Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 4 (12-2024)
J Res Dent Maxillofac Sci 2024, 9(4): 243-249 |
Back to browse issues page


Ethics code: IR.IAU.DENTAL.REC.1399.040
Clinical trials code: IRCT20200517047478N1
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
TourSavadkouhi S, Mousavi S A, Asnaashari E, Ahmadi M, Khajehmougahi K. Comparative Effects of Root Canal Irrigation with Sodium Hypochlorite and Super-oxidized Water on Post-Endodontic Pain in Single-Canal Teeth: A Clinical Trial. J Res Dent Maxillofac Sci 2024; 9 (4) :243-249
URL: http://jrdms.dentaliau.ac.ir/article-1-566-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-566-en.html
Sohrab TourSavadkouhi1 
 , Seyed Amirmasoud Mousavi2 , Ehsan Asnaashari3 , Mohammadsadegh Ahmadi4 , Koosha Khajehmougahi *5
, Seyed Amirmasoud Mousavi2 , Ehsan Asnaashari3 , Mohammadsadegh Ahmadi4 , Koosha Khajehmougahi *5 
, Seyed Amirmasoud Mousavi2 , Ehsan Asnaashari3 , Mohammadsadegh Ahmadi4 , Koosha Khajehmougahi *5
1- Dental Material Research Center, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran.
3- Endodontic Department, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
4- Dentist, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
5- Dentist, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran ,khajehmougahikousha@gmail.com
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran.
3- Endodontic Department, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
4- Dentist, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran
5- Dentist, Dental School, Islamic Azad University of Medical Sciences, Tehran, Iran ,
Full-Text [PDF 413 kb]
(1119 Downloads)
| Abstract (HTML) (2923 Views)
Full-Text: (1434 Views)
Abstract
Background and Aim: This study aimed to compare the effects of root canal irrigation with sodium hypochlorite (NaOCl) and super-oxidized water on post-endodontic pain in single-canal teeth.
Materials and Methods: This double-blind randomized clinical trial was conducted on 72 patients with irreversible pulpitis of single-canal teeth. The patients were randomly assigned to two groups (n=36) for root canal irrigation with either 1% NaOCl or 50% super-oxidized water during endodontic treatment. The root canals were instrumented by the step-back technique with a minimum and maximum apical preparation size of 30 and 50, respectively, and flaring by 5 files larger than the master apical file. Patients' pain level was quantified at 6, 12, 24, 48, and 72 hours, and 7 days postoperatively using a visual analog scale (VAS). Root canal treatments were accomplished in two sessions, and calcium hydroxide was applied as intracanal medicament. Data were analyzed by the Mann-Whitney test (alpha=0.05).
Results: At 12 hours postoperatively, the pain score was significantly higher in the NaOCl group than the super-oxidized water group (P=0.043). The pain score gradually decreased in both groups after 12 hours with no pain recorded at 7 days. The difference in pain score between the two groups was not significant at any other time point (P>0.05).
Conclusion: The present results revealed significantly lower level of pain at 12 hours post-treatment of single-canal teeth in root canal irrigation with super-oxidized water.
Keywords: Root Canal Irrigants; Root Canal Therapy; Sodium Hypochlorite; Superoxidized Water; Pain
Introduction
Post-endodontic pain remains a dilemma in dentistry and is responsible for increased anxiety level of patients and their poor cooperation in subsequent visits. Post-endodontic pain management is often challenging for dental clinicians [1]. Post-endodontic pain often leads to overconsumption of analgesics by patients. Although preoperative (prophylactic) and postoperative analgesic intake can significantly decrease post-endodontic pain, it cannot completely prevent it [2]. Post-endodontic pain has a high prevalence and is also experienced by 15%-25% of asymptomatic patients who do not have any pain before the procedure [3]. It has been demonstrated that type of root canal irrigant can affect post-endodontic pain. Thus, selection of an irrigant with minimal cytotoxicity, optimal antibacterial activity, and acceptable tissue dissolving property (for elimination of residual vital and necrotic tissues) is highly important [4].
Several irrigants are currently available for root canal irrigation, such as 5.25% sodium hypochlorite (NaOCl) and 2% chlorhexidine (CHX). NaOCl easily dissolves the residual pulp tissue and collagen fibers and is the only root canal irrigant capable of dissolving the viable and necrotic tissues [5]. It can also completely eliminate Enterococcus faecalis [6]. However, NaOCl has drawbacks such as cytotoxicity for the periapical tissues, the possibility of triggering an allergic reaction, bad odor, and the risk of hypochlorite accident [7]. CHX has some drawbacks as well. It cannot dissolve the residual tissues and can cause tooth discoloration [8]. Nonetheless, CHX has a broader spectrum of antibacterial activity than NaOCl [9].
Super-oxidized water is another irrigant which has gained recent popularity. It can effectively eliminate the intracanal bacteria, and has insignificant cytotoxicity for the periapical tissue [10]. It is a buffer with a neutral pH and 800 ppm effective substance and 50% concentration. Its effective substance reaches a concentration of 350-400 ppm after dilution. It is a shared product of Russia and Japan (Envirolyte, Tokyo, Japan).
To the best of the authors’ knowledge, the effect of root canal irrigation with super-oxidized water on post-endodontic pain has not been previously investigated. Thus, this study aimed to compare the effects of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single-canal teeth. The null hypothesis of the study was that no significant difference would be found in post-endodontic pain between NaOCl and super-oxidized water groups.
Materials and Methods
This study was conducted at the Faculty of Dentistry, Tehran Medical Science, Islamic Azad University between 2019 and 2020. The study protocol was approved by the ethics committee of the university (IR.IAU.DENTAL.REC.1399.040) and registered in the Iranian Registry of Clinical Trials (IRCT20200517047478N1).
Trial design:
A randomized double-blind clinical trial was designed in which one group received root canal irrigation with NaOCl and the other group received root canal irrigation with super-oxidized water during endodontic treatment of single-canal teeth. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were age range of 18 to 65 years, no pregnancy, no systemic diseases (ASA Class I and II), no history of allergy or toxic reaction to anesthetic agents, no intake of sedative, anxiolytic, or analgesic medications within 6 hours prior to treatment, having asymptomatic irreversible pulpitis of at least one single-canal tooth, no severe periodontal disease, and signing informed consent forms. The respective tooth had to be vital, with no sensitivity to percussion, and moderate to severe pain response to sensibility tests with no periapical lesion or periodontal ligament widening on radiographs.
The sample consisted of 72 patients presenting to the Endodontics Department of the Faculty of Dentistry, Tehran Medical Science, Islamic Azad University with single-rooted teeth requiring endodontic treatment, who were selected by convenience sampling.
Interventions:
Written informed consent was obtained from all patients prior to the procedure and study enrollment. For patient selection, the patients were first asked about the presence of pain, and type of pain before treatment. The respective teeth then underwent a cold test (Endo Ice Hygienic; Coltene/Whaldent, Switzerland) and electric pulp test (Redmonal CWA, Technology Crop Parkell, NY, USA). Those with a prolonged pain response to the tests were diagnosed with acute irreversible pulpitis. Patients with asymptomatic irreversible pulpitis were enrolled. Also, their radiographs were evaluated to rule out chronic apical periodontitis. The patients were then randomly assigned to two groups (n=36). The irrigants were delivered to dental clinicians in coded irrigation syringes with the same appearance.
In group 1, the root canals were irrigated with 5 mL of 1% NaOCl after using each file.
In group 2, the root canals were irrigated with 5 mL of 50% super-oxidized water after using each file.
For root canal treatment, local anesthesia was first induced by injection of 1.8 mL of 2% lidocaine with 1:80,000 epinephrine (Darupakhsh, Iran) within 45 seconds through an inferior alveolar nerve block for the mandibular teeth, and infiltration anesthesia for the maxillary teeth. After ensuring the success of anesthesia, and complete pulpal anesthesia by electric pulp testing, root canal treatment was performed by the step-back technique using hand files and frequent irrigation with the respective irrigant. All canals were instrumented minimally to #30 and maximally to #50. Flaring was performed by 5 files higher than the master apical file by 1 mm length reductions while ensuring apical patency during the entire procedure. All teeth underwent two-session endodontic treatment. At the end of the first treatment session, calcium hydroxide (Kimia, Iran) was applied in the canals as medicament, a cotton pellet was placed at the canal orifice, and the teeth were temporarily restored with Zonalin (Golchai, Iran). Occlusion was checked to ensure no occlusal interferences. Cusp reduction was also performed. Furthermore, the temporary restoration was checked in terms of gingival adaptation to ensure no pain due to food impaction. Patients with over-obturation, over-instrumentation, or any other parameter or event that could cause pain were excluded.
The patients were subsequently provided with a 170-mm visual analog scale (VAS) ruler to express their level of pain at 6, 12, 24, 47, and 72 hours, and 7 days after treatment [11]. After completion of the first treatment session, the patients were instructed on how to record their pain level using the VAS ruler. Also, the patients were reminded by phone at the respective time points to record their pain level. The VAS rulers were collected after 7 days. The rulers were number-free with the word “none” at one end (at 0 mm) and “maximum possible pain” at the other end (at 170 mm), and “faint” at 23 mm, “weak” at 36 mm, “mild” at 54 mm, “moderate” at 85 mm, “strong” at 114 mm, and “intense” at 144 mm. After collecting the rulers from the patients, they were superimposed on the graded rulers to record the pain score of patients at different time points. The number of taken analgesics by patients was also recorded. Moreover, the patients were asked how severe their pain should be on a scale of 1 to 10 to take an analgesic? And in case of reporting taking an analgesic, the respective score would be recorded [12].
Outcomes (primary and secondary):
The main objective of this study was to assess the effect of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single canal teeth. There was no secondary outcome.
Sample size calculation:
The sample size was calculated to be 36 in each group according to a study by Almeida et al, [13] and using Ordered Categorical Variables Power Analysis feature of PASS 11, assuming α=0.05, β=0.2, θ=1.5, and PC(1)=0.6.
Interim analyses and stopping guidelines:
No interim analyses were performed, and no stopping guidelines were established.
Randomization:
Eligible patients were randomly assigned to two groups by block randomization.
Blinding:
The irrigants were delivered to dental clinicians in coded irrigation syringes with the same appearance, such that the dental clinician and the patients were not aware of their content.
Statistical analysis:
The Shapiro-Wilk test indicated non-normal distribution of the data. Consequently, the two groups were compared using the Mann-Whitney test at various time points. Comparisons between different time points within each group were conducted using the Kruskal-Wallis test. A significance level of 0.05 was established.
Results
Participant flow:
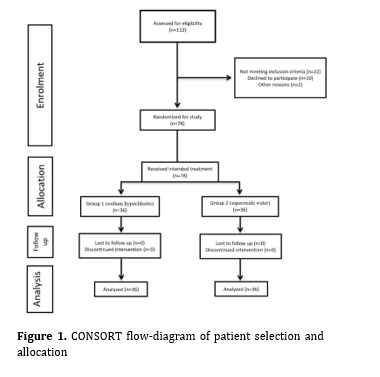
The sample consisted of 72 patients including 36 males and 36 females with a mean age of 41 years. There were 18 males and 18 females in the NaOCl group with a mean age of 39 years, and 18 males and 18 females in the super-oxidized water group with a mean age of 40 years. Figure 1 shows the CONSORT flow-diagram of patient selection and allocation.
Harms:
No patients were harmed during the study.
Subgroup analyses:
Primary outcome:
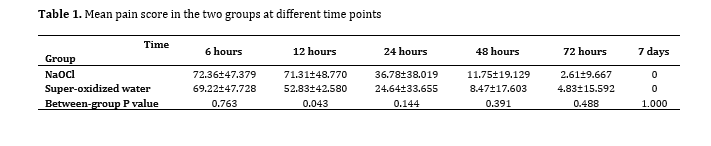
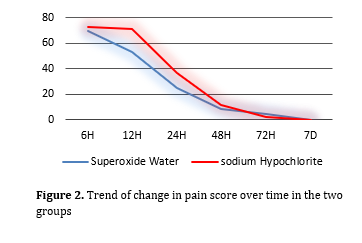
Between-group comparisons: Table 1 presents the mean pain score in the two groups at different time points. As shown, the difference in pain score was not significant at 6 hours post-treatment (P=0.8). At 12 hours, the pain score was significantly higher in the NaOCl group (P=0.043). The pain score gradually decreased in both groups after 12 hours with no pain recorded at 7 days; the difference between the two groups was not significant at any other time point (P>0.05; Figure 2).
Figure 1. CONSORT flow-diagram of patient selection and allocation
Number of taken analgesics: The number of taken analgesics was 8 in the NaOCl and 7 in the super-oxidized water group at 6 hours. The number of taken analgesics at other time points was 0 in both groups.
Table 1. Mean pain score in the two groups at different time points
Figure 2. Trend of change in pain score over time in the two groups
Discussion
This study compared the effects of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single-canal teeth. The null hypothesis of the study was that no significant difference would be found in post-endodontic pain between NaOCl and super-oxidized water groups. The results showed a significantly higher pain score in the NaOCl group only at 12 hours, postoperatively. Thus, the null hypothesis of the study was rejected. The difference between the two groups was not significant at other time points. Also, the trend of change in pain score was descending in both groups over time.
Microorganisms are among the main causes of post-endodontic pain [14]. However, only teeth with irreversible pulpitis were included in the present study, and therefore, the role of microorganisms in post-endodontic pain was ruled out in the current study. Due to the same instrumentation technique adopted in the two groups, mechanical stimulation was also the same in the two groups, and the same medicament was also applied between the two treatment sessions. Only the type of irrigant was different between the two groups. Mechanical stimulation due to instrumentation along with the high pH of calcium hydroxide [15] as well as the pain due to anesthetic injection were responsible for the comparably high pain scores in the two groups at 6 hours after treatment. Nonetheless, some others reported that calcium hydroxide application had no significant effect on post-endodontic pain [16]. The effect of irrigant with lower cytotoxicity became evident after 12 hours, resulting in significantly lower pain score in the super-oxidized water group. The pain score subsequently decreased with time in both groups after 12 hours with no significant difference between them.
Super-oxidized water is a colorless acidic solution [10], which is synthesized through saline electrolysis. In the process of electrolysis, the molecules break down, and reactive chlorine and oxygen species are formed, which can degrade the nucleic acid, proteins, and lipids [17]. The cell wall of microorganisms has a negative charge and therefore, the hypochlorous acid synthesized from super-oxidized water through chlorine reaction can penetrate into the thin cell walls of microorganisms and eliminate them or inhibit their proliferation. Low cytotoxicity and optimal biocompatibility are among other advantages of super-oxidized water [10].
Farzaneh et al. [18] evaluated the effect of irrigation with two different concentrations of sodium hypochlorite on post-endodontic pain in one-session treatment and showed lower pain score in patients who underwent root canal irrigation with 5.25% NaOCl, compared with 2.5% NaOCl, indicating the bactericidal effect of NaOCl. Mostafa et al. [19] compared the effect of irrigation with two different concentrations of NaOCl on post-endodontic pain in two-session treatment of necrotic mandibular teeth and reported lower level of post-endodontic pain in teeth that underwent irrigation with 1.3% NaOCl compared with 5.25% NaOCl. Differences between their results and those of Farzaneh et al. [18] may be due to differences in number of treatment sessions, not using calcium hydroxide by Mostafa et al. [19], method of irrigation, the possibility of extrusion of irrigant through the apex, and different root canal instrumentation and obturation techniques. Tanaka et al. [10] showed significant antimicrobial effects of super-oxidized water on different microorganisms.
A noteworthy issue is the difference in concentration of chlorine in NaOCl and super-oxidized water such that the concentration of chlorine ions in NaOCl is much higher than that in super-oxidized water. However, considering the 90% reduction in biofilm thickness and 98% reduction in colony count of microorganisms by super-oxidized water as demonstrated by Tanaka et al, [10] and lower pain level at 12 hours post-treatment in super-oxidized water group in the present study, it appears that super-oxidized water can serve as an efficient alternative to NaOCl without its adverse effects and shortcomings. Sahai et al. [20] compared the effects of root canal irrigation with 3% warm NaOCl and NaOCl at room temperature on post-endodontic pain in mandibular molars with irreversible pulpitis. They measured the pain level at 12, 24, 48, and 72 hours after treatment, and reported a significantly greater percentage of pain reduction in the warm NaOCl group at different time points, and the mean number of taken analgesics was significantly lower in this group. Mokhtari et al. [21] evaluated the effects of different concentrations and temperatures of NaOCl on pain severity after endodontic treatment of mandibular molars with irreversible pulpitis and found no significant difference between 0.5% and 1% concentrations of NaOCl used at 2.5°C, 22°C, and 40°C regarding post-endodontic pain. Variations in the results can be attributed to differences in treatment sessions, possibility of apical extrusion of solutions, different root canal preparation and obturation techniques, and differences in concentrations and temperature of NaOCl.
This study had several strengths. To the best of the authors’ knowledge, this study is the first to assess the effect of super-oxidized water on post-endodontic pain. It had a relatively large sample size and used a precise and reliable method of pain quantification [11]. Also, root canal treatment of over 75% of patients was performed by the same operator. Standardization of instrumentation and obturation techniques in all patients, and double-blind design were among other strengths of the current study.
However, pain is a subjective concept, and some inter-individual differences may affect pain perception. Future studies with a split-mouth design are recommended to eliminate the effect of such confounders on the results.
Conclusion
The present results revealed a significantly lower level of pain at 12 hours post-treatment of single-canal teeth in root canal irrigation with super-oxidized water.
Background and Aim: This study aimed to compare the effects of root canal irrigation with sodium hypochlorite (NaOCl) and super-oxidized water on post-endodontic pain in single-canal teeth.
Materials and Methods: This double-blind randomized clinical trial was conducted on 72 patients with irreversible pulpitis of single-canal teeth. The patients were randomly assigned to two groups (n=36) for root canal irrigation with either 1% NaOCl or 50% super-oxidized water during endodontic treatment. The root canals were instrumented by the step-back technique with a minimum and maximum apical preparation size of 30 and 50, respectively, and flaring by 5 files larger than the master apical file. Patients' pain level was quantified at 6, 12, 24, 48, and 72 hours, and 7 days postoperatively using a visual analog scale (VAS). Root canal treatments were accomplished in two sessions, and calcium hydroxide was applied as intracanal medicament. Data were analyzed by the Mann-Whitney test (alpha=0.05).
Results: At 12 hours postoperatively, the pain score was significantly higher in the NaOCl group than the super-oxidized water group (P=0.043). The pain score gradually decreased in both groups after 12 hours with no pain recorded at 7 days. The difference in pain score between the two groups was not significant at any other time point (P>0.05).
Conclusion: The present results revealed significantly lower level of pain at 12 hours post-treatment of single-canal teeth in root canal irrigation with super-oxidized water.
Keywords: Root Canal Irrigants; Root Canal Therapy; Sodium Hypochlorite; Superoxidized Water; Pain
Introduction
Post-endodontic pain remains a dilemma in dentistry and is responsible for increased anxiety level of patients and their poor cooperation in subsequent visits. Post-endodontic pain management is often challenging for dental clinicians [1]. Post-endodontic pain often leads to overconsumption of analgesics by patients. Although preoperative (prophylactic) and postoperative analgesic intake can significantly decrease post-endodontic pain, it cannot completely prevent it [2]. Post-endodontic pain has a high prevalence and is also experienced by 15%-25% of asymptomatic patients who do not have any pain before the procedure [3]. It has been demonstrated that type of root canal irrigant can affect post-endodontic pain. Thus, selection of an irrigant with minimal cytotoxicity, optimal antibacterial activity, and acceptable tissue dissolving property (for elimination of residual vital and necrotic tissues) is highly important [4].
Several irrigants are currently available for root canal irrigation, such as 5.25% sodium hypochlorite (NaOCl) and 2% chlorhexidine (CHX). NaOCl easily dissolves the residual pulp tissue and collagen fibers and is the only root canal irrigant capable of dissolving the viable and necrotic tissues [5]. It can also completely eliminate Enterococcus faecalis [6]. However, NaOCl has drawbacks such as cytotoxicity for the periapical tissues, the possibility of triggering an allergic reaction, bad odor, and the risk of hypochlorite accident [7]. CHX has some drawbacks as well. It cannot dissolve the residual tissues and can cause tooth discoloration [8]. Nonetheless, CHX has a broader spectrum of antibacterial activity than NaOCl [9].
Super-oxidized water is another irrigant which has gained recent popularity. It can effectively eliminate the intracanal bacteria, and has insignificant cytotoxicity for the periapical tissue [10]. It is a buffer with a neutral pH and 800 ppm effective substance and 50% concentration. Its effective substance reaches a concentration of 350-400 ppm after dilution. It is a shared product of Russia and Japan (Envirolyte, Tokyo, Japan).
To the best of the authors’ knowledge, the effect of root canal irrigation with super-oxidized water on post-endodontic pain has not been previously investigated. Thus, this study aimed to compare the effects of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single-canal teeth. The null hypothesis of the study was that no significant difference would be found in post-endodontic pain between NaOCl and super-oxidized water groups.
Materials and Methods
This study was conducted at the Faculty of Dentistry, Tehran Medical Science, Islamic Azad University between 2019 and 2020. The study protocol was approved by the ethics committee of the university (IR.IAU.DENTAL.REC.1399.040) and registered in the Iranian Registry of Clinical Trials (IRCT20200517047478N1).
Trial design:
A randomized double-blind clinical trial was designed in which one group received root canal irrigation with NaOCl and the other group received root canal irrigation with super-oxidized water during endodontic treatment of single-canal teeth. The results were reported in accordance with the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were age range of 18 to 65 years, no pregnancy, no systemic diseases (ASA Class I and II), no history of allergy or toxic reaction to anesthetic agents, no intake of sedative, anxiolytic, or analgesic medications within 6 hours prior to treatment, having asymptomatic irreversible pulpitis of at least one single-canal tooth, no severe periodontal disease, and signing informed consent forms. The respective tooth had to be vital, with no sensitivity to percussion, and moderate to severe pain response to sensibility tests with no periapical lesion or periodontal ligament widening on radiographs.
The sample consisted of 72 patients presenting to the Endodontics Department of the Faculty of Dentistry, Tehran Medical Science, Islamic Azad University with single-rooted teeth requiring endodontic treatment, who were selected by convenience sampling.
Interventions:
Written informed consent was obtained from all patients prior to the procedure and study enrollment. For patient selection, the patients were first asked about the presence of pain, and type of pain before treatment. The respective teeth then underwent a cold test (Endo Ice Hygienic; Coltene/Whaldent, Switzerland) and electric pulp test (Redmonal CWA, Technology Crop Parkell, NY, USA). Those with a prolonged pain response to the tests were diagnosed with acute irreversible pulpitis. Patients with asymptomatic irreversible pulpitis were enrolled. Also, their radiographs were evaluated to rule out chronic apical periodontitis. The patients were then randomly assigned to two groups (n=36). The irrigants were delivered to dental clinicians in coded irrigation syringes with the same appearance.
In group 1, the root canals were irrigated with 5 mL of 1% NaOCl after using each file.
In group 2, the root canals were irrigated with 5 mL of 50% super-oxidized water after using each file.
For root canal treatment, local anesthesia was first induced by injection of 1.8 mL of 2% lidocaine with 1:80,000 epinephrine (Darupakhsh, Iran) within 45 seconds through an inferior alveolar nerve block for the mandibular teeth, and infiltration anesthesia for the maxillary teeth. After ensuring the success of anesthesia, and complete pulpal anesthesia by electric pulp testing, root canal treatment was performed by the step-back technique using hand files and frequent irrigation with the respective irrigant. All canals were instrumented minimally to #30 and maximally to #50. Flaring was performed by 5 files higher than the master apical file by 1 mm length reductions while ensuring apical patency during the entire procedure. All teeth underwent two-session endodontic treatment. At the end of the first treatment session, calcium hydroxide (Kimia, Iran) was applied in the canals as medicament, a cotton pellet was placed at the canal orifice, and the teeth were temporarily restored with Zonalin (Golchai, Iran). Occlusion was checked to ensure no occlusal interferences. Cusp reduction was also performed. Furthermore, the temporary restoration was checked in terms of gingival adaptation to ensure no pain due to food impaction. Patients with over-obturation, over-instrumentation, or any other parameter or event that could cause pain were excluded.
The patients were subsequently provided with a 170-mm visual analog scale (VAS) ruler to express their level of pain at 6, 12, 24, 47, and 72 hours, and 7 days after treatment [11]. After completion of the first treatment session, the patients were instructed on how to record their pain level using the VAS ruler. Also, the patients were reminded by phone at the respective time points to record their pain level. The VAS rulers were collected after 7 days. The rulers were number-free with the word “none” at one end (at 0 mm) and “maximum possible pain” at the other end (at 170 mm), and “faint” at 23 mm, “weak” at 36 mm, “mild” at 54 mm, “moderate” at 85 mm, “strong” at 114 mm, and “intense” at 144 mm. After collecting the rulers from the patients, they were superimposed on the graded rulers to record the pain score of patients at different time points. The number of taken analgesics by patients was also recorded. Moreover, the patients were asked how severe their pain should be on a scale of 1 to 10 to take an analgesic? And in case of reporting taking an analgesic, the respective score would be recorded [12].
Outcomes (primary and secondary):
The main objective of this study was to assess the effect of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single canal teeth. There was no secondary outcome.
Sample size calculation:
The sample size was calculated to be 36 in each group according to a study by Almeida et al, [13] and using Ordered Categorical Variables Power Analysis feature of PASS 11, assuming α=0.05, β=0.2, θ=1.5, and PC(1)=0.6.
Interim analyses and stopping guidelines:
No interim analyses were performed, and no stopping guidelines were established.
Randomization:
Eligible patients were randomly assigned to two groups by block randomization.
Blinding:
The irrigants were delivered to dental clinicians in coded irrigation syringes with the same appearance, such that the dental clinician and the patients were not aware of their content.
Statistical analysis:
The Shapiro-Wilk test indicated non-normal distribution of the data. Consequently, the two groups were compared using the Mann-Whitney test at various time points. Comparisons between different time points within each group were conducted using the Kruskal-Wallis test. A significance level of 0.05 was established.
Results
Participant flow:
The sample consisted of 72 patients including 36 males and 36 females with a mean age of 41 years. There were 18 males and 18 females in the NaOCl group with a mean age of 39 years, and 18 males and 18 females in the super-oxidized water group with a mean age of 40 years. Figure 1 shows the CONSORT flow-diagram of patient selection and allocation.
Harms:
No patients were harmed during the study.
Subgroup analyses:
Primary outcome:
Between-group comparisons: Table 1 presents the mean pain score in the two groups at different time points. As shown, the difference in pain score was not significant at 6 hours post-treatment (P=0.8). At 12 hours, the pain score was significantly higher in the NaOCl group (P=0.043). The pain score gradually decreased in both groups after 12 hours with no pain recorded at 7 days; the difference between the two groups was not significant at any other time point (P>0.05; Figure 2).
Figure 1. CONSORT flow-diagram of patient selection and allocation
{kind=link}
Number of taken analgesics: The number of taken analgesics was 8 in the NaOCl and 7 in the super-oxidized water group at 6 hours. The number of taken analgesics at other time points was 0 in both groups.
Table 1. Mean pain score in the two groups at different time points
{kind=link}
Figure 2. Trend of change in pain score over time in the two groups
{kind=link}
Discussion
This study compared the effects of root canal irrigation with NaOCl and super-oxidized water on post-endodontic pain in single-canal teeth. The null hypothesis of the study was that no significant difference would be found in post-endodontic pain between NaOCl and super-oxidized water groups. The results showed a significantly higher pain score in the NaOCl group only at 12 hours, postoperatively. Thus, the null hypothesis of the study was rejected. The difference between the two groups was not significant at other time points. Also, the trend of change in pain score was descending in both groups over time.
Microorganisms are among the main causes of post-endodontic pain [14]. However, only teeth with irreversible pulpitis were included in the present study, and therefore, the role of microorganisms in post-endodontic pain was ruled out in the current study. Due to the same instrumentation technique adopted in the two groups, mechanical stimulation was also the same in the two groups, and the same medicament was also applied between the two treatment sessions. Only the type of irrigant was different between the two groups. Mechanical stimulation due to instrumentation along with the high pH of calcium hydroxide [15] as well as the pain due to anesthetic injection were responsible for the comparably high pain scores in the two groups at 6 hours after treatment. Nonetheless, some others reported that calcium hydroxide application had no significant effect on post-endodontic pain [16]. The effect of irrigant with lower cytotoxicity became evident after 12 hours, resulting in significantly lower pain score in the super-oxidized water group. The pain score subsequently decreased with time in both groups after 12 hours with no significant difference between them.
Super-oxidized water is a colorless acidic solution [10], which is synthesized through saline electrolysis. In the process of electrolysis, the molecules break down, and reactive chlorine and oxygen species are formed, which can degrade the nucleic acid, proteins, and lipids [17]. The cell wall of microorganisms has a negative charge and therefore, the hypochlorous acid synthesized from super-oxidized water through chlorine reaction can penetrate into the thin cell walls of microorganisms and eliminate them or inhibit their proliferation. Low cytotoxicity and optimal biocompatibility are among other advantages of super-oxidized water [10].
Farzaneh et al. [18] evaluated the effect of irrigation with two different concentrations of sodium hypochlorite on post-endodontic pain in one-session treatment and showed lower pain score in patients who underwent root canal irrigation with 5.25% NaOCl, compared with 2.5% NaOCl, indicating the bactericidal effect of NaOCl. Mostafa et al. [19] compared the effect of irrigation with two different concentrations of NaOCl on post-endodontic pain in two-session treatment of necrotic mandibular teeth and reported lower level of post-endodontic pain in teeth that underwent irrigation with 1.3% NaOCl compared with 5.25% NaOCl. Differences between their results and those of Farzaneh et al. [18] may be due to differences in number of treatment sessions, not using calcium hydroxide by Mostafa et al. [19], method of irrigation, the possibility of extrusion of irrigant through the apex, and different root canal instrumentation and obturation techniques. Tanaka et al. [10] showed significant antimicrobial effects of super-oxidized water on different microorganisms.
A noteworthy issue is the difference in concentration of chlorine in NaOCl and super-oxidized water such that the concentration of chlorine ions in NaOCl is much higher than that in super-oxidized water. However, considering the 90% reduction in biofilm thickness and 98% reduction in colony count of microorganisms by super-oxidized water as demonstrated by Tanaka et al, [10] and lower pain level at 12 hours post-treatment in super-oxidized water group in the present study, it appears that super-oxidized water can serve as an efficient alternative to NaOCl without its adverse effects and shortcomings. Sahai et al. [20] compared the effects of root canal irrigation with 3% warm NaOCl and NaOCl at room temperature on post-endodontic pain in mandibular molars with irreversible pulpitis. They measured the pain level at 12, 24, 48, and 72 hours after treatment, and reported a significantly greater percentage of pain reduction in the warm NaOCl group at different time points, and the mean number of taken analgesics was significantly lower in this group. Mokhtari et al. [21] evaluated the effects of different concentrations and temperatures of NaOCl on pain severity after endodontic treatment of mandibular molars with irreversible pulpitis and found no significant difference between 0.5% and 1% concentrations of NaOCl used at 2.5°C, 22°C, and 40°C regarding post-endodontic pain. Variations in the results can be attributed to differences in treatment sessions, possibility of apical extrusion of solutions, different root canal preparation and obturation techniques, and differences in concentrations and temperature of NaOCl.
This study had several strengths. To the best of the authors’ knowledge, this study is the first to assess the effect of super-oxidized water on post-endodontic pain. It had a relatively large sample size and used a precise and reliable method of pain quantification [11]. Also, root canal treatment of over 75% of patients was performed by the same operator. Standardization of instrumentation and obturation techniques in all patients, and double-blind design were among other strengths of the current study.
However, pain is a subjective concept, and some inter-individual differences may affect pain perception. Future studies with a split-mouth design are recommended to eliminate the effect of such confounders on the results.
Conclusion
The present results revealed a significantly lower level of pain at 12 hours post-treatment of single-canal teeth in root canal irrigation with super-oxidized water.
Type of Study: Randomized Clinical Trial |
Subject:
Endodontics
References
1. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013 Dec;58(4):390-407; quiz 531. [DOI:10.1111/adj.12118] [PMID]
2. DiRenzo A, Gresla T, Johnson BR, Rogers M, Tucker D, BeGole EA. Postoperative pain after 1- and 2-visit root canal therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002 May;93(5):605-10. [DOI:10.1067/moe.2002.121900] [PMID]
3. Alí A, Olivieri JG, Duran-Sindreu F, Abella F, Roig M, García-Font M. Influence of preoperative pain intensity on postoperative pain after root canal treatment: A prospective clinical study. J Dent. 2016 Feb;45:39-42. [DOI:10.1016/j.jdent.2015.12.002] [PMID]
4. Ercan E, Ozekinci T, Atakul F, Gül K. Antibacterial activity of 2% chlorhexidine gluconate and 5.25% sodium hypochlorite in infected root canal: in vivo study. J Endod. 2004 Feb;30(2):84-7. [DOI:10.1097/00004770-200402000-00005] [PMID]
5. Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014 Mar;216(6):299-303. [DOI:10.1038/sj.bdj.2014.204] [PMID]
6. Solana C, Ruiz-Linares M, Baca P, Valderrama MJ, Arias-Moliz MT, Ferrer-Luque CM. Antibiofilm Activity of Sodium Hypochlorite and Alkaline Tetrasodium EDTA Solutions. J Endod. 2017 Dec;43(12):2093-6. [DOI:10.1016/j.joen.2017.06.038] [PMID]
7. Slaughter RJ, Watts M, Vale JA, Grieve JR, Schep LJ. The clinical toxicology of sodium hypochlorite. Clin Toxicol (Phila). 2019 May;57(5):303-11. [DOI:10.1080/15563650.2018.1543889] [PMID]
8. Bashetty K, Hegde J. Comparison of 2% chlorhexidine and 5.25% sodium hypochlorite irrigating solutions on postoperative pain: a randomized clinical trial. Indian J Dent Res. 2010 Oct-Dec;21(4):523-7. [DOI:10.4103/0970-9290.74225] [PMID]
9. Gomes BP, Vianna ME, Zaia AA, Almeida JF, Souza-Filho FJ, Ferraz CC. Chlorhexidine in endodontics. Braz Dent J. 2013;24(2):89-102. [DOI:10.1590/0103-6440201302188] [PMID]
10. Tanaka H, Hirakata Y, Kaku M, Yoshida R, Takemura H, Mizukane R, Ishida K, Tomono K, Koga H, Kohno S, Kamihira S. Antimicrobial activity of superoxidized water. J Hosp Infect. 1996 Sep;34(1):43-9. [DOI:10.1016/S0195-6701(96)90124-3] [PMID]
11. Sung YT, Wu JS. The Visual Analogue Scale for Rating, Ranking and Paired-Comparison (VAS-RRP): A new technique for psychological measurement. Behav Res Methods. 2018 Aug;50(4):1694-715. [DOI:10.3758/s13428-018-1041-8] [PMID] []
12. Rago R, Forfori F, Materazzi G, Abramo A, Collareta M, Miccoli P, Giunta F. Evaluation of a preoperative pain score in response to pressure as a marker of postoperative pain and drugs consumption in surgical thyroidectomy. Clin J Pain. 2012 Jun;28(5):382-6. [DOI:10.1097/AJP.0b013e3182326495] [PMID]
13. Almeida G, Marques E, De Martin AS, da Silveira Bueno CE, Nowakowski A, Cunha RS. Influence of irrigating solution on postoperative pain following single-visit endodontic treatment: randomized clinical trial. J Can Dent Assoc. 2012;78:c84.
14. Sipavičiūtė E, Manelienė R. Pain and flare-up after endodontic treatment procedures. Stomatologija. 2014;16(1):25-30.
15. Carvalho CN, Freire LG, Carvalho AP, Duarte MA, Bauer J, Gavini G. Ions Release and pH of Calcium Hydroxide-, Chlorhexidine- and Bioactive Glass-Based Endodontic Medicaments. Braz Dent J. 2016 May-Jun;27(3):325-31. [DOI:10.1590/0103-6440201600602] [PMID]
16. Samir Abouelenien S, Mohamed Ibrahim S, Gameel Shaker O, Mohamed Ahmed G. Evaluation of postoperative pain in infected root canals after using double antibiotic paste versus calcium hydroxide as intra-canal medication: A randomized controlled trial. F1000Res. 2018 Nov 8;7:1768. [DOI:10.12688/f1000research.16820.1] [PMID] []
17. González-Espinosa D, Pérez-Romano L, Guzmán-Soriano B, Arias E, Bongiovanni CM, Gutiérrez AA. Effects of pH-neutral, super-oxidised solution on human dermal fibroblasts in vitro. Int Wound J. 2007 Sep;4(3):241-50. [DOI:10.1111/j.1742-481X.2007.00331.x] [PMID] []
18. Farzaneh S, Parirokh M, Nakhaee N, Abbott PV. Effect of two different concentrations of sodium hypochlorite on postoperative pain following single-visit root canal treatment: a triple-blind randomized clinical trial. Int Endod J. 2018 Jan;51 Suppl 1:e2-e11. [DOI:10.1111/iej.12749] [PMID]
19. Mostafa MEHAA, El-Shrief YAI, Anous WIO, Hassan MW, Salamah FTA, El Boghdadi RM, El-Bayoumi MAA, Seyam RM, Abd-El-Kader KG, Amin SAW. Postoperative pain following endodontic irrigation using 1.3% versus 5.25% sodium hypochlorite in mandibular molars with necrotic pulps: a randomized double-blind clinical trial. Int Endod J. 2020 Feb;53(2):154-66. [DOI:10.1111/iej.13222] [PMID]
20. Sahai A, Gupta A, Abraham D, Aggarwal V, Singh A, Sharma G, Gurawa A. Evaluation of postoperative pain using warm versus room temperature sodium hypochlorite as an irrigant in mandibular molars with irreversible pulpitis: A randomized controlled trial. J Conserv Dent Endod. 2023 Jul-Aug;26(4): 458-65.
21. Mokhtari H, Milani AS, Zand V, Shakuie S, Nazari L. The effect of different concentrations and temperatures of sodium hypochlorite irrigation on pain intensity following endodontic treatment of mandibular molars with irreversible pulpitis: A randomized, double-blind clinical trial. Clin Exp Dent Res. 2023 Oct;9(5):859-67. [DOI:10.1002/cre2.754] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |