Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 2 (6-2024)
J Res Dent Maxillofac Sci 2024, 9(2): 124-128 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kumar N, Kumari R. Anterior Crossbite Correction in Mixed Dentition Using a Simple Appliance: A Case Series. J Res Dent Maxillofac Sci 2024; 9 (2) :124-128
URL: http://jrdms.dentaliau.ac.ir/article-1-551-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-551-en.html



1- Department of Paediatric Dentistry, Post Graduate Institute of Child Health, Noida, Uttar Pradesh, India. , dr.neeraj001@gmail.com
2- Department of Paediatric Dentistry, PGIDS, Rohtak, Haryana, India.
2- Department of Paediatric Dentistry, PGIDS, Rohtak, Haryana, India.
Full-Text [PDF 330 kb]
(5704 Downloads)
| Abstract (HTML) (3699 Views)
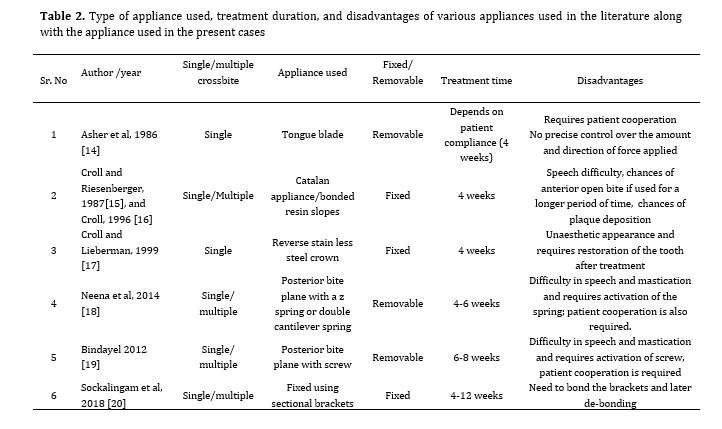
Table 2. Type of appliance used, treatment duration, and disadvantages of various appliances used in the literature along with the appliance used in the present cases
Removable appliances are safe, easy to fabricate chair side, esthetically acceptable, and easily cleanable. In the present cases, removable posterior bite planes with palatal plates were used, and the crossbite was corrected without addition of any spring or screw. The compliance of patients was good and they did not report any complication during the course of treatment and follow-up.
Conclusion
A posterior bite plane with a palatal plate is an alternative acceptable removable appliance for correction of anterior dental crossbite compared to complex fixed orthodontic appliances. In all the reported cases, correction was achieved within 4 to 6 weeks with no damage to marginal periodontal tissue. The appliance used is a simple appliance, which is easy to fabricate chair side, and corrects the single tooth crossbite efficiently. Early diagnosis and immediate intervention are required to intercept the development of malocclusion. Thus, this appliance can be used to correct anterior tooth crossbite during the mixed dentition period.
Full-Text: (3919 Views)
Abstract
Background and Aim: Anterior crossbite is the most commonly observed developing malocclusion during the mixed dentition period. Dental crossbite occurs due to over-retained deciduous teeth or their delayed exfoliation, impacted or supernumerary teeth, pathologies present around the affected teeth, or dental trauma during the primary dentition period. Various removable and fixed appliances have been used in the literature for correction of crossbite depending on the patient's age, and space availability in dental arch.
Case Presentation: This paper presents a case series of anterior crossbite cases corrected using a simple posterior bite plane appliance. This appliance is simple, easy to fabricate, and takes less time to correct the crossbite.
Conclusion: A posterior bite plane with a palatal plate could be an efficient solution for correction of anterior dental crossbite in the mixed dentition period. This chair-side fabricated appliance achieves correction quickly without harming the periodontal tissue. Developing malocclusions should be immediately identified by dentists to prevent complex treatment options in the future.
Key Words: Malocclusion; Incisor; Orthodontics, Interceptive; Dentition, Mixed
Introduction
Dental crossbite is a type of malocclusion in which normal buccolingual/labiolingual relationships of the teeth are reversed [1]. Crossbite may be skeletal or dental, depending on the position of the jaws and teeth or both [2]. In dental crossbite, there is a deviation in the buccolingual inclination of the involved tooth or teeth without altering the skeletal relationship. Anterior crossbite is defined as “a malocclusion in which one or more of the maxillary anterior teeth occlude lingually to the mandibular incisors” [3]. Single tooth crossbite is the most commonly encountered malocclusion in growing children during the mixed dentition period [3]. Various reasons may cause dental crossbite such as palatally erupting maxillary anterior teeth, over-retained deciduous tooth or root, presence of supernumerary teeth or any periapical pathology, inadequate arch length, crowding, and cleft lip and/or palate [4-6].
This developing malocclusion requires immediate interceptive orthodontic treatment to prevent mobility, periodontal inflammation, anterior tooth fracture, and temporomandibular joint problems [7]. There are many interceptive methods to treat the developing dental crossbite. Various methods such as tongue blade therapy, lower inclined plane, reverse stainless-steel crowns, Hawley retainer with springs or screws, and labial or lingual archwires have been previously used for this purpose [8]. This case series presents a simple and economical method to treat anterior dental crossbite using a posterior bite plane with a palatal plate.
Case Presentation
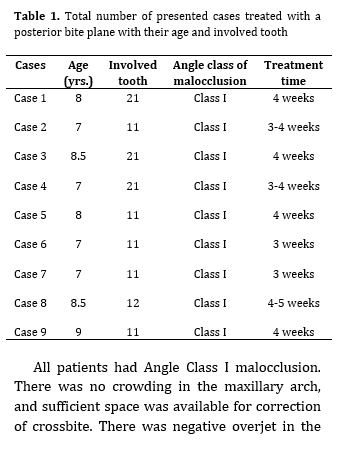
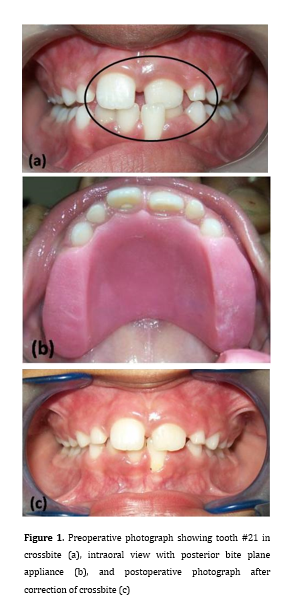
Nine patients between 7-8 years of age were evaluated with a chief complaint of palatally placed upper front teeth (Table 1). A detailed medical and dental history was taken with no remarkable finding. On extra-oral examination, the patients had a symmetrical face with a convex profile and competent lips. Intra-oral examination revealed that the patients were in the mixed dentition period with unilateral crossbite of a maxillary anterior tooth in the right or left side (Figure 1a).
Table 1. Total number of presented cases treated with a posterior bite plane with their age and involved tooth
All patients had Angle Class I malocclusion. There was no crowding in the maxillary arch, and sufficient space was available for correction of crossbite. There was negative overjet in the affected maxillary tooth. Gingival recession of the opposing mandibular anterior teeth was also present in few cases. Intraoral periapical radiography was requested to detect any periapical pathology or presence of a supernumerary tooth. A lateral cephalogram was not requested since it was more of a dental problem rather than skeletal in the developing mixed dentition. The parents were counseled about the developing malocclusion and told about the interceptive treatment plan. After obtaining informed consent, the treatment was started, and the appliance was fabricated using auto-polymerizing acrylic resin.
Fabrication of appliance:
Upper and lower arch impressions were made with irreversible hydrocolloid material i.e. alginate. Impressions were poured with dental stone, and a positive replica was duplicated. The wire components i.e. pin head clasps were fabricated using 21-gauge wire on maxillary molars. The wire components were fixed with auto-polymerizing acrylic resin (DPI, Mumbai, India), and a posterior bite plane was fabricated with palatal coverage. The appliance was inserted and checked for any gingival irritation and occlusal clearance of 2-3 mm to allow spontaneous movement of the affected tooth (Figure 1b). After 4-6 weeks, the crossbite was corrected and the appliance was removed after obtaining positive overjet (Figure 1c). No retention appliance was needed in any case after correction and achievement of positive overjet. The cases were followed-up for a period of 3 months and there was no relapse or any other deviation.
Background and Aim: Anterior crossbite is the most commonly observed developing malocclusion during the mixed dentition period. Dental crossbite occurs due to over-retained deciduous teeth or their delayed exfoliation, impacted or supernumerary teeth, pathologies present around the affected teeth, or dental trauma during the primary dentition period. Various removable and fixed appliances have been used in the literature for correction of crossbite depending on the patient's age, and space availability in dental arch.
Case Presentation: This paper presents a case series of anterior crossbite cases corrected using a simple posterior bite plane appliance. This appliance is simple, easy to fabricate, and takes less time to correct the crossbite.
Conclusion: A posterior bite plane with a palatal plate could be an efficient solution for correction of anterior dental crossbite in the mixed dentition period. This chair-side fabricated appliance achieves correction quickly without harming the periodontal tissue. Developing malocclusions should be immediately identified by dentists to prevent complex treatment options in the future.
Key Words: Malocclusion; Incisor; Orthodontics, Interceptive; Dentition, Mixed
Introduction
Dental crossbite is a type of malocclusion in which normal buccolingual/labiolingual relationships of the teeth are reversed [1]. Crossbite may be skeletal or dental, depending on the position of the jaws and teeth or both [2]. In dental crossbite, there is a deviation in the buccolingual inclination of the involved tooth or teeth without altering the skeletal relationship. Anterior crossbite is defined as “a malocclusion in which one or more of the maxillary anterior teeth occlude lingually to the mandibular incisors” [3]. Single tooth crossbite is the most commonly encountered malocclusion in growing children during the mixed dentition period [3]. Various reasons may cause dental crossbite such as palatally erupting maxillary anterior teeth, over-retained deciduous tooth or root, presence of supernumerary teeth or any periapical pathology, inadequate arch length, crowding, and cleft lip and/or palate [4-6].
This developing malocclusion requires immediate interceptive orthodontic treatment to prevent mobility, periodontal inflammation, anterior tooth fracture, and temporomandibular joint problems [7]. There are many interceptive methods to treat the developing dental crossbite. Various methods such as tongue blade therapy, lower inclined plane, reverse stainless-steel crowns, Hawley retainer with springs or screws, and labial or lingual archwires have been previously used for this purpose [8]. This case series presents a simple and economical method to treat anterior dental crossbite using a posterior bite plane with a palatal plate.
Case Presentation
Nine patients between 7-8 years of age were evaluated with a chief complaint of palatally placed upper front teeth (Table 1). A detailed medical and dental history was taken with no remarkable finding. On extra-oral examination, the patients had a symmetrical face with a convex profile and competent lips. Intra-oral examination revealed that the patients were in the mixed dentition period with unilateral crossbite of a maxillary anterior tooth in the right or left side (Figure 1a).
Table 1. Total number of presented cases treated with a posterior bite plane with their age and involved tooth
{kind=link}
All patients had Angle Class I malocclusion. There was no crowding in the maxillary arch, and sufficient space was available for correction of crossbite. There was negative overjet in the affected maxillary tooth. Gingival recession of the opposing mandibular anterior teeth was also present in few cases. Intraoral periapical radiography was requested to detect any periapical pathology or presence of a supernumerary tooth. A lateral cephalogram was not requested since it was more of a dental problem rather than skeletal in the developing mixed dentition. The parents were counseled about the developing malocclusion and told about the interceptive treatment plan. After obtaining informed consent, the treatment was started, and the appliance was fabricated using auto-polymerizing acrylic resin.
Fabrication of appliance:
Upper and lower arch impressions were made with irreversible hydrocolloid material i.e. alginate. Impressions were poured with dental stone, and a positive replica was duplicated. The wire components i.e. pin head clasps were fabricated using 21-gauge wire on maxillary molars. The wire components were fixed with auto-polymerizing acrylic resin (DPI, Mumbai, India), and a posterior bite plane was fabricated with palatal coverage. The appliance was inserted and checked for any gingival irritation and occlusal clearance of 2-3 mm to allow spontaneous movement of the affected tooth (Figure 1b). After 4-6 weeks, the crossbite was corrected and the appliance was removed after obtaining positive overjet (Figure 1c). No retention appliance was needed in any case after correction and achievement of positive overjet. The cases were followed-up for a period of 3 months and there was no relapse or any other deviation.
Figure 1. Preoperative photograph showing tooth #21 in crossbite (a), intraoral view with posterior bite plane appliance (b), and postoperative photograph after correction of crossbite (c)
Discussion
Anterior dental crossbite is a condition with major esthetic and functional concerns for children which needs interceptive intervention. Also, developing Class III or pseudo-Class III malocclusion with moderate to severe anterior dental crossbite may require immediate intervention. Dental crossbite may be caused due to palatally erupting maxillary anterior teeth, over-retained deciduous tooth or root, presence of supernumerary teeth or any periapical pathology, inadequate arch length, crowding, or cleft lip and palate [4-6].
Anterior dental crossbite results from functional forward shift of the mandible without any skeletal discrepancy. If the mandible is guided in centric relation, then a normal overjet or labio-lingual relationship of incisors can be obtained. If immediate intervention is not performed, it may lead to a skeletal malocclusion which requires more complex treatments. The ideal age to intercept dental crossbite is between 8 to 11 years, the period when the tooth is in the active eruption stage. There are few factors like age of the child, number of teeth involved or required repositioning, degree of overbite, and motivation of the child towards treatment which should be taken into consideration during treatment planning [9,10]. There are additional factors which should also be considered like adequate space in the arch, sufficient overbite to maintain the tooth in position after correction, Class I occlusion, and apical position of the tooth in crossbite that is the same as it would be in normal occlusion [11].
Developing malocclusion involving a single tooth during mixed dentition period can be easily corrected with removable appliances and does not require a comprehensive fixed orthodontic treatment. The positive overjet obtained after anterior crossbite correction is self-retentive; thus, there is no need for any retention appliance. The appliance should be worn the entire day while having meals also. The appliance should be stored in an airtight container and should be cleaned using soap solution and soft bristle brush. Oral hygiene instructions should be given to patients to prevent halitosis. The only disadvantage of removable appliances that needs to be addressed is patient compliance for regular wear, maintenance, and cleaning of the appliance.
Interceptive orthodontic procedures are commonly used in mixed dentition period to correct the developing malocclusion. Anterior crossbite is not a self-correcting condition due to locking of the upper incisor with respect to the lower incisor which causes severe malocclusion at the later stages. Thus, immediate intervention is required which establishes the muscle balance and enables a well-organized occlusal development [12,13]. There are various appliances which can be used for correction of anterior crossbite like tongue blade, reverse stainless-steel crown, reverse inclined plane or composite plane, the Hawley’s appliance with a ‘z’ spring and expansion screw, and other fixed orthodontic appliances [4-6]. Different appliances used for anterior bite correction, treatment duration, and their disadvantages are presented in Table 2 [14-20]. In tongue blade therapy, patients are instructed to put the tongue blade on the palatal aspect of the maxillary incisors, and the patients are asked to bite so that it comes in contact with the mandibular incisors acting as a fulcrum, which absorbs the reciprocating forces and generates forward thrust to the maxillary incisor. This technique is rarely used when more than one tooth is involved in the crossbite, and patient compliance is needed which is difficult in children.
Unesthetic appearance and difficulty in adapting a reverse stainless-steel crown to the tooth in crossbite are the main disadvantages of using reverse stainless-steel crowns [15]. A composite inclined bite plane is a simple and non-invasive method but it cannot be used in cases where the anterior crossbite exceeds 1/3 the crown length. Moreover, it may cause gingivitis because of the plaque deposition adjacent to the appliance and gingival area [10]. In cases of Hawley's appliance with a ‘z’ or double cantilever spring or with an expansion screw, frequent activation or expansion of the appliance is required. In the present cases, a simple posterior bite plane appliance was used without a ‘z’ spring or expansion screw, and anterior crossbite was corrected with positive overjet obviating the need for a retention appliance. The only shortcoming with this appliance is difficulty in mastication and speech in the initial few days, which is common to all removable appliances. The possible maxillary tooth movement was induced by tongue forces, exerted to the tooth in crossbite during function, such as speech and swallowing, as well as during rest [21, 22].
{kind=link}
Discussion
Anterior dental crossbite is a condition with major esthetic and functional concerns for children which needs interceptive intervention. Also, developing Class III or pseudo-Class III malocclusion with moderate to severe anterior dental crossbite may require immediate intervention. Dental crossbite may be caused due to palatally erupting maxillary anterior teeth, over-retained deciduous tooth or root, presence of supernumerary teeth or any periapical pathology, inadequate arch length, crowding, or cleft lip and palate [4-6].
Anterior dental crossbite results from functional forward shift of the mandible without any skeletal discrepancy. If the mandible is guided in centric relation, then a normal overjet or labio-lingual relationship of incisors can be obtained. If immediate intervention is not performed, it may lead to a skeletal malocclusion which requires more complex treatments. The ideal age to intercept dental crossbite is between 8 to 11 years, the period when the tooth is in the active eruption stage. There are few factors like age of the child, number of teeth involved or required repositioning, degree of overbite, and motivation of the child towards treatment which should be taken into consideration during treatment planning [9,10]. There are additional factors which should also be considered like adequate space in the arch, sufficient overbite to maintain the tooth in position after correction, Class I occlusion, and apical position of the tooth in crossbite that is the same as it would be in normal occlusion [11].
Developing malocclusion involving a single tooth during mixed dentition period can be easily corrected with removable appliances and does not require a comprehensive fixed orthodontic treatment. The positive overjet obtained after anterior crossbite correction is self-retentive; thus, there is no need for any retention appliance. The appliance should be worn the entire day while having meals also. The appliance should be stored in an airtight container and should be cleaned using soap solution and soft bristle brush. Oral hygiene instructions should be given to patients to prevent halitosis. The only disadvantage of removable appliances that needs to be addressed is patient compliance for regular wear, maintenance, and cleaning of the appliance.
Interceptive orthodontic procedures are commonly used in mixed dentition period to correct the developing malocclusion. Anterior crossbite is not a self-correcting condition due to locking of the upper incisor with respect to the lower incisor which causes severe malocclusion at the later stages. Thus, immediate intervention is required which establishes the muscle balance and enables a well-organized occlusal development [12,13]. There are various appliances which can be used for correction of anterior crossbite like tongue blade, reverse stainless-steel crown, reverse inclined plane or composite plane, the Hawley’s appliance with a ‘z’ spring and expansion screw, and other fixed orthodontic appliances [4-6]. Different appliances used for anterior bite correction, treatment duration, and their disadvantages are presented in Table 2 [14-20]. In tongue blade therapy, patients are instructed to put the tongue blade on the palatal aspect of the maxillary incisors, and the patients are asked to bite so that it comes in contact with the mandibular incisors acting as a fulcrum, which absorbs the reciprocating forces and generates forward thrust to the maxillary incisor. This technique is rarely used when more than one tooth is involved in the crossbite, and patient compliance is needed which is difficult in children.
Unesthetic appearance and difficulty in adapting a reverse stainless-steel crown to the tooth in crossbite are the main disadvantages of using reverse stainless-steel crowns [15]. A composite inclined bite plane is a simple and non-invasive method but it cannot be used in cases where the anterior crossbite exceeds 1/3 the crown length. Moreover, it may cause gingivitis because of the plaque deposition adjacent to the appliance and gingival area [10]. In cases of Hawley's appliance with a ‘z’ or double cantilever spring or with an expansion screw, frequent activation or expansion of the appliance is required. In the present cases, a simple posterior bite plane appliance was used without a ‘z’ spring or expansion screw, and anterior crossbite was corrected with positive overjet obviating the need for a retention appliance. The only shortcoming with this appliance is difficulty in mastication and speech in the initial few days, which is common to all removable appliances. The possible maxillary tooth movement was induced by tongue forces, exerted to the tooth in crossbite during function, such as speech and swallowing, as well as during rest [21, 22].
Table 2. Type of appliance used, treatment duration, and disadvantages of various appliances used in the literature along with the appliance used in the present cases
{kind=link}
Removable appliances are safe, easy to fabricate chair side, esthetically acceptable, and easily cleanable. In the present cases, removable posterior bite planes with palatal plates were used, and the crossbite was corrected without addition of any spring or screw. The compliance of patients was good and they did not report any complication during the course of treatment and follow-up.
Conclusion
A posterior bite plane with a palatal plate is an alternative acceptable removable appliance for correction of anterior dental crossbite compared to complex fixed orthodontic appliances. In all the reported cases, correction was achieved within 4 to 6 weeks with no damage to marginal periodontal tissue. The appliance used is a simple appliance, which is easy to fabricate chair side, and corrects the single tooth crossbite efficiently. Early diagnosis and immediate intervention are required to intercept the development of malocclusion. Thus, this appliance can be used to correct anterior tooth crossbite during the mixed dentition period.
Type of Study: Case report |
Subject:
pediatric
References
1. Lindauer SJ. The basic of orthodontic mechanics. Seminars in orthodontics. 2001; 7(1):2-15. [DOI:10.1053/sodo.2001.21053]
2. Jirgensone I, Liepa A, Abeltins A. Anterior crossbite correction in primary and mixed dentition with removable inclined plane (Bruckl appliance). Stomatologija. 2008;10(4):140-4.
3. Prakash P, Durgesh BH. Anterior Crossbite Correction in Early Mixed Dentition Period Using Catlan's Appliance: A Case Report. ISRN Dent. 2011;2011:298931. [DOI:10.5402/2011/298931] [PMID] []
4. Mc Donald. Dentistry for the Child and Adolescent. 8th Ed. Elsevier (A Division of Reed Elsevier India Pvt. Limited); 2005.
5. Peter S. Essentials of preventive and community dentistry. Arya (Medi) Publishing House; 2009.
6. Bayrak S, Tunc ES. Treatment of anterior dental crossbite using bonded resin-composite slopes: case reports. Eur J Dent. 2008 Oct;2(4):303-6. [DOI:10.1055/s-0039-1697397] [PMID] []
7. Hiremath MC, Suresh KS. Rapid Correction of Anterior Dental Crossbite Using A Sectional Fixed Appliance: A Case Report. Arch Oral Sci & Res. 2011; 1(1):11-13.
8. Major PW, Glover K. Treatment of anterior cross-bites in the early mixed dentition. J Can Dent Assoc. 1992 Jul;58(7):574-5, 578-9.
9. Kiyak HA. Patients' and parents' expectations from early treatment. Am J Orthod Dentofacial Orthop. 2006 Apr;129(4 Suppl):S50-4. [DOI:10.1016/j.ajodo.2005.09.018] [PMID]
10. Croll TP, Riesenberger RE. Anterior crossbite correction in the primary dentition using fixed inclined planes. II. Further examples and discussion. Quintessence Int. 1988 Jan;19(1):45-51.
11. Lee BD. Correction of crossbite. Dent Clin North Am. 1978 Oct;22(4):647-68. [DOI:10.1016/S0011-8532(22)01244-7] [PMID]
12. White L. Early orthodontic intervention. Am J Orthod Dentofacial Orthop. 1998 Jan;113(1):24-8. [DOI:10.1016/S0889-5406(98)70273-2] [PMID]
13. Yang EY, Kiyak HA. Orthodontic treatment timing: a survey of orthodontists. Am J Orthod Dentofacial Orthop. 1998 Jan;113(1):96-103. [DOI:10.1016/S0889-5406(98)70281-1] [PMID]
14. Asher RS, Kuster C, Erickson LC. Anterior dental crossbite correction using a simple fixed appliance: case report. Pediatr Dent. 1986; 8(1):53-5.
15. Croll TP, Riesenberger RE. Anterior crossbite correction in the primary dentition using fixed inclined planes. I. Technique and examples. Quintessence Int. 1987 Dec;18(12):847-53.
16. Croll TP. Correction of anterior tooth crossbite with bonded resin-composite slopes. Quintessence Int. 1996 Jan;27(1):7-10.
17. Croll TP, Lieberman WH. Bonded compomer slope for anterior tooth crossbite correction. Pediatr Dent. 1999 Jul-Aug;21(4):293-4.
18. Neena IE, Anantharaj A, Ashwini BL. Management of anterior teeth crossbite using double cantilever spring with posterior bite plane - A case report. CODS J Dent 2014; 6(2);122-3. [DOI:10.5005/cods-6-2-122]
19. Bindayel NA. Simple removable appliances to correct anterior and posterior crossbite in mixed dentition: Case report. Saudi Dent J. 2012 Apr;24(2):105-13. [DOI:10.1016/j.sdentj.2011.12.005] [PMID] []
20. Sockalingam SNMP, Khan KAM, Kuppusamy E. Interceptive Correction of Anterior Crossbite Using Short-Span Wire-Fixed Orthodontic Appliance: A Report of Three Cases. Case Rep Dent. 2018 Apr 29;2018:4323945. [DOI:10.1155/2018/4323945] [PMID] []
21. Graber TM. Orthodontics Principles and Practice. 3rd ed. Philadelphia: W.B. Saunders Company; 1972.
22. Proffit WR. Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod. 1978 Jul;48(3):175-86.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |