Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 3 (9-2024)
J Res Dent Maxillofac Sci 2024, 9(3): 184-192 |
Back to browse issues page


Ethics code: IR.GUMS.REC.1398.318
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kia S J, Basirat M, Soleimani R, Tadayon K, Najar-Karimi F. Association of Psychological Factors with Burning Mouth Syndrome in Psychiatric Diseases. J Res Dent Maxillofac Sci 2024; 9 (3) :184-192
URL: http://jrdms.dentaliau.ac.ir/article-1-568-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-568-en.html
Seyed Javad Kia1 

 , Maryam Basirat2 , Robabeh Soleimani3 , Kiana Tadayon4 , Fereshteh Najar-Karimi *5
, Maryam Basirat2 , Robabeh Soleimani3 , Kiana Tadayon4 , Fereshteh Najar-Karimi *5
, Maryam Basirat2 , Robabeh Soleimani3 , Kiana Tadayon4 , Fereshteh Najar-Karimi *5
1- Dental Sciences Research Center, Department of Oral and Maxillofacial Medicine, School of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
2- Dental Sciences Research Center, Medical Education Research Center, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- Department of Psychiatry, School of Medicine, Shafa Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Restorative Dentistry, School of Dentistry, Iran University of Medical Sciences, Tehran, Iran.
5- Assistant Professor, Dental Science Research Center, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Alborz University of Medical Sciences, Karaj, Iran. ,mastane_fk91@yahoo.com
2- Dental Sciences Research Center, Medical Education Research Center, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Guilan University of Medical Sciences, Rasht, Iran.
3- Department of Psychiatry, School of Medicine, Shafa Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Restorative Dentistry, School of Dentistry, Iran University of Medical Sciences, Tehran, Iran.
5- Assistant Professor, Dental Science Research Center, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Alborz University of Medical Sciences, Karaj, Iran. ,
Full-Text [PDF 371 kb]
(991 Downloads)
| Abstract (HTML) (2584 Views)
Full-Text: (860 Views)
Abstract
Background and Aim: Burning mouth syndrome (BMS) is characterized by pain sensation in the tongue and oral mucosa. It has no clinical or laboratory manifestations in early stages. The present study aimed to investigate the relationship of BMS with psychiatric diseases and the associated factors.
Materials and Methods: This descriptive-analytical study was conducted on 239 psychiatric patients referred to Shafa Hospital in Rasht, Iran. After recording the demographic information and medical history, mouth dryness and burning severity were assessed by the FOX questionnaire and a visual analogue scale (VAS), respectively. Data were analyzed by the Chi-square test, independent t-test, and Mann-Whitney test using SPSS version 22.
Results: According to the results, 13.8% of the participants (psychiatric patients) were suffering from BMS, and of all the investigated factors, wearing a denture was the only factor with a statistically significant association with BMS (P=0.044), such that a higher percentage of patients with dentures had BMS. Other factors had no significant relationship with BMS (P>0.05).
Conclusion: The results showed that BMS had a significant relationship with wearing a denture, which highlights the necessity of further attention to denture hygiene in BMS patients with psychiatric disorders. Moreover, psychiatric patients in this study showed a higher incidence of BMS. It appears that timely diagnosis and appropriate psychiatric treatment can be effective in better controlling the BMS.
Keywords: Burning Mouth Syndrome; Dentures; Mental disorders
Introduction
Burning mouth syndrome (BMS) is characterized by persistent pain or hypersensitivity in the tongue and other oral mucosa with a minimum duration of 4-6 months and no specific clinical or laboratory manifestations [1, 2]. Currently, there are no criteria for diagnosis of this multifactorial syndrome, which has an approximate prevalence of 0.7% to 7% [1, 3]. BMS often manifests as a bilateral burning sensation or numbness, with different intensities during the day, which can be accompanied by altered taste, some degrees of mouth dryness, or foreign body sensation in the mouth [1, 2]. The most commonly affected areas are the tongue, lips, hard palate, and floor of the mouth [1, 4].
BMS has two types of primary (idiopathic; no apparent local/systemic causes) and secondary (burning of the mouth due to detectable local, systemic, or psychological factors) [2]. Meanwhile, psychological factors such as depression and anxiety may be present in the majority of BMS patients [1]. BMS has been the topic of many investigations; however, little is known about the relationship of personal, social, and demographic characteristics with the triggering factors and symptoms of BMS [3]. On the other hand, it has been reported that the burning sensation can be aggravated by psychological problems [5]. Although psychological factors can play a role in the occurrence, persistence, and exacerbation of BMS, the relationship between these factors and BMS is not completely clear [3].
Therefore, the present study was conducted aiming to assess the relationship of BMS and psychiatric diseases and the associated factors.
Materials and Methods
This descriptive, analytical, cross-sectional study was conducted on 239 patients referred to Shafa Psychiatric Hospital in Rasht, Iran. The study was approved by the Ethics Committee of Guilan Faculty of Medical Sciences (Ethics code: IR.GUMS.REC.1398.318).
The inclusion criteria were willingness to participate in the study and a history of at least 6 months of neuropsychological diseases, and the exclusion criteria were inability to comprehend the questions (patients with severe neuropsychological disorders), using oral appliances, and presence of lesions or oral ulcers with pain and burning sensation such as lichen planus, lupus erythematosus, and geographic tongue. The sample size was calculated to be 175 patients (95% confidence interval; α=0.05) [2].
After informing the patients about the study and obtaining their written informed consent (from the volunteers or their legal guardians), their demographic information including age, gender and educational level, their medical history, general health status and habits, medications taken in the past 6 months, time of menopause, oral hygiene status, and history of chronic diseases (e.g., hypertension) and hormonal disorders were extracted from the patients' medical records [2]. The type of psychiatric disease was diagnosed by a specialist or determined according to the patients’ medical records. The sensation of dry mouth (xerostomia) was evaluated through interviews with patients using the Persian translation of the FOX questionnaire [6] with previously confirmed validity and reliability [7]. Patients who gave a positive answer to at least 3 questions were diagnosed with xerostomia.
BMS was diagnosed using a questionnaire and based on the presence of diffuse and usually bilateral burning sensation of the oral mucosa for at least 4-6 months. BMS was considered primary in absence of clinical/laboratory findings, and secondary in presence of such findings [8]. Moreover, a 10-score visual analog scale (VAS) was used to assess the pain severity in BMS (with 0 indicating no pain and 10 indicating severe pain) [9]. Next, the patients diagnosed with BMS were clinically examined by a trained senior dental student using a disposable dental mirror with the help of a flashlight for oral candidiasis and other oral conditions or lesions.
In the next step, based on presence or absence of BMS, the patients were divided into two groups: (I) patients with psychiatric disorders and BMS, and (II) patients with psychiatric disorders without BMS. Also, the frequency of BMS in patients with psychiatric disorders was examined. In patients with denture who were diagnosed with BMS, a clinical examination was performed using a disposable dental mirror and, if necessary, a flashlight to assess presence/absence of oral candidiasis.
Statistical Analysis
The Shapiro-Wilk or Kolmogorov-Smirnov test was used to assess the normality of data distribution. Accordingly, the data were analyzed using the Chi-square test, independent t-test, and Mann-Whitney test. Logistic regression was used to simultaneously examine the effects of independent variables in the two groups. All statistical analyses were conducted using SPSS version 22 at 0.05 level of significance (P ≤0.05).
Results
A total of 239 patients with psychiatric disorders [102 (42.7%) males and 137 (57.3%) females] in three age groups of <37 years (31.8%), 37-49 years (36.8%), and > 49 years (31.4 %) participated in this study; among whom, 206 (86.2%) did not have BMS and 33 (13.8%) had BMS. Also, 141 (59%) patients did not have xerostomia while 98 (41%) suffered from xerostomia. Furthermore, 72.2% of BMS patients had xerostomia.
In addition, 209 (87.4%), 126 (52.7%), 11 (4.6%), and 100 (41.8%) participants had anxiety, depression, bipolar disorder, and both anxiety and depression, respectively.
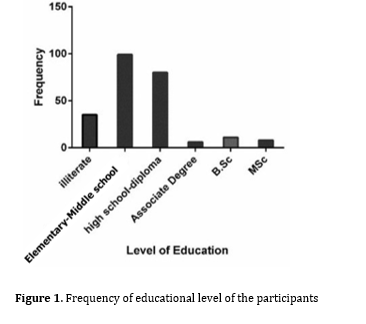
Figure 1 shows the frequency of educational level of the participants. The highest frequency was related to middle school/high-school educational level (41.4%) and high-school diploma (33.5%), respectively.
According to the findings, the most and the least affected areas in BMS were the tip of the tongue (84.8%) and hard palate (0.06%), respectively. Also, the mean pain score in patients with BMS was 5.36 ± 2.19 (range 1 to 10).
The results showed no statistically significant relationship between menopause and BMS (P>0.05).
As shown in Tables 1 and 2, in patients with psychiatric disorders, BMS and xerostomia had no significant association with gender, age group, anxiety, depression, bipolar disorder, diabetes mellitus, respiratory disorders, hepatic diseases, hypertension, seasonal allergies, hypothyroidism, hyperthyroidism, neurological diseases, anemia, hormonal problems, smoking, use of antihypertensives, frequency of toothbrushing, flossing, using a mouthwash, and gingival bleeding (P>0.05).
Figure 1. Frequency of educational level of the participants
Table 1. Relationship of different variables with BMS and xerostomia in patients with psychiatric disorders
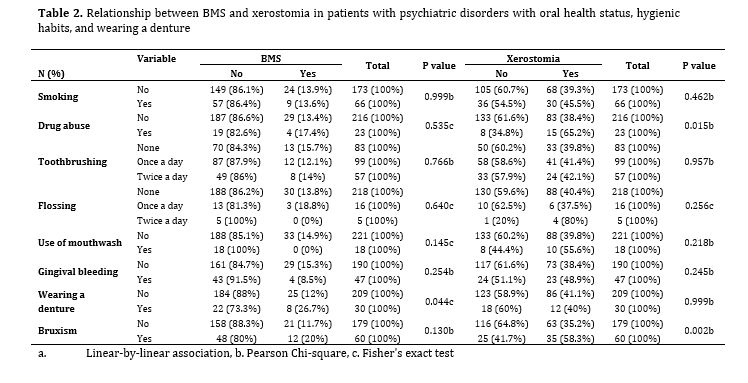
Table 2. Relationship between BMS and xerostomia in patients with psychiatric disorders with oral health status, hygienic habits, and wearing a denture
Among patients with psychiatric disorders, a significant positive relationship was observed between xerostomia and drug abuse (P=0.015), bruxism (P=0.002), gastrointestinal diseases (P=0.008), and educational level (P=0.010). Moreover, the incidence of xerostomia was higher in patients with elementary-middle school and high-school diploma educational levels compared to others. No statistically significant relationship was observed between BMS and any of the variables mentioned above (Tables 1 and 2).
Among the investigated variables, a statistically significant relationship was only found between wearing a denture and BMS (P=0.044) such that a higher percentage of patients who did not use dentures had BMS. However, no significant relationship was observed between xerostomia and denture use (P=0.999; Table 2).
Also, approximately 27% of denture wearers (9 out of 33 patients) had oral candidiasis.
Discussion
In the present study, the frequency of BMS in patients with psychiatric disorders was 13.8%, which was significantly higher than that in the normal population [2]. In addition, 41% of all participants and 72.2% of those with BMS had xerostomia, which is higher than the values reported in studies performed by Kia et al. and Ogle et al. [2, 10] but close to the value reported by Aditya et al [11]. Veerabhadrappa et al. [12] reported that the prevalence of xerostomia in patients with anxiety, depression, bipolar disorder, and controls was 51%, 47%, 41%, and 27%, respectively. Similarly, in the present study, the frequency of xerostomia was higher in patients with anxiety than other psychiatric disorders. Since the FOX questionnaire is more reliable than other questionnaires in assessing xerostomia [13], the diagnosis of this condition in the present study was made based on the FOX questionnaire. The difference in the results of studies may be due to differences in the eligibility criteria, and method of assessing xerostomia (by using a questionnaire or objectively through quantitative measurement of the saliva volume).
A VAS was used to assess the pain intensity in BMS in the present study because it is simple and easy to use [2, 14]. The mean VAS pain score was 5.36 ± 2.19, which was close to the results reported by most studies, including those conducted by Kia et al. and Takenoshita et al. [2, 14]. However, the possibility of reduction of BMS pain intensity by psychiatric medications has also been reported by patients [15]. Moreover, the most common site of involvement in BMS was the tip and lateral borders of the tongue, which was in line with most previous studies [1, 2, 10].
Although age and hormonal changes have been reported as factors with a potential role in the occurrence of BMS [2, 16], in the present study, no statistically significant relationship was observed between any of them with BMS or xerostomia. Similarly, Schiavone et al. [17] found no significant relationship between age and BMS. On the other hand, most previous studies reported that BMS was more prevalent among females than males [1-3]. In the present study, no statistically significant relationship was observed between gender and BMS, which was in line with the results of Schiavone et al, and Canfora et al [17, 18]. The difference in the results may be related to the different age and gender distribution of the study participants and high female to male ratio of the participants in some studies.
In the present study, a significant relationship was observed between xerostomia and educational level, while this relationship was not significant with BMS. Schiavone et al. and Canfora et al. [17, 18], also reported no significant relationship between educational level and BMS. In the current study, despite the high frequency of anxiety in BMS patients, no statistically significant relationship was observed between anxiety and BMS, which could be due to the heterogeneity of the number of participants in terms of the anxiety variable (209 patients with anxiety vs. 30 without it). On the other hand, although the frequency of depression in patients with BMS was higher than that in patients without BMS, no statistically significant relationship was observed between depression and BMS, which was consistent with the results of Takenoshita et al. [14]. However, Galli et al. [19] reported anxiety and depression as the most prevalent mental disorders in BMS. The reason for this difference may be the differences in the study populations, individual differences, presence of intervening factors, and the study methodology. One of the limitations of the present study was the high frequency of stress and anxiety in the study population, which could act as a confounding factor. Moreover, most of the studies on BMS have been performed on the population of patients with this syndrome, aiming at investigating the level of anxiety and depression, while in the present study, on the contrary, the frequency of BMS in the population of patients with psychological disorders was investigated, which was a strength of the present study.
In the current study, no significant relationship was observed between menopause and BMS. In contrast, Kia et al. [2] reported high incidence of BMS in postmenopausal women due to the reduction in estrogen and progesterone levels after the menopause. However, they did not report a statistically significant relationship between BMS and menopause [2]. The lower mean age of female participants and those not reaching menopause could be the reason for the difference in the results.
In the present study, there was no significant relationship between BMS and various systemic diseases such as diabetes mellitus, gastrointestinal disorders, hypertension, etc. However, a statistically significant relationship was observed between xerostomia and gastrointestinal diseases (P=0.008), which was in line with the results of Kia et al. [2]. Better control of diabetes mellitus in the recent years can be one reason for insignificance of this relationship. According to the classification by Lamb et al. [20], 31 out of 33 patients with BMS in the present study had type 3 BMS (patients who also experience pain-free periods). It has been reported that this type of BMS has the least relationship with various systemic diseases, including diabetes mellitus [20]. Due to the absence of previous studies on the relationship between the afore-mentioned diseases and BMS, it is not possible to accurately compare the results of previous studies with the present study. On the other hand, regional, climatic, and cultural differences can affect the possible association of BMS with various systemic diseases by creating different risk factors.
Contrary to the present study, as well as the study by Soares et al. [21] in which no significant relationship was observed between the use of antihypertensives and BMS, Azzi et al. [22] found BMS to be associated with the use of antihypertensives. Considering that among the antihypertensives, most angiotensin-converting enzyme inhibitors are known to be associated with BMS [23], the diversity in antihypertensive categories can be one of the reasons for the contradictory results of the studies mentioned above.
In the present study, no significant relationship was observed between BMS with seasonal allergies, smoking, and drug abuse; however, the relationship between drug abuse and xerostomia was significant (p=0.015). Kia et al. [2] reported an insignificant relationship between allergy and BMS. In line with the current study, Kohorst et al. [24] reported no significant relationship between smoking and BMS, which was inconsistent with the results of Gao et al. [25]. According to a report, vitamin B12 and folic acid deficiency in the serum and oral mucosal cells of smokers who smoke ≥ 20 cigarettes per day may cause BMS in the long-term [26]. Therefore, differences in the number of cigarettes smoked and duration of smoking can affect the results.
The present results revealed no significant relationship between the level of oral hygiene (frequency of daily toothbrushing, flossing, and mouthwash use) and gingival bleeding with BMS, which was consistent with the results of Kia et al. [2]. On the other hand, there was a significant relationship between wearing a denture and BMS. In a study by Colak et al. [27], 50% of patients with BMS had dentures. In contrast, Kia et al. [2] did not report a significant relationship between wearing a denture and BMS. The reason for this difference can be less attention to oral hygiene in patients with psychiatric disorders and resultantly higher rate of tooth loss and denture use. On the other hand, in the present study, after examining the patients with dentures for presence of candidiasis, approximately 27% of those with BMS (9 out of 33 patients) had oral candidiasis, which can be one of the causes of BMS in denture wearers.
In the current study, no significant relationship was observed between bruxism and BMS, while its relationship with xerostomia was significant. There is no consensus about the role of parafunctional habits in the etiology of BMS [28, 29]. Controlling the parafunctional habits has been reported as an influential factor in resolution of burning sensation in BMS patients [30]. Therefore, considering the possible role of psychiatric medications in inducing sedative effects and subsequently reducing the parafunctional habits in patients with psychiatric disorders, it seems that medications might have acted as a confounding factor in determining the actual relationship between bruxism and BMS in the present study.
Unlike most previous studies that determined the prevalence of various factors including anxiety in patients with BMS, in the present study, the prevalence of BMS and its relationship with psychological factors were determined in psychiatric patients with a larger sample size for a more detailed investigation of this relationship, which can be considered as a strength. The lower mean age of female participants and lack of BMS examination in patients recently diagnosed with mental disorders who had not yet started any medical treatment were the limitations of the present study. Future studies are suggested to be conducted in larger communities with a larger sample size and with the investigation of hyposalivation (by measuring the salivary flow rate) along with xerostomia.
Conclusion
The results showed that BMS had a significant relationship with wearing a denture, which may highlight the necessity of further attention to hygiene of dentures in BMS patients with psychiatric disorders. Moreover, psychiatric patients in this study showed higher incidence of BMS. Thus, it appears that timely diagnosis and appropriate psychiatric treatment can be effective in better controlling the BMS.
Conflict of Interest Statement
The authors declare no conflict of interests.
Acknowledgement
The authors would like to thank Dr. Mohammad Ebrahim Ghaffari Assistant Professor of Biostatistics, Qom University of Medical Sciences for performing the statistical analysis.
Background and Aim: Burning mouth syndrome (BMS) is characterized by pain sensation in the tongue and oral mucosa. It has no clinical or laboratory manifestations in early stages. The present study aimed to investigate the relationship of BMS with psychiatric diseases and the associated factors.
Materials and Methods: This descriptive-analytical study was conducted on 239 psychiatric patients referred to Shafa Hospital in Rasht, Iran. After recording the demographic information and medical history, mouth dryness and burning severity were assessed by the FOX questionnaire and a visual analogue scale (VAS), respectively. Data were analyzed by the Chi-square test, independent t-test, and Mann-Whitney test using SPSS version 22.
Results: According to the results, 13.8% of the participants (psychiatric patients) were suffering from BMS, and of all the investigated factors, wearing a denture was the only factor with a statistically significant association with BMS (P=0.044), such that a higher percentage of patients with dentures had BMS. Other factors had no significant relationship with BMS (P>0.05).
Conclusion: The results showed that BMS had a significant relationship with wearing a denture, which highlights the necessity of further attention to denture hygiene in BMS patients with psychiatric disorders. Moreover, psychiatric patients in this study showed a higher incidence of BMS. It appears that timely diagnosis and appropriate psychiatric treatment can be effective in better controlling the BMS.
Keywords: Burning Mouth Syndrome; Dentures; Mental disorders
Introduction
Burning mouth syndrome (BMS) is characterized by persistent pain or hypersensitivity in the tongue and other oral mucosa with a minimum duration of 4-6 months and no specific clinical or laboratory manifestations [1, 2]. Currently, there are no criteria for diagnosis of this multifactorial syndrome, which has an approximate prevalence of 0.7% to 7% [1, 3]. BMS often manifests as a bilateral burning sensation or numbness, with different intensities during the day, which can be accompanied by altered taste, some degrees of mouth dryness, or foreign body sensation in the mouth [1, 2]. The most commonly affected areas are the tongue, lips, hard palate, and floor of the mouth [1, 4].
BMS has two types of primary (idiopathic; no apparent local/systemic causes) and secondary (burning of the mouth due to detectable local, systemic, or psychological factors) [2]. Meanwhile, psychological factors such as depression and anxiety may be present in the majority of BMS patients [1]. BMS has been the topic of many investigations; however, little is known about the relationship of personal, social, and demographic characteristics with the triggering factors and symptoms of BMS [3]. On the other hand, it has been reported that the burning sensation can be aggravated by psychological problems [5]. Although psychological factors can play a role in the occurrence, persistence, and exacerbation of BMS, the relationship between these factors and BMS is not completely clear [3].
Therefore, the present study was conducted aiming to assess the relationship of BMS and psychiatric diseases and the associated factors.
Materials and Methods
This descriptive, analytical, cross-sectional study was conducted on 239 patients referred to Shafa Psychiatric Hospital in Rasht, Iran. The study was approved by the Ethics Committee of Guilan Faculty of Medical Sciences (Ethics code: IR.GUMS.REC.1398.318).
The inclusion criteria were willingness to participate in the study and a history of at least 6 months of neuropsychological diseases, and the exclusion criteria were inability to comprehend the questions (patients with severe neuropsychological disorders), using oral appliances, and presence of lesions or oral ulcers with pain and burning sensation such as lichen planus, lupus erythematosus, and geographic tongue. The sample size was calculated to be 175 patients (95% confidence interval; α=0.05) [2].
After informing the patients about the study and obtaining their written informed consent (from the volunteers or their legal guardians), their demographic information including age, gender and educational level, their medical history, general health status and habits, medications taken in the past 6 months, time of menopause, oral hygiene status, and history of chronic diseases (e.g., hypertension) and hormonal disorders were extracted from the patients' medical records [2]. The type of psychiatric disease was diagnosed by a specialist or determined according to the patients’ medical records. The sensation of dry mouth (xerostomia) was evaluated through interviews with patients using the Persian translation of the FOX questionnaire [6] with previously confirmed validity and reliability [7]. Patients who gave a positive answer to at least 3 questions were diagnosed with xerostomia.
BMS was diagnosed using a questionnaire and based on the presence of diffuse and usually bilateral burning sensation of the oral mucosa for at least 4-6 months. BMS was considered primary in absence of clinical/laboratory findings, and secondary in presence of such findings [8]. Moreover, a 10-score visual analog scale (VAS) was used to assess the pain severity in BMS (with 0 indicating no pain and 10 indicating severe pain) [9]. Next, the patients diagnosed with BMS were clinically examined by a trained senior dental student using a disposable dental mirror with the help of a flashlight for oral candidiasis and other oral conditions or lesions.
In the next step, based on presence or absence of BMS, the patients were divided into two groups: (I) patients with psychiatric disorders and BMS, and (II) patients with psychiatric disorders without BMS. Also, the frequency of BMS in patients with psychiatric disorders was examined. In patients with denture who were diagnosed with BMS, a clinical examination was performed using a disposable dental mirror and, if necessary, a flashlight to assess presence/absence of oral candidiasis.
Statistical Analysis
The Shapiro-Wilk or Kolmogorov-Smirnov test was used to assess the normality of data distribution. Accordingly, the data were analyzed using the Chi-square test, independent t-test, and Mann-Whitney test. Logistic regression was used to simultaneously examine the effects of independent variables in the two groups. All statistical analyses were conducted using SPSS version 22 at 0.05 level of significance (P ≤0.05).
Results
A total of 239 patients with psychiatric disorders [102 (42.7%) males and 137 (57.3%) females] in three age groups of <37 years (31.8%), 37-49 years (36.8%), and > 49 years (31.4 %) participated in this study; among whom, 206 (86.2%) did not have BMS and 33 (13.8%) had BMS. Also, 141 (59%) patients did not have xerostomia while 98 (41%) suffered from xerostomia. Furthermore, 72.2% of BMS patients had xerostomia.
In addition, 209 (87.4%), 126 (52.7%), 11 (4.6%), and 100 (41.8%) participants had anxiety, depression, bipolar disorder, and both anxiety and depression, respectively.
Figure 1 shows the frequency of educational level of the participants. The highest frequency was related to middle school/high-school educational level (41.4%) and high-school diploma (33.5%), respectively.
According to the findings, the most and the least affected areas in BMS were the tip of the tongue (84.8%) and hard palate (0.06%), respectively. Also, the mean pain score in patients with BMS was 5.36 ± 2.19 (range 1 to 10).
The results showed no statistically significant relationship between menopause and BMS (P>0.05).
As shown in Tables 1 and 2, in patients with psychiatric disorders, BMS and xerostomia had no significant association with gender, age group, anxiety, depression, bipolar disorder, diabetes mellitus, respiratory disorders, hepatic diseases, hypertension, seasonal allergies, hypothyroidism, hyperthyroidism, neurological diseases, anemia, hormonal problems, smoking, use of antihypertensives, frequency of toothbrushing, flossing, using a mouthwash, and gingival bleeding (P>0.05).
Figure 1. Frequency of educational level of the participants
{kind=link}
Table 1. Relationship of different variables with BMS and xerostomia in patients with psychiatric disorders
Table 2. Relationship between BMS and xerostomia in patients with psychiatric disorders with oral health status, hygienic habits, and wearing a denture
{kind=link}
Among patients with psychiatric disorders, a significant positive relationship was observed between xerostomia and drug abuse (P=0.015), bruxism (P=0.002), gastrointestinal diseases (P=0.008), and educational level (P=0.010). Moreover, the incidence of xerostomia was higher in patients with elementary-middle school and high-school diploma educational levels compared to others. No statistically significant relationship was observed between BMS and any of the variables mentioned above (Tables 1 and 2).
Among the investigated variables, a statistically significant relationship was only found between wearing a denture and BMS (P=0.044) such that a higher percentage of patients who did not use dentures had BMS. However, no significant relationship was observed between xerostomia and denture use (P=0.999; Table 2).
Also, approximately 27% of denture wearers (9 out of 33 patients) had oral candidiasis.
Discussion
In the present study, the frequency of BMS in patients with psychiatric disorders was 13.8%, which was significantly higher than that in the normal population [2]. In addition, 41% of all participants and 72.2% of those with BMS had xerostomia, which is higher than the values reported in studies performed by Kia et al. and Ogle et al. [2, 10] but close to the value reported by Aditya et al [11]. Veerabhadrappa et al. [12] reported that the prevalence of xerostomia in patients with anxiety, depression, bipolar disorder, and controls was 51%, 47%, 41%, and 27%, respectively. Similarly, in the present study, the frequency of xerostomia was higher in patients with anxiety than other psychiatric disorders. Since the FOX questionnaire is more reliable than other questionnaires in assessing xerostomia [13], the diagnosis of this condition in the present study was made based on the FOX questionnaire. The difference in the results of studies may be due to differences in the eligibility criteria, and method of assessing xerostomia (by using a questionnaire or objectively through quantitative measurement of the saliva volume).
A VAS was used to assess the pain intensity in BMS in the present study because it is simple and easy to use [2, 14]. The mean VAS pain score was 5.36 ± 2.19, which was close to the results reported by most studies, including those conducted by Kia et al. and Takenoshita et al. [2, 14]. However, the possibility of reduction of BMS pain intensity by psychiatric medications has also been reported by patients [15]. Moreover, the most common site of involvement in BMS was the tip and lateral borders of the tongue, which was in line with most previous studies [1, 2, 10].
Although age and hormonal changes have been reported as factors with a potential role in the occurrence of BMS [2, 16], in the present study, no statistically significant relationship was observed between any of them with BMS or xerostomia. Similarly, Schiavone et al. [17] found no significant relationship between age and BMS. On the other hand, most previous studies reported that BMS was more prevalent among females than males [1-3]. In the present study, no statistically significant relationship was observed between gender and BMS, which was in line with the results of Schiavone et al, and Canfora et al [17, 18]. The difference in the results may be related to the different age and gender distribution of the study participants and high female to male ratio of the participants in some studies.
In the present study, a significant relationship was observed between xerostomia and educational level, while this relationship was not significant with BMS. Schiavone et al. and Canfora et al. [17, 18], also reported no significant relationship between educational level and BMS. In the current study, despite the high frequency of anxiety in BMS patients, no statistically significant relationship was observed between anxiety and BMS, which could be due to the heterogeneity of the number of participants in terms of the anxiety variable (209 patients with anxiety vs. 30 without it). On the other hand, although the frequency of depression in patients with BMS was higher than that in patients without BMS, no statistically significant relationship was observed between depression and BMS, which was consistent with the results of Takenoshita et al. [14]. However, Galli et al. [19] reported anxiety and depression as the most prevalent mental disorders in BMS. The reason for this difference may be the differences in the study populations, individual differences, presence of intervening factors, and the study methodology. One of the limitations of the present study was the high frequency of stress and anxiety in the study population, which could act as a confounding factor. Moreover, most of the studies on BMS have been performed on the population of patients with this syndrome, aiming at investigating the level of anxiety and depression, while in the present study, on the contrary, the frequency of BMS in the population of patients with psychological disorders was investigated, which was a strength of the present study.
In the current study, no significant relationship was observed between menopause and BMS. In contrast, Kia et al. [2] reported high incidence of BMS in postmenopausal women due to the reduction in estrogen and progesterone levels after the menopause. However, they did not report a statistically significant relationship between BMS and menopause [2]. The lower mean age of female participants and those not reaching menopause could be the reason for the difference in the results.
In the present study, there was no significant relationship between BMS and various systemic diseases such as diabetes mellitus, gastrointestinal disorders, hypertension, etc. However, a statistically significant relationship was observed between xerostomia and gastrointestinal diseases (P=0.008), which was in line with the results of Kia et al. [2]. Better control of diabetes mellitus in the recent years can be one reason for insignificance of this relationship. According to the classification by Lamb et al. [20], 31 out of 33 patients with BMS in the present study had type 3 BMS (patients who also experience pain-free periods). It has been reported that this type of BMS has the least relationship with various systemic diseases, including diabetes mellitus [20]. Due to the absence of previous studies on the relationship between the afore-mentioned diseases and BMS, it is not possible to accurately compare the results of previous studies with the present study. On the other hand, regional, climatic, and cultural differences can affect the possible association of BMS with various systemic diseases by creating different risk factors.
Contrary to the present study, as well as the study by Soares et al. [21] in which no significant relationship was observed between the use of antihypertensives and BMS, Azzi et al. [22] found BMS to be associated with the use of antihypertensives. Considering that among the antihypertensives, most angiotensin-converting enzyme inhibitors are known to be associated with BMS [23], the diversity in antihypertensive categories can be one of the reasons for the contradictory results of the studies mentioned above.
In the present study, no significant relationship was observed between BMS with seasonal allergies, smoking, and drug abuse; however, the relationship between drug abuse and xerostomia was significant (p=0.015). Kia et al. [2] reported an insignificant relationship between allergy and BMS. In line with the current study, Kohorst et al. [24] reported no significant relationship between smoking and BMS, which was inconsistent with the results of Gao et al. [25]. According to a report, vitamin B12 and folic acid deficiency in the serum and oral mucosal cells of smokers who smoke ≥ 20 cigarettes per day may cause BMS in the long-term [26]. Therefore, differences in the number of cigarettes smoked and duration of smoking can affect the results.
The present results revealed no significant relationship between the level of oral hygiene (frequency of daily toothbrushing, flossing, and mouthwash use) and gingival bleeding with BMS, which was consistent with the results of Kia et al. [2]. On the other hand, there was a significant relationship between wearing a denture and BMS. In a study by Colak et al. [27], 50% of patients with BMS had dentures. In contrast, Kia et al. [2] did not report a significant relationship between wearing a denture and BMS. The reason for this difference can be less attention to oral hygiene in patients with psychiatric disorders and resultantly higher rate of tooth loss and denture use. On the other hand, in the present study, after examining the patients with dentures for presence of candidiasis, approximately 27% of those with BMS (9 out of 33 patients) had oral candidiasis, which can be one of the causes of BMS in denture wearers.
In the current study, no significant relationship was observed between bruxism and BMS, while its relationship with xerostomia was significant. There is no consensus about the role of parafunctional habits in the etiology of BMS [28, 29]. Controlling the parafunctional habits has been reported as an influential factor in resolution of burning sensation in BMS patients [30]. Therefore, considering the possible role of psychiatric medications in inducing sedative effects and subsequently reducing the parafunctional habits in patients with psychiatric disorders, it seems that medications might have acted as a confounding factor in determining the actual relationship between bruxism and BMS in the present study.
Unlike most previous studies that determined the prevalence of various factors including anxiety in patients with BMS, in the present study, the prevalence of BMS and its relationship with psychological factors were determined in psychiatric patients with a larger sample size for a more detailed investigation of this relationship, which can be considered as a strength. The lower mean age of female participants and lack of BMS examination in patients recently diagnosed with mental disorders who had not yet started any medical treatment were the limitations of the present study. Future studies are suggested to be conducted in larger communities with a larger sample size and with the investigation of hyposalivation (by measuring the salivary flow rate) along with xerostomia.
Conclusion
The results showed that BMS had a significant relationship with wearing a denture, which may highlight the necessity of further attention to hygiene of dentures in BMS patients with psychiatric disorders. Moreover, psychiatric patients in this study showed higher incidence of BMS. Thus, it appears that timely diagnosis and appropriate psychiatric treatment can be effective in better controlling the BMS.
Conflict of Interest Statement
The authors declare no conflict of interests.
Acknowledgement
The authors would like to thank Dr. Mohammad Ebrahim Ghaffari Assistant Professor of Biostatistics, Qom University of Medical Sciences for performing the statistical analysis.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Alsabbagh R, Ouanounou A. Burning Mouth Syndrome: Etiology, clinical presentations, and treatment alternatives. Dent Rev. 2022;2(1):10003-6. [DOI:10.1016/j.dentre.2022.100036]
2. Kia S, Saberi B, Basirat M, Rajabpour K, Vahedi M. Burning Mouth Syndrome and Its Related Risk Factors in Females. Avicenna J Dent Res. 2017;9(4):e12412. [DOI:10.5812/ajdr.12412]
3. Adamo D, Celentano A, Ruoppo E, Cucciniello C, Pecoraro G, Aria M, Mignogna MD. The Relationship Between Sociodemographic Characteristics and Clinical Features in Burning Mouth Syndrome. Pain Med. 2015 Nov;16(11):2171-9. [DOI:10.1111/pme.12808] [PMID]
4. Aggarwal A, Panat SR. Burning mouth syndrome: A diagnostic and therapeutic dilemma. J Clin Exp Dent. 2012 Jul;4(3):e180-5. [DOI:10.4317/jced.50764] [PMID] []
5. Kisely S, Forbes M, Sawyer E, Black E, Lalloo R. A systematic review of randomized trials for the treatment of burning mouth syndrome. J Psychosom Res. 2016 Jul;86:39-46. [DOI:10.1016/j.jpsychores.2016.05.001] [PMID]
6. Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987 Oct;115(4):581-4. [DOI:10.1016/S0002-8177(87)54012-0] [PMID]
7. Rad M, Chamani G, Shahravan A, Hedayati N, Alizadeh F. Survey of prevalence of xerostomia in a population of Kerman, Iran, attending medical and dental clinics. Oral Health Oral Epidemiol. 2013;2(1):28-34.
8. Thakkar JP, Lane CJ. Hyposalivation and Xerostomia and Burning Mouth Syndrome: Medical Management. Oral Maxillofac Surg Clin North Am. 2022 Feb;34(1):135-46. [DOI:10.1016/j.coms.2021.08.002] [PMID]
9. Gao Y, Yang J, Sun H, Zhou H. Efficacy of Danzhixiaoyao pills in the treatment of burning mouth syndrome:An randomized controlled trial. 2023; P. 1-20. [DOI:10.21203/rs.3.rs-3525236/v1]
10. Ogle OE, Dym H, Leslie. H. Burning Mouth Syndrome. Oral and Maxillofacial Surgery, Medicine, and Pathology for the Clinician. 1st ed: Wiley-Blackwell; 2023. p. 301-9. [DOI:10.1002/9781119362579.ch25]
11. Aditya A, Lele S. Prevalence of Xerostomia and Burning Sensation in Patients with Psychosocial Disorders. Journal of International Dental and Medical Research. 2011;4(3):111-6.
12. Veerabhadrappa SK, Chandrappa PR, Patil S, Roodmal SY, Kumarswamy A, Chappi MK. Evaluation of Xerostomia in Different Psychological Disorders: An Observational Study. J Clin Diagn Res. 2016 Sep;10(9):ZC24-ZC27. [DOI:10.7860/JCDR/2016/19020.8437] [PMID] []
13. Indre MG, Sampelean D, Taru V, Cozma A, Sampelean D, Milaciu M, et al. Non-dental oral cavity findings in gastroesophageal reflux disease: a systematic review and meta-analysis. J Mind Med Sci. 2021; 8(1): 60-70. [DOI:10.22543/7674.81.P6070]
14. Takenoshita M, Sato T, Kato Y, Katagiri A, Yoshikawa T, Sato Y, Matsushima E, Sasaki Y, Toyofuku A. Psychiatric diagnoses in patients with burning mouth syndrome and atypical odontalgia referred from psychiatric to dental facilities. Neuropsychiatr Dis Treat. 2010 Oct 13;6:699-705. [DOI:10.2147/NDT.S12605] [PMID] []
15. Feller L, Fourie J, Bouckaert M, Khammissa RAG, Ballyram R, Lemmer J. Burning Mouth Syndrome: Aetiopathogenesis and Principles of Management. Pain Res Manag. 2017;2017:1926269. [DOI:10.1155/2017/1926269] [PMID] []
16. Ślebioda Z, Szponar E. Burning mouth syndrome - a common dental problem in perimenopausal women. Prz Menopauzalny. 2014 Jun;13(3):198-202. [DOI:10.5114/pm.2014.43825] [PMID] []
17. Schiavone V, Adamo D, Ventrella G, Morlino M, De Notaris EB, Ravel MG, Kusmann F, Piantadosi M, Pollio A, Fortuna G, Mignogna MD. Anxiety, depression, and pain in burning mouth syndrome: first chicken or egg? Headache. 2012 Jun;52(6):1019-25. [DOI:10.1111/j.1526-4610.2012.02171.x] [PMID]
18. Canfora F, Calabria E, Pecoraro G, D Aniello L, Aria M, Marenzi G, et al. The use of self-report questionnaires in an analysis of the multidimensional aspects of pain and a correlation with the psychological profile and quality of life in patients with burning mouth syndrome: A case-control study. J Oral Rehabil. 2022 Sep;49(9):890-914. [DOI:10.1111/joor.13343] [PMID] []
19. Galli F, Lodi G, Sardella A, Vegni E. Role of psychological factors in burning mouth syndrome: A systematic review and meta-analysis. Cephalalgia. 2017 Mar;37(3):265-77. [DOI:10.1177/0333102416646769] [PMID]
20. Lamb AB, Lamey PJ, Reeve PE. Burning mouth syndrome: psychological aspects. Br Dent J. 1988 Oct 8;165(7):256-60. [DOI:10.1038/sj.bdj.4806586] [PMID]
21. Soares MS, Chimenos-Küstner E, Subirá-Pifarrè C, Rodríguez de Rivera-Campillo ME, López-López J. Association of burning mouth syndrome with xerostomia and medicines. Med Oral Patol Oral Cir Bucal. 2005 Aug-Oct;10(4):301-8.
22. Azzi L, Veronesi G, Tagliabue A, Croveri F, Maurino V, Reguzzoni M, Tettamanti L, Protasoni M, Spadari F. Is there an association between drugs and burning mouth syndrome? A case-control study. Oral Dis. 2019 Sep;25(6):1634-44. [DOI:10.1111/odi.13116] [PMID]
23. Sridhar N, Tosur Z. Lisinopril-induced burning mouth syndrome. AIM Clinical Cases. 2023;2:e221103. [DOI:10.7326/aimcc.2022.1103]
24. Kohorst JJ, Bruce AJ, Torgerson RR, Schenck LA, Davis MD. A population-based study of the incidence of burning mouth syndrome. Mayo Clin Proc. 2014 Nov;89(11):1545-52. [DOI:10.1016/j.mayocp.2014.05.018] [PMID] []
25. Gao J, Chen L, Zhou J, Peng J. A case-control study on etiological factors involved in patients with burning mouth syndrome. J Oral Pathol Med. 2009 Jan;38(1):24-8. [DOI:10.1111/j.1600-0714.2008.00708.x] [PMID]
26. Wu YH, Wu YC, Chang JY, Lang MJ, Chiang CP, Sun A. Anemia, hematinic deficiencies, and hyperhomocysteinemia in younger and older burning mouth syndrome patients. J Dent Sci. 2022 Jul;17(3):1144-50. [DOI:10.1016/j.jds.2022.02.005] [PMID] []
27. Colak H, Bayraktar Y, Hamidi M, Uzgur R, Toptanci İ, Dallı M. Prevalence of burning mouth syndrome in adult Turkish population. Dicle Medical Journal. 2011;38(3):289-93. [DOI:10.5798/diclemedj.0921.2011.03.0033]
28. Hakeberg M, Berggren U, Hägglin C, Ahlqwist M. Reported burning mouth symptoms among middle-aged and elderly women. Eur J Oral Sci. 1997 Dec;105(6):539-43. [DOI:10.1111/j.1600-0722.1997.tb00214.x] [PMID]
29. Sruthi K, Yashoda RH, Puranik M. Association between oral health status and salivary flow rate among individuals with and without burning mouth: a case control study. Journal of Indian Association of Public Health Dentistry. 2020;18(1):47-53. [DOI:10.4103/jiaphd.jiaphd_135_19]
30. Kwon DK, Park HK. Effect of Botulinum Toxin Injection and Physical Therapy to Reduce Tongue Pain and Discomfort: Case Reports. J Oral Med Pain 2020;45:120-3. [DOI:10.14476/jomp.2020.45.4.120]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |