Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 4 (12-2024)
J Res Dent Maxillofac Sci 2024, 9(4): 297-304 |
Back to browse issues page


Ethics code: IR.SBMU.DRC.REC.1398.098
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tahmasbi S, Tavakol Davani S, Namdari M, Atai M. Surface Microhardness, Masking, and Color Stability of white Spot Lesions Infiltrated by Icon versus an Experimental Resin Containing MA-POSS Nanoparticles. J Res Dent Maxillofac Sci 2024; 9 (4) :297-304
URL: http://jrdms.dentaliau.ac.ir/article-1-571-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-571-en.html



1- Department of Orthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Department of Orthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran ,sh.tavakoldavani@gmail.com
3- Department of Community Oral Health, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- DDepartment of Polymer Science, Iran Polymer and Petrochemical Institute (IPPI), Tehran, Iran
2- Department of Orthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran ,
3- Department of Community Oral Health, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- DDepartment of Polymer Science, Iran Polymer and Petrochemical Institute (IPPI), Tehran, Iran
Keywords: Resins, Synthetic, Dental Caries, Polyhedral Oligomeric Silsesquioxane Methacrylate, Tooth Discoloration
Full-Text [PDF 339 kb]
(1022 Downloads)
| Abstract (HTML) (2252 Views)
Table 2. Mean and standard deviation of masking and color stability parameters in the two resin groups at different phases
When enamel pores are filled with Icon resin, the refractive index increases to 1.52; resultantly, the infiltrated lesion would have an appearance resembling that of normal enamel [33].
Paris et al. [7] compared the efficacy of Icon with five experimental resins; they also investigated the relationship between the resin refractive index and its ability to camouflage the lesions. The results showed that the infiltrated lesions had a normal appearance compared with the control group. There was a moderate relationship between the refractive index and lesion camouflage. Therefore, resins with a refractive index similar to that of apatite crystals (sound enamel) may be more effective. However, several parameters such as the depth of lesion and infiltration, lesion activity, complete or incomplete infiltration, polymerization shrinkage, and resin color may also affect the results [7]. The refractive index of the experimental resin in the present study was estimated at 1.46, which was close to the refractive index of Icon (1.52). The colorimetric analysis after infiltration showed no significant deference between the two groups.
Rocha Gomes Torres et al. [34] compared the efficacy of resin infiltration and fluoride remineralization for masking of WSLs. In their study, the camouflage effect of resin infiltration was compared with daily (0.05%) and weekly (2%) use of fluoride mouthwash. They acquired superior results with resin infiltration. In addition, resin infiltration showed the lowest color change following a new acidic challenge after infiltration. Shan et al. [35] compared microabrasion and resin infiltration for WSLs post-orthodontic treatment in a randomized clinical trial. The results showed that the two approaches were not significantly different regarding reduction of WSL size but resin infiltration was more esthetically appealing. In a meta-analysis, resin infiltration was concluded to be moderately superior to fluoride varnish treatment with regard to optical improvement of WSLs [36].
Comparison of resin infiltration with remineralization and conventional oral care indicates that one advantage of resin infiltration is its time efficiency; while, the latter two approaches fail to be effective in the short-term [37-39].
Although ΔE is the most commonly used parameter for color assessment [7, 29, 37], some studies [26, 31] considered the L* parameter (brightness) as the most important parameter in terms of masking of WSLs. According to such studies, demineralization increases the L* parameter; while, resin infiltration decreases it, which is consistent with the results of the present study.
Restorative resins are susceptible to staining over time, which can be affected by water sorption, degree of polymerization, and polishing technique [16]. Also, camphorquinone is usually used as photo-initiator in light-cure materials, which adds a slight yellow tint to insufficiently-cured resin [30]. It was shown that specimens infiltrated with resin were more susceptible to staining compared with those treated with microabrasion [27] and remineralization [16].
Polishing of an infiltrated lesion increases its color stability, which is probably due to the reduction of surface roughness and porosities, as well as the removal of oxygen-inhibited layer [7]. The results of the present study revealed that the color stability of the experimental resin group was lower than desired, although it was not significantly different from the Icon group. Safaei et al. [40] reported that addition of MA-POSS nanoparticles to resin materials slightly decreased their degree of polymerization. Thus, higher staining in the experimental group may be related to the lower degree of polymerization and consequently undesirable yellow tint of camphorquinone.
MalekiGorji et al. [41] sought a more domestically accessible method to resolve tooth discoloration using 18% HCl (Kimia, Iran) instead of 15% HCl (Icon-Etch®, DMG, USA) for etching prior to resin infiltration or microabrasion. They indicated that 18% HCl group was more effective as it caused a greater depth of erosion in a shorter period; thus, it may be used to improve the results of our experimental resin. Further investigations are recommended to assess the wear and penetration depth of our experimental resin.
Conclusion
The experimental resin has comparable masking, color stability, and surface microhardness improvement to that of Icon with the main advantage of easier availability in Iran. Further investigations are recommended to be carried out to test its wear and penetration depth.
Full-Text: (609 Views)
Abstract
Background and Aim: This study compared the efficacy of an experimental resin containing polyhedral oligomeric silsesquioxane (POSS) nanoparticles with methacrylate groups (MA-POSS) versus the Icon resin regarding the masking, color stability, and microhardness of artificially induced white spot lesions (WSLs).
Materials and Methods: In this in vitro study, 60 bovine enamel specimens were assigned to two groups for assessment of color (group C) and surface microhardness (group H). white spot lesions were induced on the specimens using demineralizing and remineralizing solutions. Each group was divided into two subgroups for the application of experimental resin and Icon. the color and surface microhardness of specimens were measured, after the induction of WSLs, and after infiltration. Group C samples were immersed in coffee (1 hour/day for one week) and their color was measured again. ANCOVA was used to compare microhardness between the two resin groups. To compare the masking and staining of infiltrated lesions, ΔE, ΔL and L* values after infiltration and staining were compared with the values after the induction of WSLs using independent t-test and repeated measures ANCOVA (α=0.05).
Results: Microhardness analysis by ANCOVA revealed no significant difference between the groups following resin infiltration (P=0.144). The performance of the two resins after infiltration (P=0.75 for ΔE, P=0.20 for ΔL, P=0.57 for L*) and after staining (P=0.31 for ΔE, P=0.07 for ΔL, P=0.32 for L*) was not significantly different.
Conclusion: The experimental resin was comparable to Icon with the main advantage of easier availability in Iran.
Keywords: Resins, Synthetic; Dental Caries; Polyhedral Oligomeric Silsesquioxane Methacrylate; Tooth Discoloration
Introduction
As time passes since the onset of orthodontic treatment, qualitative and quantitative changes occur in the oral microbiota, leading to an increase in cariogenic bacteria [1]. Fixed appliances are the most commonly used modality in orthodontic treatment, which may increase the risk of development of white spot lesions (WSLs), and bring about poor esthetic outcomes [2]. In addition to optimal oral hygiene, some other preventive measures such as the use of fluoride-releasing bonding agents, and daily use of 0.05% sodium fluoride and chlorhexidine mouthwashes are often recommended to prevent WSLs [3,4]. Despite the implementation of these protocols, approximately 46% of patients with fixed orthodontic appliances show at least one WSL within 12 months after the treatment onset [5]. In a previous study on an Iranian population, 90.5% of patients had at least one WSL. The highest prevalence belonged to the maxillary lateral incisors (37%-48%) [6].
Incipient carious lesions may be managed by the application of fluoride or casein phosphopeptide amorphous calcium phosphate to reverse demineralization. These techniques are effective to arrest caries progression [7] but with no improvement in esthetics [8]. In addition, the hypermineralized outer enamel layer prevents remineralization of the subsurface lesions [9]. Microabrasion is indicated for shallow WSLs but it technically requires the elimination of the outer enamel layer, which can be remineralized. Furthermore, composite or ceramic restorations have excellent esthetic results, but require the removal of sound tooth structure. Therefore, considering the reversible nature of WSLs, conservative approaches are preferred for their management [10, 11].
Low-viscosity light-cure resin infiltration is a promising treatment option for WSLs [12], which was commenced by the introduction of Icon (DMG, Hamburg, Germany) in 2009 [13]. After etching of the apparently normal superficial layer, the low-viscosity resin penetrates the lesion by the capillary forces and decreases the infiltration of acids and mineral dissolution by occluding the pores. Thus, the process of caries progression is decelerated or stopped [14]. The cured resin also mechanically stabilizes the fragile crystalline structure of hydroxyapatite and prevents its collapse [15]. The infiltrated resin has a refractive index similar to that of apatite crystals, leading to lower light scattering and minimal color difference with the enamel [7]; therefore, resin infiltration would conceal the unsightly carious lesions [16]. Performing resin infiltration on tooth surfaces prior to orthodontic treatment could also reduce interfacial microleakage between teeth and bonded orthodontic brackets, and may lower the prevalence of WSLs [17].
Polyhedral oligomeric silsesquioxane (POSS) nanoparticles have a well-defined architecture and variable size ranging from 1-3 nm. They are considered as the smallest version of silica particles [18, 19]. The biocompatibility and non-toxic nature of POSS have been previously confirmed ensuring its safe incorporation into the formulation of resins [20-22]. Polymers containing POSS derivatives have higher thermal stability, oxidation resistance, glass transition temperature, and surface microhardness, and lower flammability and viscosity [13, 23]. This study aimed to investigate the efficacy of a newly developed resin containing POSS nanoparticles with methacrylate groups (MA-POSS) and compare it with the Icon infiltration resin regarding the masking, color stability, and surface microhardness of artificially induced WSLs.
Materials and Methods
The ethics committee of Shahid Beheshti University of Medical Sciences approved the protocol of this in vitro, experimental study (IR.SBMU.DRC.REC.1398.098).
A pilot study was initially performed to find the most appropriate resin by comparing resins containing 1%, 3%, and 5% MA-POSS nanoparticles. The surface microhardness and color of WSLs were recorded at baseline, after artificial induction of WSLs, and following resin infiltration. The results revealed that the performance of the experimental resin with 3% MA-POSS nanoparticles was more similar to that of Icon; therefore, this resin was selected for further evaluation.
Specimen preparation:
Twenty-four extracted permanent bovine incisors were stored in distilled water. The crowns were cut by a high-speed handpiece; depending on the size, each crown was sectioned into 2, 3, or 4 slices. The specimens for color assessment (group C) were obtained from the incisal half while the specimens for the surface microhardness assessment (group H) were obtained from the cervical half of the crowns. The specimens were mounted in wax (Figure 1) and auto-polymerizing acrylic resin (Acropars, Iran) (Figure 2), with their labial surface parallel to the horizon. Next, windows were created by sticking 3 x 3 mm labels on the specimens in group H, while other parts were covered with acid-resistant nail varnish (Mavala, Switzerland) (Figure 2). The labels were placed on areas free from cracks and parallel to the horizon regardless of the tooth convexity.
Each specimen was then polished with pumice paste and low-speed handpiece for 20 seconds, followed by using 400-, 600-, 800- and 1200-grit silicium carbide abrasive papers (Matador, Germany), each for 20 seconds. Thirty specimens in group C and 30 specimens in group H were randomly assigned to two subgroups (n=15) by using the RAND function of Excel; the specimens in subgroup I were infiltrated with Icon (DMG, Hamburg, Germany) while the specimens in subgroup R were infiltrated with the experimental resin.
Figure 1. A specimen mounted in wax for colorimetry: (A) top view, (B) side view
Figure 2. A specimen mounted in auto-polymerizing acrylic resin after nail varnish application and removing the label for microhardness testing
Artificial induction of WSLs:
All specimens (60 enamel sections) were immersed in a demineralizing solution composed of 1.5 mM CaCl2, 0.9 mM KH2PO4, 50 mM acetic acid, and KOH (School of Dentistry of Tehran University of Medical Sciences, Tehran, Iran) to adjust the pH at 5 for 2 weeks [24]. The specimens were then immersed in a demineralizing solution with a pH of 4 with daily renewal for one additional week. The specimens were subsequently immersed in a remineralizing solution (1.5 mM CaCl2, 0.9 mM NaH2PO4, 0.15 mM KCl, pH = 7) for one week [25].
Resin infiltration:
The specimens were etched with 15% HCL gel (Icon Etch) for 2 minutes in the Icon group, and with 37% H3PO4 gel (Morva Etch, Iran) for 30 seconds in the experimental resin group [18], and rinsed with air-water spray for 30 seconds. The lesions were dried with 100% ethanol for 30 seconds, the resin was applied by a microbrush for 3 minutes, the tooth surface was gently sprayed for 10 seconds, and then curing was performed for 40 seconds. Resin was then reapplied for 3 minutes and cured for 40 seconds.
After resin infiltration, the specimens were polished with 1200-grit abrasive paper to remove excess resin and were then immersed in distilled water [26].
Staining:
To evaluate the color stability of resins, the specimens in group C were immersed in coffee solution (pH = 5) for one hour daily for one week [27]. The specimens were then polished with 1200-grit abrasive paper and immersed in distilled water.
Surface microhardness testing:
Microhardness was measured by a Vickers hardness tester (ZHVµ; Zwick Roell, UK) at the WSL induction and infiltration phases as follows: Indentations were created at three points (200 g, 10 seconds) yielding 3 hardness numbers for each specimen. Then, the mean of the three values was calculated and recorded as the microhardness number of each specimen [28].
Color assessment:
The color of WSLs was recorded using a spectrophotometer (Xrite, CIX6, USA) at baseline, after WSL induction, after resin infiltration, and after staining. The L*, a* and b* color parameters were measured. A gray card (18% gray) was used as the reference to standardize the lighting conditions. The CIE L*a*b* color space describes the color parameters in three dimensions: brightness (L*; 0-100), green-red spectrum (a*; -150 to +100) and blue-yellow spectrum (b*; -100 to +150) [10]. The color was recorded through a 6-mm circular valve, and the color change (ΔE) was automatically calculated using the following formula: ΔE = [(ΔL*)2 + (Δa*)2+ (Δb*)2]1/2 [26, 29, 30].
Post-infiltration color improvement and stability were assessed by spectrophotometry. The same procedure was performed after staining. In addition to ΔE, some studies [26, 31] used L* and ΔL (brightness value) to assess the effectiveness of infiltrating resin to mask the WSLs. Therefore, we calculated these parameters in the present study as well.
Statistical analysis:
Data analysis was performed using SPSS version 21.0 (SPSS Inc., IL, USA). The mean (± standard deviation) value was reported for the tested parameters. ANCOVA was applied to compare the experimental resin with Icon regarding microhardness, and also in order to adjust the effect of specimens’ microhardness before resin infiltration (after WSL induction) on the results. The ΔL and ΔE values were assessed in the resin infiltration and staining phases compared with the WSL induction phase. These values were compared between the Icon and experimental resin groups by independent t-test. The significance level was set at α=0.05.
Results
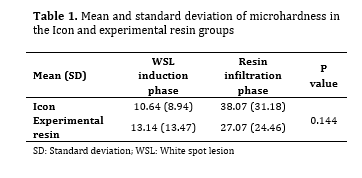
Table 1 shows the mean and standard deviation of microhardness after the induction of WSLs, and after resin infiltration. Comparison of the microhardness of Icon and experimental resin groups by ANCOVA at the resin infiltration phase showed no significant difference (P=0.144).
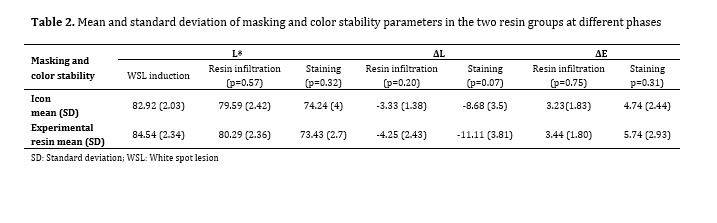
To compare the L* values between the experimental resin and Icon groups in the resin infiltration and staining phases, repeated measures ANCOVA was applied, and the L* value at the WSL induction phase was adjusted in statistical analysis. The effect of type of resin was compared in the resin infiltration and staining phases by the Bonferroni adjustment, which showed that there was no significant difference in L* parameter between the two resins at the resin infiltration and staining phases (P=0.57 and P=0.32, respectively; Table 2).
In order to compare the efficacy of Icon and the experimental resin, ΔE and ΔL were compared by independent t-test at the resin infiltration and staining phases. Considering the baseline values (WSL induction), no difference was found between the two groups (P>0.05, Table 2).
Table 1. Mean and standard deviation of microhardness in the Icon and experimental resin groups
Background and Aim: This study compared the efficacy of an experimental resin containing polyhedral oligomeric silsesquioxane (POSS) nanoparticles with methacrylate groups (MA-POSS) versus the Icon resin regarding the masking, color stability, and microhardness of artificially induced white spot lesions (WSLs).
Materials and Methods: In this in vitro study, 60 bovine enamel specimens were assigned to two groups for assessment of color (group C) and surface microhardness (group H). white spot lesions were induced on the specimens using demineralizing and remineralizing solutions. Each group was divided into two subgroups for the application of experimental resin and Icon. the color and surface microhardness of specimens were measured, after the induction of WSLs, and after infiltration. Group C samples were immersed in coffee (1 hour/day for one week) and their color was measured again. ANCOVA was used to compare microhardness between the two resin groups. To compare the masking and staining of infiltrated lesions, ΔE, ΔL and L* values after infiltration and staining were compared with the values after the induction of WSLs using independent t-test and repeated measures ANCOVA (α=0.05).
Results: Microhardness analysis by ANCOVA revealed no significant difference between the groups following resin infiltration (P=0.144). The performance of the two resins after infiltration (P=0.75 for ΔE, P=0.20 for ΔL, P=0.57 for L*) and after staining (P=0.31 for ΔE, P=0.07 for ΔL, P=0.32 for L*) was not significantly different.
Conclusion: The experimental resin was comparable to Icon with the main advantage of easier availability in Iran.
Keywords: Resins, Synthetic; Dental Caries; Polyhedral Oligomeric Silsesquioxane Methacrylate; Tooth Discoloration
Introduction
As time passes since the onset of orthodontic treatment, qualitative and quantitative changes occur in the oral microbiota, leading to an increase in cariogenic bacteria [1]. Fixed appliances are the most commonly used modality in orthodontic treatment, which may increase the risk of development of white spot lesions (WSLs), and bring about poor esthetic outcomes [2]. In addition to optimal oral hygiene, some other preventive measures such as the use of fluoride-releasing bonding agents, and daily use of 0.05% sodium fluoride and chlorhexidine mouthwashes are often recommended to prevent WSLs [3,4]. Despite the implementation of these protocols, approximately 46% of patients with fixed orthodontic appliances show at least one WSL within 12 months after the treatment onset [5]. In a previous study on an Iranian population, 90.5% of patients had at least one WSL. The highest prevalence belonged to the maxillary lateral incisors (37%-48%) [6].
Incipient carious lesions may be managed by the application of fluoride or casein phosphopeptide amorphous calcium phosphate to reverse demineralization. These techniques are effective to arrest caries progression [7] but with no improvement in esthetics [8]. In addition, the hypermineralized outer enamel layer prevents remineralization of the subsurface lesions [9]. Microabrasion is indicated for shallow WSLs but it technically requires the elimination of the outer enamel layer, which can be remineralized. Furthermore, composite or ceramic restorations have excellent esthetic results, but require the removal of sound tooth structure. Therefore, considering the reversible nature of WSLs, conservative approaches are preferred for their management [10, 11].
Low-viscosity light-cure resin infiltration is a promising treatment option for WSLs [12], which was commenced by the introduction of Icon (DMG, Hamburg, Germany) in 2009 [13]. After etching of the apparently normal superficial layer, the low-viscosity resin penetrates the lesion by the capillary forces and decreases the infiltration of acids and mineral dissolution by occluding the pores. Thus, the process of caries progression is decelerated or stopped [14]. The cured resin also mechanically stabilizes the fragile crystalline structure of hydroxyapatite and prevents its collapse [15]. The infiltrated resin has a refractive index similar to that of apatite crystals, leading to lower light scattering and minimal color difference with the enamel [7]; therefore, resin infiltration would conceal the unsightly carious lesions [16]. Performing resin infiltration on tooth surfaces prior to orthodontic treatment could also reduce interfacial microleakage between teeth and bonded orthodontic brackets, and may lower the prevalence of WSLs [17].
Polyhedral oligomeric silsesquioxane (POSS) nanoparticles have a well-defined architecture and variable size ranging from 1-3 nm. They are considered as the smallest version of silica particles [18, 19]. The biocompatibility and non-toxic nature of POSS have been previously confirmed ensuring its safe incorporation into the formulation of resins [20-22]. Polymers containing POSS derivatives have higher thermal stability, oxidation resistance, glass transition temperature, and surface microhardness, and lower flammability and viscosity [13, 23]. This study aimed to investigate the efficacy of a newly developed resin containing POSS nanoparticles with methacrylate groups (MA-POSS) and compare it with the Icon infiltration resin regarding the masking, color stability, and surface microhardness of artificially induced WSLs.
Materials and Methods
The ethics committee of Shahid Beheshti University of Medical Sciences approved the protocol of this in vitro, experimental study (IR.SBMU.DRC.REC.1398.098).
A pilot study was initially performed to find the most appropriate resin by comparing resins containing 1%, 3%, and 5% MA-POSS nanoparticles. The surface microhardness and color of WSLs were recorded at baseline, after artificial induction of WSLs, and following resin infiltration. The results revealed that the performance of the experimental resin with 3% MA-POSS nanoparticles was more similar to that of Icon; therefore, this resin was selected for further evaluation.
Specimen preparation:
Twenty-four extracted permanent bovine incisors were stored in distilled water. The crowns were cut by a high-speed handpiece; depending on the size, each crown was sectioned into 2, 3, or 4 slices. The specimens for color assessment (group C) were obtained from the incisal half while the specimens for the surface microhardness assessment (group H) were obtained from the cervical half of the crowns. The specimens were mounted in wax (Figure 1) and auto-polymerizing acrylic resin (Acropars, Iran) (Figure 2), with their labial surface parallel to the horizon. Next, windows were created by sticking 3 x 3 mm labels on the specimens in group H, while other parts were covered with acid-resistant nail varnish (Mavala, Switzerland) (Figure 2). The labels were placed on areas free from cracks and parallel to the horizon regardless of the tooth convexity.
Each specimen was then polished with pumice paste and low-speed handpiece for 20 seconds, followed by using 400-, 600-, 800- and 1200-grit silicium carbide abrasive papers (Matador, Germany), each for 20 seconds. Thirty specimens in group C and 30 specimens in group H were randomly assigned to two subgroups (n=15) by using the RAND function of Excel; the specimens in subgroup I were infiltrated with Icon (DMG, Hamburg, Germany) while the specimens in subgroup R were infiltrated with the experimental resin.
Figure 1. A specimen mounted in wax for colorimetry: (A) top view, (B) side view
{kind=link}
Figure 2. A specimen mounted in auto-polymerizing acrylic resin after nail varnish application and removing the label for microhardness testing
{kind=link}
Artificial induction of WSLs:
All specimens (60 enamel sections) were immersed in a demineralizing solution composed of 1.5 mM CaCl2, 0.9 mM KH2PO4, 50 mM acetic acid, and KOH (School of Dentistry of Tehran University of Medical Sciences, Tehran, Iran) to adjust the pH at 5 for 2 weeks [24]. The specimens were then immersed in a demineralizing solution with a pH of 4 with daily renewal for one additional week. The specimens were subsequently immersed in a remineralizing solution (1.5 mM CaCl2, 0.9 mM NaH2PO4, 0.15 mM KCl, pH = 7) for one week [25].
Resin infiltration:
The specimens were etched with 15% HCL gel (Icon Etch) for 2 minutes in the Icon group, and with 37% H3PO4 gel (Morva Etch, Iran) for 30 seconds in the experimental resin group [18], and rinsed with air-water spray for 30 seconds. The lesions were dried with 100% ethanol for 30 seconds, the resin was applied by a microbrush for 3 minutes, the tooth surface was gently sprayed for 10 seconds, and then curing was performed for 40 seconds. Resin was then reapplied for 3 minutes and cured for 40 seconds.
After resin infiltration, the specimens were polished with 1200-grit abrasive paper to remove excess resin and were then immersed in distilled water [26].
Staining:
To evaluate the color stability of resins, the specimens in group C were immersed in coffee solution (pH = 5) for one hour daily for one week [27]. The specimens were then polished with 1200-grit abrasive paper and immersed in distilled water.
Surface microhardness testing:
Microhardness was measured by a Vickers hardness tester (ZHVµ; Zwick Roell, UK) at the WSL induction and infiltration phases as follows: Indentations were created at three points (200 g, 10 seconds) yielding 3 hardness numbers for each specimen. Then, the mean of the three values was calculated and recorded as the microhardness number of each specimen [28].
Color assessment:
The color of WSLs was recorded using a spectrophotometer (Xrite, CIX6, USA) at baseline, after WSL induction, after resin infiltration, and after staining. The L*, a* and b* color parameters were measured. A gray card (18% gray) was used as the reference to standardize the lighting conditions. The CIE L*a*b* color space describes the color parameters in three dimensions: brightness (L*; 0-100), green-red spectrum (a*; -150 to +100) and blue-yellow spectrum (b*; -100 to +150) [10]. The color was recorded through a 6-mm circular valve, and the color change (ΔE) was automatically calculated using the following formula: ΔE = [(ΔL*)2 + (Δa*)2+ (Δb*)2]1/2 [26, 29, 30].
Post-infiltration color improvement and stability were assessed by spectrophotometry. The same procedure was performed after staining. In addition to ΔE, some studies [26, 31] used L* and ΔL (brightness value) to assess the effectiveness of infiltrating resin to mask the WSLs. Therefore, we calculated these parameters in the present study as well.
Statistical analysis:
Data analysis was performed using SPSS version 21.0 (SPSS Inc., IL, USA). The mean (± standard deviation) value was reported for the tested parameters. ANCOVA was applied to compare the experimental resin with Icon regarding microhardness, and also in order to adjust the effect of specimens’ microhardness before resin infiltration (after WSL induction) on the results. The ΔL and ΔE values were assessed in the resin infiltration and staining phases compared with the WSL induction phase. These values were compared between the Icon and experimental resin groups by independent t-test. The significance level was set at α=0.05.
Results
Table 1 shows the mean and standard deviation of microhardness after the induction of WSLs, and after resin infiltration. Comparison of the microhardness of Icon and experimental resin groups by ANCOVA at the resin infiltration phase showed no significant difference (P=0.144).
To compare the L* values between the experimental resin and Icon groups in the resin infiltration and staining phases, repeated measures ANCOVA was applied, and the L* value at the WSL induction phase was adjusted in statistical analysis. The effect of type of resin was compared in the resin infiltration and staining phases by the Bonferroni adjustment, which showed that there was no significant difference in L* parameter between the two resins at the resin infiltration and staining phases (P=0.57 and P=0.32, respectively; Table 2).
In order to compare the efficacy of Icon and the experimental resin, ΔE and ΔL were compared by independent t-test at the resin infiltration and staining phases. Considering the baseline values (WSL induction), no difference was found between the two groups (P>0.05, Table 2).
Table 1. Mean and standard deviation of microhardness in the Icon and experimental resin groups
{kind=link}
Discussion
WSL infiltration aims to fill the porosities in the body of lesions and inhibit caries progression. Resin infiltration could also be beneficial with regards to improving enamel resistance to acid attacks as it forms a hybrid layer [32]. Increased microhardness after resin infiltration indicates the ability of low-viscosity resin to fill the gaps between the pores and the remaining crystals [28].
The MA-POSS nanoparticles were used in the present study to synthesize a resin with similar or superior features compared with Icon infiltration resin. Studies have demonstrated that these nanoparticles can also increase the surface microhardness [14, 23]. Therefore, the authors expected a surface microhardness similar to, or higher than that in the Icon group. Mandava et al. [28] evaluated the surface microhardness of artificial WSLs infiltrated with Icon resin compared with colloidal silica nanoparticles. The results showed that the microhardness of the Icon-infiltrated group was significantly higher than that of the colloidal silica group. In another study, Belli et al. [15] investigated the wear resistance and morphology of lesions infiltrated with Icon compared with a commercial etch-and-rinse resin (Scotchbond 1TX; 3M ESPE, St. Paul, MN, USA). Although the wear resistance was the same in both groups, Icon showed superior outcomes in terms of surface morphology, strength, and infiltration quality. However, our experimental resin showed no significant difference with Icon regarding surface microhardness.
Cariogenic acids increase the enamel surface porosities and create a chalky white appearance. Due to the replacement of air with water in inter-crystalline spaces, incipient carious lesions need to be air-dried in order to be clinically visible. Normal enamel has a refractive index of approximately 1.62; while the refractive index of water and air is 1.33 and 1, respectively. Therefore, greater difference in the refractive index results in more opaque enamel surface, which is easily detectable [16, 33].
WSL infiltration aims to fill the porosities in the body of lesions and inhibit caries progression. Resin infiltration could also be beneficial with regards to improving enamel resistance to acid attacks as it forms a hybrid layer [32]. Increased microhardness after resin infiltration indicates the ability of low-viscosity resin to fill the gaps between the pores and the remaining crystals [28].
The MA-POSS nanoparticles were used in the present study to synthesize a resin with similar or superior features compared with Icon infiltration resin. Studies have demonstrated that these nanoparticles can also increase the surface microhardness [14, 23]. Therefore, the authors expected a surface microhardness similar to, or higher than that in the Icon group. Mandava et al. [28] evaluated the surface microhardness of artificial WSLs infiltrated with Icon resin compared with colloidal silica nanoparticles. The results showed that the microhardness of the Icon-infiltrated group was significantly higher than that of the colloidal silica group. In another study, Belli et al. [15] investigated the wear resistance and morphology of lesions infiltrated with Icon compared with a commercial etch-and-rinse resin (Scotchbond 1TX; 3M ESPE, St. Paul, MN, USA). Although the wear resistance was the same in both groups, Icon showed superior outcomes in terms of surface morphology, strength, and infiltration quality. However, our experimental resin showed no significant difference with Icon regarding surface microhardness.
Cariogenic acids increase the enamel surface porosities and create a chalky white appearance. Due to the replacement of air with water in inter-crystalline spaces, incipient carious lesions need to be air-dried in order to be clinically visible. Normal enamel has a refractive index of approximately 1.62; while the refractive index of water and air is 1.33 and 1, respectively. Therefore, greater difference in the refractive index results in more opaque enamel surface, which is easily detectable [16, 33].
Table 2. Mean and standard deviation of masking and color stability parameters in the two resin groups at different phases
{kind=link}
When enamel pores are filled with Icon resin, the refractive index increases to 1.52; resultantly, the infiltrated lesion would have an appearance resembling that of normal enamel [33].
Paris et al. [7] compared the efficacy of Icon with five experimental resins; they also investigated the relationship between the resin refractive index and its ability to camouflage the lesions. The results showed that the infiltrated lesions had a normal appearance compared with the control group. There was a moderate relationship between the refractive index and lesion camouflage. Therefore, resins with a refractive index similar to that of apatite crystals (sound enamel) may be more effective. However, several parameters such as the depth of lesion and infiltration, lesion activity, complete or incomplete infiltration, polymerization shrinkage, and resin color may also affect the results [7]. The refractive index of the experimental resin in the present study was estimated at 1.46, which was close to the refractive index of Icon (1.52). The colorimetric analysis after infiltration showed no significant deference between the two groups.
Rocha Gomes Torres et al. [34] compared the efficacy of resin infiltration and fluoride remineralization for masking of WSLs. In their study, the camouflage effect of resin infiltration was compared with daily (0.05%) and weekly (2%) use of fluoride mouthwash. They acquired superior results with resin infiltration. In addition, resin infiltration showed the lowest color change following a new acidic challenge after infiltration. Shan et al. [35] compared microabrasion and resin infiltration for WSLs post-orthodontic treatment in a randomized clinical trial. The results showed that the two approaches were not significantly different regarding reduction of WSL size but resin infiltration was more esthetically appealing. In a meta-analysis, resin infiltration was concluded to be moderately superior to fluoride varnish treatment with regard to optical improvement of WSLs [36].
Comparison of resin infiltration with remineralization and conventional oral care indicates that one advantage of resin infiltration is its time efficiency; while, the latter two approaches fail to be effective in the short-term [37-39].
Although ΔE is the most commonly used parameter for color assessment [7, 29, 37], some studies [26, 31] considered the L* parameter (brightness) as the most important parameter in terms of masking of WSLs. According to such studies, demineralization increases the L* parameter; while, resin infiltration decreases it, which is consistent with the results of the present study.
Restorative resins are susceptible to staining over time, which can be affected by water sorption, degree of polymerization, and polishing technique [16]. Also, camphorquinone is usually used as photo-initiator in light-cure materials, which adds a slight yellow tint to insufficiently-cured resin [30]. It was shown that specimens infiltrated with resin were more susceptible to staining compared with those treated with microabrasion [27] and remineralization [16].
Polishing of an infiltrated lesion increases its color stability, which is probably due to the reduction of surface roughness and porosities, as well as the removal of oxygen-inhibited layer [7]. The results of the present study revealed that the color stability of the experimental resin group was lower than desired, although it was not significantly different from the Icon group. Safaei et al. [40] reported that addition of MA-POSS nanoparticles to resin materials slightly decreased their degree of polymerization. Thus, higher staining in the experimental group may be related to the lower degree of polymerization and consequently undesirable yellow tint of camphorquinone.
MalekiGorji et al. [41] sought a more domestically accessible method to resolve tooth discoloration using 18% HCl (Kimia, Iran) instead of 15% HCl (Icon-Etch®, DMG, USA) for etching prior to resin infiltration or microabrasion. They indicated that 18% HCl group was more effective as it caused a greater depth of erosion in a shorter period; thus, it may be used to improve the results of our experimental resin. Further investigations are recommended to assess the wear and penetration depth of our experimental resin.
Conclusion
The experimental resin has comparable masking, color stability, and surface microhardness improvement to that of Icon with the main advantage of easier availability in Iran. Further investigations are recommended to be carried out to test its wear and penetration depth.
Type of Study: Original article |
Subject:
orthodontic
References
1. Santonocito S, Polizzi A. Oral Microbiota Changes during Orthodontic Treatment. Front Biosci (Elite Ed). 2022 Jul 27;14(3):19. [DOI:10.31083/j.fbe1403019] [PMID]
2. Knösel M, Eckstein A, Helms HJ. Durability of esthetic improvement following Icon resin infiltration of multibracket-induced white spot lesions compared with no therapy over 6 months: a single-center, split-mouth, randomized clinical trial. Am J Orthod Dentofacial Orthop. 2013 Jul;144(1):86-96. [DOI:10.1016/j.ajodo.2013.02.029] [PMID]
3. Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed brace treatment. Cochrane Database Syst Rev. 2004;(3):CD003809. [DOI:10.1002/14651858.CD003809.pub2]
4. Øgaard B, Larsson E, Henriksson T, Birkhed D, Bishara SE. Effects of combined application of antimicrobial and fluoride varnishes in orthodontic patients. Am J Orthod Dentofacial Orthop. 2001 Jul;120(1):28-35. [DOI:10.1067/mod.2001.114644] [PMID]
5. Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 2011 Mar;81(2):206-10. [DOI:10.2319/051710-262.1] [PMID] []
6. Mojtahedzadeh F, Heshmat H, Sheibani Nia A, Kharazi Fard M J, Mahmoud Hashemi T, Moravej Salehi E. Investigating The Prevalence of White Spot Lesions and Related Factors in Orthodontic Patients of Two Orthodontic Departments. J Res Dent Sci 2012;9(2):80-6.
7. Paris S, Schwendicke F, Keltsch J, Dörfer C, Meyer-Lueckel H. Masking of white spot lesions by resin infiltration in vitro. J Dent. 2013 Nov;41 Suppl 5:e28-34. [DOI:10.1016/j.jdent.2013.04.003] [PMID]
8. Bailey DL, Adams GG, Tsao CE, Hyslop A, Escobar K, Manton DJ, et al. Regression of post-orthodontic lesions by a remineralizing cream. J Dent Res. 2009 Dec;88(12):1148-53. [DOI:10.1177/0022034509347168] [PMID]
9. Naumova EA, Niemann N, Aretz L, Arnold WH. Effects of different amine fluoride concentrations on enamel remineralization. J Dent. 2012 Sep;40(9):750-5. [DOI:10.1016/j.jdent.2012.05.006] [PMID]
10. Waggoner WF, Johnston WM, Schumann S, Schikowski E. Microabrasion of human enamel in vitro using hydrochloric acid and pumice. Pediatr Dent. 1989 Dec;11(4):319-23.
11. Wong FS, Winter GB. Effectiveness of microabrasion technique for improvement of dental aesthetics. Br Dent J. 2002 Aug 10;193(3):155-8. [DOI:10.1038/sj.bdj.4801511a] [PMID]
12. Paris S, Meyer-Lueckel H, Kielbassa AM. Resin infiltration of natural caries lesions. J Dent Res. 2007 Jul;86(7):662-6. [DOI:10.1177/154405910708600715] [PMID]
13. Doméjean S, Ducamp R, Léger S, Holmgren C. Resin infiltration of non-cavitated caries lesions: a systematic review. Med Princ Pract. 2015;24(3):216-21. [DOI:10.1159/000371709] [PMID] []
14. Sulca NM, Adriana L, Popescu R, Sorina G, Iovu H. New Polymeric Nanocomposites Based on Polyhedral Oligomeric Silsesquioxanes. Materiale Plastice. 2009;46(1).
15. Belli R, Rahiotis C, Schubert EW, Baratieri LN, Petschelt A, Lohbauer U. Wear and morphology of infiltrated white spot lesions. J Dent. 2011 May;39(5):376-85. [DOI:10.1016/j.jdent.2011.02.009] [PMID]
16. Cohen-Carneiro F, Pascareli AM, Christino MR, Vale HF, Pontes DG. Color stability of carious incipient lesions located in enamel and treated with resin infiltration or remineralization. Int J Paediatr Dent. 2014 Jul;24(4):277-85. [DOI:10.1111/ipd.12071] [PMID]
17. Qibi LH, Hasan LA, Dewachi Z. Influence of resin infiltration pretreatment on the microleakage under orthodontic bracket (an in vitro study). J Orthod Sci. 2023 Sep 4;12:43. [DOI:10.4103/jos.jos_102_22] [PMID] []
18. Lopez T, Bosch P, Navarrete J, Asomoza M, Gomez R. Structure of Pd/SiO2 sol-gel and impregnated catalysts. J Solgel Sci Technol. 1994;1(2):193-203. [DOI:10.1007/BF00490249]
19. Pan G. Physical Properties of Polymers Handbook. SpringerMaterials; 2007. doi:10.1007/978-0-387-69002-5_34 [DOI:10.1007/978-0-387-69002-5_34]
20. John Ł. Selected developments and medical applications of organic-inorganic hybrid biomaterials based on functionalized spherosilicates. Mater Sci Eng C Mater Biol Appl. 2018 Jul 1;88:172-81. [DOI:10.1016/j.msec.2018.02.007] [PMID]
21. Xue Y, Sant V, Phillippi J, Sant S. Biodegradable and biomimetic elastomeric scaffolds for tissue-engineered heart valves. Acta Biomater. 2017 Jan 15;48:2-19. [DOI:10.1016/j.actbio.2016.10.032] [PMID]
22. Yang L-q, Lu L, Zhang C-w, Zhou C-r. Highly stretchable and self-healing hydrogels based on poly(acrylic acid) and functional POSS. Chinese Journal of Polymer Science. 2016;34(2):185-94. [DOI:10.1007/s10118-016-1744-1]
23. Shockey E, Bolf AG, Jones PF, Schwab J, Chaffee K, Haddad T, et al. Functionalized polyhedral oligosilsesquioxane (POSS) macromers: new graftable POSS hydride, POSS α-olefin, POSS epoxy, and POSS chlorosilane macromers and POSS-siloxane triblocks. Appl Organomet Chem. 1999;13:311-27.
https://doi.org/10.1002/(SICI)1099-0739(199904)13:4<311::AID-AOC847>3.0.CO;2-1 [DOI:10.1002/(SICI)1099-0739(199904)13:43.0.CO;2-1]
24. Pliska BT, Warner GA, Tantbirojn D, Larson BE. Treatment of white spot lesions with ACP paste and microabrasion. Angle Orthod. 2012 Sep;82(5):765-9. [DOI:10.2319/111611-710.1] [PMID] []
25. Ozgul BM, Orhan K, Oz FT. Micro-computed tomographic analysis of progression of artificial enamel lesions in primary and permanent teeth after resin infiltration. J Oral Sci. 2015 Sep;57(3):177-83. [DOI:10.2334/josnusd.57.177] [PMID]
26. Borges A, Caneppele T, Luz M, Pucci C, Torres C. Color stability of resin used for caries infiltration after exposure to different staining solutions. Oper Dent. 2014 Jul-Aug;39(4):433-40. [DOI:10.2341/13-150-L] [PMID]
27. Silva LO, Signori C, Peixoto AC, Cenci MS, Faria-E-Silva AL. Color restoration and stability in two treatments for white spot lesions. Int J Esthet Dent. 2018;13(3):394-403.
28. Mandava J, Reddy YS, Kantheti S, Chalasani U, Ravi RC, Borugadda R, Konagala RK. Microhardness and Penetration of Artificial White Spot Lesions Treated with Resin or Colloidal Silica Infiltration. J Clin Diagn Res. 2017 Apr;11(4):ZC142-ZC146. [DOI:10.7860/JCDR/2017/25512.9706] [PMID] []
29. Leland A, Akyalcin S, English JD, Tufekci E, Paravina R. Evaluation of staining and color changes of a resin infiltration system. Angle Orthod. 2016 Nov;86(6):900-4. [DOI:10.2319/111615-777.1] [PMID] []
30. Ertaş E, Güler AU, Yücel AC, Köprülü H, Güler E. Color stability of resin composites after immersion in different drinks. Dent Mater J. 2006 Jun;25(2):371-6. [DOI:10.4012/dmj.25.371] [PMID]
31. Mohamed AM, Wong KH, Lee WJ, Marizan Nor M, Mohd Hussaini H, Rosli TI. In vitro study of white spot lesion: Maxilla and mandibular teeth. Saudi Dent J. 2018 Apr;30(2):142-50. [DOI:10.1016/j.sdentj.2017.12.001] [PMID] []
32. Perdigão J. Resin infiltration of enamel white spot lesions: An ultramorphological analysis. J Esthet Restor Dent. 2020 Apr;32(3):317-24. [DOI:10.1111/jerd.12550] [PMID]
33. Kim S, Kim EY, Jeong TS, Kim JW. The evaluation of resin infiltration for masking labial enamel white spot lesions. Int J Paediatr Dent. 2011 Jul;21(4):241-8. [DOI:10.1111/j.1365-263X.2011.01126.x] [PMID]
34. Rocha Gomes Torres C, Borges AB, Torres LM, Gomes IS, de Oliveira RS. Effect of caries infiltration technique and fluoride therapy on the colour masking of white spot lesions. J Dent. 2011 Mar;39(3):202-7. [DOI:10.1016/j.jdent.2010.12.004] [PMID]
35. Shan D, He Y, Gao M, Liu H, Zhu Y, Liao L, Hadaegh F, Long H, Lai W. A comparison of resin infiltration and microabrasion for postorthodontic white spot lesion. Am J Orthod Dentofacial Orthop. 2021 Oct;160(4):516-522. [DOI:10.1016/j.ajodo.2020.04.039] [PMID]
36. Bourouni S, Dritsas K, Kloukos D, Wierichs RJ. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis - a systematic review and meta-analysis. Clin Oral Investig. 2021 Aug;25(8):4711-9. [DOI:10.1007/s00784-021-03931-7] [PMID] []
37. Abbas BA, Marzouk ES, Zaher AR. Treatment of various degrees of white spot lesions using resin infiltration-in vitro study. Prog Orthod. 2018 Aug 6;19(1):27. [DOI:10.1186/s40510-018-0223-3] [PMID] []
38. Simon LS, Dash JK, U D, Philip S, Sarangi S. Management of Post Orthodontic White Spot Lesions Using Resin Infiltration and CPP-ACP Materials- A Clinical Study. J Clin Pediatr Dent. 2022 Jan 1;46(1):70-74. [DOI:10.17796/1053-4625-46.1.12] [PMID]
39. Youssef A, Farid M, Zayed M, Lynch E, Alam MK, Kielbassa AM. Improving oral health: a short-term split-mouth randomized clinical trial revealing the superiority of resin infiltration over remineralization of white spot lesions. Quintessence Int. 2020;51(9):696-709.
40. Safaei M, Yeganeh H, Atai M. Effect of incorporation of MA-POSS on properties of thiol-ene systems for dental resins. 2014. Available from: https://sid.ir/paper/919329/en
41. MalekiGorji M, Banava S, Saghiri M. Enamel Erosion by 15% and 18% Hydrochloric Acid Gels after Different Application Times. J Res Dent Maxillofac Sci 2017;2(4):14-9. [DOI:10.29252/jrdms.2.4.14]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |