Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 4 (12-2024)
J Res Dent Maxillofac Sci 2024, 9(4): 287-296 |
Back to browse issues page


Ethics code: Ref.no/DRI/IMS.SH/2021/664
Clinical trials code: NA
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kumari K S, Gaur M, Dixit S, Dash P, Subudh E. Nutritional Types and Drug Resistance Profiling of Microbiota Harboring Dental Root Canal of Patients with Apical Periodontitis. J Res Dent Maxillofac Sci 2024; 9 (4) :287-296
URL: http://jrdms.dentaliau.ac.ir/article-1-652-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-652-en.html



1- Institute of Dental Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Bhubaneswar 751003, India
2- Centre for Biotechnology, School of Pharmaceutical Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Kalinga Nagar, Ghatikia, Bhubaneswar-751029, Odisha, India
2- Centre for Biotechnology, School of Pharmaceutical Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Kalinga Nagar, Ghatikia, Bhubaneswar-751029, Odisha, India
Full-Text [PDF 553 kb]
(702 Downloads)
| Abstract (HTML) (2035 Views)
Full-Text: (1593 Views)
Abstract
Background and Aim: Identification of harbored bacteria and their resistance profile is crucial to manage endodontic treatment. This study aimed to assess the nutritional types and drug resistance profiling of microbiota harboring dental root canal of patients with apical periodontitis.
Materials and Methods: This cross-sectional study identified bacteria and their resistance profile in 10 samples taken from acute and chronic periodontitis patients using the VITEK 2 system.
Results: A total of 49 bacteria belonging to 24 species were recovered from two sets of 10 samples together with a higher bacterial diversity in chronic periodontitis condition. Enterococcus, Clostridium, Streptococcus, Prevotella and Propionibacterium bacterial species were identified in both cases but Streptococcus, Enterococcus, and Propionibacterium were more prevalent in chronic patients. The prevalence of facultative anaerobes (51.02%) was the highest, and that of obligate aerobes (4.08%) was the lowest; obligate anaerobes accounted for 16.33%, while strict anaerobes accounted for 20.4% in both conditions. Microaerophilic organisms (Lactobacillus species) were found only in persistent apical periodontitis (8.16%); whereas, aerobes were predominant (7.14%) in acute conditions. The majority of the strains were resistant to tetracycline, cefoxitin, and oxacillin but the members of the four predominant genera (Enterococcus, Clostridium, Streptococcus, Propionibacterium) were resistant to penicillin, cefotaxime and cefoxitin. Very few strains exhibited resistance to ofloxacin, vancomycin and gentamycin.
Conclusion: The present results showed that acute and chronic root canal infections were polymicrobial infections, with Enterococcus, Streptococcus and Propionibacterium species being the predominant ones. These predominant bacteria were resistant to penicillin, cefotaxime and cefoxitin.
Keywords: Periapical Periodontitis; Coinfection; Drug Resistance,
Introduction
Materials and Methods: This cross-sectional study identified bacteria and their resistance profile in 10 samples taken from acute and chronic periodontitis patients using the VITEK 2 system.
Results: A total of 49 bacteria belonging to 24 species were recovered from two sets of 10 samples together with a higher bacterial diversity in chronic periodontitis condition. Enterococcus, Clostridium, Streptococcus, Prevotella and Propionibacterium bacterial species were identified in both cases but Streptococcus, Enterococcus, and Propionibacterium were more prevalent in chronic patients. The prevalence of facultative anaerobes (51.02%) was the highest, and that of obligate aerobes (4.08%) was the lowest; obligate anaerobes accounted for 16.33%, while strict anaerobes accounted for 20.4% in both conditions. Microaerophilic organisms (Lactobacillus species) were found only in persistent apical periodontitis (8.16%); whereas, aerobes were predominant (7.14%) in acute conditions. The majority of the strains were resistant to tetracycline, cefoxitin, and oxacillin but the members of the four predominant genera (Enterococcus, Clostridium, Streptococcus, Propionibacterium) were resistant to penicillin, cefotaxime and cefoxitin. Very few strains exhibited resistance to ofloxacin, vancomycin and gentamycin.
Conclusion: The present results showed that acute and chronic root canal infections were polymicrobial infections, with Enterococcus, Streptococcus and Propionibacterium species being the predominant ones. These predominant bacteria were resistant to penicillin, cefotaxime and cefoxitin.
Keywords: Periapical Periodontitis; Coinfection; Drug Resistance,
Introduction
Evidence shows that bacteria can initiate inflammation in pulpal and periapical tissues [1]. Apical periodontitis is a common infectious and inflammatory disease induced by biofilm formation by the bacteria around the root apex, resulting in an endodontic lesion. It possesses a heterogeneous etiology with involvement of multiple bacteria. The involvement of multiple bacteria in disease development and progression has been established. Thus, no single species is often responsible for lesion development [2]. Primary (acute) root canal infections ensue when bacteria gain access, invade the pulp tissue, colonize it, and impair its function [3].
Treatment of these lesions is aimed at elimination of bacteria from the necrotic root canals. Secondary endodontic infections are due to the failure of the previously treated endodontic lesions, mainly because of the persistence of primary infecting microorganisms resisting intracanal antibacterial treatments and their survival in the root canal system post-treatment [4,5]. Infected root canals are predominated by obligate anaerobes [2]. Primary root canal infections exhibit polymicrobial flora with a wide variety of combinations that are predominantly anaerobic and Gram-negative; whereas, in persistent or secondary endodontic infections, the causative bacteria are predominantly facultative anaerobes and Gram-positive species [6].
Moreover, the types and numbers of bacteria present in these two conditions vary depending on race, gender, age, lifestyle, and food habits, including the geographic locations of patients. For a successful endodontic treatment or retreatment, prevention and eradication of infectious agents from the root and periodontal tissues is a primary objective. Therefore, complete information about the microbiota inhabiting these tissues is crucial.
Although advanced molecular methods can reveal the presence of various taxa, including non-cultivable species in periapical disease, they still have pros and cons. The interference of dead bacteria's DNA may bring biased results, which might have played some ecological role through their amplification [7]. Furthermore, presence of some bacteria which access the root canal but cannot grow dynamically may add to the total count [8]. Therefore, although traditional and not free from limitations, the cultivable method of identifying the microflora using a single-step, faster and user-friendly globally accepted VITEK 2 COMPACT system (Biomatrix, USA) may be the most sought-after option [9]. In any tertiary care hospital, these automated analytical methods for identification and antibiotic-resistant profiling are instrumental and, thus, preferred [9].
Since the past decade, human pathogens have been reported to develop resistance due to the non-judicious antibiotic prescriptions for treatment of various infections. Antibiotics at sub-inhibitory concentrations, when absorbed through circulation, may develop resistance in bacteria [2]. As dental infections are polymicrobial, broad-spectrum antibiotics are advised in addition to biomechanical canal preparation to decrease the load of infecting microorganisms. The resistant microbiome isolated from endodontic infections exhibits significant concern. Antibiotic resistance profiles of various endodontic bacterial species make their eradication more complicated. For an endodontic treatment to be successful, it is crucial to be aware of the harbored species of bacteria inside the root canal and to understand their resistance profile.
In the present study, efforts were taken to estimate the differential predominance of bacteria, selecting 10 cases from each of the primary and secondary endodontic treatments from a university teaching dental care center in Odisha, India. Furthermore, the isolates were subjected to antimicrobial susceptibility test to understand the prevailing resistance in them using a range of antibiotics.
Materials and Methods
Treatment of these lesions is aimed at elimination of bacteria from the necrotic root canals. Secondary endodontic infections are due to the failure of the previously treated endodontic lesions, mainly because of the persistence of primary infecting microorganisms resisting intracanal antibacterial treatments and their survival in the root canal system post-treatment [4,5]. Infected root canals are predominated by obligate anaerobes [2]. Primary root canal infections exhibit polymicrobial flora with a wide variety of combinations that are predominantly anaerobic and Gram-negative; whereas, in persistent or secondary endodontic infections, the causative bacteria are predominantly facultative anaerobes and Gram-positive species [6].
Moreover, the types and numbers of bacteria present in these two conditions vary depending on race, gender, age, lifestyle, and food habits, including the geographic locations of patients. For a successful endodontic treatment or retreatment, prevention and eradication of infectious agents from the root and periodontal tissues is a primary objective. Therefore, complete information about the microbiota inhabiting these tissues is crucial.
Although advanced molecular methods can reveal the presence of various taxa, including non-cultivable species in periapical disease, they still have pros and cons. The interference of dead bacteria's DNA may bring biased results, which might have played some ecological role through their amplification [7]. Furthermore, presence of some bacteria which access the root canal but cannot grow dynamically may add to the total count [8]. Therefore, although traditional and not free from limitations, the cultivable method of identifying the microflora using a single-step, faster and user-friendly globally accepted VITEK 2 COMPACT system (Biomatrix, USA) may be the most sought-after option [9]. In any tertiary care hospital, these automated analytical methods for identification and antibiotic-resistant profiling are instrumental and, thus, preferred [9].
Since the past decade, human pathogens have been reported to develop resistance due to the non-judicious antibiotic prescriptions for treatment of various infections. Antibiotics at sub-inhibitory concentrations, when absorbed through circulation, may develop resistance in bacteria [2]. As dental infections are polymicrobial, broad-spectrum antibiotics are advised in addition to biomechanical canal preparation to decrease the load of infecting microorganisms. The resistant microbiome isolated from endodontic infections exhibits significant concern. Antibiotic resistance profiles of various endodontic bacterial species make their eradication more complicated. For an endodontic treatment to be successful, it is crucial to be aware of the harbored species of bacteria inside the root canal and to understand their resistance profile.
In the present study, efforts were taken to estimate the differential predominance of bacteria, selecting 10 cases from each of the primary and secondary endodontic treatments from a university teaching dental care center in Odisha, India. Furthermore, the isolates were subjected to antimicrobial susceptibility test to understand the prevailing resistance in them using a range of antibiotics.
Materials and Methods
Patient selection:
Out of a total of 450 patients who visited the Outdoor Patient’s Department of the Institute of Dental Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Bhubaneswar, Odisha from October 2020 to March 2021, 94 were diagnosed with apical periodontitis and referred to the Department of Conservative Dentistry and Endodontics. They required root canal treatment or retreatment and were considered for further screening according to the inclusion and exclusion criteria of the present study.
Inclusion criteria:
The inclusion criteria for this study were as follows. For primary apical periodontitis, patients with a tooth with periapical radiolucency (single-rooted or multi-rooted) as seen on radiographs, aged from 20 to 70 years were included in this study. Similarly, for secondary apical periodontitis cases, patients with radiographs showing apical radiolucency of endodontically treated teeth performed at least two years earlier aged 20 to 70 years were included in this study.
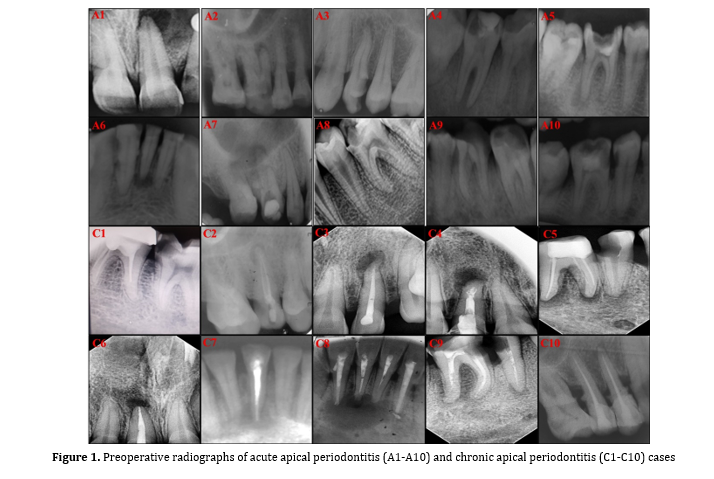
The periapical status of the infected tooth was assessed according to the periapical index (PAI) scoring system [10,11] using a scale ranging from 1 to 5, where score 0 indicates undisturbed or intact periapical bone structure, score 1 indicates periapical radiolucency with a diameter ranging from 0.5 mm to 1 mm, score 2 indicates radiolucency with a diameter ranging from 1 mm to 2 mm, score 3 indicates radiolucency with a diameter ranging from 2 mm to 4 mm, score 4 indicates radiolucency with a diameter ranging from 4 mm to 8 mm, and score 5 indicates radiolucency with a diameter exceeding 8 mm (Figure 1).
In the present study, 2 patients had acute apical periodontitis (A2, A4) with PAI score 1, six patients (A1, A3, A5, A7, A9, A10) had PAI score 2, and 2 patients (A6, A8) had PAI score 3. Four patients (C1, C2, C7, C10) had chronic apical periodontitis with score 1, two patients (C5, C9) had score 2, and 4 patients (C3, C4, C6, C8) had score 3.
Exclusion criteria:
The exclusion criteria for primary apical periodontitis were i) having received antibiotics in the past 3 months, ii) presence of a systemic disease, iii) inability to isolate the involved tooth by rubber dam placement, iv) teeth with curved root in the apical third, v) infected teeth with a periodontal pocket depth more than 4 mm, and vi) pregnant women and lactating mothers. Nevertheless, patients with systemic diseases, either root canal treatment done in the past 2 years or broken endodontic files in any canal, were excluded from the secondary apical periodontitis group.
Based on the above-mentioned criteria, 60 patients were eliminated out of 76 with acute apical periodontitis due to age below 20 years (n=4), inability to perform rubber dam isolation (n=8), teeth with curved root in the apical third (n=7), not interested in participating in the study (n=6), narrow canals with difficult canal negotiation without solvents (n=8), presence of systemic diseases (n=12), antibiotic administration within the past 3 months (n=18), and periodontal pocket depth more than 4 mm (n=3). Similarly, in chronic apical periodontitis group, 8 patients were eliminated out of 18 from the study due to previous root canal therapy done within the past 2 years (n=2), broken endodontic file in involved teeth (n=3), antibiotic administration within the past 3 months (n=2), and presence of systemic disease (n=1). Finally, out of 60 patients, 10 cases from each group of acute and chronic apical periodontitis were selected for inclusion in the present study. The preoperative radiographs of acute apical periodontitis (A1-A10) and chronic apical periodontitis (C1-C10) cases are illustrated in Figure 1.
Out of a total of 450 patients who visited the Outdoor Patient’s Department of the Institute of Dental Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Bhubaneswar, Odisha from October 2020 to March 2021, 94 were diagnosed with apical periodontitis and referred to the Department of Conservative Dentistry and Endodontics. They required root canal treatment or retreatment and were considered for further screening according to the inclusion and exclusion criteria of the present study.
Inclusion criteria:
The inclusion criteria for this study were as follows. For primary apical periodontitis, patients with a tooth with periapical radiolucency (single-rooted or multi-rooted) as seen on radiographs, aged from 20 to 70 years were included in this study. Similarly, for secondary apical periodontitis cases, patients with radiographs showing apical radiolucency of endodontically treated teeth performed at least two years earlier aged 20 to 70 years were included in this study.
The periapical status of the infected tooth was assessed according to the periapical index (PAI) scoring system [10,11] using a scale ranging from 1 to 5, where score 0 indicates undisturbed or intact periapical bone structure, score 1 indicates periapical radiolucency with a diameter ranging from 0.5 mm to 1 mm, score 2 indicates radiolucency with a diameter ranging from 1 mm to 2 mm, score 3 indicates radiolucency with a diameter ranging from 2 mm to 4 mm, score 4 indicates radiolucency with a diameter ranging from 4 mm to 8 mm, and score 5 indicates radiolucency with a diameter exceeding 8 mm (Figure 1).
In the present study, 2 patients had acute apical periodontitis (A2, A4) with PAI score 1, six patients (A1, A3, A5, A7, A9, A10) had PAI score 2, and 2 patients (A6, A8) had PAI score 3. Four patients (C1, C2, C7, C10) had chronic apical periodontitis with score 1, two patients (C5, C9) had score 2, and 4 patients (C3, C4, C6, C8) had score 3.
Exclusion criteria:
The exclusion criteria for primary apical periodontitis were i) having received antibiotics in the past 3 months, ii) presence of a systemic disease, iii) inability to isolate the involved tooth by rubber dam placement, iv) teeth with curved root in the apical third, v) infected teeth with a periodontal pocket depth more than 4 mm, and vi) pregnant women and lactating mothers. Nevertheless, patients with systemic diseases, either root canal treatment done in the past 2 years or broken endodontic files in any canal, were excluded from the secondary apical periodontitis group.
Based on the above-mentioned criteria, 60 patients were eliminated out of 76 with acute apical periodontitis due to age below 20 years (n=4), inability to perform rubber dam isolation (n=8), teeth with curved root in the apical third (n=7), not interested in participating in the study (n=6), narrow canals with difficult canal negotiation without solvents (n=8), presence of systemic diseases (n=12), antibiotic administration within the past 3 months (n=18), and periodontal pocket depth more than 4 mm (n=3). Similarly, in chronic apical periodontitis group, 8 patients were eliminated out of 18 from the study due to previous root canal therapy done within the past 2 years (n=2), broken endodontic file in involved teeth (n=3), antibiotic administration within the past 3 months (n=2), and presence of systemic disease (n=1). Finally, out of 60 patients, 10 cases from each group of acute and chronic apical periodontitis were selected for inclusion in the present study. The preoperative radiographs of acute apical periodontitis (A1-A10) and chronic apical periodontitis (C1-C10) cases are illustrated in Figure 1.
{kind=link}
Sampling:
The selected teeth were isolated using a pre-disinfected rubber dam, and samples were collected. The operating area (tooth and the field surrounding it) was cleaned using H2O2 (30%), swabbed with 2.5% NaOCl, and then inactivated with 5% Na2S2O3. The cavity was prepared, or old restorative material was removed using a sterile bur. The cleaned teeth were further disinfected before operating on the pulp chamber following the previous protocol. All routine aseptic conditions were maintained while collecting the samples [12,13].
In primary apical periodontitis, in order to enlarge the root canals, the ProTaper SX file was employed and then sterile K-files (08-15) were used to work up the peri-apical region of the canals. The K-files, after removing from the canals, were cut off at the point of handle by a pre-sterilized wire cutter and then placed in cryotubes filled with reduced transport fluid [12,13]. Similarly, the pre-sterilized paper points were inserted into the root canal up to the predetermined working length with the help of an electronic apex locator according to the radiographs. The paper points were kept inside the canal for approximately one minute and then transferred to the respective cryotubes.
In secondary apical periodontitis cases, Gates-Glidden drills were used to remove the gutta-percha from the coronal part of the canal accessing the root canal orifice. An electronic apex locator was employed to establish the working length following radiography. Then, the canals were gradually enlarged sequentially reaching #30 file size, restricting the instrumentation to minimum use. No solvent was used. Finally, the collected apical gutta-percha was placed in a sterile RTF vial. Similar to the acute cases, the paper points were kept inside the canal for approximately one minute and then transferred to the respective cryotubes.
Identification of microorganisms and antimicro-bial susceptibility testing:
The samples collected in sterile RTF vials were inoculated into dehydrated media purchased from HIMedia, India. They were subjected to identification and antibiotic susceptibility testing using an automated VITEK2 Compact system (bioMerieux, India) in the Central Laboratory of our University Medical College, Institute of Medical Sciences, Bhubaneswar. The antibiotic sensitivity testing was done against amoxicillin-clavulanate, oxacillin, penicillin, tetracycline, cefoxitin, cefuroxime, cefotaxime, ciprofloxacin, ofloxacin, vancomycin, gentamycin and metronidazole. The sensitivity profile outcomes were interpreted according to the guidelines of EUCAST 2020 and CLSI 2018 [14,15].
Results
The selected teeth were isolated using a pre-disinfected rubber dam, and samples were collected. The operating area (tooth and the field surrounding it) was cleaned using H2O2 (30%), swabbed with 2.5% NaOCl, and then inactivated with 5% Na2S2O3. The cavity was prepared, or old restorative material was removed using a sterile bur. The cleaned teeth were further disinfected before operating on the pulp chamber following the previous protocol. All routine aseptic conditions were maintained while collecting the samples [12,13].
In primary apical periodontitis, in order to enlarge the root canals, the ProTaper SX file was employed and then sterile K-files (08-15) were used to work up the peri-apical region of the canals. The K-files, after removing from the canals, were cut off at the point of handle by a pre-sterilized wire cutter and then placed in cryotubes filled with reduced transport fluid [12,13]. Similarly, the pre-sterilized paper points were inserted into the root canal up to the predetermined working length with the help of an electronic apex locator according to the radiographs. The paper points were kept inside the canal for approximately one minute and then transferred to the respective cryotubes.
In secondary apical periodontitis cases, Gates-Glidden drills were used to remove the gutta-percha from the coronal part of the canal accessing the root canal orifice. An electronic apex locator was employed to establish the working length following radiography. Then, the canals were gradually enlarged sequentially reaching #30 file size, restricting the instrumentation to minimum use. No solvent was used. Finally, the collected apical gutta-percha was placed in a sterile RTF vial. Similar to the acute cases, the paper points were kept inside the canal for approximately one minute and then transferred to the respective cryotubes.
Identification of microorganisms and antimicro-bial susceptibility testing:
The samples collected in sterile RTF vials were inoculated into dehydrated media purchased from HIMedia, India. They were subjected to identification and antibiotic susceptibility testing using an automated VITEK2 Compact system (bioMerieux, India) in the Central Laboratory of our University Medical College, Institute of Medical Sciences, Bhubaneswar. The antibiotic sensitivity testing was done against amoxicillin-clavulanate, oxacillin, penicillin, tetracycline, cefoxitin, cefuroxime, cefotaxime, ciprofloxacin, ofloxacin, vancomycin, gentamycin and metronidazole. The sensitivity profile outcomes were interpreted according to the guidelines of EUCAST 2020 and CLSI 2018 [14,15].
Results
Out of 94 patients reported to the hospital for root canal therapy or re-treatment, 74 were excluded from the study following the previously mentioned stricter exclusion criteria. Ten were selected for root canal therapy or re-treatment. Forty-nine cultivable isolates were recovered from the collected samples, including aerobic and anaerobic bacterial strains belonging to 24 different microbial genera. In primary endodontic infection cases, a total of 49 isolated bacteria belonged to 14 genera. Bacteria belonging to Enterococci sp., Clostridium sp., Streptococcus sp. and Prevotella sp. were found to be two in number whereas those belonging to Actinomyces sp., Bacillus sp., Bifidobacterium sp., Candida sp., Fusobacterium sp. and Propioni-bacterium sp. were found to be single in number. Eleven of the total strains found in primary apical periodontitis cases were Gram-positive, and only three strains (Fusobacterium mortiferum, Prevotella intermedia, Prevotella corporis) were Gram-negative. Secondarily infected canals showed a much more diverse cultivable microbiota than primary infections. From such cases, 35 strains were isolated, the majority of which were comprised of 8 strains of Streptococcus sp. (22.85%) and 7 of Enterococcus sp. (20%), followed by Propionibacterium sp. (n=6, 17.14%), Lactobacillus sp. (n=4, 11.43%), Clostridium sp. (n=3,8.57%) and Actinomyces sp. (n=3,8.57%). Candida albicans, which is a facultative anaerobic fungus, was present in both primary and secondary endodontic infections.
Of a total of 49 isolates, only three were found to be Gram-negative (Fusobacterium sp., Prevotella intermedia, Prevotella corporis) and were present in primarily infected canals. Whereas, Gram-positive strains accounted for 93.87% of the total isolates. Facultative anaerobes accounted for 51.02% of the total isolates, but their percentage of occurrence was 42.86% out of the total isolates in primary cases, and 54.28% in secondarily infected canals. Obligate anaerobes accounted for 36.73% of the total; whereas, their percentage varied in primary (50%) and secondary (31.43%) infections. Obligate aerobes were minor in abundance and accounted for 4.08%. Four strains of Lactobacillus sp. were found in secondary infection cases that were microaerophilic or aerotolerant anaerobes (8.16%).
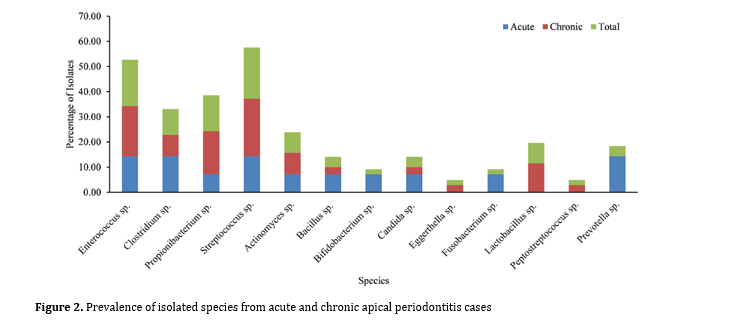
The percentage of prevalence of microbial genera in primary and secondary endodontic infections was found to be viz; Streptococcus sp. (20.41%), Enterococcus sp. (18.37%), Propioni-bacterium sp. (14.29%), Clostridium sp. (10.20%), Lactobacillus sp. (8.16%), Actinomyces sp. (8.16%), Candida albicans (4.08%), Prevotella sp. (4.08%), and Fusobacterium sp. (2.04%). Streptococcus sp., Enterococcus sp., Lactobacillus sp. and Propionibacterium sp. were found to be predominant in secondarily infected canals. Prevotella sp., Fusobacterium sp., Candida albicans, and Clostridium sp. were found in approximately equal proportions in both primary and secondary infections (Figure 2).
Antibiotic susceptibility:
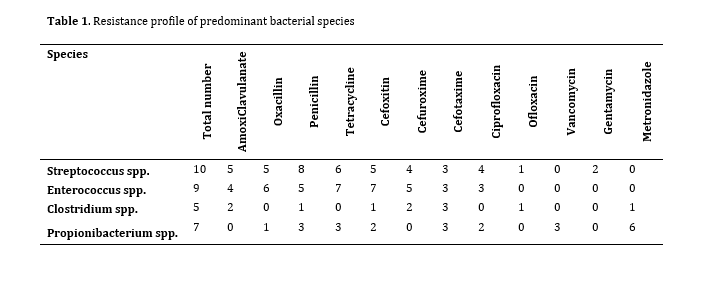
The susceptibility test of 4 major species recovered from primary and secondary infections was conducted against various antibiotics. It was found that Enterococcus sp. did not show resistance to ofloxacin, vancomycin, gentamycin and metronidazole; whereas, the majority of the strains were resistant to tetracycline, cefoxitin and oxacillin (Table 1). The Streptococci strains were sensitive to most antibiotics (β-lactams, cephalosporins, and quinolones) except vancomycin and metronidazole.
None of the strains of Propionibacterium sp. showed resistance to amoxicillin-clavulanate, cefuroxime, ofloxacin and gentamycin; whereas, most strains showed resistance to metronidazole. Similarly, none of the Clostridium isolates resisted oxacillin, tetracycline, ciprofloxacin, vancomycin and gentamycin. Few members of all the four significant genera detected in the culture method showed resistance to penicillin, cefotaxime and cefoxitin. Very few strains resisted ofloxacin, vancomycin and gentamycin (Table 1).
Figure 2. Prevalence of isolated species from acute and chronic apical periodontitis cases
Table 1. Resistance profile of predominant bacterial species
Discussion
Of a total of 49 isolates, only three were found to be Gram-negative (Fusobacterium sp., Prevotella intermedia, Prevotella corporis) and were present in primarily infected canals. Whereas, Gram-positive strains accounted for 93.87% of the total isolates. Facultative anaerobes accounted for 51.02% of the total isolates, but their percentage of occurrence was 42.86% out of the total isolates in primary cases, and 54.28% in secondarily infected canals. Obligate anaerobes accounted for 36.73% of the total; whereas, their percentage varied in primary (50%) and secondary (31.43%) infections. Obligate aerobes were minor in abundance and accounted for 4.08%. Four strains of Lactobacillus sp. were found in secondary infection cases that were microaerophilic or aerotolerant anaerobes (8.16%).
The percentage of prevalence of microbial genera in primary and secondary endodontic infections was found to be viz; Streptococcus sp. (20.41%), Enterococcus sp. (18.37%), Propioni-bacterium sp. (14.29%), Clostridium sp. (10.20%), Lactobacillus sp. (8.16%), Actinomyces sp. (8.16%), Candida albicans (4.08%), Prevotella sp. (4.08%), and Fusobacterium sp. (2.04%). Streptococcus sp., Enterococcus sp., Lactobacillus sp. and Propionibacterium sp. were found to be predominant in secondarily infected canals. Prevotella sp., Fusobacterium sp., Candida albicans, and Clostridium sp. were found in approximately equal proportions in both primary and secondary infections (Figure 2).
Antibiotic susceptibility:
The susceptibility test of 4 major species recovered from primary and secondary infections was conducted against various antibiotics. It was found that Enterococcus sp. did not show resistance to ofloxacin, vancomycin, gentamycin and metronidazole; whereas, the majority of the strains were resistant to tetracycline, cefoxitin and oxacillin (Table 1). The Streptococci strains were sensitive to most antibiotics (β-lactams, cephalosporins, and quinolones) except vancomycin and metronidazole.
None of the strains of Propionibacterium sp. showed resistance to amoxicillin-clavulanate, cefuroxime, ofloxacin and gentamycin; whereas, most strains showed resistance to metronidazole. Similarly, none of the Clostridium isolates resisted oxacillin, tetracycline, ciprofloxacin, vancomycin and gentamycin. Few members of all the four significant genera detected in the culture method showed resistance to penicillin, cefotaxime and cefoxitin. Very few strains resisted ofloxacin, vancomycin and gentamycin (Table 1).
Figure 2. Prevalence of isolated species from acute and chronic apical periodontitis cases
{kind=link}
Table 1. Resistance profile of predominant bacterial species
{kind=link}
Discussion
The pulp tissue of the root canal is initially invaded and colonized by various microorganisms, resulting in primary endodontic infection called acute apical periodontitis, more predominantly by anaerobic bacteria [16]. Whenever such infected root canals are subjected to treatment, some of the microorganisms of primary infection may survive, withstand the chemo-mechanical preparation procedures, and may sustain a nutrient-deprived phase leading to secondary or persistent infections called chronic apical periodontitis [16]. Several attempts are made to understand the microbiota identified through cultivable methods [17]. There are differences in bacterial composition of endodontic microbiota in patients, depending on geographical location, differences in nutritional habits, and lifestyle of patients [17,18]. In addition, variations in the microbiota composition largely depend on the type of irrigating procedure, type of root canal treatment, and variation in coronal leakage due to the quality of coronal seal, which plays a significant role in reinfection of the involved teeth [19].
In absence of reports on the prevailing microbiota of apical periodontitis patients from the eastern part of India, the samples were collected from those presenting to the Outdoor Patient’s Department and analyzed using the VITEK 2 COMPACT system (BioMérieux, USA) in the present study. Our surveillance focused on the cultivable method of identification of prevailing microflora in two different etiological states such as acute and chronic apical periodontitis and their resistance profiling for the most common antibiotics. Therefore, single-step, fast and user-friendly VITEK 2 COMPACT system was used for the abovementioned purpose, as it is the most sought-after globally accepted option, while working in a tertiary care hospital, for both identification and antibiotic-resistant profiling, although traditional [9]. However, attention must be given to timely upgradation through the replacement of recent diagnostic cards in the system to root out any biochemical bias.
Recovery of 49 cultivable isolates belonging to 25 different microbial species indicates the polymicrobial nature of the infection in apical periodontitis [2]. In the present study, the diversity of microbiota was relatively higher in persistent chronic apical periodontitis infections (n=35) as compared to primary infections (n=14) or acute apical periodontitis. Enterococcus, Clostridium, Streptococcus, Prevotella and Propionibacterium bacterial species were found in both sample types but Streptococcus, Enterococcus, and Propioni-bacterium were more prevalent in chronic apical periodontitis as compared to acute patients. However, the percentage of availability and oxygen concentration in dental tissues favor the multiplication of facultative anaerobes like Streptococcus and Enterococcus, resulting in reinfection of the same tooth [2]. Streptococcus sp. was the most predominant (22.86%) in secondary root canal infections. The revealed composition of bacteria could be due to the differences in prevailing nutrition and the environmental conditions around the root canal space [20]. The similar report on a shift towards a complex microbial community in secondarily infected canals with a more diverse and higher number of microorganisms like Propionibacterium, Lactobacillus, Clostridium, and Actinomyces species could be due to variations in treatment history, microbial succession and niche adaptation. In addition, the predominance of Streptococcus and Enterococcus species could be due to their persistence or re-colonization in cases of secondary infection [7,21]. Primarily, one of the major reasons for the differential microbiota composition could be incomplete removal of bacteria from the root canal during root canal treatment of primary infection that favors the growth and multiplication of some of the species [7]. In addition, there is a greater risk of invasion of infecting microorganisms through the canals to the periapical tissues in persistent root canal infections in teeth with defective or dislodged coronal restoration. The composition of microorganisms prevailing in the root canal in acute and chronic apical periodontitis cases differs based on their metabolic activities as well as their nutritional needs. Besides, the recovery of the facultative anaerobic fungus Candida albicans in both types of infections emphasizes on its detection and management while treating such cases [2].
While classifying the nutritional types, we found a higher prevalence of facultative anaerobes (51.02%), but obligate aerobes (4.08%) had the lowest prevalence. Similarly, the obligate anaerobes accounted for 16.33%, while strict anaerobes were 20.4% in both cases. Microaerophilic organisms (Lactobaci-llus species) were found only in persistent apical periodontitis cases with a prevalence of 8.16%; whereas, aerobes were predominant (7.14%) in acute conditions [22, 23, 24]. In acute conditions, in response to infection, there is an influx of tissue breakdown products like peptides and polysaccharides due to inflammation. This reinforces mostly the facultative anaerobes like Streptococcus spp. and Enterococcus spp. as they can use oxygen and perform fermentation for energy production. Moreover, obligate anaerobes like Prevotella spp. and Fusobacterium spp. may be able to sustain in an anaerobic environment utilizing the organic substrates for their energy requirement. On the other hand, in the root canal of chronic apical periodontitis cases, tissue necrosis occurs, more often leading to apical granuloma and cyst formation. This results in accumulation of complex organic substrates like elastin, glycosaminoglycan, and collagen, which promote the growth of obligate anaerobes, although the presence of facultative anaerobes is not ruled out. The complexity of nutrition and environment encourages more diverse microbiota as compared to acute infection conditions. Different studies show a disparity in presence of Enterococcus faecalis in secondary endodontic infections [2,5,6, 24]. Some supported E. faecalis as a minor component, while others reported it as a significant component [2,6,7,24,25,26]. In the present study, E. faecalis ranked second among facultative anaerobic bacteria (20%). It has been understood that the types and numbers of bacteria present in these two conditions vary depending on race, gender, age, lifestyle, and food habits, including the geographic location of patients [2].
Resistance profiling of Streptococcus sp. revealed that they were resistant to most antibiotics except to vancomycin and metronidazole (Table 1), which agrees with earlier published reports [21,23,25]. The present study supports the prescription of vancomycin and metronidazole for treatment of streptococcal infections. Enterococcus species were found to be resistant to a significant group of antibiotics (amoxicillin-clavulanate, tetracycline, cefoxitin, cefuroxime, oxacillin, penicillin etc.), which corroborates with other studies [3,9,23]. Previous reports on the susceptibility of Streptococcus species to such a wide spectrum of antibiotics match our outcome, which provides scope of recommending a wide range of antibiotics to eradicate these bacteria involved in apical periodontal infections [3,21,23]. It was also noted that Enterococcus sp. was sensitive to ofloxacin, metronidazole, vancomycin and gentamycin, which indicates that such drugs may be prescribed for chronic infective cases.
Six species of Propionibacterium in the present study showed resistance to metronidazole. However, they were susceptible to amoxicillin-clavulanate, cefuroxime, ofloxacin, and gentamycin, which provides a scope for their use against such infections. Also, two strains of Clostridium sp. were found in primary infections and three in secondary infections. The resistance profile showed that Clostridium species were resistant to amoxicillin-clavulanate, penicillin, cefoxitin, cefuroxime, cefotaxime, ofloxacin, and metro-nidazole (Table 1).
The advantage of performing antibiotic resistance profiling of the prevailing bacteria is to judiciously prescribe the most suitable antibiotic regimen for a specific infection type instead of opting for broad-spectrum or random multiple antibiotics in absence of a susceptibility report. Resistance profiling analysis highlights the existing complex interplay between apical periodontal bacterial species and antibiotic resistance patterns. It underscores paving a path for optimized treatment approaches for improved clinical outcomes.
To the best of the authors’ knowledge, this study, although preliminary, is the first bacterial prevalence and antibiotic profiling study on apical periodontitis infections in a tertiary dental care center in the eastern part of India. A multi-centric routine surveillance study is the need of the hour targeting a larger sample size and geographically different locations for a thickly populated state like Odisha, India for a better perceptible conclusion.
Conclusion
In absence of reports on the prevailing microbiota of apical periodontitis patients from the eastern part of India, the samples were collected from those presenting to the Outdoor Patient’s Department and analyzed using the VITEK 2 COMPACT system (BioMérieux, USA) in the present study. Our surveillance focused on the cultivable method of identification of prevailing microflora in two different etiological states such as acute and chronic apical periodontitis and their resistance profiling for the most common antibiotics. Therefore, single-step, fast and user-friendly VITEK 2 COMPACT system was used for the abovementioned purpose, as it is the most sought-after globally accepted option, while working in a tertiary care hospital, for both identification and antibiotic-resistant profiling, although traditional [9]. However, attention must be given to timely upgradation through the replacement of recent diagnostic cards in the system to root out any biochemical bias.
Recovery of 49 cultivable isolates belonging to 25 different microbial species indicates the polymicrobial nature of the infection in apical periodontitis [2]. In the present study, the diversity of microbiota was relatively higher in persistent chronic apical periodontitis infections (n=35) as compared to primary infections (n=14) or acute apical periodontitis. Enterococcus, Clostridium, Streptococcus, Prevotella and Propionibacterium bacterial species were found in both sample types but Streptococcus, Enterococcus, and Propioni-bacterium were more prevalent in chronic apical periodontitis as compared to acute patients. However, the percentage of availability and oxygen concentration in dental tissues favor the multiplication of facultative anaerobes like Streptococcus and Enterococcus, resulting in reinfection of the same tooth [2]. Streptococcus sp. was the most predominant (22.86%) in secondary root canal infections. The revealed composition of bacteria could be due to the differences in prevailing nutrition and the environmental conditions around the root canal space [20]. The similar report on a shift towards a complex microbial community in secondarily infected canals with a more diverse and higher number of microorganisms like Propionibacterium, Lactobacillus, Clostridium, and Actinomyces species could be due to variations in treatment history, microbial succession and niche adaptation. In addition, the predominance of Streptococcus and Enterococcus species could be due to their persistence or re-colonization in cases of secondary infection [7,21]. Primarily, one of the major reasons for the differential microbiota composition could be incomplete removal of bacteria from the root canal during root canal treatment of primary infection that favors the growth and multiplication of some of the species [7]. In addition, there is a greater risk of invasion of infecting microorganisms through the canals to the periapical tissues in persistent root canal infections in teeth with defective or dislodged coronal restoration. The composition of microorganisms prevailing in the root canal in acute and chronic apical periodontitis cases differs based on their metabolic activities as well as their nutritional needs. Besides, the recovery of the facultative anaerobic fungus Candida albicans in both types of infections emphasizes on its detection and management while treating such cases [2].
While classifying the nutritional types, we found a higher prevalence of facultative anaerobes (51.02%), but obligate aerobes (4.08%) had the lowest prevalence. Similarly, the obligate anaerobes accounted for 16.33%, while strict anaerobes were 20.4% in both cases. Microaerophilic organisms (Lactobaci-llus species) were found only in persistent apical periodontitis cases with a prevalence of 8.16%; whereas, aerobes were predominant (7.14%) in acute conditions [22, 23, 24]. In acute conditions, in response to infection, there is an influx of tissue breakdown products like peptides and polysaccharides due to inflammation. This reinforces mostly the facultative anaerobes like Streptococcus spp. and Enterococcus spp. as they can use oxygen and perform fermentation for energy production. Moreover, obligate anaerobes like Prevotella spp. and Fusobacterium spp. may be able to sustain in an anaerobic environment utilizing the organic substrates for their energy requirement. On the other hand, in the root canal of chronic apical periodontitis cases, tissue necrosis occurs, more often leading to apical granuloma and cyst formation. This results in accumulation of complex organic substrates like elastin, glycosaminoglycan, and collagen, which promote the growth of obligate anaerobes, although the presence of facultative anaerobes is not ruled out. The complexity of nutrition and environment encourages more diverse microbiota as compared to acute infection conditions. Different studies show a disparity in presence of Enterococcus faecalis in secondary endodontic infections [2,5,6, 24]. Some supported E. faecalis as a minor component, while others reported it as a significant component [2,6,7,24,25,26]. In the present study, E. faecalis ranked second among facultative anaerobic bacteria (20%). It has been understood that the types and numbers of bacteria present in these two conditions vary depending on race, gender, age, lifestyle, and food habits, including the geographic location of patients [2].
Resistance profiling of Streptococcus sp. revealed that they were resistant to most antibiotics except to vancomycin and metronidazole (Table 1), which agrees with earlier published reports [21,23,25]. The present study supports the prescription of vancomycin and metronidazole for treatment of streptococcal infections. Enterococcus species were found to be resistant to a significant group of antibiotics (amoxicillin-clavulanate, tetracycline, cefoxitin, cefuroxime, oxacillin, penicillin etc.), which corroborates with other studies [3,9,23]. Previous reports on the susceptibility of Streptococcus species to such a wide spectrum of antibiotics match our outcome, which provides scope of recommending a wide range of antibiotics to eradicate these bacteria involved in apical periodontal infections [3,21,23]. It was also noted that Enterococcus sp. was sensitive to ofloxacin, metronidazole, vancomycin and gentamycin, which indicates that such drugs may be prescribed for chronic infective cases.
Six species of Propionibacterium in the present study showed resistance to metronidazole. However, they were susceptible to amoxicillin-clavulanate, cefuroxime, ofloxacin, and gentamycin, which provides a scope for their use against such infections. Also, two strains of Clostridium sp. were found in primary infections and three in secondary infections. The resistance profile showed that Clostridium species were resistant to amoxicillin-clavulanate, penicillin, cefoxitin, cefuroxime, cefotaxime, ofloxacin, and metro-nidazole (Table 1).
The advantage of performing antibiotic resistance profiling of the prevailing bacteria is to judiciously prescribe the most suitable antibiotic regimen for a specific infection type instead of opting for broad-spectrum or random multiple antibiotics in absence of a susceptibility report. Resistance profiling analysis highlights the existing complex interplay between apical periodontal bacterial species and antibiotic resistance patterns. It underscores paving a path for optimized treatment approaches for improved clinical outcomes.
To the best of the authors’ knowledge, this study, although preliminary, is the first bacterial prevalence and antibiotic profiling study on apical periodontitis infections in a tertiary dental care center in the eastern part of India. A multi-centric routine surveillance study is the need of the hour targeting a larger sample size and geographically different locations for a thickly populated state like Odisha, India for a better perceptible conclusion.
Conclusion
The study results showed that although both acute and chronic root canal infections were due to manifestations of polymicrobial infections, their microbial composition and nutritional requirements of the involved bacteria may vary based on the stage and severity of the infection because of the variability in metabolic activities of bacterial communities and the prevailing environment inside the root canal system. The majority of the bacterial species resisted major antibiotic classes (β-lactams, cephalosporins, quinolones). Understanding the differences in bacterial nutritional types and their resistance profile provides information about the possible treatment prescriptions for management of apical periodontitis infections.
Acknowledgements
Acknowledgements
The authors are thankful to the Dean, Head of the Departments of Conservative and Endodontics of the Institutes of Dental Sciences and President of the Siksha ‘O’ Anusandhan (Deemed to be University), Odisha, for providing the necessary infrastructure, resources and encouragement to accomplish this research work.
Type of Study: Original article |
Subject:
Periodontology
References
1. Wong J, Manoil D, Näsman P, Belibasakis GN, Neelakantan P. Microbiological Aspects of Root Canal Infections and Disinfection Strategies: An Update Review on the Current Knowledge and Challenges. Front Oral Health. 2021 Jun 25;2:672887. [DOI:10.3389/froh.2021.672887] [PMID] []
2. Siqueira Junior JF, Rôças IDN, Marceliano-Alves MF, Pérez AR, Ricucci D. Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz Oral Res. 2018 Oct 18;32(suppl 1):e65. [DOI:10.1590/1807-3107bor-2018.vol32.0065] [PMID]
3. Ersahan S, Hepsenoglu YE. Microbial analysis of endodontic infections in teeth with post-treatment apical periodontitis before and after medication. Aust Endod J. 2023 Apr;49(1):75-86. [DOI:10.1111/aej.12613] [PMID]
4. Siqueira JF Jr, Rôças IN. Present status and future directions: Microbiology of endodontic infections. Int Endod J. 2022 May;55 Suppl 3:512-30. [DOI:10.1111/iej.13677] [PMID]
5. Dioguardi M, Di Gioia G, Illuzzi G, Arena C, Caponio VCA, Caloro GA, et al. Inspection of the Microbiota in Endodontic Lesions. Dent J (Basel). 2019 May 1;7(2):47. [DOI:10.3390/dj7020047] [PMID] []
6. Gomes BPFA, Louzada LM, Almeida-Gomes RF, Pinheiro ET, Sousa ELR, Jacinto RC, et al. Investigation of Filifactor alocis in primary and in secondary endodontic infections: A molecular study. Arch Oral Biol. 2020 Oct;118:104826. [DOI:10.1016/j.archoralbio.2020.104826] [PMID]
7. Korona-Glowniak I, Piatek D, Fornal E, Lukowiak A, Gerasymchuk Y, Kedziora A, et al. Patterns of Oral Microbiota in Patients with Apical Periodontitis. J Clin Med. 2021 Jun 19;10(12):2707. [DOI:10.3390/jcm10122707] [PMID] []
8. Suprewicz Ł, Tokajuk G, Cieśluk M, Deptuła P, Sierpińska T, Wolak P, et al. Bacteria Residing at Root Canals Can Induce Cell Proliferation and Alter the Mechanical Properties of Gingival and Cancer Cells. Int J Mol Sci. 2020 Oct 24;21(21):7914. [DOI:10.3390/ijms21217914] [PMID] []
9. Joyanes P, del Carmen Conejo M, Martínez-Martínez L, Perea EJ. Evaluation of the VITEK 2 system for the identification and susceptibility testing of three species of nonfermenting gram-negative rods frequently isolated from clinical samples. J Clin Microbiol. 2001 Sep;39(9):3247-53. [DOI:10.1128/JCM.39.9.3247-3253.2001] [PMID] []
10. Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986 Feb;2(1):20-34. [DOI:10.1111/j.1600-9657.1986.tb00119.x] [PMID]
11. Hussain MA, Singh SK, Naz S, Haque M, Shah HK, Singh A. Predictors of apical periodontitis in root canal treated teeth from an adult Nepalese subpopulation: a cross-sectional study. BMC Oral Health. 2024 Mar 29;24(1):400. [DOI:10.1186/s12903-024-04139-3] [PMID] []
12. Zahran S, Patel S, Koller G, Mannocci F. The impact of an enhanced infection control protocol on molar root canal treatment outcome - a randomized clinical trial. Int Endod J. 2021 Nov;54(11):1993-2005. [DOI:10.1111/iej.13605] [PMID]
13. Rørslett Hardersen L, Enersen M, Kristoffersen AK, Ørstavik D, Sunde PT. Maintenance of the aseptic working field during endodontic treatment. Acta Odontol Scand. 2019 Oct;77(7):502-7. [DOI:10.1080/00016357.2019.1606935] [PMID]
14. Wayne PA. Clinical and laboratory standards institute: performance standards for antimicrobial susceptibility testing: informational supplement, M100. Clinical and Laboratory Standards Institute (CLSI). 2018 Jan 23.
15. EUCAST. "The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 14.0, 2024. Http://WwwEucastOrg [Internet]. 2024;12,0:0-77.
16. Nagy-Bota MC, Man A, Santacroce L, Brinzaniuc K, Pap Z, Pacurar M, et al. Essential oils as alternatives for root-canal treatment and infection control against enterococcus faecalis- A preliminary study. Applied Sciences (Switzerland). 2021;11(4):1-13. [DOI:10.3390/app11041422]
17. Arias-Moliz MT, Ordinola-Zapata R, Staley C, Pérez-Carrasco V, García-Salcedo JA, Uroz-Torres D, et al. Exploring the root canal microbiome in previously treated teeth: A comparative study of diversity and metabolic pathways across two geographical locations. Int Endod J. 2024 Jul;57(7):885-94. [DOI:10.1111/iej.13934] [PMID]
18. Kumar G, Bhadury P. Exploring the influences of geographical variation on sequence signatures in the human gut microbiome. J Genet. 2023;102:51. [DOI:10.1007/s12041-023-01448-4] [PMID]
19. Gomes BPFA, Aveiro E, Kishen A. Irrigants and irrigation activation systems in Endodontics. Braz Dent J. 2023 Jul-Aug;34(4):1-33. [DOI:10.1590/0103-6440202305577]
20. Zargar N, Marashi MA, Ashraf H, Hakopian R, Beigi P. Identification of microorganisms in persistent/secondary endodontic infections with respect to clinical and radiographic findings: bacterial culture and molecular detection. Iran J Microbiol. 2019 Apr;11(2):120-8. [DOI:10.18502/ijm.v11i2.1073] [PMID] []
21. Wong J, Manoil D, Näsman P, Belibasakis GN, Neelakantan P. Microbiological Aspects of Root Canal Infections and Disinfection Strategies: An Update Review on the Current Knowledge and Challenges. Front Oral Health. 2021 Jun 25;2:672887. [DOI:10.3389/froh.2021.672887] [PMID] []
22. Bordagaray MJ, Fernández A, Garrido M, Astorga J, Hoare A, Hernández M. Systemic and Extraradicular Bacterial Translocation in Apical Periodontitis. Front Cell Infect Microbiol. 2021 Mar 19;11:649925. [DOI:10.3389/fcimb.2021.649925] [PMID] []
23. Siqueira Junior JF, Rôças IDN, Marceliano-Alves MF, Pérez AR, Ricucci D. Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz Oral Res. 2018 Oct 18;32(suppl 1):e65. [DOI:10.1590/1807-3107bor-2018.vol32.0065] [PMID]
24. Bouillaguet S, Manoil D, Girard M, Louis J, Gaïa N, Leo S, et al. Root Microbiota in Primary and Secondary Apical Periodontitis. Front Microbiol. 2018 Oct 9;9:2374. [DOI:10.3389/fmicb.2018.02374] [PMID] []
25. Elashiry MM, Bergeron BE, Tay FR. Enterococcus faecalis in secondary apical periodontitis: Mechanisms of bacterial survival and disease persistence. Microb Pathog. 2023 Oct;183:106337. [DOI:10.1016/j.micpath.2023.106337] [PMID]
26. Johnson AF, LaRock CN. Antibiotic Treatment, Mechanisms for Failure, and Adjunctive Therapies for Infections by Group A Streptococcus. Front Microbiol. 2021 Nov 4;12:760255. [DOI:10.3389/fmicb.2021.760255] [PMID] []
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |