Journal of Research in Dental
and Maxillofacial Sciences
Volume 10, Issue 2 (6-2025)
J Res Dent Maxillofac Sci 2025, 10(2): 125-133 |
Back to browse issues page

Ethics code: IR.SBMU.DRC.REC.1399.12.7
Clinical trials code: IRCT20090506001882N10
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Eghbali Zarch A, Amiri Tehranizadeh N, Ansari G, Fallahinejad Ghajari M. Sedative Effect of Intravenous Propofol-Ketamine and Midazolam Ketamine Combinations for Dental Treatment of Uncooperative 2-6 Year-Old Children: A Clinical Trial. J Res Dent Maxillofac Sci 2025; 10 (2) :125-133
URL: http://jrdms.dentaliau.ac.ir/article-1-636-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-636-en.html
Ahmad Eghbali Zarch1 

 , Narjes Amiri Tehranizadeh2 , Ghassem Ansari3 , Masoud Fallahinejad Ghajari *4
, Narjes Amiri Tehranizadeh2 , Ghassem Ansari3 , Masoud Fallahinejad Ghajari *4
, Narjes Amiri Tehranizadeh2 , Ghassem Ansari3 , Masoud Fallahinejad Ghajari *4
1- Department of Anesthesiology, Medical School, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Private Pediatric Dentistry Practice, Tehran, Iran.
3- Department of Pediatric Dentistry, Dental Research Center, Research Institute of Dental Sciences, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Pediatric Dentistry, Dental Research Center, Research Institute of Dental Sciences, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,masfalnegh@sbmu.ac.ir
2- Private Pediatric Dentistry Practice, Tehran, Iran.
3- Department of Pediatric Dentistry, Dental Research Center, Research Institute of Dental Sciences, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Pediatric Dentistry, Dental Research Center, Research Institute of Dental Sciences, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Keywords: Deep Sedation, Conscious Sedation, Pediatric Dentistry, Anesthetics, Dissociative, Midazolam, Ketamine, Propofol
Full-Text [PDF 432 kb]
(2827 Downloads)
| Abstract (HTML) (2407 Views)
Full-Text: (1175 Views)
Abstract
Background and Aim: Various medications are used for intravenous (IV) sedation in pediatric dentistry. This study evaluated the efficacy of IV midazolam/ketamine (MK) versus propofol/ketamine (PK) for dental sedation of uncooperative children.
Materials and Methods: This double-blind, randomized controlled clinical trial was carried out on 22 healthy, uncooperative children aged 2-6 years requiring two similar dental treatment sessions. Children were randomly assigned to two groups. Group A received PK in their first, and MK in their second visit. Group B received the same combinations in a reverse order. Oxygen saturation rate (SPO2) and heart rate (HR) were recorded at baseline, at the time of IV administration, local anesthetic injection, 15 and 30 minutes later, and at the time of discharge. Two independent calibrated pedodontists scored the sedation level using the Houpt scale during treatment. Data were analyzed by t-test, Wilcoxon, Mann-Whitney, and one-sample Kolmogorov-Smirnov tests.
Results: The mean age of the participants was 3.6 years with a mean weight of 15.68 kg. SPO2 was not significantly different between the two groups (P=0.609). However, the HR was significantly higher in the MK combination (P=0.001). No significant difference was detected between the two combinations for sleepiness (P=0.283), movement (P=0.180), crying (P=0.093), or overall behavior (P=0.364). The recovery time in the PK group was significantly shorter than that in the MK group (P=0.03).
Conclusion: Both sedation regimens are effective for dental treatment of uncooperative children. PK combination provided a more acceptable hemodynamic stability and shorter recovery.
Keywords: Deep Sedation; Conscious Sedation; Pediatric Dentistry; Anesthetics, Dissociative; Midazolam; Ketamine; Propofol
Introduction
Materials and Methods: This double-blind, randomized controlled clinical trial was carried out on 22 healthy, uncooperative children aged 2-6 years requiring two similar dental treatment sessions. Children were randomly assigned to two groups. Group A received PK in their first, and MK in their second visit. Group B received the same combinations in a reverse order. Oxygen saturation rate (SPO2) and heart rate (HR) were recorded at baseline, at the time of IV administration, local anesthetic injection, 15 and 30 minutes later, and at the time of discharge. Two independent calibrated pedodontists scored the sedation level using the Houpt scale during treatment. Data were analyzed by t-test, Wilcoxon, Mann-Whitney, and one-sample Kolmogorov-Smirnov tests.
Results: The mean age of the participants was 3.6 years with a mean weight of 15.68 kg. SPO2 was not significantly different between the two groups (P=0.609). However, the HR was significantly higher in the MK combination (P=0.001). No significant difference was detected between the two combinations for sleepiness (P=0.283), movement (P=0.180), crying (P=0.093), or overall behavior (P=0.364). The recovery time in the PK group was significantly shorter than that in the MK group (P=0.03).
Conclusion: Both sedation regimens are effective for dental treatment of uncooperative children. PK combination provided a more acceptable hemodynamic stability and shorter recovery.
Keywords: Deep Sedation; Conscious Sedation; Pediatric Dentistry; Anesthetics, Dissociative; Midazolam; Ketamine; Propofol
Introduction
Various agents have been utilized to provide intravenous sedation in pediatric dentistry. Propofol is among the most widely used medications to induce anesthesia and sedation. It is an alkylphenol with a strong hypnotic effect and a short half-life (8-10 min). Short recovery time is the primary benefit of this drug. However, painful intravenous injection and unstable action are the main disadvantages of propofol [1]. Ketamine is a hypnotic-sedative drug with a modest analgesic effect. The main disadvantage of ketamine is some degree of hallucination following anesthesia and sedation [2]. Midazolam is the most common anxiolytic drug used in pediatric dentistry. It has a rapid onset and limited sedative effect. The downsides of midazolam include short duration of action and potential for increased irritability and agitation [3].
Rai et al. [4] compared the efficacy and safety of midazolam, ketamine, and propofol, for full oral rehabilitation of 30 uncooperative children aged 3-6 years, and showed propofol to act quickly; however, it had substantial pain on injection causing children to cry. Despite the longest onset of action, midazolam was not efficient in treatment completion due to the children’s crying and movements. Maximum cooperation was observed in working with ketamine, while having no clear side effects; they recommended the use of ketamine in combination with other sedatives.
Dal et al. [5] evaluated the effectiveness and safety of midazolam-ketamine (MK) and propofol-ketamine (PK) for sedation and reported a rise in the heart rate (HR) at 10 min in the MK group compared with the PK; the recovery time was also significantly longer in the MK than PK. Ahmed et al. [6] found that although procedural duration and recovery time were similar in all groups, the discharge time was significantly shorter in the PK group compared to other groups. They concluded that sedation with propofol could be performed safely and effectively in children. Canpolat et al. [7] reported that propofol is an excellent choice when compared to ketamine alone or together, based on its shorter recovery time, lack of nausea and vomiting, and acceptable surgical satisfaction.
Kip et al. [8] stated that a reduction in ketamine dose in Ketofol mixture was associated with a faster recovery, although the dentist’s satisfaction was lower. A 1:2 ratio was proven to be more reliable after simultaneous evaluation of all parameters [8]. Dixon et al. [9] stated that sedation with propofol may be safer than general anesthesia for dental treatment of adolescents with high therapeutic needs and prolonged operating time. Uludag et al. [10] suggested that MK provided a more stable hemodynamic state during dental sedation, while patients in both groups were similar in the level of comfort and post-sedation recovery. Adiban et al. [11] compared Ketofol with MK in children and concluded that a rise in HR and blood pressure was associated with the MK use, which was statistically significant. However, both combinations provided acceptable levels of sedation.
Wallace et al. [12] indicated that receiving and recording feedback can improve service quality following intravenous (IV) sedation with propofol. The purpose of using different drugs in combination is to exploit the benefits of various drugs while reducing the individual drug doses.
Thus, this study aimed to compare the sedation potential of PK with MK combinations for dental treatment of uncooperative children aged 2-6 years.
Materials and Methods
Rai et al. [4] compared the efficacy and safety of midazolam, ketamine, and propofol, for full oral rehabilitation of 30 uncooperative children aged 3-6 years, and showed propofol to act quickly; however, it had substantial pain on injection causing children to cry. Despite the longest onset of action, midazolam was not efficient in treatment completion due to the children’s crying and movements. Maximum cooperation was observed in working with ketamine, while having no clear side effects; they recommended the use of ketamine in combination with other sedatives.
Dal et al. [5] evaluated the effectiveness and safety of midazolam-ketamine (MK) and propofol-ketamine (PK) for sedation and reported a rise in the heart rate (HR) at 10 min in the MK group compared with the PK; the recovery time was also significantly longer in the MK than PK. Ahmed et al. [6] found that although procedural duration and recovery time were similar in all groups, the discharge time was significantly shorter in the PK group compared to other groups. They concluded that sedation with propofol could be performed safely and effectively in children. Canpolat et al. [7] reported that propofol is an excellent choice when compared to ketamine alone or together, based on its shorter recovery time, lack of nausea and vomiting, and acceptable surgical satisfaction.
Kip et al. [8] stated that a reduction in ketamine dose in Ketofol mixture was associated with a faster recovery, although the dentist’s satisfaction was lower. A 1:2 ratio was proven to be more reliable after simultaneous evaluation of all parameters [8]. Dixon et al. [9] stated that sedation with propofol may be safer than general anesthesia for dental treatment of adolescents with high therapeutic needs and prolonged operating time. Uludag et al. [10] suggested that MK provided a more stable hemodynamic state during dental sedation, while patients in both groups were similar in the level of comfort and post-sedation recovery. Adiban et al. [11] compared Ketofol with MK in children and concluded that a rise in HR and blood pressure was associated with the MK use, which was statistically significant. However, both combinations provided acceptable levels of sedation.
Wallace et al. [12] indicated that receiving and recording feedback can improve service quality following intravenous (IV) sedation with propofol. The purpose of using different drugs in combination is to exploit the benefits of various drugs while reducing the individual drug doses.
Thus, this study aimed to compare the sedation potential of PK with MK combinations for dental treatment of uncooperative children aged 2-6 years.
Materials and Methods
This study was approved by the Ethics Committee of Shahid Beheshti University, Dental School, Tehran, Iran (IR.SBMU.DRC.REC. 1399.12.7) and registered as a clinical trial in the Iranian Registry of Clinical Trials under the code IRCT20090506001882N10.
Trial design:
This double-blind, randomized cross-over clinical trial was conducted on children who had two similar treatment sessions, and the treatments were designed such that each child served as both the test and control groups.
Participants, eligibility criteria, and settings:
Twenty-two uncooperative children between 2 to 6 years referred to the sedation unit of the Pediatric Dentistry department of the university were recruited. The inclusion criteria were healthy children (ASA 1) who required at least two similar dental treatment sessions; were ranked as definitely negative by the Frankl scale [13], and did not have any airway obstruction, systemic disease, common cold, or fever.
The exclusion criteria were systemic diseases, history of allergy to medications used, common cold or nasal obstruction during the treatment session, and failure to complete two treatment sessions. The children were selected by convenience sampling.
Sample size calculation:
To estimate the sample size, considering the study design and the quantitative nature of the dependent variables of the study, the following formula was used:
In this formula, assuming the type 1 error of the test (α)=0.05, type 2 error of the test (β)=0.2 (study power of 80%), and extracting the values of σ=0.7 and µ∆ equal to 0.7 for each main dependent variable of the study, the number of samples was calculated to be 20 in each group at each assessment time point.
Randomization:
Assignment of the children to the two treatment groups was done randomly by coin toss. Children were randomly allocated to one of the two groups with group I receiving IV PK combination (A) at the first session and IV MK (B) at their second session. Group II received the same combinations in reverse order of sessions. AB in the tables refers to children who received drug A in their first visit and drug B in the second (n=12 subjects), whereas BA represents the children who received drug B first and then drug A at the following session (n=10 subjects).
Blinding:
The children and individuals assessing the criteria were blinded to the type of medication prescribed. The operator, assessors, and patients were all blinded to the administered drug regimen and the groups.
Intervention:
Prior to sedation, the necessary instructions were given to the parents in both written and verbal forms. The children were required to abstain from solid food and milk for 6 hours before drug administration and not to drink water for 3 hours before the procedure. Written informed consent was obtained from the parents.
The two treatment sessions were scheduled in similar terms in terms of treatment type and duration. The Patients’ HR and arterial oxygen saturation rate (SPO2) were recorded at baseline of each session and 15-minute intervals afterwards. An initial dose of oral midazolam (5 mg/mL midazolam vial; Tehran Chemie, Pharmaceutical Co., Tehran, Iran) was administered mixed with sweetened water in a syringe to all children in 0.3 mg/kg dose 30 minutes before intravenous injection. Ketamine (50 mg/mL vial, ROTEXMEDICAL, Germany) with propofol (2 mg/kg) and midazolam (5 mg/mL vial, Darupakhsh Co, Iran) at 0.2 mg/kg dose were administered on the basis of the protocol of this investigation. Atropine (0.2 mg/kg) (0.5 mg/mL vial, Caspian Tamin Co., Rasht, Iran) was also administered equally in all patients in order to lower the salivary secretion rate. A pulse oximeter probe and a nasal cannula were placed for all patients immediately after the sedation induction with the oxygen flow rate of 5 L/min. Local anesthesia was achieved using Persocaine E (2% lidocaine with 1:100,000 epinephrine; Daroupakhsh Co, Iran) and dental treatment was initiated while data recording was started by the assisting pediatric dentists.
Oxygen saturation (SPO2) and HR were recorded before drug administration (baseline), during IV injection (at venipuncture), at the time of local anesthetic injection, every 15 minutes afterwards during the procedure, and at the time of discharge, using a multi-purpose patient care monitoring device (Alborz, Saadat Co., Tehran, Iran).
The children’s behavioral changes were recorded throughout the procedure using the Houpt scale [14] which includes: the level of sleepiness, crying, movement, and overall behavior during catheter placement, anesthesia injection, and first and second 15 minutes of dental procedure. Evaluations were performed and recorded by two calibrated pediatric dentists who were unaware of the children’s assignment to the treatment group or the drugs administered. Each treatment session was completed within about 30 minutes.
Upon completion of the dental treatment, the children were monitored until the discharge criteria were met. Time to full recovery was recorded from the last dose administration before the treatment termination until the signs of complete recovery were observed.
Any potential side effects of medications were recorded before and after discharge according to the parents’ report. The second treatment session was scheduled within 2-3 weeks of the first session.
Statistical analysis:
Data distribution was normal for SPO2 and HR in both groups as shown by the Kolmogorov-Smirnov test (P>0.05). Independent t-test was used to assess the treatment, carryover, and washout effects of HR and SPO2. For non-normally distributed data (recovery time) and qualitative data (Houpt scale variables), the Wilcoxon or Mann-Whitney non-parametric tests were used.
Results
Trial design:
This double-blind, randomized cross-over clinical trial was conducted on children who had two similar treatment sessions, and the treatments were designed such that each child served as both the test and control groups.
Participants, eligibility criteria, and settings:
Twenty-two uncooperative children between 2 to 6 years referred to the sedation unit of the Pediatric Dentistry department of the university were recruited. The inclusion criteria were healthy children (ASA 1) who required at least two similar dental treatment sessions; were ranked as definitely negative by the Frankl scale [13], and did not have any airway obstruction, systemic disease, common cold, or fever.
The exclusion criteria were systemic diseases, history of allergy to medications used, common cold or nasal obstruction during the treatment session, and failure to complete two treatment sessions. The children were selected by convenience sampling.
Sample size calculation:
To estimate the sample size, considering the study design and the quantitative nature of the dependent variables of the study, the following formula was used:
In this formula, assuming the type 1 error of the test (α)=0.05, type 2 error of the test (β)=0.2 (study power of 80%), and extracting the values of σ=0.7 and µ∆ equal to 0.7 for each main dependent variable of the study, the number of samples was calculated to be 20 in each group at each assessment time point.
Randomization:
Assignment of the children to the two treatment groups was done randomly by coin toss. Children were randomly allocated to one of the two groups with group I receiving IV PK combination (A) at the first session and IV MK (B) at their second session. Group II received the same combinations in reverse order of sessions. AB in the tables refers to children who received drug A in their first visit and drug B in the second (n=12 subjects), whereas BA represents the children who received drug B first and then drug A at the following session (n=10 subjects).
Blinding:
The children and individuals assessing the criteria were blinded to the type of medication prescribed. The operator, assessors, and patients were all blinded to the administered drug regimen and the groups.
Intervention:
Prior to sedation, the necessary instructions were given to the parents in both written and verbal forms. The children were required to abstain from solid food and milk for 6 hours before drug administration and not to drink water for 3 hours before the procedure. Written informed consent was obtained from the parents.
The two treatment sessions were scheduled in similar terms in terms of treatment type and duration. The Patients’ HR and arterial oxygen saturation rate (SPO2) were recorded at baseline of each session and 15-minute intervals afterwards. An initial dose of oral midazolam (5 mg/mL midazolam vial; Tehran Chemie, Pharmaceutical Co., Tehran, Iran) was administered mixed with sweetened water in a syringe to all children in 0.3 mg/kg dose 30 minutes before intravenous injection. Ketamine (50 mg/mL vial, ROTEXMEDICAL, Germany) with propofol (2 mg/kg) and midazolam (5 mg/mL vial, Darupakhsh Co, Iran) at 0.2 mg/kg dose were administered on the basis of the protocol of this investigation. Atropine (0.2 mg/kg) (0.5 mg/mL vial, Caspian Tamin Co., Rasht, Iran) was also administered equally in all patients in order to lower the salivary secretion rate. A pulse oximeter probe and a nasal cannula were placed for all patients immediately after the sedation induction with the oxygen flow rate of 5 L/min. Local anesthesia was achieved using Persocaine E (2% lidocaine with 1:100,000 epinephrine; Daroupakhsh Co, Iran) and dental treatment was initiated while data recording was started by the assisting pediatric dentists.
Oxygen saturation (SPO2) and HR were recorded before drug administration (baseline), during IV injection (at venipuncture), at the time of local anesthetic injection, every 15 minutes afterwards during the procedure, and at the time of discharge, using a multi-purpose patient care monitoring device (Alborz, Saadat Co., Tehran, Iran).
The children’s behavioral changes were recorded throughout the procedure using the Houpt scale [14] which includes: the level of sleepiness, crying, movement, and overall behavior during catheter placement, anesthesia injection, and first and second 15 minutes of dental procedure. Evaluations were performed and recorded by two calibrated pediatric dentists who were unaware of the children’s assignment to the treatment group or the drugs administered. Each treatment session was completed within about 30 minutes.
Upon completion of the dental treatment, the children were monitored until the discharge criteria were met. Time to full recovery was recorded from the last dose administration before the treatment termination until the signs of complete recovery were observed.
Any potential side effects of medications were recorded before and after discharge according to the parents’ report. The second treatment session was scheduled within 2-3 weeks of the first session.
Statistical analysis:
Data distribution was normal for SPO2 and HR in both groups as shown by the Kolmogorov-Smirnov test (P>0.05). Independent t-test was used to assess the treatment, carryover, and washout effects of HR and SPO2. For non-normally distributed data (recovery time) and qualitative data (Houpt scale variables), the Wilcoxon or Mann-Whitney non-parametric tests were used.
Results
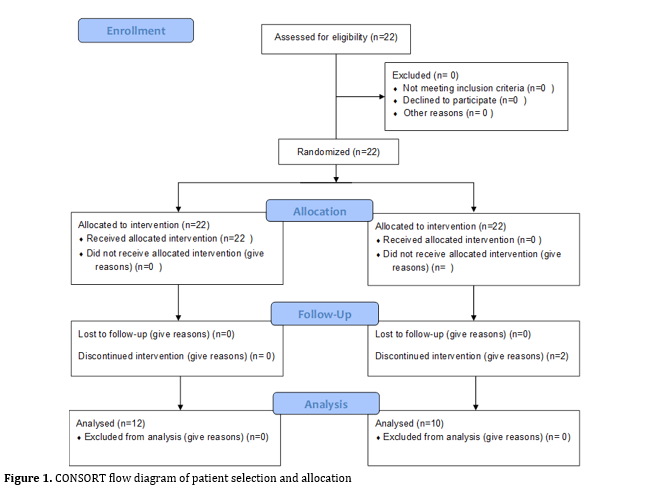
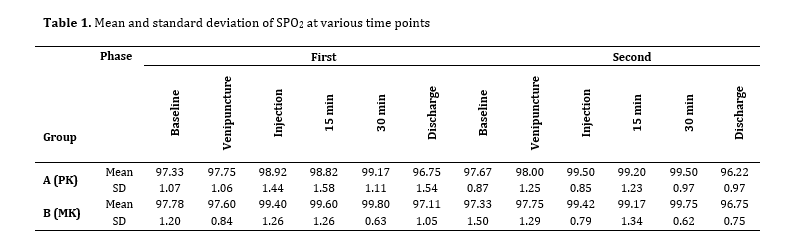
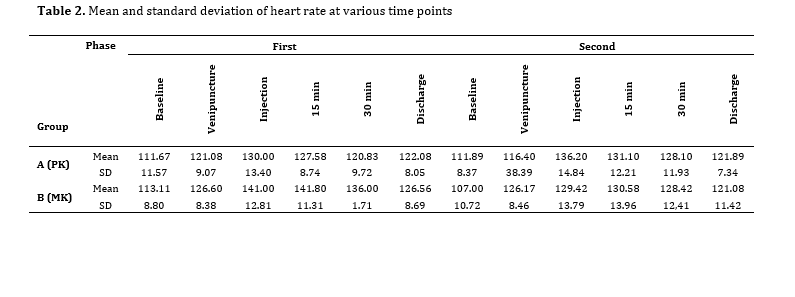
In total, 22 children including 9 girls (40.9%) and 13 boys (51.9%) with a mean age of 3.6±0.97 years and a mean weight of 15.68±2.68 kg were included in data analysis (Figure 1). The mean changes in SPO2 and HR reached the highest at 15 min after local anesthetic injection; details of SPO2 and HR changes at different time points are presented in Tables 1 and 2.
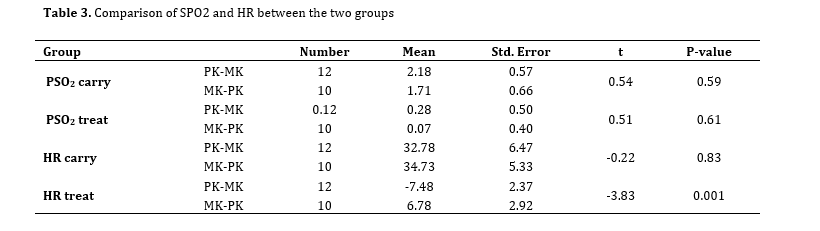
One-sample Kolmogorov-Smirnov test revealed no carry-over effect on the AB (P=0.89) and BA groups (P=0.91). The results revealed no significant difference in level of changes in SPO2 and HR between the first and second sessions (P=0.59 and P=0.83, respectively). The treatment effect on SPO2 was not significantly different between the two groups (P=0.61). However, this effect was significantly different between the groups on HR (P=0.001). The increase in HR was lower when PK was administered compared with MK (Table 3).
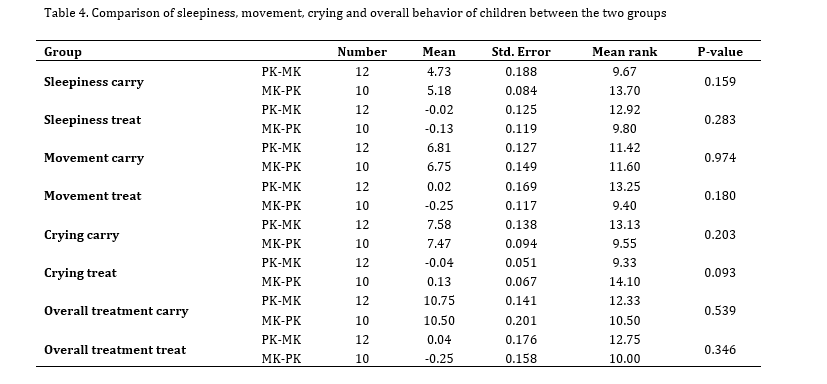
The Mann-Whitney test found no significant difference in the Houpt score of children between the first and second sessions indicative of no carry-over effect. The differences in sleepiness (P=0.16), movement (P=0.97), crying (P=0.20), and overall behavior (P=0.54) were not significant between the two groups. The depth of sedation induced by the two combination drugs did not show any significant difference when assessing children with the same scale (P=0.18, Table 4).
Despite the paucity of the recovery data, the distribution was not normal. Thus, a non-parametric Mann-Whitney test was used to examine the effect of medication type on the recovery time, which showed a significant difference between the two medication groups, such that the recovery time in the PK group was significantly shorter than that in the MK group (P=0.03).
Figure 1. CONSORT flow diagram of patient selection and allocation
Table 1. Mean and standard deviation of SPO2 at various time points
Table 2. Mean and standard deviation of heart rate at various time points
Table 3. Comparison of SPO2 and HR between the two groups
Table 4. Comparison of sleepiness, movement, crying and overall behavior of children between the two groups
Discussion
One-sample Kolmogorov-Smirnov test revealed no carry-over effect on the AB (P=0.89) and BA groups (P=0.91). The results revealed no significant difference in level of changes in SPO2 and HR between the first and second sessions (P=0.59 and P=0.83, respectively). The treatment effect on SPO2 was not significantly different between the two groups (P=0.61). However, this effect was significantly different between the groups on HR (P=0.001). The increase in HR was lower when PK was administered compared with MK (Table 3).
The Mann-Whitney test found no significant difference in the Houpt score of children between the first and second sessions indicative of no carry-over effect. The differences in sleepiness (P=0.16), movement (P=0.97), crying (P=0.20), and overall behavior (P=0.54) were not significant between the two groups. The depth of sedation induced by the two combination drugs did not show any significant difference when assessing children with the same scale (P=0.18, Table 4).
Despite the paucity of the recovery data, the distribution was not normal. Thus, a non-parametric Mann-Whitney test was used to examine the effect of medication type on the recovery time, which showed a significant difference between the two medication groups, such that the recovery time in the PK group was significantly shorter than that in the MK group (P=0.03).
Figure 1. CONSORT flow diagram of patient selection and allocation
{kind=link}
Table 1. Mean and standard deviation of SPO2 at various time points
{kind=link}
Table 2. Mean and standard deviation of heart rate at various time points
{kind=link}
Table 3. Comparison of SPO2 and HR between the two groups
{kind=link}
Table 4. Comparison of sleepiness, movement, crying and overall behavior of children between the two groups
{kind=link}
Discussion
Researchers have long been in search of a desirable cocktail of drugs to provide efficient and safe sedation in children with no consensus. The current results showed no significant difference between the two groups in their efficacy and safety. The oxygen saturation level was stable in almost all steps of the procedure. Ahmed et al. [6] reported 24% incidence of hypoxia in their sedated patients without proper oxygenation and concluded that taking such measures helped resolve the problem.
The current results also showed that the HR in the MK group was significantly higher than that in the PK group, which may be due to the cardiac depressive effects of propofol [1].
Interestingly, Canpolat et al. [7] reported higher HR in the MK than the PK group. Kip et al. [8] stated that higher doses of ketamine were associated with tachycardia. Similarly, Dal et al. [5] reported higher HR associated with MK combination compared to PK. Elevation of HR at the time of catheter placement and injection in their study indicated the presence of pain, and atropine was used rather than sedative drugs. An overall stable HR was within the normal range in both groups, which can be of benefit in patients with tachycardia. Ketamine, as a sedative agent, is known for its sympathomimetic properties and atropine causes an increase in HR while cardiovascular effects of midazolam are minimal and propofol causes a reduction in HR.
Both groups of medications were reasonably effective with no significant difference in their effect on sleepiness, crying, or movement. Following the administration of sedative drug combinations (PK and MK), children showed an increased level of disorientation and drowsiness to complete sleep. The ratings for movement and crying lied in the ranges of no or intermittent crying, and no movement to controllable movement. The dental procedure was completed in both groups, and children presented good to excellent overall behavior. These results are in line with the reports by Dal et al. [5], Ahmed et al. [6], and Canpolat et al. [7]. However, contrary results were reported by Kip et al. [8] who showed that changes in ketamine to propofol dose ratio altered the cooperation level of children, and decreasing the ketamine dose was associated with lower satisfaction of dental clinicians with the level of sedation.
One of the most significant benefits of propofol is its short half-life, which reduces the recovery time. In the present study, the recovery time in the PK group was clearly shorter than that in the MK group [6-9].
Rai et al. [4] showed that propofol was able to quickly sedate; however, its administration was associated with substantial pain at the injection site and children’s crying and movement. Midazolam had a long onset of action and was inefficient for treatment completion as children continued crying and moving. The maximum effect was reported when ketamine was administered since the children were quiet with no movement or crying. It is advised to avoid single drug use for more advanced and lengthier dental procedures as sedation would be short and ineffective. It is best to avoid increasing the dose of a single drug administered and instead use lower doses of two synergic medications to eliminate the risks.
Akbulut et al. [15] reported a higher incidence of side effects in the recovery stage associated with the use of a drug combination. The MK combination required a longer recovery time; while, adding propofol to this combination provided a more effective sedation and reduced the recovery time because of the reduced dose of administered ketamine.
Uludag et al. [10] showed that the KM combination compared to midazolam-propofol provided better hemodynamic variables, although the difference was not significant in terms of patient satisfaction and overall procedural quality. Thus, ketamine, as a hypnotic drug, can be considered useful for pediatric sedation due to its analgesic and anxiolytic properties and high safety margin.
Massaeli et al. [16] reported that propofol is the most commonly used drug for sedation and analgesia in emergency departments, followed by ketamine and etomidate. Adiban et al. [11] indicated that the efficacy of MK was much higher than that of PK despite minor changes in physiological parameters of PK. Chayapathi et al. [17] compared MK with propofol and reported a significantly lower sedative effect in the propofol group which could be explained by its short half-life and absence of maintenance dose.
The cross-over design of the current study minimized the confounding effect of variables such as patients’ behavioral differences by allowing the cases to serve as their own control. Nevertheless, a major limitation of cross-over studies is the carry-over effect. The children’s experience in each treatment session will likely affect their behavior and response in the next session [18]. The potential carry-over effect of this investigation was therefore statistically analyzed, and no statistically significant differences were found between the two sessions based on their presentations according to the Houpt sedation rating scale.
Based on the present data, a shorter recovery time was recorded in those who received PK while the sedation rate of both combinations was almost the same. None of the patients experienced any laryngospasm in the course of treatment. Utmost care taken in correct patient positioning, using a shoulder and head rest, using rubber dam and a high-volume surgical suction, and using a pharyngeal pack would effectively reduce the risk of airway obstruction and adverse reactions during sedation. Administration of atropine has been proven to be helpful by reducing the salivary secretions.
Since there are still controversies on an ideal drug cocktail with maximum sedation efficacy and safety without any side effects and short recovery time, drugs and sedation routes are selected based on the treatment type and duration, patient’s age, general health, and dentist and anesthesiologist’s experience. To date, ketamine and midazolam have been given the highest score among the drugs tested based on the optimal sedative and analgesic properties of ketamine [5] and anxiolytic and amnestic properties of midazolam [19]. This investigation suggests that addition of propofol provides rapid onset of sedation with a shorter recovery time.
Conclusion
The current results also showed that the HR in the MK group was significantly higher than that in the PK group, which may be due to the cardiac depressive effects of propofol [1].
Interestingly, Canpolat et al. [7] reported higher HR in the MK than the PK group. Kip et al. [8] stated that higher doses of ketamine were associated with tachycardia. Similarly, Dal et al. [5] reported higher HR associated with MK combination compared to PK. Elevation of HR at the time of catheter placement and injection in their study indicated the presence of pain, and atropine was used rather than sedative drugs. An overall stable HR was within the normal range in both groups, which can be of benefit in patients with tachycardia. Ketamine, as a sedative agent, is known for its sympathomimetic properties and atropine causes an increase in HR while cardiovascular effects of midazolam are minimal and propofol causes a reduction in HR.
Both groups of medications were reasonably effective with no significant difference in their effect on sleepiness, crying, or movement. Following the administration of sedative drug combinations (PK and MK), children showed an increased level of disorientation and drowsiness to complete sleep. The ratings for movement and crying lied in the ranges of no or intermittent crying, and no movement to controllable movement. The dental procedure was completed in both groups, and children presented good to excellent overall behavior. These results are in line with the reports by Dal et al. [5], Ahmed et al. [6], and Canpolat et al. [7]. However, contrary results were reported by Kip et al. [8] who showed that changes in ketamine to propofol dose ratio altered the cooperation level of children, and decreasing the ketamine dose was associated with lower satisfaction of dental clinicians with the level of sedation.
One of the most significant benefits of propofol is its short half-life, which reduces the recovery time. In the present study, the recovery time in the PK group was clearly shorter than that in the MK group [6-9].
Rai et al. [4] showed that propofol was able to quickly sedate; however, its administration was associated with substantial pain at the injection site and children’s crying and movement. Midazolam had a long onset of action and was inefficient for treatment completion as children continued crying and moving. The maximum effect was reported when ketamine was administered since the children were quiet with no movement or crying. It is advised to avoid single drug use for more advanced and lengthier dental procedures as sedation would be short and ineffective. It is best to avoid increasing the dose of a single drug administered and instead use lower doses of two synergic medications to eliminate the risks.
Akbulut et al. [15] reported a higher incidence of side effects in the recovery stage associated with the use of a drug combination. The MK combination required a longer recovery time; while, adding propofol to this combination provided a more effective sedation and reduced the recovery time because of the reduced dose of administered ketamine.
Uludag et al. [10] showed that the KM combination compared to midazolam-propofol provided better hemodynamic variables, although the difference was not significant in terms of patient satisfaction and overall procedural quality. Thus, ketamine, as a hypnotic drug, can be considered useful for pediatric sedation due to its analgesic and anxiolytic properties and high safety margin.
Massaeli et al. [16] reported that propofol is the most commonly used drug for sedation and analgesia in emergency departments, followed by ketamine and etomidate. Adiban et al. [11] indicated that the efficacy of MK was much higher than that of PK despite minor changes in physiological parameters of PK. Chayapathi et al. [17] compared MK with propofol and reported a significantly lower sedative effect in the propofol group which could be explained by its short half-life and absence of maintenance dose.
The cross-over design of the current study minimized the confounding effect of variables such as patients’ behavioral differences by allowing the cases to serve as their own control. Nevertheless, a major limitation of cross-over studies is the carry-over effect. The children’s experience in each treatment session will likely affect their behavior and response in the next session [18]. The potential carry-over effect of this investigation was therefore statistically analyzed, and no statistically significant differences were found between the two sessions based on their presentations according to the Houpt sedation rating scale.
Based on the present data, a shorter recovery time was recorded in those who received PK while the sedation rate of both combinations was almost the same. None of the patients experienced any laryngospasm in the course of treatment. Utmost care taken in correct patient positioning, using a shoulder and head rest, using rubber dam and a high-volume surgical suction, and using a pharyngeal pack would effectively reduce the risk of airway obstruction and adverse reactions during sedation. Administration of atropine has been proven to be helpful by reducing the salivary secretions.
Since there are still controversies on an ideal drug cocktail with maximum sedation efficacy and safety without any side effects and short recovery time, drugs and sedation routes are selected based on the treatment type and duration, patient’s age, general health, and dentist and anesthesiologist’s experience. To date, ketamine and midazolam have been given the highest score among the drugs tested based on the optimal sedative and analgesic properties of ketamine [5] and anxiolytic and amnestic properties of midazolam [19]. This investigation suggests that addition of propofol provides rapid onset of sedation with a shorter recovery time.
Conclusion
Based on the results of the current study, both sedative regimens were efficiently effective for dental treatment of uncooperative children. Also, the PK combination provided sedation with better hemodynamic stability and shorter recovery.
Acknowledgement
Acknowledgement
The authors would like to thank the Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences for their scientific support. The authors would also like to express their special appreciation to the Late Prof. Shahnaz Shayeghi for her advice and help throughout this work.
Type of Study: Randomized Clinical Trial |
Subject:
pediatric
References
1. Miller RD, Pardo MC. Basics of Anesthesia. 7th ed . Philadelphia PA, Elsevier:2018
2. Malamed SF. Sedation: A guide to patient management. 6th ed. St Louis: Mosby, 2017
3. Casamassimo I, Paul S. Pediatric Dentistry: infancy through adolescence. 6th ed. Philadelphia : Elsevier: 2018
4. Rai K, Hegde AM, Goel K. Sedation in uncooperative children undergoing dental procedures: a comparative evaluation of midazolam, propofol and ketamine. J Clin Pediatr Dent. 2007 Fall;32(1):1-4. [DOI:10.17796/jcpd.32.1.v74872j8n74qu81k] [PMID]
5. Dal T, Sazak H, Tunç M, Sahin S, Yılmaz A. A comparison of ketamine-midazolam and ketamine-propofol combinations used for sedation in the endobronchial ultrasound-guided transbronchial needle aspiration: a prospective, single-blind, randomized study. J Thorac Dis. 2014 Jun;6(6):742-51.
6. Ahmed SS, Hicks SR, Slaven JE, Nitu ME. Deep Sedation for Pediatric Dental Procedures: Is this a Safe and Effective Option? J Clin Pediatr Dent. 2016;40(2):156-60. [DOI:10.17796/1053-4628-40.2.156] [PMID]
7. Canpolat DG, Yildirim MD, Aksu R, Kutuk N, Alkan A, Cantekin K. Intravenous ketamine, propofol and propofol-ketamine combination used for pediatric dental sedation: A randomized clinical study. Pak J Med Sci. 2016 May-Jun;32(3):682-7. [DOI:10.12669/pjms.323.9834]
8. Kip G, Atabek D, Bani M. Comparison of three different ketofol proportions in children undergoing dental treatment. Niger J Clin Pract. 2018 Nov;21(11):1501-7. [DOI:10.4103/njcp.njcp_188_18] [PMID]
9. Dixon C, Aspinall A, Rolfe S, Stevens C. Acceptability of intravenous propofol sedation for adolescent dental care. Eur Arch Paediatr Dent. 2020 Jun;21(3):295-302. [DOI:10.1007/s40368-019-00482-0] [PMID] []
10. Uludağ Ö, Doğukan M, Kaya R, Tutak A, Dumlupınar E. Comparison of the effects of midazolam-ketamine or midazolam-propofol combinations on hemodynamic stability, patient comfort, and post-anesthesia recovery in children undergoing sedation for magnetic resonance imaging procedures. Ain-Shams Journal of Anesthesiology. 2020 Jan 29;12(1). [DOI:10.1186/s42077-019-0037-7]
11. Adiban V, Matin S, Hassanpour-Darghah M, Seyed Sadeghi M, Ghorbanzadeh K. A Comparison of the Sedative Effect of Ketofol and Midazolam-Ketamine Combination in Upper GI Tract Endoscopy in 1-14 Years Childeren. Journal of Ardabil University of Medical Sciences. 2020 Jan 1;20(1):104-15. [DOI:10.29252/jarums.20.1.104]
12. Wallace A, Hodgetts V, Kirby J, Yesudian G, Nasse H, Zaitoun H, et al. Evaluation of a new paediatric dentistry intravenous sedation service. Br Dent J. 2021 Mar 11. [DOI:10.1038/s41415-021-2700-1]
13. Frankl SN. Should the parent remain with the child in the dental operatory?. J. Dent. Child.. 1962;29:150-63.
14. Houpt M. Project USAP the use of sedative agents in pediatric dentistry: 1991 update. Pediatr Dent. 1993 Jan-Feb;15(1):36-40.
15. Akbulut UE, Saylan S, Sengu B, Akcali GE, Erturk E, et al. A comparison of sedation with midazolam-ketamine versus propofol-fentanyl during endoscopy in children: a randomized trial. Eur J Gastroenterol Hepatol. 2017 Jan;29(1):112-8. [DOI:10.1097/MEG.0000000000000751] [PMID] []
16. Massaeli M, Nasouhi S, Motallebzadeh A, Shahabian M. Midazolam, etomidate, propofol, fentanyl, ketamine, and propofol/ketamine for procedural sedation and analgesia among adults in the emergency departments: a systematic review. Shiraz E-Med J. 2020 Jan 1;21:e96024. [DOI:10.5812/semj.96024]
17. Chayapathi V, Kalra M, Bakshi AS, Mahajan A. A comparison of ketamine + midazolam to propofol for procedural sedation for lumbar puncture in pediatric oncology by nonanesthesiologists-a randomized comparative trial. Pediatr Blood Cancer. 2018 Aug;65(8):e27108. [DOI:10.1002/pbc.27108] [PMID]
18. Pandey RK, Padmanabhan MY, Saksena AK, Chandra G. Midazolam-fentanyl analgo-sedation in pediatric dental patients--a pilot study. J Clin Pediatr Dent. 2010 Fall;35(1): 105-10. [DOI:10.17796/jcpd.35.1.t275680587226k66] [PMID]
19. Khader R, Oreadi D, Finkelman M, Jarmoc M, Chaudhary S, Schumann R, Rosenberg M. A prospective randomized controlled trial of two different sedation sequences for third molar removal in adults. J Oral Maxillofac Surg. 2015 Feb;73(2):224-31. [DOI:10.1016/j.joms.2014.08.033] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |