenamel junction and were inspected under a stereomicroscope at x10 magnification to ensure their integrity. For standardization of the smear layer and creation of a smooth surface, the specimens were mounted in putty (Speedex, Coltene, Switzerland) from their palatal surface such that their buccal surface remained exposed. The tooth enamel was polished with 1200-grit abrasive paper (Soflex,3M Espe, USA) and polishing paste with 0.1 µm diamond particles (Diamond Paste; Jota Ruthi, Switzerland), and inspected again under a microscope to ensure no dentin exposure. Before bleaching treatment, the teeth were immersed in artificial saliva with the composition of 0.103 g/L CaCl2, 0.019 g/L MgCl2.6H2O, 0.544 g/L KH2PO4, 2.24 g/L KCL, and 0.650 g/L KOH at 37°C. A spectrophotometer (Spectroshade; MHD, Verona, Italy) was used to measure the color parameters at the center of the incisal, middle, and cervical thirds of the buccal surface three times for each specimen, and the mean values were calculated and reported. Next, to standardize the tooth color, 1% sodium hypochlorite (DATERRA; Manipulation Pharmacy, Ribeirão Preto, SP, Brazil) was used for 30 minutes to eliminate the external stains and discolorations. Enamel was then etched with 37% phosphoric acid (Scotchbond Universal Etchant, 3M ESPE, St. Paul, MN, USA) for 6 seconds, and rinsed with water for 30 seconds. Afterwards, 2 g of loose tea (Lipton Black Tea, Unilever, UK) was added to 100 mL of distilled water (Ebne Sina, Pars Peyvand, Iran) and heated for 10 minutes until boiling. The solution was filtered through a sterile gauze and allowed to cool down. The teeth were immersed in this solution for 6 days. The solution was refreshed every 24 hours [10]. The teeth were then randomly divided into 4 groups (n=10):
Background and Aim: This study assessed the effects of laser-assisted and light emitting diode (LED)-assisted bleaching on color parameters.
Materials and Methods: This in vitro study evaluated 40 sound central incisors and premolars immersed in tea solution for 6 days. They were then randomly divided into 4 groups: (I) Bleaching with White Smile containing 40% hydrogen peroxide gel + LED irradiation (Monitex; 4 blue lights with 420-490 nm wavelength and 1 red light with 620-630 nm wavelength), (II) Opalescence Boost containing 40% hydrogen peroxide gel without activation, (III) Opalescence Boost activated by LED, and (IV) Opalescence Boost activated by 980 nm diode laser with 2 W/cm2 power. The color parameters of the teeth were measured at baseline, after staining, immediately after bleaching, and 1 week after bleaching. Color change (∆E) was calculated and analyzed by one-way ANOVA and Tukey’s test (alpha=0.05).
Results: Discoloration was significantly resolved in all groups with significant ∆E values (P<0.05). All modalities had a comparable performance regarding the changes in value in the middle and coronal thirds, and caused tooth shade lightening. Opalescence Boost was superior to laser-assisted Opalescence Boost in the incisal third. The changes in a* and b* parameters were not significant and were within the range of lower chroma.
Conclusion: The results showed that laser-assisted bleaching with Opalescence Boost had the poorest performance regarding changes in L* parameter. The performance of the conventional Opalescence Boost, LED-assisted Opalescence Boost, and LED-assisted White Smile was the same regarding ∆L, ∆a, and ∆b.
Keywords: Bleaching Agents; Color; Lasers; Tooth Bleaching
Introduction
Tooth discoloration may occur due to several reasons, such as smoking (extrinsic staining), or endodontic treatment (intrinsic staining).
Bleaching is an effective and relatively safe dental procedure for correction of discoloration [1,2]. Chemical bleaching agents include oxidizing and reducing agents. The majority of the bleaching agents are oxidizing agents with different compositions. The bleaching mechanism is based on oxidation of hydrogen peroxide or its derivatives in the presence of activating agents such as heat and light [3]. The bleaching agents penetrate the enamel and dentin and remove the pigments by chemical reactions [4]. Bleaching corrects tooth discoloration and lightens the inherent color shade of dentin [5]. Hydrogen peroxide, due to its low molecular weight, can diffuse into the organic matrix of enamel and dentin; the generated free radicals attack the organic molecules and are eventually stabilized. This reaction results in further release of free radicals. At the same time, free radicals react with unsaturated bonds, cause cleavage of bonds, and change the energy level of enamel organic molecules. Resultantly, simpler molecules are formed that reflect less light and appear lighter [6].
Different light sources may be used for light-activated bleaching, such as light emitting diode (LED) and laser. LEDs (430-490 nm) usually have an output energy density of 200-2000 mW/cm2. Diode lasers with different wavelengths can also be used in continuous-wave or gated mode. Depending on the wavelength, lasers may have slight absorption in water and mineral phase of the tooth structure, and high absorption by pigments and penetrate deep into the hard tooth structure [7].
At present, different instruments are available for clinical shade matching and tooth color assessment such as spectrophotometers, colorimeters, and imaging systems. Dental clinicians may select any of these modalities based on their advantages and disadvantages. Spectrophotometers provide a colored digital map of the incisal, middle, and cervical thirds. They can be used with a smaller window size to detect color change (∆E) using the CIE L*a*b* color space [8]. In this system, the reflected light from an object is analyzed automatically and then the respective reflectance curve is drawn by the system and the Z, Y, and X parameters which are equivalent to L*, a*, and b* color parameters, respectively, are measured as such [9].
Dionysopoulos et al. [10] evaluated the efficacy of Er,Cr:YSGG laser-assisted bleaching spectrophotometrically and showed that laser-assisted bleaching can provide superior results with respect to ∆E and correction of discoloration. Also, Kiomars et al. [11] evaluated the efficacy of 810 and 980 nm diode laser irradiation for correction of tooth discolorations after external bleaching and showed that all bleaching techniques equally caused a significant ∆E. Fekrazad et al. [12] evaluated the efficacy of bleaching with Opalescence Xtra Boost® in comparison with the use of LaserSmile gel + 810 nm diode laser. The results showed that ∆E of the teeth in the laser-assisted bleaching group was 1.88 times greater than that in the conventional bleaching group. They showed that both bleaching methods with and without laser activation, caused significant ∆E, but laser-assisted bleaching had higher efficacy for this purpose.
This study aimed to assess the effects of laser-assisted bleaching versus LED-assisted bleaching on different color parameters such as ∆E, L*, a*, and b*. The null hypothesis of the study was that the performance of laser-assisted bleaching would not be significantly different from that of LED-assisted bleaching.
Materials and Methods
In this in vitro experimental study, the required sample size for each group was calculated to be 10 according to a study by Kiomars et al. [11] using one-way ANOVA power analysis feature of PASS 11, assuming α=0.05, β=0.2, mean standard deviation of 3.09, and effect size of 0.53. The study protocol was approved by the ethics committee of the university (IR.TUMS.DENTISTRY.REC.1398.145). Forty human central incisors and premolars, extracted as part of orthodontic treatment or due to periodontal disease, were used in this study. Teeth with cracks or structural defects were excluded. The teeth were selected by convenience sampling and were then randomly divided (by simple randomization) into four groups (n=10). The specimens were immersed in 0.5% chloramine T solution (Wako Pure Chemical Industry, Osaka, Japan) for 24 hours [10]. To standardize the specimens, the crowns were cut at 2 mm below the cementoenamel junction and were inspected under a stereomicroscope at x10 magnification to ensure their integrity. For standardization of the smear layer and creation of a smooth surface, the specimens were mounted in putty (Speedex, Coltene, Switzerland) from their palatal surface such that their buccal surface remained exposed. The tooth enamel was polished with 1200-grit abrasive paper (Soflex,3M Espe, USA) and polishing paste with 0.1 µm diamond particles (Diamond Paste; Jota Ruthi, Switzerland), and inspected again under a microscope to ensure no dentin exposure. Before bleaching treatment, the teeth were immersed in artificial saliva with the composition of 0.103 g/L CaCl2, 0.019 g/L MgCl2.6H2O, 0.544 g/L KH2PO4, 2.24 g/L KCL, and 0.650 g/L KOH at 37°C. A spectrophotometer (Spectroshade; MHD, Verona, Italy) was used to measure the color parameters at the center of the incisal, middle, and cervical thirds of the buccal surface three times for each specimen, and the mean values were calculated and reported. Next, to standardize the tooth color, 1% sodium hypochlorite (DATERRA; Manipulation Pharmacy, Ribeirão Preto, SP, Brazil) was used for 30 minutes to eliminate the external stains and discolorations. Enamel was then etched with 37% phosphoric acid (Scotchbond Universal Etchant, 3M ESPE, St. Paul, MN, USA) for 6 seconds, and rinsed with water for 30 seconds. Afterwards, 2 g of loose tea (Lipton Black Tea, Unilever, UK) was added to 100 mL of distilled water (Ebne Sina, Pars Peyvand, Iran) and heated for 10 minutes until boiling. The solution was filtered through a sterile gauze and allowed to cool down. The teeth were immersed in this solution for 6 days. The solution was refreshed every 24 hours [10]. The teeth were then randomly divided into 4 groups (n=10):
- The teeth in group 1 were subjected to bleaching with White Smile (Mani Schortz Co., Germany) containing 40% hydrogen peroxide (its concentration reaches 32% after mixing with accelerator). The bleaching agent was applied in 1.5 mm thickness, and subjected to Monitex LED activation [4 blue lights (420-490 nm) and 1 red light (620 to 630 nm)] (Whiten MAX, Taiwan) with 3 W/cm2 power at the closest distance from the tooth surface (1 mm distance) for 20 minutes. This process was repeated one more time (a total of 40 minutes).
- In group 2, Opalescence Boost (Ultradent, South Jordan, UT, USA) containing 40% hydrogen
- peroxide was used for bleaching of the teeth in 1.5 mm thickness two times, each time for 20 minutes (for a total of 40 minutes). This group served as the control group.
- In group 3, the teeth were bleached with Opalescence Boost and Monitex LED with the same parameters as in group 1.
- In group 4, the teeth were bleached with Opalescence Boost (40% hydrogen peroxide) which was applied on the tooth surface in 1.5 mm thickness and activated by diode laser irradiation (Wiser, Doctor Smile, Italy) with 980 nm wavelength, 2 W/cm2 power density, and single tooth tip with 7 mm diameter in continuous-wave mode with 2 mm distance from the surface for 30 seconds, followed by a 1-minute interval. This process was repeated two more times (90 seconds of irradiation with 2-minute intervals for a total of 3.5 minutes). Finally, the gel remained on the tooth surface for 7 minutes (a total of 10.5 minutes).
The color parameters of the teeth were measured by a spectrophotometer (Spectroshade, MHD, Verona, Italy) according to the VITA system at baseline (before staining), after staining, immediately after bleaching, and 1 week after bleaching at the incisal, middle, and cervical thirds. The samples were stored in artificial saliva until the experiment. Finally, the ∆E of the specimens was calculated using the CIE 1976 formula by MATLAB software.
(ΔE = [(La -Lb) 2 + (aa -ab) 2 + (ba -bb*) 2] 1/2
Statistical analysis:
Data were analyzed using SPSS version 25. The measures of central dispersion (mean, standard deviation, minimum, and maximum values) of the L*a*b* color parameters of the teeth and the overall ∆E were reported separately for the four bleaching protocols at different time points for the incisal, middle, and cervical thirds. The four bleaching protocols were compared regarding the changes in value (∆L), a (∆a), and b (∆b) parameters at different time points by one-way ANOVA. Pairwise comparisons were performed by the Tukey’s post-hoc test. P<0.05 was considered statistically significant.
Results
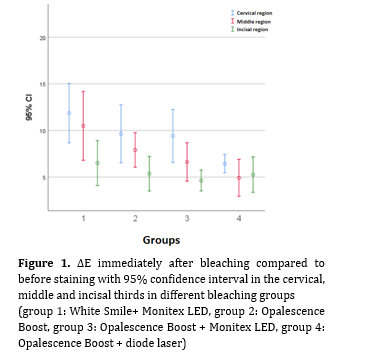
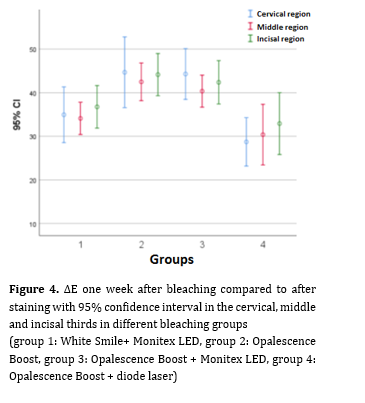
One-way ANOVA showed significant ∆E in all groups towards correction of discoloration. The overall ∆E in the cervical third was greater than that in the middle and incisal thirds. According to the results of one-way ANOVA, significant differences were found in ∆E among different groups immediately after bleaching compared to before bleaching in the cervical (P=0.000), middle (P=0.000) and incisal thirds of the teeth (P=0.000). Also, significant differences were found in ∆E among different groups after one week compared to before bleaching in the cervical third (P=0.002), middle third (P=0.000) and incisal third (P=0.000), immediately after bleaching compared to after staining in the cervical third (P=0.000), middle third (P=0.000) and incisal third (P=0.000), and also after one week compared to after staining in the cervical third (P=0.00), middle third (P=0.00), and incisal third (P=0.00). Figures 1 to 4 indicate ∆E of the four groups at different time points.
Figure 1. ∆E immediately after bleaching compared to before staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
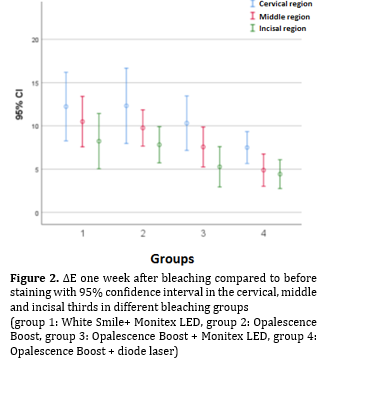
Figure 2. ∆E one week after bleaching compared to before staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
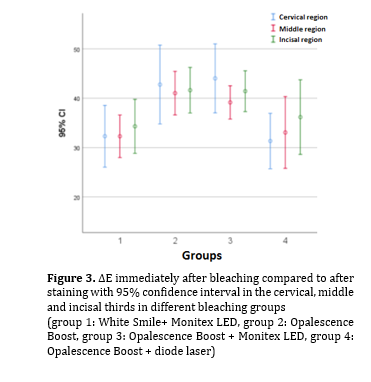
Figure 3. ∆E immediately after bleaching compared to after staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
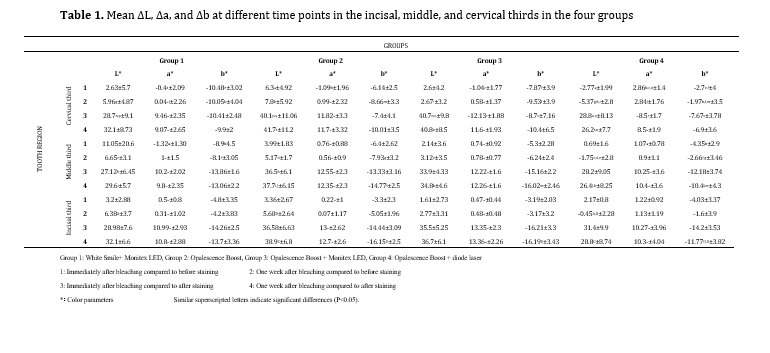
In groups 1-3, ∆a and ∆b values were significant in the incisal, middle, and cervical thirds immediately and 1 week after bleaching compared with before bleaching, and also immediately and 1 week after bleaching compared with after staining, indicating a shift towards greenness (for ∆a) and blueness (for ∆b), resulting in correction of discoloration. In group 4, ∆a was significant at one week after bleaching compared with after staining in the incisal, middle, and cervical thirds, indicating a shift towards greenness and correction of staining. However, other comparisons showed changes towards yellowness, causing aggravation of staining. The ∆b in the incisal, middle, and cervical thirds showed changes towards correction of discoloration (shift to blueness) (Table 1).
Figure 4. ∆E one week after bleaching compared to after staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
Table 1. Mean ∆L, ∆a, and ∆b at different time points in the incisal, middle, and cervical thirds in the four groups
In group 1, ∆L (changes in value) in the incisal, middle, and cervical thirds showed a change towards tooth shade lightening. ∆L in groups 2 and 3 also exhibited changes towards lightening of the tooth shade. In group 4, ∆L in the incisal, middle, and cervical thirds showed a change towards tooth shade lightening at 1 week after bleaching compared with after staining. Other comparisons showed changes towards darkening of the tooth shade (Table 1).
Table 1 shows pairwise comparisons of the groups at different time points by the Tukey’s test. As shown, maximum significant difference at different time points was recorded in the cervical third.
Discussion
The efficacy of laser-assisted bleaching has always been a controversial topic. Lasers with various wavelengths (810-980 nm) have been used for bleaching treatments. In some cases, laser-assisted bleaching has not shown promising results especially when the laser wavelength was out of the normal wavelength range [13]. For laser-assisted bleaching, the gel must contain a suitable absorber that matches the light wavelength used to activate the gel. In addition, special filtering materials are used to conserve energy inside the gel and prevent pulpal temperature rise [14]. The safety of the bleaching procedure may be improved as such [15].
The main effects of laser energy are its photo-thermal effects, which can enhance and accelerate tooth bleaching and absorption of bleaching agent by converting the radiation energy to heat. This absorption, however, depends on the laser wavelength and type of bleaching agent [16,17]. In recent years, diode laser in 810 to 980 nm wavelengths has been used for laser-assisted bleaching [16]. Thus, 980 nm diode laser with 1.5 W power was used in the present study.
It appears that type of bleaching agent and its method of application greatly affect the color change. In the present study, White Smile gel containing 40% hydrogen peroxide (reaches 32% after mixing with accelerator) was used. It has yellow pigments, which absorb LED red light at 630 nm wavelength to yield more favorable bleaching results. Ontiveros and Paravina [18] evaluated the efficacy of bleaching with 25% hydrogen peroxide with/without light activation by technical (CIE L*a*b*) and visual (Bleached guide 3D Master by Vita) assessments. They found that bleaching with light activation at 400-700 nm wavelength (power bleaching) yielded more favorable results compared with conventional bleaching, which was almost in agreement with the present findings, probably because the wavelength of light in their study was similar to the wavelength of Monitex in the present study. Some other studies also showed that power bleaching increased the efficacy of hydrogen peroxide and decreased the time required for bleaching [19,20].
In the present study, the changes in value (∆L) in the middle and cervical thirds were the same in all groups after bleaching compared with before staining, indicating a shift towards an improvement in lightness. However, in the incisal third, Opalescence Boost showed a superior efficacy compared with laser-assisted Boost. Regarding ∆a, the results showed that laser-assisted Opalescence Boost had the lowest efficacy in all areas, except in the incisal third, with respect to reduction of discoloration; however, all other modalities corrected the discolorations. Regarding ∆b, laser-assisted Opalescence Boost showed the lowest efficacy for correction of discoloration in all areas, except in the incisal third. However, other modalities decreased discolorations.
Kwon et al. [21] evaluated the efficacy of laser-assisted bleaching with Opalescence Boost, and reported maximum ∆E in the Opalescence Boost group (40% hydrogen peroxide gel) activated by 810 nm laser compared with the conventional gel (40% hydrogen peroxide gel). They explained that laser heat causes greater and faster activation of the conventional gel, and results in greater generation of singlet oxygen. However, in the present study, Opalescence Boost activated by diode laser caused lower color change compared with the control group. The reason may be that Opalescence Boost does not have a specific pigment for absorption of 980 nm diode laser. Thus, application of laser decreased its efficacy. Therefore, difference in the results of the two studies may be due to the differences in laser wavelengths and application times.
A randomized single-blinded controlled clinical trial showed that there was no statistically significant difference among laser-activated bleaching, light-activated bleaching, and chemical-activated bleaching regarding color change; but laser-activated bleaching had the best color stability over time and may be suitable for patients who seek favorable results with a shorter chair time [22]. However, they used very high power (7 W) laser, which may explain their different result. Therefore, laser parameters can serve as an important factor as shown by Papadopoulou et al [23].
In the current study, all modalities showed similar ∆L at 1 week after bleaching compared with baseline, indicating a shift towards tooth shade lightening, except in the cervical third, where laser-assisted Opalescence Boost had a lower performance than other modalities.
The results regarding the stability of bleaching results are controversial, and precise comparisons are not possible due to the use of different measurement techniques of color parameters [24,25]. Bernardone et al. [26] evaluated the clinical efficacy of in-office and at-home vital bleaching techniques with/without using LED/laser light. They showed that all techniques were effective for tooth bleaching and after 2 weeks, the level of bleaching was the same in all groups. Color stability was acceptable during a 16-week period. He et al. [27] evaluated the effects of light activation on the efficacy of vital in-office bleaching in a systematic review. They indicated that in use of low concentrations of hydrogen peroxide (15-20%), LED- and laser-activated bleaching systems yielded more favorable immediate results compared with the conventional systems without light activation. However, in use of high concentrations of hydrogen peroxide (25-35%), no significant difference was noted between the light-activated and conventional bleaching, neither immediately after bleaching nor in the short-term. Hahn et al. [28] evaluated the color stability of teeth after light-activated bleaching by using NM530 halogen light, 980 nm diode laser (KaVo Laser), and 480 nm LED (Elipar Free Light 2), versus chemical activation (38% hydrogen peroxide, Opalescence Xtra Boost) for up to 3 months after treatment. They found that light activation of bleaching agent had no positive effect on color change up to 3 months after bleaching. Also, the esthetic results were the same in the conventional and light-activated bleaching groups and all modalities, except for activation with LED, caused whitening of teeth over time. Difference between their findings and the present results can be due to different application parameters such as LED wavelengths in the two studies.
Torres et al. [29] evaluated the color change of teeth over time following light-activated bleaching using hybrid 470-830 nm LED light and infrared low-level diode laser (795-830 nm). They reported significant ∆E in the first 2 weeks compared with baseline and also at 12 months after bleaching. They concluded that light-activation of bleaching gel with LED and diode laser yielded superior and faster results compared with the conventional activation of bleaching gel without light activation. It appears that heat generation by light activation was responsible for this finding, which causes faster generation of singlet oxygen by the bleaching agent. However, low-level diode laser irradiation for activation had no significant effect on ∆E. Thus, their results in the short-term were in line with the present findings; however, the results deteriorated after one year.
Regarding the ∆a in the present study, laser-assisted Opalescence Boost in all three regions showed the lowest efficacy for correction of discoloration; other modalities decreased the discolorations. Regarding the ∆b, laser-assisted Opalescence Boost showed the poorest performance in correction of discoloration in all three areas (except for the incisal third). Other modalities decreased discoloration. It appears that light activation has no significant effect on Opalescence Boost because it has no specific pigment for absorption of 980 nm diode laser. Thus, application of laser decreased its efficacy. Kiomars et al. [11] evaluated the color change of teeth and efficacy of bleaching systems activated by 810 and 980 nm diode laser. They used Heydent bleaching agent (30% hydrogen peroxide), which contains titanium oxide. Also, they used Opalescence Boost bleaching agent containing 40% hydrogen peroxide as the control group, similar to the present study. They found that bleaching with different diode laser wavelengths yielded relatively similar results, and all techniques were equally effective for tooth bleaching. In their study, the control group (Opalescence Boost) experienced greater color change and caused higher tooth whitening probably due to longer duration of application of gel on the tooth surface and high concentration of hydrogen peroxide in Opalescence Boost.
Gurgan et al. [19] clinically assessed the effect of bleaching treatments by using 810 nm diode laser, Biolase, LED and Opalescence Boost bleaching agent. They found that LaserWhite along with 810 nm laser (Biolase) caused greater color change. The reason appears to be the faster release of singlet oxygen by the bleaching gel through the activity of light absorbing pigments [30,31], and dehydration of tooth surface due to the use of light source, which causes the teeth to appear whiter [19]. Fekrazad et al. [12] evaluated the efficacy of bleaching with Opalescence Xtra Boost and laser-assisted bleaching by using LaserWhite + 810 nm diode laser (Laser Smile). They found that laser-assisted bleaching had a superior efficacy compared with conventional bleaching with regard to ∆E. Dionysopoulos et al. [10] evaluated the efficacy of bleaching with Er,Cr:YSGG laser and conventional bleaching, and found that laser-assisted bleaching with 35% hydrogen peroxide had higher efficacy than conventional bleaching (use of hydrogen peroxide alone). This result is explained by the fact that the heat generated by light activation causes faster generation of singlet oxygen [31,32]. The difference between their results and the present findings may be due to the use of different materials and different concentrations of bleaching agents.
In general, it may be stated that several factors are involved in obtaining controversial results regarding the efficacy of power bleaching, such as the use of different light sources with different wavelengths and energy levels, distance between the light source and tooth, chemical bleaching agents and their different concentrations, and also different techniques and instruments for assessment of color change. Thus, more comprehensive studies are required for more precise assessments [33].
Conclusion
Within the limitations of this study, the following results were obtained:
(ΔE = [(La -Lb) 2 + (aa -ab) 2 + (ba -bb*) 2] 1/2
Statistical analysis:
Data were analyzed using SPSS version 25. The measures of central dispersion (mean, standard deviation, minimum, and maximum values) of the L*a*b* color parameters of the teeth and the overall ∆E were reported separately for the four bleaching protocols at different time points for the incisal, middle, and cervical thirds. The four bleaching protocols were compared regarding the changes in value (∆L), a (∆a), and b (∆b) parameters at different time points by one-way ANOVA. Pairwise comparisons were performed by the Tukey’s post-hoc test. P<0.05 was considered statistically significant.
Results
One-way ANOVA showed significant ∆E in all groups towards correction of discoloration. The overall ∆E in the cervical third was greater than that in the middle and incisal thirds. According to the results of one-way ANOVA, significant differences were found in ∆E among different groups immediately after bleaching compared to before bleaching in the cervical (P=0.000), middle (P=0.000) and incisal thirds of the teeth (P=0.000). Also, significant differences were found in ∆E among different groups after one week compared to before bleaching in the cervical third (P=0.002), middle third (P=0.000) and incisal third (P=0.000), immediately after bleaching compared to after staining in the cervical third (P=0.000), middle third (P=0.000) and incisal third (P=0.000), and also after one week compared to after staining in the cervical third (P=0.00), middle third (P=0.00), and incisal third (P=0.00). Figures 1 to 4 indicate ∆E of the four groups at different time points.
Figure 1. ∆E immediately after bleaching compared to before staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
{kind=link}
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
Figure 2. ∆E one week after bleaching compared to before staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
{kind=link}
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
Figure 3. ∆E immediately after bleaching compared to after staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
{kind=link}
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
In groups 1-3, ∆a and ∆b values were significant in the incisal, middle, and cervical thirds immediately and 1 week after bleaching compared with before bleaching, and also immediately and 1 week after bleaching compared with after staining, indicating a shift towards greenness (for ∆a) and blueness (for ∆b), resulting in correction of discoloration. In group 4, ∆a was significant at one week after bleaching compared with after staining in the incisal, middle, and cervical thirds, indicating a shift towards greenness and correction of staining. However, other comparisons showed changes towards yellowness, causing aggravation of staining. The ∆b in the incisal, middle, and cervical thirds showed changes towards correction of discoloration (shift to blueness) (Table 1).
Figure 4. ∆E one week after bleaching compared to after staining with 95% confidence interval in the cervical, middle and incisal thirds in different bleaching groups
{kind=link}
(group 1: White Smile+ Monitex LED, group 2: Opalescence Boost, group 3: Opalescence Boost + Monitex LED, group 4: Opalescence Boost + diode laser)
Table 1. Mean ∆L, ∆a, and ∆b at different time points in the incisal, middle, and cervical thirds in the four groups
{kind=link}
In group 1, ∆L (changes in value) in the incisal, middle, and cervical thirds showed a change towards tooth shade lightening. ∆L in groups 2 and 3 also exhibited changes towards lightening of the tooth shade. In group 4, ∆L in the incisal, middle, and cervical thirds showed a change towards tooth shade lightening at 1 week after bleaching compared with after staining. Other comparisons showed changes towards darkening of the tooth shade (Table 1).
Table 1 shows pairwise comparisons of the groups at different time points by the Tukey’s test. As shown, maximum significant difference at different time points was recorded in the cervical third.
Discussion
The efficacy of laser-assisted bleaching has always been a controversial topic. Lasers with various wavelengths (810-980 nm) have been used for bleaching treatments. In some cases, laser-assisted bleaching has not shown promising results especially when the laser wavelength was out of the normal wavelength range [13]. For laser-assisted bleaching, the gel must contain a suitable absorber that matches the light wavelength used to activate the gel. In addition, special filtering materials are used to conserve energy inside the gel and prevent pulpal temperature rise [14]. The safety of the bleaching procedure may be improved as such [15].
The main effects of laser energy are its photo-thermal effects, which can enhance and accelerate tooth bleaching and absorption of bleaching agent by converting the radiation energy to heat. This absorption, however, depends on the laser wavelength and type of bleaching agent [16,17]. In recent years, diode laser in 810 to 980 nm wavelengths has been used for laser-assisted bleaching [16]. Thus, 980 nm diode laser with 1.5 W power was used in the present study.
It appears that type of bleaching agent and its method of application greatly affect the color change. In the present study, White Smile gel containing 40% hydrogen peroxide (reaches 32% after mixing with accelerator) was used. It has yellow pigments, which absorb LED red light at 630 nm wavelength to yield more favorable bleaching results. Ontiveros and Paravina [18] evaluated the efficacy of bleaching with 25% hydrogen peroxide with/without light activation by technical (CIE L*a*b*) and visual (Bleached guide 3D Master by Vita) assessments. They found that bleaching with light activation at 400-700 nm wavelength (power bleaching) yielded more favorable results compared with conventional bleaching, which was almost in agreement with the present findings, probably because the wavelength of light in their study was similar to the wavelength of Monitex in the present study. Some other studies also showed that power bleaching increased the efficacy of hydrogen peroxide and decreased the time required for bleaching [19,20].
In the present study, the changes in value (∆L) in the middle and cervical thirds were the same in all groups after bleaching compared with before staining, indicating a shift towards an improvement in lightness. However, in the incisal third, Opalescence Boost showed a superior efficacy compared with laser-assisted Boost. Regarding ∆a, the results showed that laser-assisted Opalescence Boost had the lowest efficacy in all areas, except in the incisal third, with respect to reduction of discoloration; however, all other modalities corrected the discolorations. Regarding ∆b, laser-assisted Opalescence Boost showed the lowest efficacy for correction of discoloration in all areas, except in the incisal third. However, other modalities decreased discolorations.
Kwon et al. [21] evaluated the efficacy of laser-assisted bleaching with Opalescence Boost, and reported maximum ∆E in the Opalescence Boost group (40% hydrogen peroxide gel) activated by 810 nm laser compared with the conventional gel (40% hydrogen peroxide gel). They explained that laser heat causes greater and faster activation of the conventional gel, and results in greater generation of singlet oxygen. However, in the present study, Opalescence Boost activated by diode laser caused lower color change compared with the control group. The reason may be that Opalescence Boost does not have a specific pigment for absorption of 980 nm diode laser. Thus, application of laser decreased its efficacy. Therefore, difference in the results of the two studies may be due to the differences in laser wavelengths and application times.
A randomized single-blinded controlled clinical trial showed that there was no statistically significant difference among laser-activated bleaching, light-activated bleaching, and chemical-activated bleaching regarding color change; but laser-activated bleaching had the best color stability over time and may be suitable for patients who seek favorable results with a shorter chair time [22]. However, they used very high power (7 W) laser, which may explain their different result. Therefore, laser parameters can serve as an important factor as shown by Papadopoulou et al [23].
In the current study, all modalities showed similar ∆L at 1 week after bleaching compared with baseline, indicating a shift towards tooth shade lightening, except in the cervical third, where laser-assisted Opalescence Boost had a lower performance than other modalities.
The results regarding the stability of bleaching results are controversial, and precise comparisons are not possible due to the use of different measurement techniques of color parameters [24,25]. Bernardone et al. [26] evaluated the clinical efficacy of in-office and at-home vital bleaching techniques with/without using LED/laser light. They showed that all techniques were effective for tooth bleaching and after 2 weeks, the level of bleaching was the same in all groups. Color stability was acceptable during a 16-week period. He et al. [27] evaluated the effects of light activation on the efficacy of vital in-office bleaching in a systematic review. They indicated that in use of low concentrations of hydrogen peroxide (15-20%), LED- and laser-activated bleaching systems yielded more favorable immediate results compared with the conventional systems without light activation. However, in use of high concentrations of hydrogen peroxide (25-35%), no significant difference was noted between the light-activated and conventional bleaching, neither immediately after bleaching nor in the short-term. Hahn et al. [28] evaluated the color stability of teeth after light-activated bleaching by using NM530 halogen light, 980 nm diode laser (KaVo Laser), and 480 nm LED (Elipar Free Light 2), versus chemical activation (38% hydrogen peroxide, Opalescence Xtra Boost) for up to 3 months after treatment. They found that light activation of bleaching agent had no positive effect on color change up to 3 months after bleaching. Also, the esthetic results were the same in the conventional and light-activated bleaching groups and all modalities, except for activation with LED, caused whitening of teeth over time. Difference between their findings and the present results can be due to different application parameters such as LED wavelengths in the two studies.
Torres et al. [29] evaluated the color change of teeth over time following light-activated bleaching using hybrid 470-830 nm LED light and infrared low-level diode laser (795-830 nm). They reported significant ∆E in the first 2 weeks compared with baseline and also at 12 months after bleaching. They concluded that light-activation of bleaching gel with LED and diode laser yielded superior and faster results compared with the conventional activation of bleaching gel without light activation. It appears that heat generation by light activation was responsible for this finding, which causes faster generation of singlet oxygen by the bleaching agent. However, low-level diode laser irradiation for activation had no significant effect on ∆E. Thus, their results in the short-term were in line with the present findings; however, the results deteriorated after one year.
Regarding the ∆a in the present study, laser-assisted Opalescence Boost in all three regions showed the lowest efficacy for correction of discoloration; other modalities decreased the discolorations. Regarding the ∆b, laser-assisted Opalescence Boost showed the poorest performance in correction of discoloration in all three areas (except for the incisal third). Other modalities decreased discoloration. It appears that light activation has no significant effect on Opalescence Boost because it has no specific pigment for absorption of 980 nm diode laser. Thus, application of laser decreased its efficacy. Kiomars et al. [11] evaluated the color change of teeth and efficacy of bleaching systems activated by 810 and 980 nm diode laser. They used Heydent bleaching agent (30% hydrogen peroxide), which contains titanium oxide. Also, they used Opalescence Boost bleaching agent containing 40% hydrogen peroxide as the control group, similar to the present study. They found that bleaching with different diode laser wavelengths yielded relatively similar results, and all techniques were equally effective for tooth bleaching. In their study, the control group (Opalescence Boost) experienced greater color change and caused higher tooth whitening probably due to longer duration of application of gel on the tooth surface and high concentration of hydrogen peroxide in Opalescence Boost.
Gurgan et al. [19] clinically assessed the effect of bleaching treatments by using 810 nm diode laser, Biolase, LED and Opalescence Boost bleaching agent. They found that LaserWhite along with 810 nm laser (Biolase) caused greater color change. The reason appears to be the faster release of singlet oxygen by the bleaching gel through the activity of light absorbing pigments [30,31], and dehydration of tooth surface due to the use of light source, which causes the teeth to appear whiter [19]. Fekrazad et al. [12] evaluated the efficacy of bleaching with Opalescence Xtra Boost and laser-assisted bleaching by using LaserWhite + 810 nm diode laser (Laser Smile). They found that laser-assisted bleaching had a superior efficacy compared with conventional bleaching with regard to ∆E. Dionysopoulos et al. [10] evaluated the efficacy of bleaching with Er,Cr:YSGG laser and conventional bleaching, and found that laser-assisted bleaching with 35% hydrogen peroxide had higher efficacy than conventional bleaching (use of hydrogen peroxide alone). This result is explained by the fact that the heat generated by light activation causes faster generation of singlet oxygen [31,32]. The difference between their results and the present findings may be due to the use of different materials and different concentrations of bleaching agents.
In general, it may be stated that several factors are involved in obtaining controversial results regarding the efficacy of power bleaching, such as the use of different light sources with different wavelengths and energy levels, distance between the light source and tooth, chemical bleaching agents and their different concentrations, and also different techniques and instruments for assessment of color change. Thus, more comprehensive studies are required for more precise assessments [33].
Conclusion
Within the limitations of this study, the following results were obtained:
- All bleaching techniques caused color change in teeth.
- Laser-assisted Opalescence Boost showed the poorest performance with respect to changes in lightness.
- Conventional Opalescence Boost, Opalescence Boost activated by Monitex, and White Smile showed similar efficacy regarding changes in lightness.
- No significant change was noted in the groups regarding ∆a and ∆b, and the changes were in the range of lower chroma. All groups had a similar performance in this respect.
Type of Study: Original article |
Subject:
Restorative Dentistry
References
1. Atali PY, Topbaşi FB. The effect of different bleaching methods on the surface roughness and hardness of resin composites. J Dent Oral Hyg. 2011 Feb 28;3(2):10-7.
2. Khoroushi M, Fardashtaki SR. Effect of light-activated bleaching on the microleakage of Class V tooth-colored restorations. Oper Dent. 2009 Sep-Oct;34(5):565-70. [DOI:10.2341/08-050-L] [PMID]
3. Haywood VB, Heymann HO. Nightguard vital bleaching. Quintessence Int. 1989 Mar;20(3):173-6.
4. Haywood VB. History, safety, and effectiveness of current bleaching techniques and applications of the nightguard vital bleaching technique. Quintessence Int. 1992 Jul;23(7):471-88.
5. McCaslin AJ, Haywood VB, Potter BJ, Dickinson GL, Russell CM. Assessing dentin color changes from nightguard vital bleaching. J Am Dent Assoc. 1999 Oct;130(10):1485-90. [DOI:10.14219/jada.archive.1999.0061] [PMID]
6. Summit J, Robbins J, Hilton T, Schwartz R. Fundamentals of Operative Dentistry. Third Ed. Quintessence Publishing Co. 2006;Chap15:437-457.
7. Buchalla W, Attin T. External bleaching therapy with activation by heat, light or laser--a systematic review. Dent Mater. 2007 May;23(5):586-96. [DOI:10.1016/j.dental.2006.03.018] [PMID]
8. Chu SJ, Trushkowsky RD, Paravina RD. Dental color matching instruments and systems. Review of clinical and research aspects. J Dent. 2010;38 Suppl 2:e2-16. [DOI:10.1016/j.jdent.2010.07.001] [PMID]
9. Adobe systems Incorporated: Hand book Adobe Photoshop CS5. Boenningstedt. Software-service GmbH 2010;65-80.
10. Dionysopoulos D, Strakas D, Tolidis K, Tsitrou E, Koumpia E, Koliniotou-Koumpia E. Spectrophotometric analysis of the effectiveness of a novel in-office laser-assisted tooth bleaching method using Er,Cr:YSGG laser. Lasers Med Sci. 2017 Nov;32(8):1811-8. [DOI:10.1007/s10103-017-2274-y] [PMID]
11. Kiomars N, Azarpour P, Mirzaei M, Hashemi Kamangar SS, Kharazifard MJ, Chiniforush N. Evaluation of the Diode laser (810nm, 980 nm) on color change of teeth after external bleaching. Laser Ther. 2016 Dec 30;25(4):267-2. [DOI:10.5978/islsm.16-OR-21] [PMID] []
12. Fekrazad R, Alimazandarani S, Kalhori KA, Assadian H, Mirmohammadi SM. Comparison of laser and power bleaching techniques in tooth color change. J Clin Exp Dent. 2017 Apr 1;9(4):e511-e515. [DOI:10.4317/jced.53435] [PMID] []
13. Coluzzi DJ. Fundamentals of dental lasers: science and instruments. Dent Clin North Am. 2004 Oct;48(4):751-70, v. [DOI:10.1016/j.cden.2004.05.003] [PMID]
14. Zach L, Cohen G. Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol. 1965 Apr;19:515-30. [DOI:10.1016/0030-4220(65)90015-0] [PMID]
15. Lin LC, Pitts DL, Burgess LW Jr. An investigation into the feasibility of photobleaching tetracycline-stained teeth. J Endod. 1988 Jun;14(6):293-9. [DOI:10.1016/S0099-2399(88)80029-3] [PMID]
16. Gontijo IT, Navarro RS, Ciamponi AL, Miyakawa W, Zezell DM. Color and surface temperature variation during bleaching in human devitalized primary teeth: an in vitro study. J Dent Child (Chic). 2008 Sep-Dec;75(3):229-34.
17. Garber DA. Dentist-monitored bleaching: a discussion of combination and laser bleaching. J Am Dent Assoc. 1997 Apr;128 Suppl:26S-30S. [DOI:10.14219/jada.archive.1997.0419] [PMID]
18. Ontiveros JC, Paravina RD. Color change of vital teeth exposed to bleaching performed with and without supplementary light. J Dent. 2009 Nov;37(11):840-7. [DOI:10.1016/j.jdent.2009.06.015] [PMID]
19. Gurgan S, Cakir FY, Yazici E. Different light-activated in-office bleaching systems: a clinical evaluation. Lasers Med Sci. 2010 Nov;25(6):817-22. [DOI:10.1007/s10103-009-0688-x] [PMID]
20. Mena-Serrano AP, Garcia E, Luque-Martinez I, Grande R, Loguercio AD, Reis A. A Single-Blind Randomized Trial About the Effect of Hydrogen Peroxide Concentration on Light-Activated Bleaching. Oper Dent. 2016 Sep-Oct;41(5):455-64. [DOI:10.2341/15-077-C] [PMID]
21. Kwon SR, Oyoyo U, Li Y. Effect of light activation on tooth whitening efficacy and hydrogen peroxide penetration: an in vitro study. J Dent. 2013 Aug;41 Suppl 3:e39-45. [DOI:10.1016/j.jdent.2012.12.003] [PMID]
22. Alghonaimy H, Fayed AM, Elzayat IM, Khairy AE. Comparison Between Color Stability and post bleaching hypersensitivity of Different Bleaching Protocols-Randomized single-blinded Controlled Clinical Trial. Egyptian Dental Journal. 2021 Oct 67(4):3663-76. [DOI:10.21608/edj.2021.78326.1654]
23. Papadopoulou A, Dionysopoulos D, Strakas D, Kouros P, Vamvakoudi E, Tsetseli P, Kolokitha OE, Tolidis K. Exploring the efficacy of laser-assisted in-office tooth bleaching: A study on varied irradiation times and power settings utilizing a diode laser (445 nm). J Photochem Photobiol B. 2024 Aug;257:112970. [DOI:10.1016/j.jphotobiol.2024.112970] [PMID]
24. Tay LY, Kose C, Herrera DR, Reis A, Loguercio AD. Long-term efficacy of in-office and at-home bleaching: a 2-year double-blind randomized clinical trial. Am J Dent. 2012 Aug;25(4): 199-204.
25. Meireles SS, Santos IS, Bona AD, Demarco FF. A double-blind randomized clinical trial of two carbamide peroxide tooth bleaching agents: 2-year follow-up. J Dent. 2010 Dec;38(12):956-63. [DOI:10.1016/j.jdent.2010.08.003] [PMID]
26. Bernardon JK, Sartori N, Ballarin A, Perdigão J, Lopes GC, Baratieri LN. Clinical performance of vital bleaching techniques. Oper Dent. 2010 Jan-Feb;35(1):3-10. [DOI:10.2341/09-008CR] [PMID]
27. He LB, Shao MY, Tan K, Xu X, Li JY. The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: a systematic review and meta-analysis. J Dent. 2012 Aug;40(8):644-53. [DOI:10.1016/j.jdent.2012.04.010] [PMID]
28. Hahn P, Schondelmaier N, Wolkewitz M, Altenburger MJ, Polydorou O. Efficacy of tooth bleaching with and without light activation and its effect on the pulp temperature: an in vitro study. Odontology. 2013 Jan;101(1):67-74. [DOI:10.1007/s10266-012-0063-4] [PMID]
29. Torres CR, Barcellos DC, Batista GR, Borges AB, Cassiano KV, Pucci CR. Assessment of the effectiveness of light-emitting diode and diode laser hybrid light sources to intensify dental bleaching treatment. Acta Odontol Scand. 2011 May;69(3): 176-81. [DOI:10.3109/00016357.2010.549503] [PMID]
30. Sulieman M, MacDonald E, Rees JS, Addy M. Comparison of three in-office bleaching systems based on 35% hydrogen peroxide with different light activators. Am J Dent. 2005 Jun;18(3):194-7.
31. Joiner A. Tooth colour: a review of the literature. J Dent. 2004;32 Suppl 1:3-12. [DOI:10.1016/j.jdent.2003.10.013] [PMID]
32. Joiner A. The bleaching of teeth: a review of the literature. J Dent. 2006 Aug;34(7):412-9. [DOI:10.1016/j.jdent.2006.02.002] [PMID]
33. Luk K, Tam L, Hubert M. Effect of light energy on peroxide tooth bleaching. J Am Dent Assoc. 2004 Feb;135(2):194-201; quiz 228-9. [DOI:10.14219/jada.archive.2004.0151] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |