Journal of Research in Dental
and Maxillofacial Sciences
Volume 9, Issue 1 (3-2024)
J Res Dent Maxillofac Sci 2024, 9(1): 15-20 |
Back to browse issues page


Ethics code: confirmation attached
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esfahanizadeh G, Kooshki R, Karimipoor H, Rastin V. In Vitro Effects of Chlorhexidine and Listerine Mouthwashes on Color Stability of Glazed Bilayer Zirconia and IPS E.Max Ceramics. J Res Dent Maxillofac Sci 2024; 9 (1) :15-20
URL: http://jrdms.dentaliau.ac.ir/article-1-507-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-507-en.html



1- Department of Prosthodontics, Faculty of Dentistry, Tehran Medical Science, Islamic Azad University, Tehran, Iran
2- Department of Prosthodontics, Faculty of Dentistry, Tehran Medical Science, Islamic Azad University, Tehran, Iran ,Hamed64karimi@gmail.com
2- Department of Prosthodontics, Faculty of Dentistry, Tehran Medical Science, Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 257 kb]
(765 Downloads)
| Abstract (HTML) (3358 Views)
Full-Text: (1293 Views)
Abstract
Background and Aim: This study aimed to assess the effects of chlorhexidine (CHX) and Listerine mouthwashes on color stability of glazed bilayer zirconia and IPs e.max ceramics.
Materials and Methods: This in vitro experimental study was conducted on 36 glazed bilayer zirconia and IPS e.max ceramic specimens. The baseline CIE L*a*b* color parameters of specimens were measured by a spectrophotometer. The bilayer zirconia and IPS e.max ceramic specimens were then randomly assigned to two subgroups for immersion in 10 mL of 0.2% CHX (n=9) and 10 mL of Listerine (n=9). The specimens were immersed in the respective solutions for 2 minutes daily for 7 days. Next, their color parameters were spectrophotometrically measured again. The color change (∆E) of ceramics in the three groups was calculated and compared by the Kruskal-Wallis test and two-way ANOVA (alpha=0.05).
Results: The L*, a*, and b* color parameters of glazed bilayer zirconia and IPs e.max ceramic specimens were not significantly different at baseline (P=0.8) or after the intervention (P=0.6). The ∆E of the subgroups was not significantly different either (P>0.05).
Conclusion: Both glazed bilayer zirconia and IPs e.max ceramics showed clinically acceptable color stability (∆E<3.3) following immersion in CHX and Listerine mouthwashes.
Key Words: Color; Chlorhexidine; Listerine; Mouthwashes; Ceramics
Background and Aim: This study aimed to assess the effects of chlorhexidine (CHX) and Listerine mouthwashes on color stability of glazed bilayer zirconia and IPs e.max ceramics.
Materials and Methods: This in vitro experimental study was conducted on 36 glazed bilayer zirconia and IPS e.max ceramic specimens. The baseline CIE L*a*b* color parameters of specimens were measured by a spectrophotometer. The bilayer zirconia and IPS e.max ceramic specimens were then randomly assigned to two subgroups for immersion in 10 mL of 0.2% CHX (n=9) and 10 mL of Listerine (n=9). The specimens were immersed in the respective solutions for 2 minutes daily for 7 days. Next, their color parameters were spectrophotometrically measured again. The color change (∆E) of ceramics in the three groups was calculated and compared by the Kruskal-Wallis test and two-way ANOVA (alpha=0.05).
Results: The L*, a*, and b* color parameters of glazed bilayer zirconia and IPs e.max ceramic specimens were not significantly different at baseline (P=0.8) or after the intervention (P=0.6). The ∆E of the subgroups was not significantly different either (P>0.05).
Conclusion: Both glazed bilayer zirconia and IPs e.max ceramics showed clinically acceptable color stability (∆E<3.3) following immersion in CHX and Listerine mouthwashes.
Key Words: Color; Chlorhexidine; Listerine; Mouthwashes; Ceramics
Introduction
Dental ceramics are among the most popular tooth-colored restorative materials due to their optimal properties such as favorable biocompatibility, long-term clinical service, high strength, and excellent esthetics [1,2]. At present, patients have high demands and expectations with regard to the esthetic appearance of dental restorations [2,3]. Optical properties of tooth-colored restorations are influenced by the oral environment, as well as their composition and solubility [4]. It has been reported that acidic solutions such as cola, orange juice, coffee, stomach acid, and some mouthwashes can affect the optical properties and surface roughness of ceramic restorations [1,5]. Color change of restorations compromises their esthetic appearance [6].
Several mouthwashes such as chlorhexidine (CHX) are used as an adjunct to mechanical plaque removal because of their antimicrobial properties. However, long-term use of such mouthwashes including CHX can cause brownish discoloration of tooth and restoration surfaces, and dorsal surface of the tongue [6]. Due to its highly cationic nature, CHX reacts with anionic ions and exerts its antimicrobial effects as such. CHX is commonly used for treatment of oral infections, resolution of inflammation and mouth malodor, and decreasing the occurrence of dental caries [5]. A previous study showed that CHX had the least effect on color of ceramics, compared with other mouthwashes [7]. CHX is available in 0.2% and 0.02% concentrations, and is commonly used for dental plaque control since it is highly effective against the bacteria [8-10].
Listerine Zero is a non-alcoholic mouthwash and a neutral phenolic compound, which is used to prevent dental caries, dental plaque, and calculus formation [11]. However, information regarding its effect on color of ceramics is limited [12].
Evidence shows that of different commonly used solutions that cause discoloration of dental ceramics such as orange juice, tea, coffee, and cola, coffee has the highest effect [13,14]. However, information regarding the discoloration of ceramics caused by mouthwashes is limited.
Considering the gap of information regarding the effect of Listerine Zero on different types of ceramic restorations, this study aimed to compare the effects of CHX and Listerine Zero on color of glazed bilayer zirconia and IPS e.max ceramics.
Materials and Methods
This in vitro experimental study was ethically approved by the Research Council, Dental Faculty of Islamic Azad University (No: P.129.D.961110).
The sample size was calculated assuming alpha=0.05, beta=0.2, and study power of 80%.
The present study was conducted on 36 disc-shaped ceramic specimens in two groups (A and B). Group A included 19 discs of bilayer zirconia (Amann Girrbach, Germany) with 10 mm diameter and 2 mm thickness fabricated by the computer-aided design/computer aided manufacturing (CAD/CAM, Amann Girrbach, Germany) system. After coloring with A2 shade, the specimens were coated with a thin layer of glaze paste (IPS e.max Ceram Glaze, Ivoclar Vivadent, Schaan, Liechtenstein) and sintered in a vacuum furnace (Austromat 3001; Dekema Dental Keramiköfen, Germany) at 950°C for 30 seconds [11,14]. Group B included 19 discs with 10 mm diameter and 2 mm thickness fabricated from A2 shade IPS e.max Ceram ingots (Ivoclar Vivadent, Germany) by the press technique (Ivoclar Vivadent, Germany). They were also glazed at 740°C [14]. To remove superficial impurities, the specimens were rinsed with distilled water and auto-glazed. All specimens were immersed in distilled water and incubated at 37±1°C for 24 hours. The specimens in each group were divided into two subgroups. Specimens in the first subgroup were immersed in 0.2% CHX (Shahr Daru Pharmaceutical Co., Tehran, Iran) with a pH of 5.1 at 37°C once daily for 2 minutes for a total duration of 7 days [11,12]. The specimens in the second subgroup (n=9) were immersed in non-alcoholic Listerine mouthwash (Listerine® Tooth Defense Antic, Johnson & Johnson, Italy) with a pH of 4.2 at 37°C once daily for 2 minutes for a total duration of 7 days.
Two other discs were also fabricated as control to verify the fabrication process of specimens. They were immersed in distilled water once daily for 2 minutes for a total duration of 7 days.
All specimens were then immersed in artificial saliva (Rooyingar Sanaat, Tehran, Iran) during the time interval between immersions in mouthwashes. The artificial saliva was refreshed daily as well.
The CIE L*A*B* color system is used almost exclusively for color assessment in dentistry and defines the color space by three coordinates of L*, a* and b*. L* is similar to the Munsell system’s value, and a* and b* describe the chromatic characters of the color [15,16]. The baseline color parameters of dried specimens were measured by a calibrated spectrophotometer (T 70 PG instrument, Alma Park, Leicestershire, United Kingdom) against a white background. The color parameters of all specimens were measured in a reproducible position under similar conditions of D56 lighting at 380-780 nm wavelength [3]. After 7 days, the specimens were dried and their CIE L*a*b* color parameters were spectrophotometrically measured for the second time as explained earlier [11].
The color change (∆E) of specimens was calculated by the following formula:
ΔE*ab = ([ΔL*]2 + [Δa*]2 + [Δb*]2)1/2
ΔE values ranging from 1 to 3 are not detectable by the naked eye while values greater than 3.3 are clinically unacceptable [12].
Two-way ANOVA was used to analyze the effects of ceramic type, mouthwash type, and their interaction on ΔE*, ΔL*, Δa*, and Δb* values. Comparison of the means was performed by the Kruskal-Wallis test (alpha=0.05).
Results
Dental ceramics are among the most popular tooth-colored restorative materials due to their optimal properties such as favorable biocompatibility, long-term clinical service, high strength, and excellent esthetics [1,2]. At present, patients have high demands and expectations with regard to the esthetic appearance of dental restorations [2,3]. Optical properties of tooth-colored restorations are influenced by the oral environment, as well as their composition and solubility [4]. It has been reported that acidic solutions such as cola, orange juice, coffee, stomach acid, and some mouthwashes can affect the optical properties and surface roughness of ceramic restorations [1,5]. Color change of restorations compromises their esthetic appearance [6].
Several mouthwashes such as chlorhexidine (CHX) are used as an adjunct to mechanical plaque removal because of their antimicrobial properties. However, long-term use of such mouthwashes including CHX can cause brownish discoloration of tooth and restoration surfaces, and dorsal surface of the tongue [6]. Due to its highly cationic nature, CHX reacts with anionic ions and exerts its antimicrobial effects as such. CHX is commonly used for treatment of oral infections, resolution of inflammation and mouth malodor, and decreasing the occurrence of dental caries [5]. A previous study showed that CHX had the least effect on color of ceramics, compared with other mouthwashes [7]. CHX is available in 0.2% and 0.02% concentrations, and is commonly used for dental plaque control since it is highly effective against the bacteria [8-10].
Listerine Zero is a non-alcoholic mouthwash and a neutral phenolic compound, which is used to prevent dental caries, dental plaque, and calculus formation [11]. However, information regarding its effect on color of ceramics is limited [12].
Evidence shows that of different commonly used solutions that cause discoloration of dental ceramics such as orange juice, tea, coffee, and cola, coffee has the highest effect [13,14]. However, information regarding the discoloration of ceramics caused by mouthwashes is limited.
Considering the gap of information regarding the effect of Listerine Zero on different types of ceramic restorations, this study aimed to compare the effects of CHX and Listerine Zero on color of glazed bilayer zirconia and IPS e.max ceramics.
Materials and Methods
This in vitro experimental study was ethically approved by the Research Council, Dental Faculty of Islamic Azad University (No: P.129.D.961110).
The sample size was calculated assuming alpha=0.05, beta=0.2, and study power of 80%.
The present study was conducted on 36 disc-shaped ceramic specimens in two groups (A and B). Group A included 19 discs of bilayer zirconia (Amann Girrbach, Germany) with 10 mm diameter and 2 mm thickness fabricated by the computer-aided design/computer aided manufacturing (CAD/CAM, Amann Girrbach, Germany) system. After coloring with A2 shade, the specimens were coated with a thin layer of glaze paste (IPS e.max Ceram Glaze, Ivoclar Vivadent, Schaan, Liechtenstein) and sintered in a vacuum furnace (Austromat 3001; Dekema Dental Keramiköfen, Germany) at 950°C for 30 seconds [11,14]. Group B included 19 discs with 10 mm diameter and 2 mm thickness fabricated from A2 shade IPS e.max Ceram ingots (Ivoclar Vivadent, Germany) by the press technique (Ivoclar Vivadent, Germany). They were also glazed at 740°C [14]. To remove superficial impurities, the specimens were rinsed with distilled water and auto-glazed. All specimens were immersed in distilled water and incubated at 37±1°C for 24 hours. The specimens in each group were divided into two subgroups. Specimens in the first subgroup were immersed in 0.2% CHX (Shahr Daru Pharmaceutical Co., Tehran, Iran) with a pH of 5.1 at 37°C once daily for 2 minutes for a total duration of 7 days [11,12]. The specimens in the second subgroup (n=9) were immersed in non-alcoholic Listerine mouthwash (Listerine® Tooth Defense Antic, Johnson & Johnson, Italy) with a pH of 4.2 at 37°C once daily for 2 minutes for a total duration of 7 days.
Two other discs were also fabricated as control to verify the fabrication process of specimens. They were immersed in distilled water once daily for 2 minutes for a total duration of 7 days.
All specimens were then immersed in artificial saliva (Rooyingar Sanaat, Tehran, Iran) during the time interval between immersions in mouthwashes. The artificial saliva was refreshed daily as well.
The CIE L*A*B* color system is used almost exclusively for color assessment in dentistry and defines the color space by three coordinates of L*, a* and b*. L* is similar to the Munsell system’s value, and a* and b* describe the chromatic characters of the color [15,16]. The baseline color parameters of dried specimens were measured by a calibrated spectrophotometer (T 70 PG instrument, Alma Park, Leicestershire, United Kingdom) against a white background. The color parameters of all specimens were measured in a reproducible position under similar conditions of D56 lighting at 380-780 nm wavelength [3]. After 7 days, the specimens were dried and their CIE L*a*b* color parameters were spectrophotometrically measured for the second time as explained earlier [11].
The color change (∆E) of specimens was calculated by the following formula:
ΔE*ab = ([ΔL*]2 + [Δa*]2 + [Δb*]2)1/2
ΔE values ranging from 1 to 3 are not detectable by the naked eye while values greater than 3.3 are clinically unacceptable [12].
Two-way ANOVA was used to analyze the effects of ceramic type, mouthwash type, and their interaction on ΔE*, ΔL*, Δa*, and Δb* values. Comparison of the means was performed by the Kruskal-Wallis test (alpha=0.05).
Results
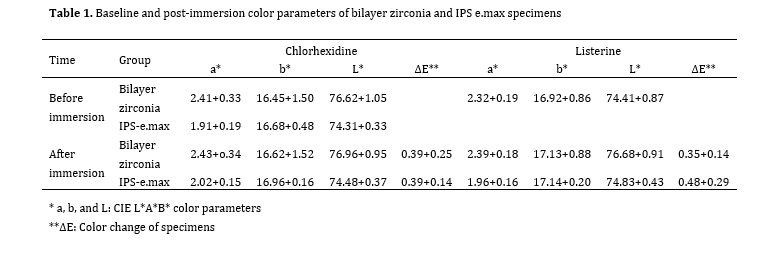
Table1 presents the baseline and post-immersion color parameters of the specimens and their ∆E in the groups. As shown, the baseline a*, b*, and L* parameters were not significantly different in the subgroups (P=0.8). The post-immersion a*, b*, and L* parameters were not significantly different in the subgroups either (P=0.7). The maximum ∆E (0.48) was noted in IPS e.max specimens immersed in Listerine, while the minimum ∆E was recorded in zirconia bilayer specimens immersed in Listerine (0.35). The ∆E values were not significantly different among the subgroups either (P=0.6). Also, all ∆E values were within the clinically acceptable range (∆E<3.3).
Discussion
Discussion
Considering the gap of information regarding the effect of Listerine Zero on different types of ceramic restorations, this study compared the effects of CHX and Listerine Zero on color of glazed bilayer zirconia and IPS e.max ceramics. The results showed no significant difference in color parameters of the groups at baseline or after the intervention. The ∆E values were not significantly different either.
Table 1. Baseline and post-immersion color parameters of bilayer zirconia and IPS e.max specimens
Derafshi et al. [11] evaluated the effects of CHX and Listerine mouthwashes on color stability of monolithic zirconia and feldspathic porcelain, and reported that their ∆E after immersion in CHX and Listerine was within the clinically acceptable range and non-perceivable by the human eye. They reported maximum ∆E following immersion of ceramics in CHX, which was different from the present findings. This difference may be due to higher frequency of spectrophotometric measurements of secondary color parameters in their study, which increased the accuracy of their findings. Palla et al. [17] evaluated the color stability of lithium disilicate ceramics after thermocycling and immersion in commonly consumed drinks. They showed clinically undetectable ∆E values in all groups, except for the specimens immersed in tea. Tea caused significant color change of specimens. Also, glazed ceramics had higher color stability than non-glazed ceramics. This finding was in line with the present results, showing optimal color stability of glazed ceramics.
Heydari et al. [18] evaluated the effect of polishing and glazing on discoloration of CERAMCO III dental porcelain immersed in CHX. They reported clinically acceptable color stability of both glazed and polished specimens with no significant difference in ∆E between them. Color change was not significant in any group, which was similar to the present findings. In general, it has been shown that CERAMCO III and glazed ceramics have high color stability against CHX [17-20].
Lee et al. [21] evaluated the color stability and surface properties of lithium disilicate ceramic, polymer-infiltrated ceramic, high-translucency zirconia, nano-ceramic resin, and feldspathic porcelain immersed in four types of mouthwashes. They revealed that immersion in Listerine Healthy White whitening mouthwash caused a significant color change in all groups, which was different from the present findings. Difference between their results and the present findings may be due to the use of different types of Listerine mouthwashes and the fact that they used 100 ppm mouthwash for 180 hours to simulate 15 years of clinical service. They found a significant difference in ∆E of zirconia in CHX and Listerine Healthy White groups in comparison with Listerine and distilled water groups. Difference between their results and the current findings can also be due to the use of high-translucency zirconia in their study versus bilayer zirconia in the present study, and their larger sample size (200 versus 38). Sasany et al. [4] evaluated the effect of different mouthwashes on optical properties of laminate and all-ceramic CAD/CAM restorations. They used lithium disilicate, Y-TZP, and Zirkonzahn zirconia and showed that both zirconia types experienced greater ∆E after immersion in Listerine, compared with CHX, which was similar to the present findings. They reported maximum ∆E in all three ceramics following immersion in Listerine. However, the ∆E in all groups was within the clinically acceptable range. Haralur et al. [22] assessed the effects of commonly consumed drinks and mouthwashes on color stability of lithium disilicate and zirconia-based ceramics. They fabricated lithium disilicate ceramics by the heat press technique. They compared lithium disilicate, bilayer zirconia, and monolithic zirconia specimens and concluded that immersion in coffee caused maximum ∆E in monolithic zirconia, followed by bilayer zirconia and then lithium disilicate. Immersion in green tea caused maximum ∆E in monolithic zirconia followed by bilayer zirconia. CHX caused minimum ∆E in all three ceramic groups. Their results were different from the present findings since they reported higher ∆E in monolithic zirconia and then bilayer zirconia. This difference may be due to the conduction of 3000 hydrothermal aging cycles between 5-55°C, which can cause small cracks in zirconia and increase its porosities while the aging process was not performed in the present study. Lower ∆E in bilayer zirconia can be due to its coating with feldspathic ceramic, which prevents the penetration of coloring agents into the cracks and subsequent discoloration [22]. Khaledi et al. evaluated the effect of CHX on over-glazed, auto-glazed, and polished ceramics. They reported significant ∆E in ceramics, which appears to be due to the high frequency of exposures to the mouthwash for 16 days [16].
The present study had some limitations. In vitro design limits the generalization of the results to the clinical setting, since oral clinical conditions and eating habits of individuals could not be simulated in vitro. Also, secondary color parameters were only measured once while it would be ideal to repeat each measurement at least three times [11].
Conclusion
{kind=link}
Derafshi et al. [11] evaluated the effects of CHX and Listerine mouthwashes on color stability of monolithic zirconia and feldspathic porcelain, and reported that their ∆E after immersion in CHX and Listerine was within the clinically acceptable range and non-perceivable by the human eye. They reported maximum ∆E following immersion of ceramics in CHX, which was different from the present findings. This difference may be due to higher frequency of spectrophotometric measurements of secondary color parameters in their study, which increased the accuracy of their findings. Palla et al. [17] evaluated the color stability of lithium disilicate ceramics after thermocycling and immersion in commonly consumed drinks. They showed clinically undetectable ∆E values in all groups, except for the specimens immersed in tea. Tea caused significant color change of specimens. Also, glazed ceramics had higher color stability than non-glazed ceramics. This finding was in line with the present results, showing optimal color stability of glazed ceramics.
Heydari et al. [18] evaluated the effect of polishing and glazing on discoloration of CERAMCO III dental porcelain immersed in CHX. They reported clinically acceptable color stability of both glazed and polished specimens with no significant difference in ∆E between them. Color change was not significant in any group, which was similar to the present findings. In general, it has been shown that CERAMCO III and glazed ceramics have high color stability against CHX [17-20].
Lee et al. [21] evaluated the color stability and surface properties of lithium disilicate ceramic, polymer-infiltrated ceramic, high-translucency zirconia, nano-ceramic resin, and feldspathic porcelain immersed in four types of mouthwashes. They revealed that immersion in Listerine Healthy White whitening mouthwash caused a significant color change in all groups, which was different from the present findings. Difference between their results and the present findings may be due to the use of different types of Listerine mouthwashes and the fact that they used 100 ppm mouthwash for 180 hours to simulate 15 years of clinical service. They found a significant difference in ∆E of zirconia in CHX and Listerine Healthy White groups in comparison with Listerine and distilled water groups. Difference between their results and the current findings can also be due to the use of high-translucency zirconia in their study versus bilayer zirconia in the present study, and their larger sample size (200 versus 38). Sasany et al. [4] evaluated the effect of different mouthwashes on optical properties of laminate and all-ceramic CAD/CAM restorations. They used lithium disilicate, Y-TZP, and Zirkonzahn zirconia and showed that both zirconia types experienced greater ∆E after immersion in Listerine, compared with CHX, which was similar to the present findings. They reported maximum ∆E in all three ceramics following immersion in Listerine. However, the ∆E in all groups was within the clinically acceptable range. Haralur et al. [22] assessed the effects of commonly consumed drinks and mouthwashes on color stability of lithium disilicate and zirconia-based ceramics. They fabricated lithium disilicate ceramics by the heat press technique. They compared lithium disilicate, bilayer zirconia, and monolithic zirconia specimens and concluded that immersion in coffee caused maximum ∆E in monolithic zirconia, followed by bilayer zirconia and then lithium disilicate. Immersion in green tea caused maximum ∆E in monolithic zirconia followed by bilayer zirconia. CHX caused minimum ∆E in all three ceramic groups. Their results were different from the present findings since they reported higher ∆E in monolithic zirconia and then bilayer zirconia. This difference may be due to the conduction of 3000 hydrothermal aging cycles between 5-55°C, which can cause small cracks in zirconia and increase its porosities while the aging process was not performed in the present study. Lower ∆E in bilayer zirconia can be due to its coating with feldspathic ceramic, which prevents the penetration of coloring agents into the cracks and subsequent discoloration [22]. Khaledi et al. evaluated the effect of CHX on over-glazed, auto-glazed, and polished ceramics. They reported significant ∆E in ceramics, which appears to be due to the high frequency of exposures to the mouthwash for 16 days [16].
The present study had some limitations. In vitro design limits the generalization of the results to the clinical setting, since oral clinical conditions and eating habits of individuals could not be simulated in vitro. Also, secondary color parameters were only measured once while it would be ideal to repeat each measurement at least three times [11].
Conclusion
The results revealed that both glazed bilayer zirconia and IPs e.max ceramics showed clinically acceptable color stability following immersion in CHX and Listerine for 7 days. Maximum ∆E was noted in IPS e.max specimens immersed in Listerine while minimum ∆E was noted in bilayer zirconia specimens immersed in Listerine.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors have no proprietary, financial, or other personal interest of any nature or kind in any product, service, and/or company that is presented in this article.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors have no proprietary, financial, or other personal interest of any nature or kind in any product, service, and/or company that is presented in this article.
Type of Study: Original article |
Subject:
Prosthodontics
References
1. Farheen S, Rajawat I, Rai N. Advancement in dental ceramics. Guident. 2023;16(6):16-7. [DOI:10.36106/gjra/9102935]
2. Karanjkar RR, Preshaw PM, Ellis JS, Holliday R. Effect of tobacco and nicotine in causing staining of dental hard tissues and dental materials: A systematic review and meta-analysis. Clin Exp Dent Res. 2023 Feb;9(1):150-64. [DOI:10.1002/cre2.683] [PMID] []
3. Adawi HA, Al Mialeem MM, Al Ahmari NM, Shariff M, Qahhar MA, Muharraq SMH, Alghazali NA. Assessment of Color Stainability of Computer-Aided Design and Computer-Aided Manufacturing (CAD/CAM) Ceramic Materials After Hot and Cold Coffee Immersion at Different Time Intervals. Med Sci Monit. 2021 Oct 3;27:e932745. [DOI:10.12659/MSM.932745] [PMID] []
4. Sasany R, Ergun-Kunt G, Yilmaz B. Effect of mouth rinses on optical properties of CAD-CAM materials used for laminate veneers and crowns. J Esthet Restor Dent. 2021 Jun;33(4):648-53. [DOI:10.1111/jerd.12720] [PMID]
5. Soygun K, Varol O, Ozer A, Bolayir G. Investigations on the effects of mouthrinses on the color stability and surface roughness of different dental bioceramics. J Adv Prosthodont. 2017 Jun;9(3):200-7. [DOI:10.4047/jap.2017.9.3.200] [PMID] []
6. Koksal T, Dikbas I. Color stability of different denture teeth materials against various staining agents. Dent Mater J. 2008 Jan;27(1):139-44. [DOI:10.4012/dmj.27.139] [PMID]
7. Alpkilic DS, Ongul D, Isler Deger S. Stainability of different ceramic materials against mouth rinses and effect of polishing after staining. J Prosthet Dent. 2021 Nov;126(5):686.e1-686.e7. [DOI:10.1016/j.prosdent.2021.06.002] [PMID]
8. Patel A, Sethuraman R, Prajapati P, Patel J, Naveen Y. A comparative analysis of staining characteristics of mouthrinses on provisional acrylic resin: An in vitro study. Journal of Interdisciplinary Dentistry. 2013;3(3):167-73. [DOI:10.4103/2229-5194.131213]
9. Kirubagaran SS. Effect of Fluoride Mouth Rinses Inducing Color Change in Esthetic Veneer Restoration-A Spectrophotometric Analysis. Journal of Pharmaceutical Sciences and Research. 2016;8(4):210-3.
10. Vlachojannis C, Al-Ahmad A, Hellwig E, Chrubasik S. Listerine® Products: An Update on the Efficacy and Safety. Phytother Res. 2016 Mar;30(3):367-73. [DOI:10.1002/ptr.5555] [PMID]
11. Derafshi R, Khorshidi H, Kalantari M, Ghaffarlou I. Effect of mouthrinses on color stability of monolithic zirconia and feldspathic ceramic: an in vitro study. BMC Oral Health. 2017 Nov 7;17(1):129. [DOI:10.1186/s12903-017-0419-9] [PMID] []
12. Singh I, Kalyan SS, Gupta RK, Lone P, Chandarani S. Spectrophotometric analysis of color stability of esthetic restorative material in chlorhexidine mouthwash: An in vitro study. J Conserv Dent. 2022 Nov-Dec;25(6):621-4. [DOI:10.4103/jcd.jcd_220_22] [PMID] []
13. Mathur S, Mathur T, Srivastava R, Khatri R. Chlorhexidine: The gold standard in chemical plaque control. Natl J Physiol Pharm Pharmacol. 2011;1(2):45-50.
14. Alhabdan AA, El-Hejazi AA. Comparison of surface roughness of ceramics after polishing with different intraoral polishing systems using profilometer and SEM. J Dent Health Oral Disord Ther. 2015;2(3):101-11. [DOI:10.15406/jdhodt.2015.02.00050]
15. Rosenstiel SF, Land MF, Walter R. Contemporary Fixed Prosthodontics. 6th ed. Elsevier Health Sciences; 2022.
16. Khaledi AA, Safari A, Adibi A, Adibi S. The Effect of Chlorhexidine Mouth Rinse on the Colour Stability of Porcelain with Three Different Surface Treatments: An in Vitro Study. Journal of Dental Biomaterials, 2014; 1(1): 3-8.
17. Palla ES, Kontonasaki E, Kantiranis N, Papadopoulou L, Zorba T, Paraskevopoulos KM, Koidis P. Color stability of lithium disilicate ceramics after aging and immersion in common beverages. J Prosthet Dent. 2018 Apr;119(4):632-42. [DOI:10.1016/j.prosdent.2017.04.031] [PMID]
18. Heydari M, Salari M, Heydari M. The Effect of Glazing and Polishing on color stability of CERAMCO III dental Porcelain in Chlorhexidine mouth rinse. J Res Dent Sci 2017; 13 (4) :174-80. [DOI:10.18869/acadpub.jrds.13.4.174]
19. Yilmaz C, Korkmaz T, Demirköprülü H, Ergün G, Ozkan Y. Color stability of glazed and polished dental porcelains. J Prosthodont. 2008 Jan;17(1):20-4. [DOI:10.1111/j.1532-849X.2007.00237.x] [PMID]
20. Etemadi A, Bitaraf T, Amini A, Goudarzi M, Nadafpour N. Bacterial Accumulation on Triclosan-Coated and Silk Sutures After Dental Implant Surgery. J Res Dent Maxillofac Sci. 2019;4(3):1-4. [DOI:10.29252/jrdms.4.3.1]
21. Lee JH, Kim SH, Yoon HI, Yeo IL, Han JS. Color stability and surface properties of high-translucency restorative materials for digital dentistry after simulated oral rinsing. Eur J Oral Sci. 2020 Apr;128(2):170-80.
22. Haralur SB, Raqe S Alqahtani N, Alhassan Mujayri F. Effect of Hydrothermal Aging and Beverages on Color Stability of Lithium Disilicate and Zirconia Based Ceramics. Medicina (Kaunas). 2019 Nov 19;55(11):749. [DOI:10.3390/medicina55110749] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |